peripheral nerve injuries
TRANSCRIPT

Nerve injuries in orthopedics
(common nerve injuries and their clinical features)
Reem Ahmed Alyahya212522156
Group 4
Introduction
• Peripheral nerve damage affecting the upper and lower extremities can vary widely in cause and extent. E.g. stretching, compression and transection.
• Many disorders, ranging from mild carpal tunnel syndrome to severe brachial plexopathy, need to be considered in a patient presenting with pain, sensory loss, or weakness involving the shoulder, arm, or hand.

Common nerve injuries
Upper limb
• Axillary nerve injury• Radial nerve injury• Median nerve injury• Ulnar nerve injury
Lower limb
• Femoral nerve injury• Sciatic nerve injury• Peroneal nerve injury

Nerve injuries in the upper limb
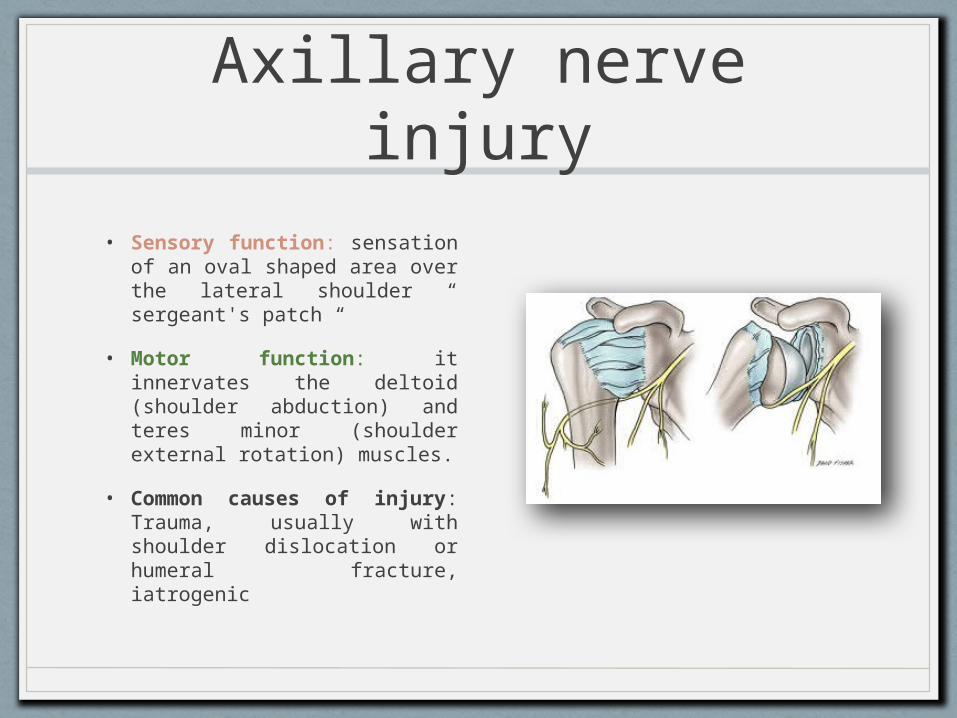
Axillary nerve injury• Sensory function:
sensation of an oval shaped area over the lateral shoulder “ sergeant's patch “
• Motor function: it innervates the deltoid (shoulder abduction) and teres minor (shoulder external rotation) muscles.
• Common causes of injury: Trauma, usually with shoulder dislocation or humeral fracture, iatrogenic
Axillary nerve injury manifestations
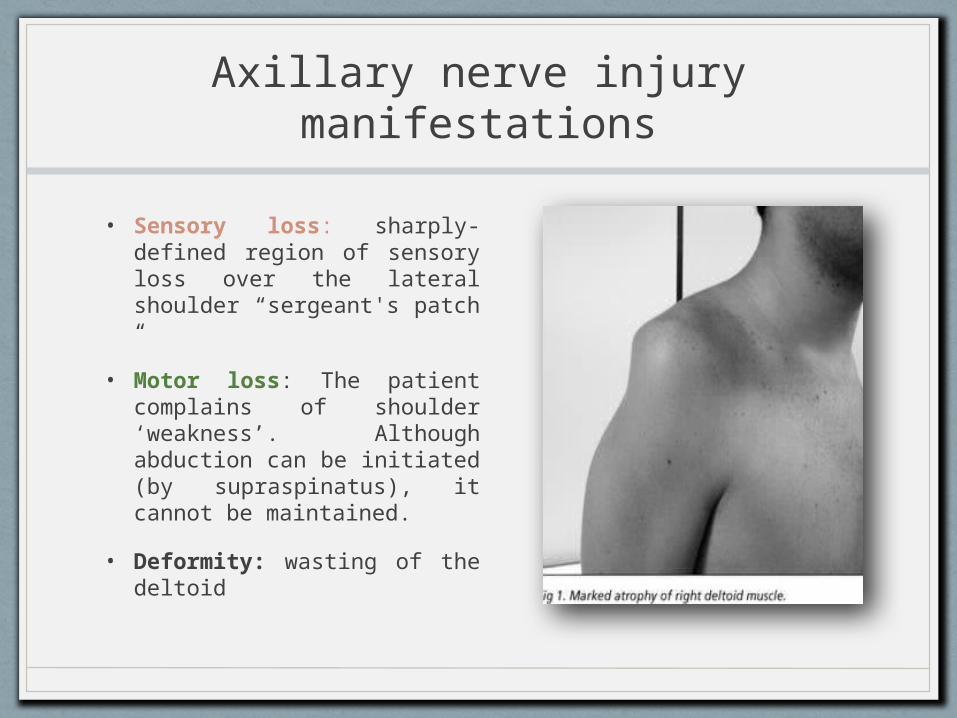
• Sensory loss: sharply-defined region of sensory loss over the lateral shoulder “sergeant's patch “
• Motor loss: The patient complains of shoulder ‘weakness’. Although abduction can be initiated (by supraspinatus), it cannot be maintained.
• Deformity: wasting of the deltoid
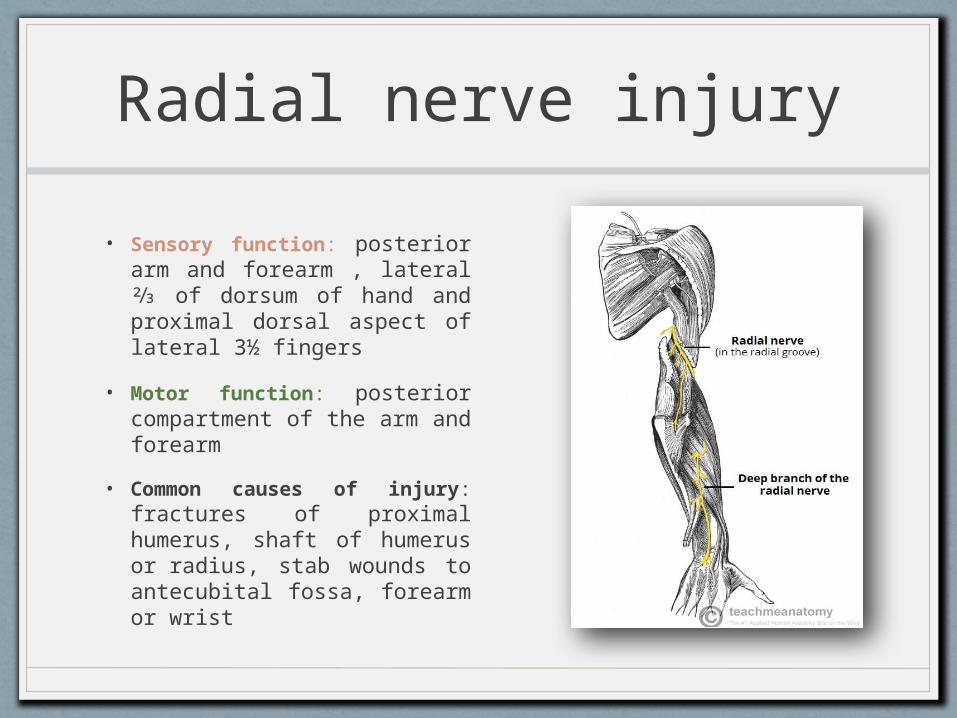
Radial nerve injury• Sensory function: posterior
arm and forearm , lateral ⅔ of dorsum of hand and proximal dorsal aspect of lateral 3½ fingers
• Motor function: posterior compartment of the arm and forearm
• Common causes of injury: fractures of proximal humerus, shaft of humerus or radius, stab wounds to antecubital fossa, forearm or wrist
Radial nerve injury manifestations
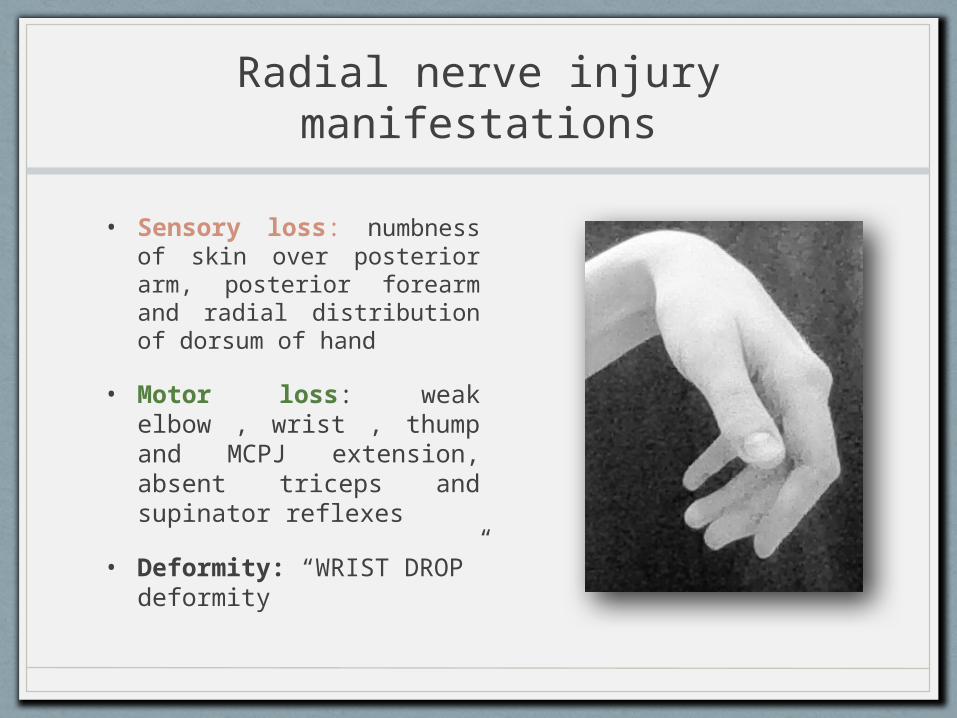
• Sensory loss: numbness of skin over posterior arm, posterior forearm and radial distribution of dorsum of hand
• Motor loss: weak elbow , wrist , thump and MCPJ extension, absent triceps and supinator reflexes
• Deformity: “WRIST DROP” deformity
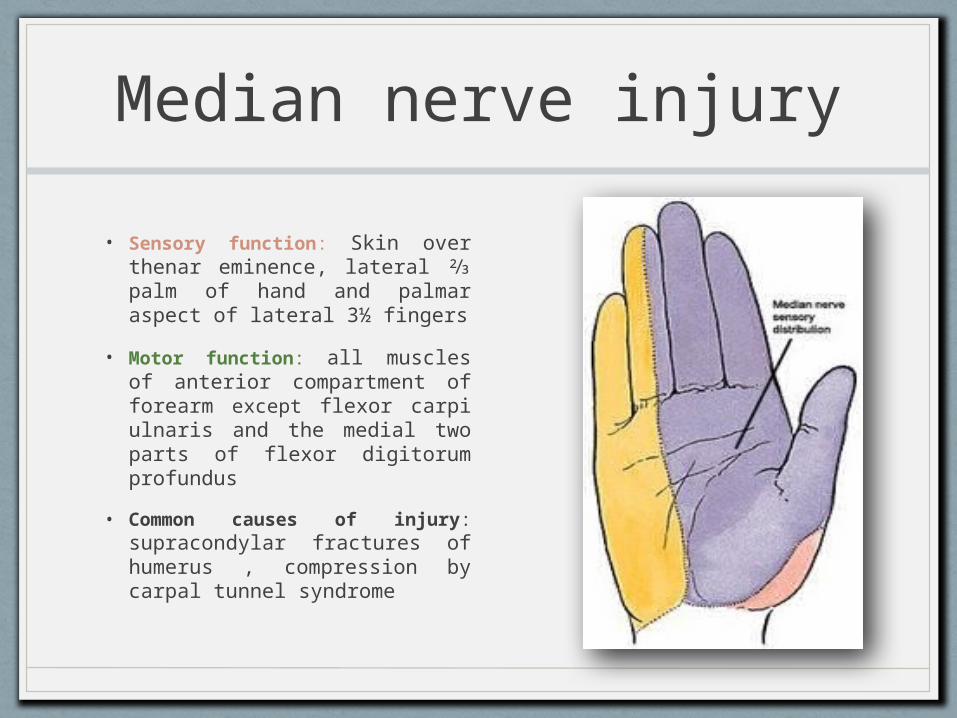
Median nerve injury• Sensory function: Skin over
thenar eminence, lateral ⅔ palm of hand and palmar aspect of lateral 3½ fingers
• Motor function: all muscles of anterior compartment of forearm except flexor carpi ulnaris and the medial two parts of flexor digitorum profundus
• Common causes of injury: supracondylar fractures of humerus , compression by carpal tunnel syndrome
Median nerve injury manifestations
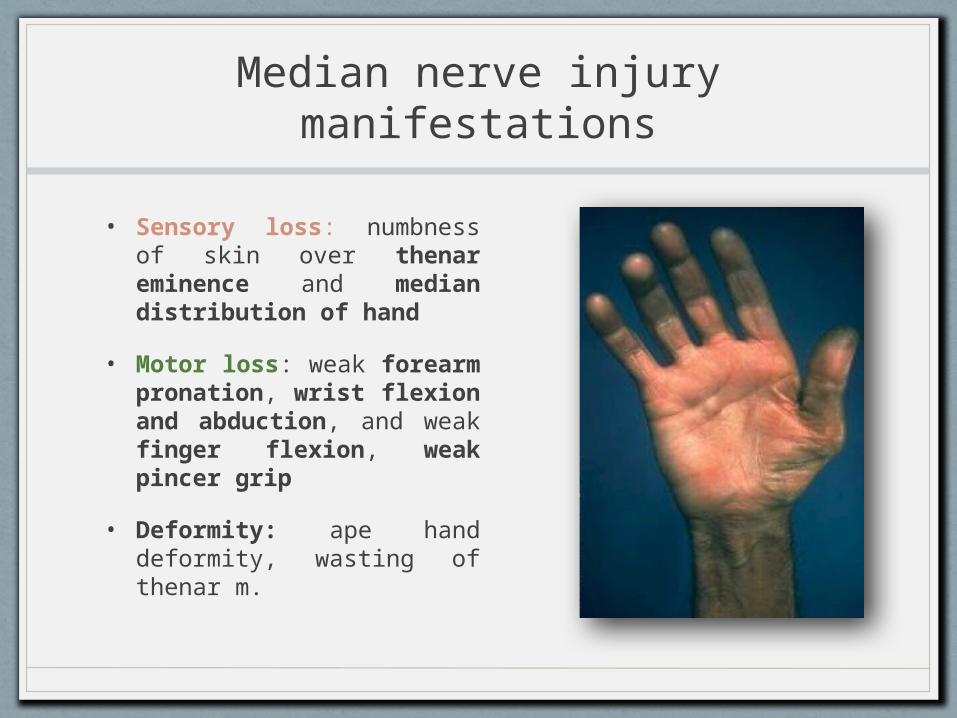
• Sensory loss: numbness of skin over thenar eminence and median distribution of hand
• Motor loss: weak forearm pronation, wrist flexion and abduction, and weak finger flexion, weak pincer grip
• Deformity: ape hand deformity, wasting of thenar m.

Ulnar nerve injury• Sensory function: skin over
hypothenar eminence, medial ⅓ palm of hand ,palmar aspect of lateral 1½ fingers
• Motor function: two muscles of anterior compartment of forearm , and most of the intrinsic muscles of the hand
• Common causes of injury: supracondylar fractures of humerus , compression cubital tunnel in the elbow.
Ulnar nerve injury manifestations
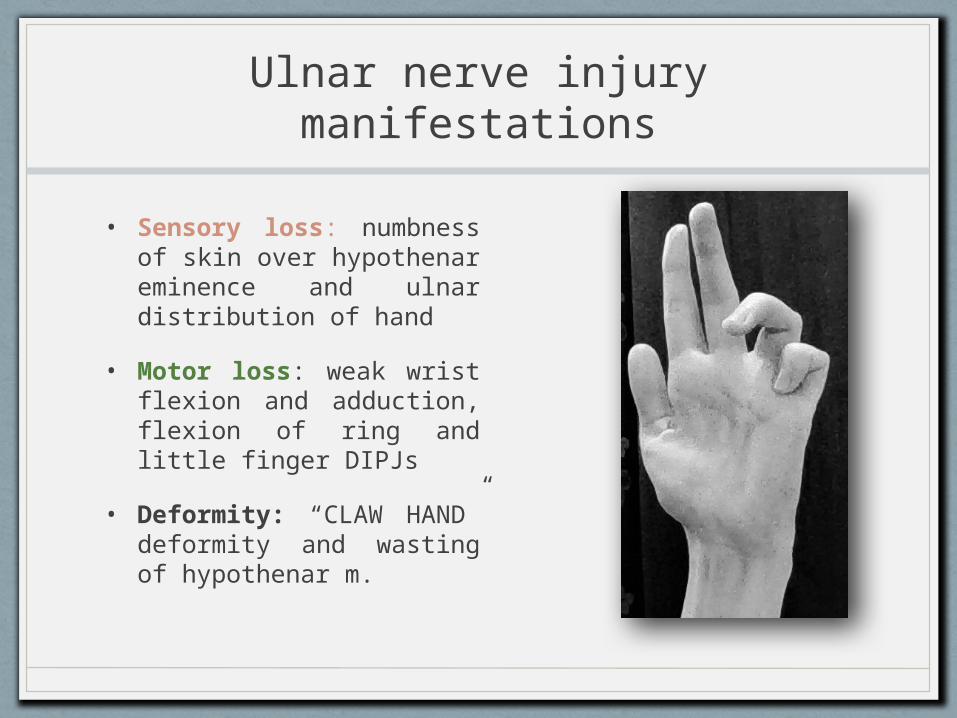
• Sensory loss: numbness of skin over hypothenar eminence and ulnar distribution of hand
• Motor loss: weak wrist flexion and adduction, flexion of ring and little finger DIPJs
• Deformity: “CLAW HAND” deformity and wasting of hypothenar m.
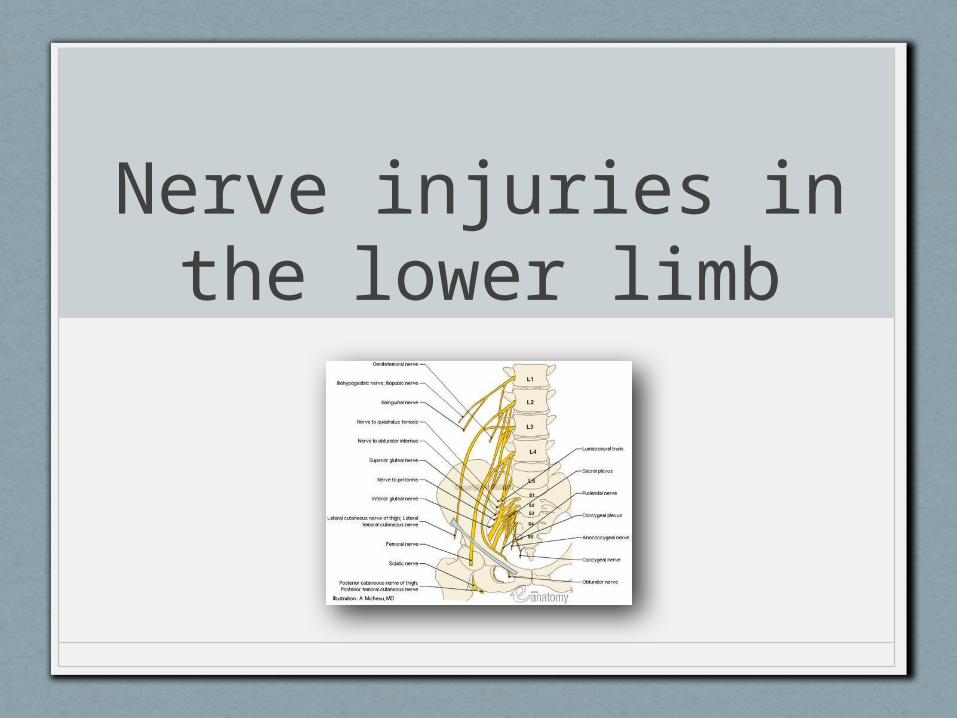
Nerve injuries in the lower limb
Femoral nerve injury
• The femoral nerve may be injured by a gunshot wound, hip or pelvic fractures, by pressure or traction during an operation or by bleeding into the thigh.
• Clinical manifestations: Quadriceps action is lacking (week knee extension). There is numbness of the anterior thigh and medial aspect of the leg. The knee reflex is depressed. Severe neurogenic pain is common
Sciatic nerve injury
• Division of the main sciatic nerve is rare except in gunshot wounds. Traction lesions may occur with traumatic hip dislocations and with pelvic fractures.
• Clinical manifestations: In a complete lesion the hamstrings and all muscles below the knee are paralyzed; the ankle jerk is absent. Sensation is lost below the knee, The patient walks with a drop foot and a high-stepping gait to avoid dragging the insensitive foot on the ground.

Common peroneal nerve injury
• The most frequent site of injury is just below the knee as the nerve wraps around the lateral aspect of the fibula, immediately before dividing into its deep and superficial branches
• Common causes include: Trauma or injury to the knee , Fracture of the fibula , Crossing the legs, protracted squatting, and leg casts.
Common peroneal nerve injury
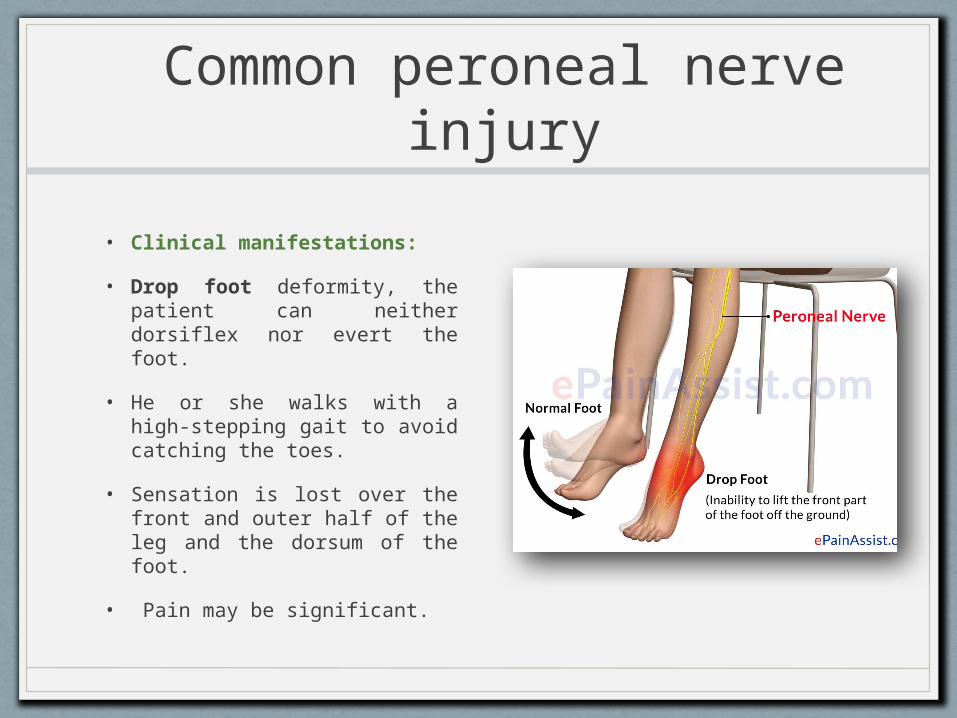
• Clinical manifestations:
• Drop foot deformity, the patient can neither dorsiflex nor evert the foot.
• He or she walks with a high-stepping gait to avoid catching the toes.
• Sensation is lost over the front and outer half of the leg and the dorsum of the foot.
• Pain may be significant.
References:
• Apley’s system of orthopedics and fractures 9th edition.
• UpToDate