perioperative management of traumatic brain...
TRANSCRIPT

Perioperative Management of Traumatic Brain Injury
C. Werner
Perioperative Management of TBI
• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

Primary and Secondary InjuryHypoxia, Hypotension, Hypercapnia,
Hypocapnia, Hyperglycemia, HyperthermiaVasospasm
Thrombus formation
ATP-deprivation
Anaerobic glycolysis
Lactic acidosis
Inflammation
Autodigestion

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

ICP - MonitoringDuration of Intracranial Hypertension and Response to
Treatment vs. Absolute ICP
Treggiari M. Neurocrit Care (2007)
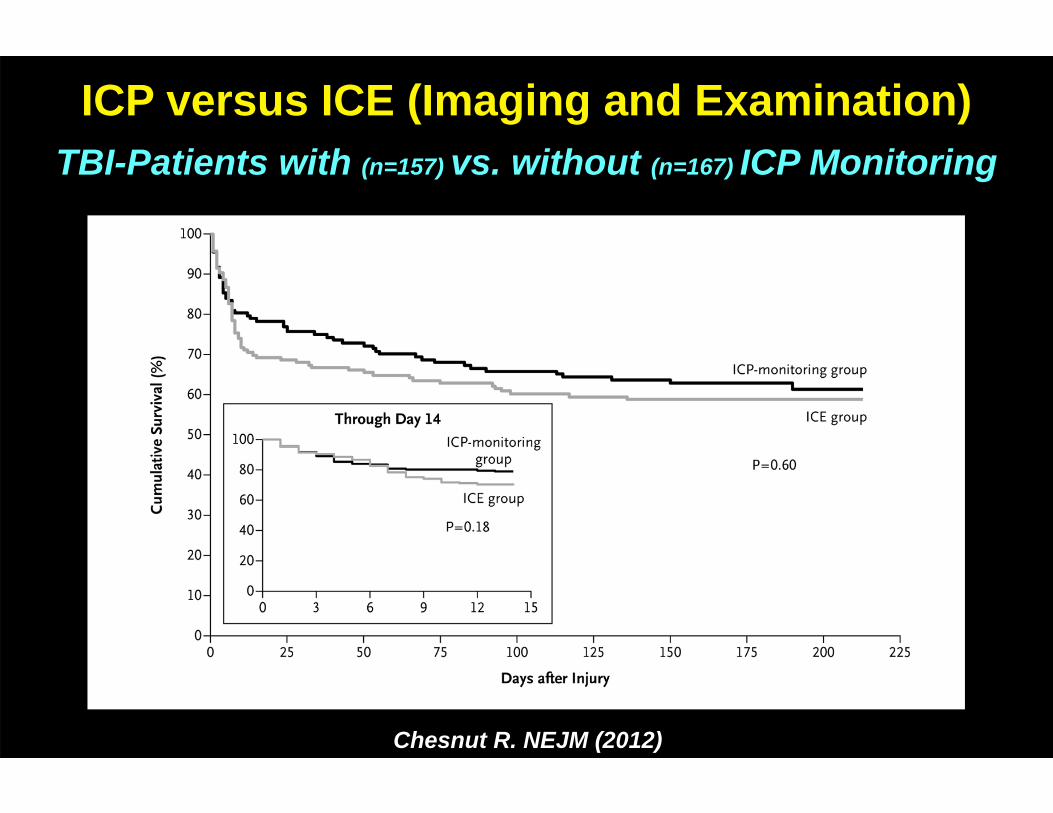
Chesnut R. NEJM (2012)
ICP versus ICE (Imaging and Examination)TBI-Patients with (n=157) vs. without (n=167) ICP Monitoring
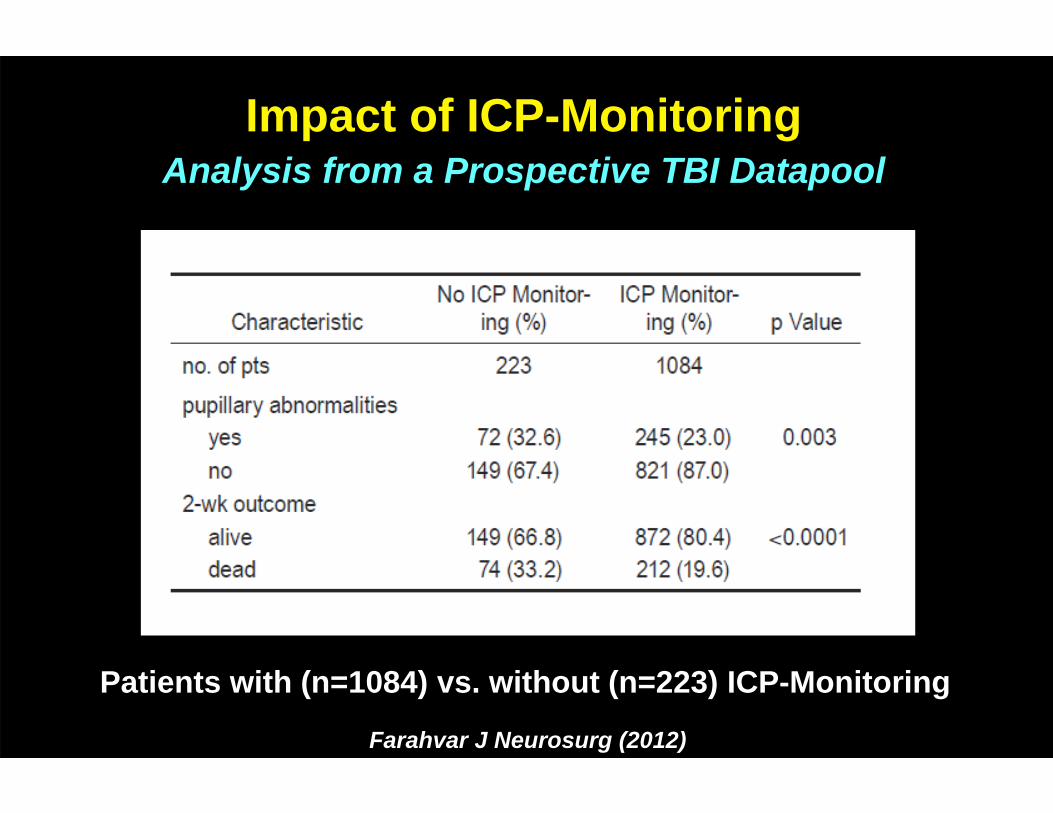
Farahvar J Neurosurg (2012)
Impact of ICP-MonitoringAnalysis from a Prospective TBI Datapool
Patients with (n=1084) vs. without (n=223) ICP-Monitoring

ICP - (and Tissue pO2) - Monitoring
Fauci AS. Harrisons´s Principles of Internal Medicine (17th Edition)
Treatment Goal:
ICP max. 20-22 mmHg(consider monitoring of SvjO2 or ptiO2)
Guideline for ICP - Monitoring
• comatose patients (GCS 3-8) with pathological CCT
• comatose patients (GCS 3-8) with normal CCT, but:
age > 40 years
unilateral or bilateral posturing
systolic arterial blood pressure < 90 mmHg
Carney N: Neurosurgery (2016)
• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI
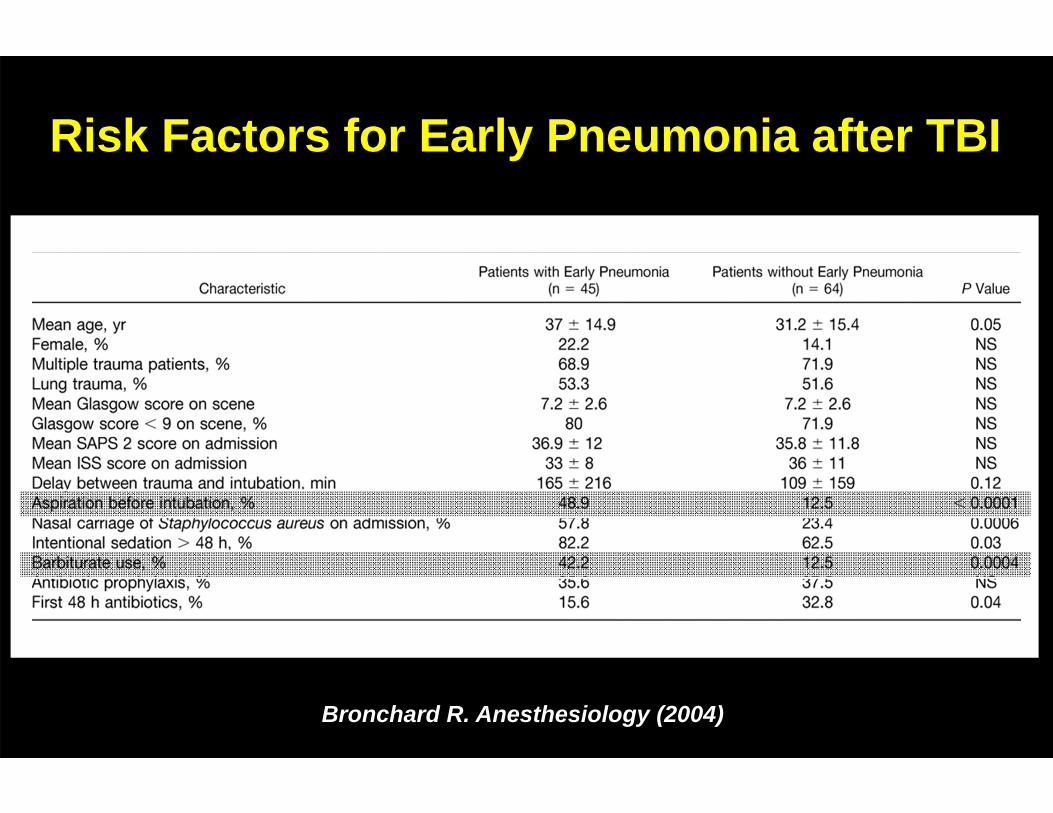
Risk Factors for Early Pneumonia after TBI
Bronchard R. Anesthesiology (2004)

Lung Brain
Ventilation Mode PCV VCV
Tidal Volume ~ 600 ml > 600 ml
PEEP high low
PaCO2 hypercapnia hypocapnia
Positioning evidence venous congestion
Volume Management hypovolemia normovolemia
Competing Treatment Strategies ?Lung vs. Brain

Alveolar Recruitment, PEEP OptimizationReduction of Atelectasis and Cyclic Recruitment
McGuire G. Crit Care Med (1997)
elevated

Kinetic Therapy
rightleft
Supine 30°
• Avoid flexion of the neck
• Avoid torsion of the neck
Maintain MAP constant!

Mortality with Kinetic Therapy in ARDS
Guérin C. N Engl J Med (2013)
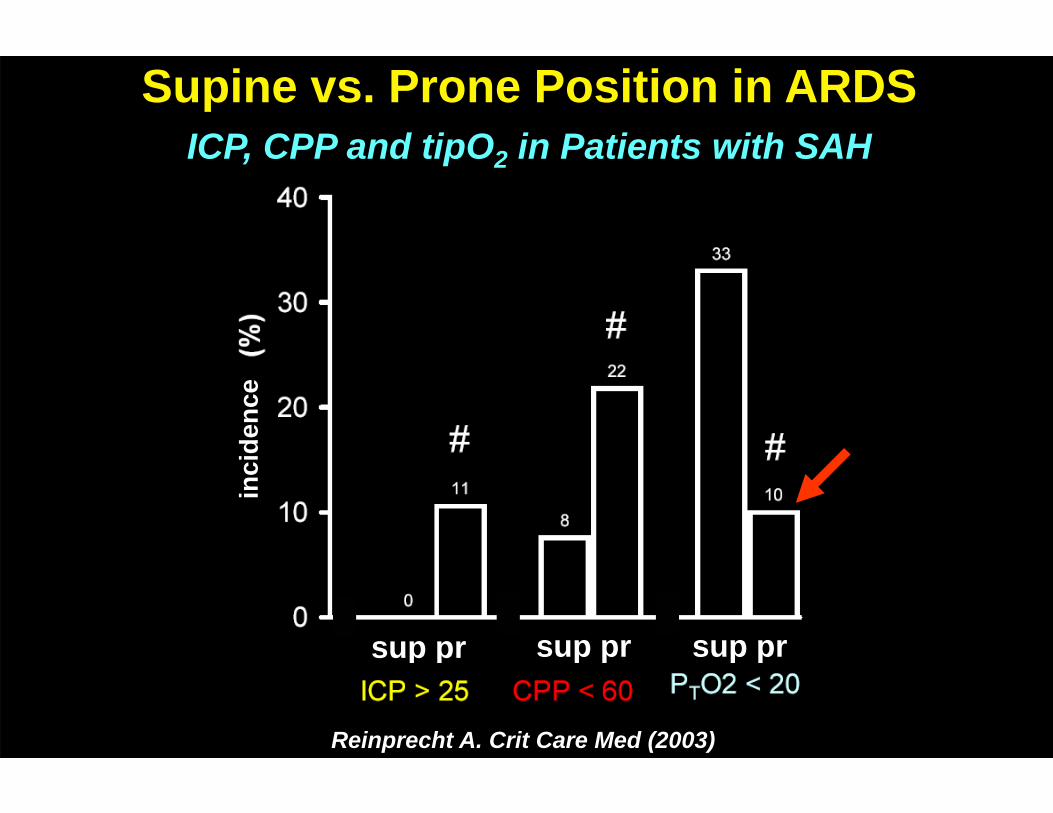
Reinprecht A. Crit Care Med (2003)
Supine vs. Prone Position in ARDSICP, CPP and tipO2 in Patients with SAH
sup pr sup pr sup pr
inci
denc
e

CBF with Hyperventilation
Coles JP: Brit J Anaesth (2007)

Management of Hyperventilation
Option: transient hyperventilation
• paCO2: 30-34 mmHg during ICP crisis or cerebral protrusion
Standard: normoventilation
• paCO2: 35-38 mmHg during tolerable ICP or SvjO2 < 50%
TBI Management Guidelines BTF 4th Ed. (2016); Stocchetti N: Chest (2005)

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

IMAPCT-StudiesPooled Data from 10 Studies and 8172 TBI Patients
Maas A. Lancet Neurology (2013)

ischemia
ARDS
(50) 60-70 mmHg
CPP
CB
F
Management of CPP
TBI Management Guidelines BTF 4th Ed. (2016)
Treatment Goals:
ICP < 20-22 mmHg
CPP (50) 60-70 mmHg

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI
Fluid Management
Maintain Normovolemia, Avoid Hypoosmolarity
adequate: - isotonic cristalloids
- isotonic colloids
- hypertonic cristalloids / colloids
rather adequate: - lactated Ringer´s solution
inadequate: - glucose, free water

Mannitol vs. Hypertonic SalineRetrospective, Dose and Volume to the Effect on ICP
Mangat HS. J Neurosurg (2015)

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

ICP, MAP and CPP during Barbiturate Coma
Cormio M. J Neurotrauma (1999)

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI
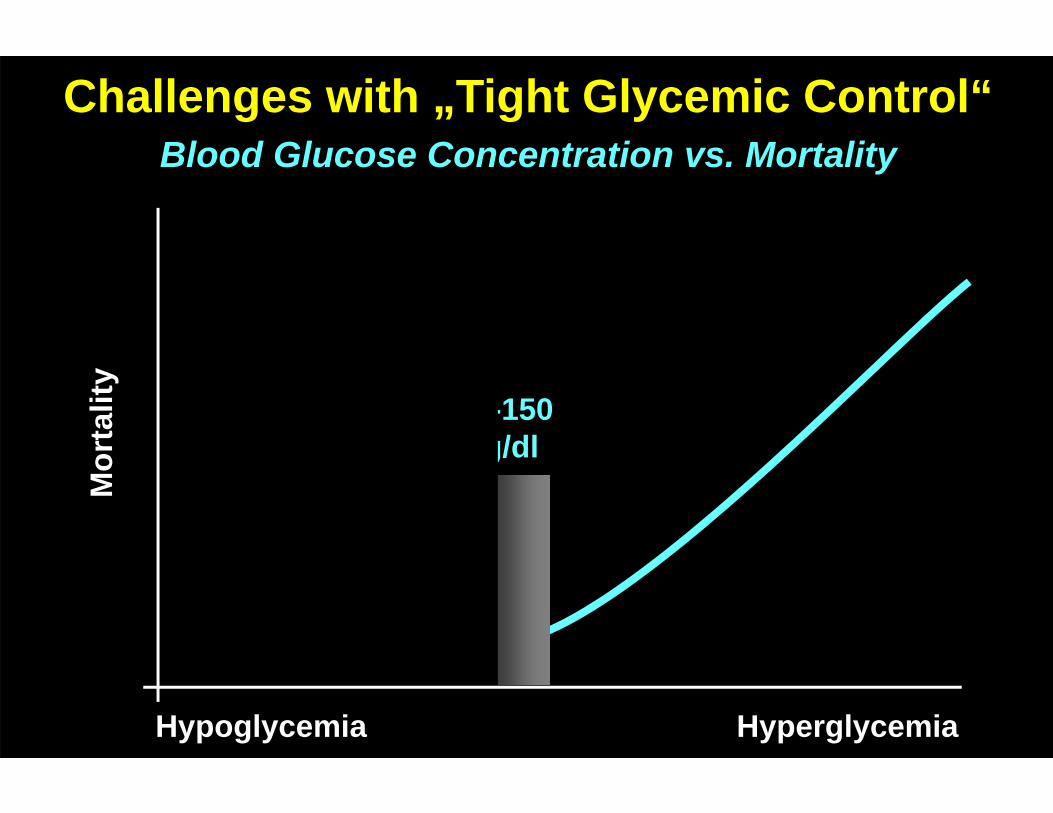
110-150 mg/dl
Challenges with „Tight Glycemic Control“Blood Glucose Concentration vs. Mortality
Mor
talit
y
HyperglycemiaHypoglycemia

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI
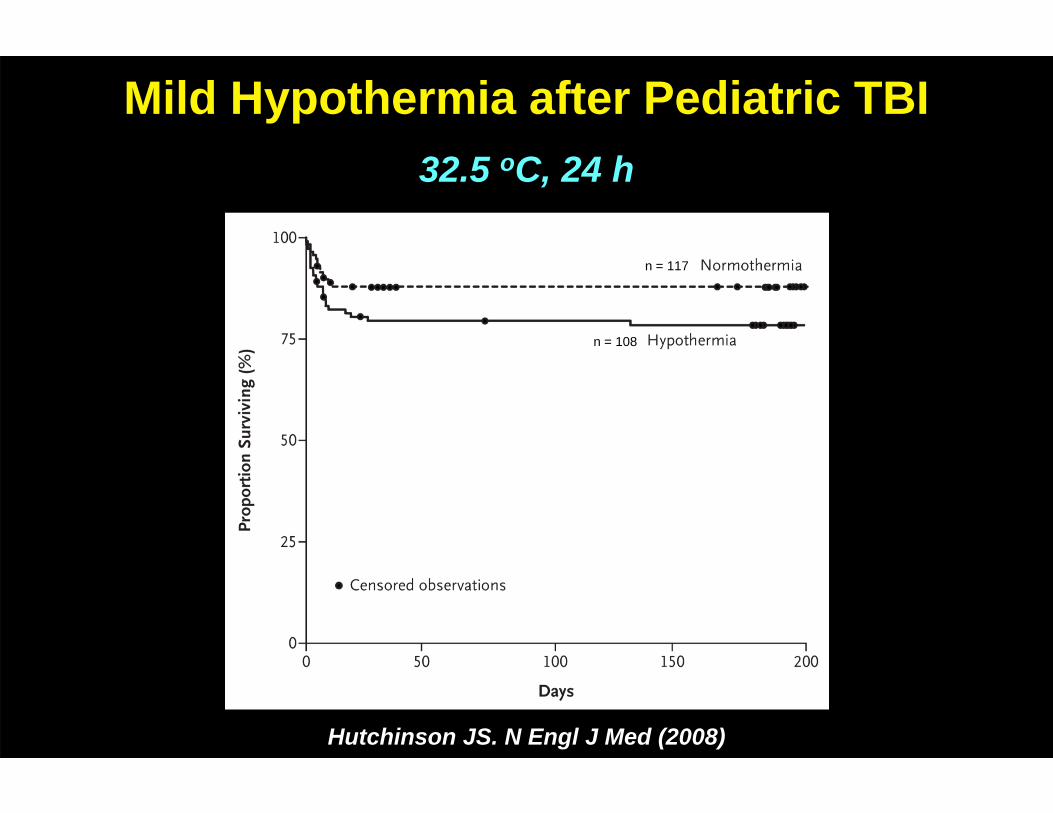
Mild Hypothermia after Pediatric TBI32.5 oC, 24 h
n = 117
n = 108
Hutchinson JS. N Engl J Med (2008)

Hutchinson JS. Dev Neurosci (2010)
n = 117
n = 108
Mild Hypothermia after Pediatric TBI32.5 oC, 24 h

Mild Hypothermia in Adult TBI33oC, 48 h (NABISH-II)
Clifton GL. Lancet Neurol (2011)
n = 108

Andrews PJD. N Engl J Med (2015)
n = 117
n = 108
ICP
CPP
Outcome
Mild Hypothermia in Adult TBI (32-35oC, 48 h)

HyperthermiaMortality and ICU/Hospital Length of Stay
Diringer MN: Crit Care Med (2004)
Treat Fever !

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI
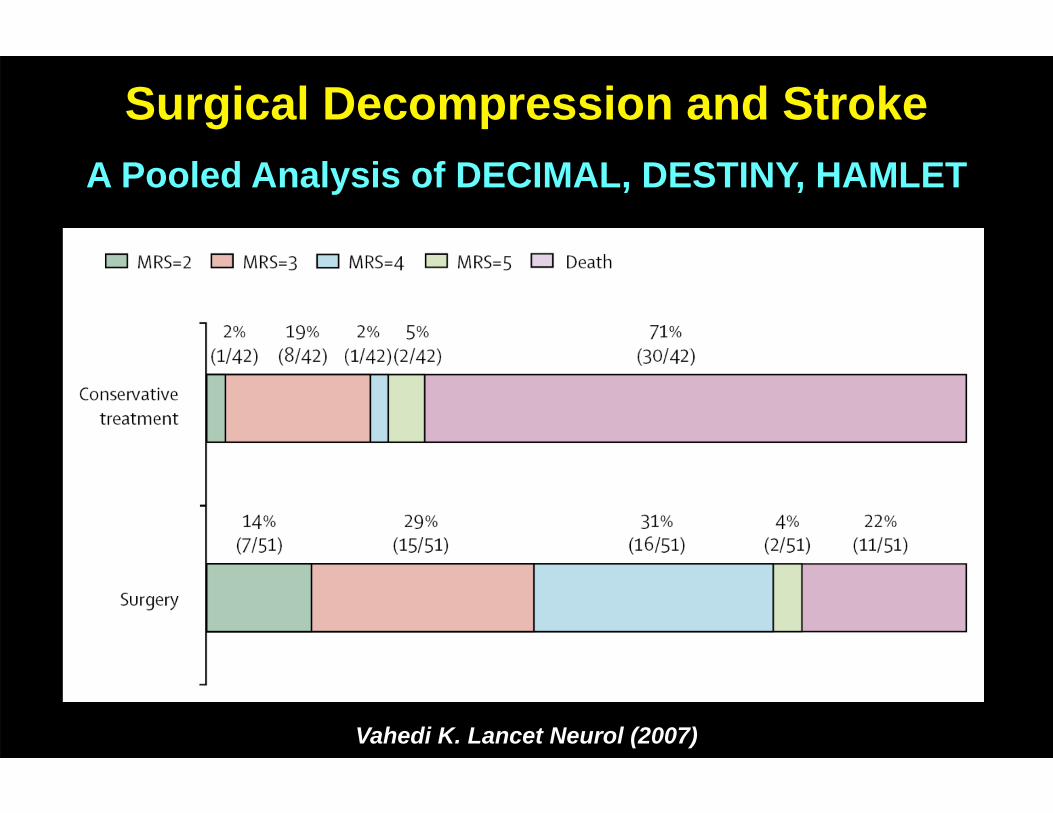
Surgical Decompression and StrokeA Pooled Analysis of DECIMAL, DESTINY, HAMLET
Vahedi K. Lancet Neurol (2007)
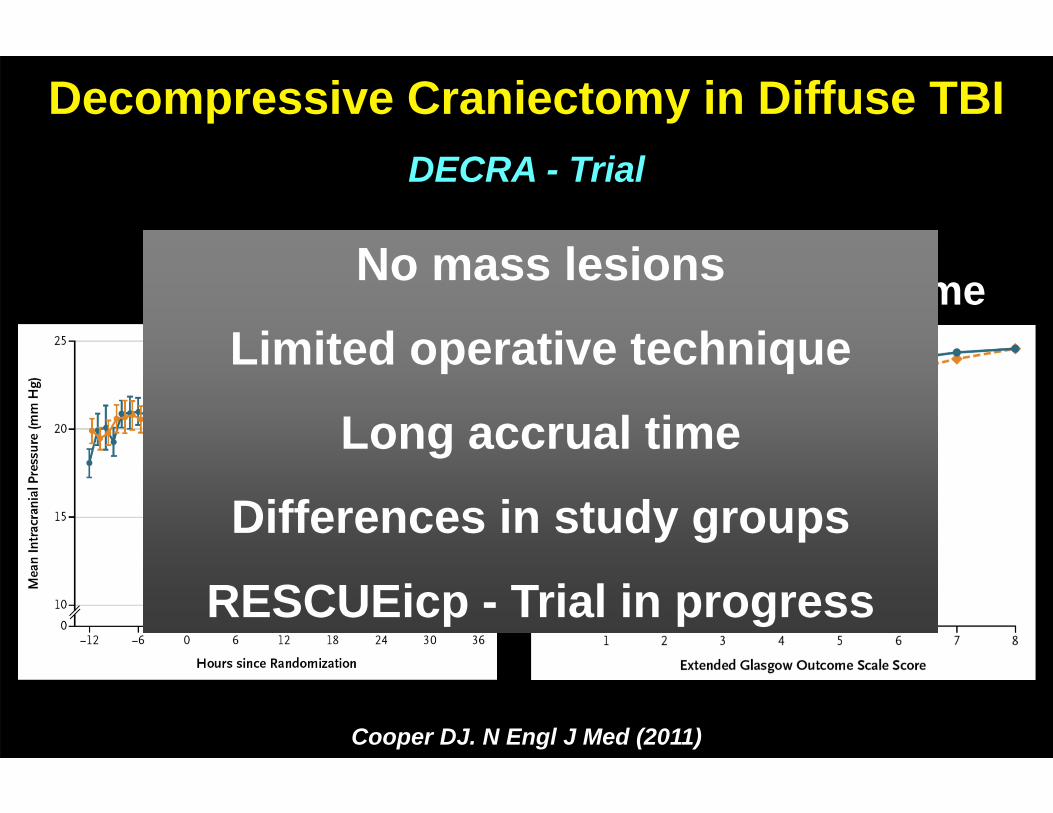
Decompressive Craniectomy in Diffuse TBIDECRA - Trial
Cooper DJ. N Engl J Med (2011)
ICP Composite OutcomeNo mass lesions
Limited operative technique
Long accrual time
Differences in study groups
RESCUEicp - Trial in progress
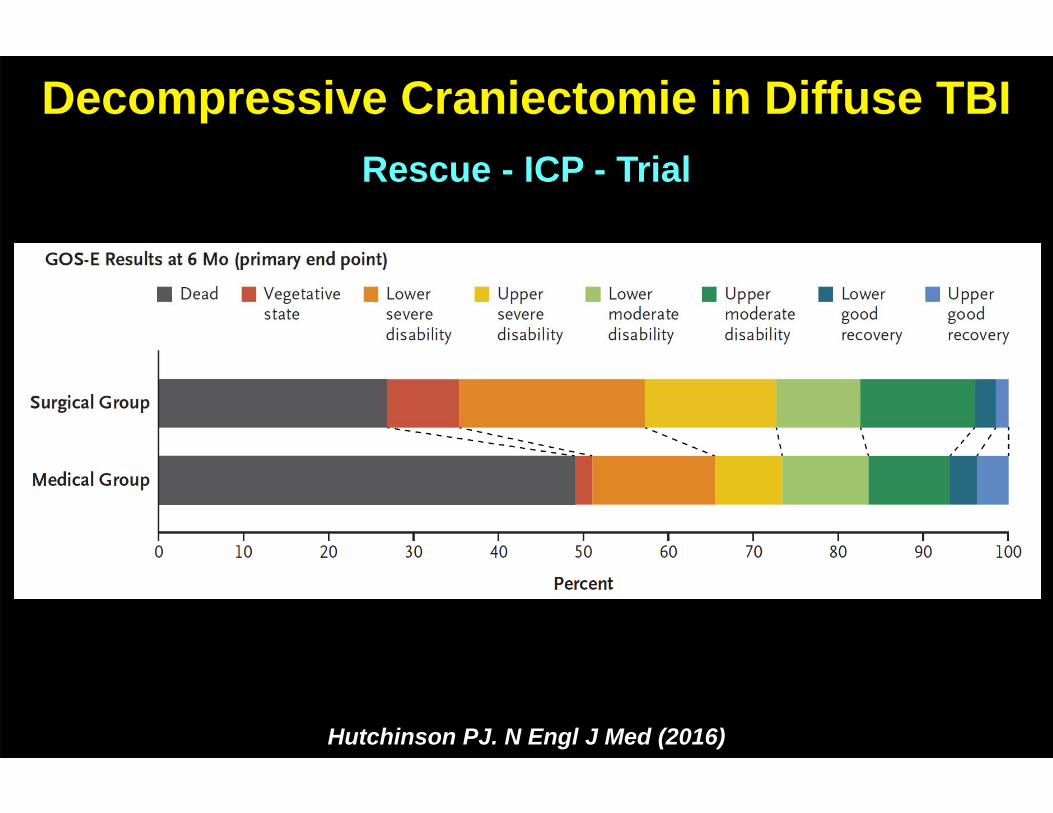
Decompressive Craniectomie in Diffuse TBIRescue - ICP - Trial
Hutchinson PJ. N Engl J Med (2016)

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

„Neuroprotective“ Drugs after TBI
CRASH trial collaborators. Lancet (2004); Langham J. The Cochrane Library (2003)
Skolnick BE. NEJM (2014); Temkin NR. Lancet Neurol (2007); Robertson CS. JAMA (2014)
• Steroids: No effect
• Ca++-antagonists: No effect
• Progesterone: No effect
• Magnesium: No effect
• Erythropoietin: No effect
• NMDA/AMPA antagonists: No effect
• Etc., etc………

• Pathophysiology
• Monitoring
• Oxygenation
• CPP
• Fluid Management
• Sedatives
• Glycemic Control
• Temperature Management
• Surgical Decompression
• „Neuroprotective“ Drugs
• Summary
Perioperative Management of TBI

• Normovolemia
• Normotension (CPP=(50) 60-70 mmHg)
• Normocapnia (paCO2=35-38 mmHg)
• Normoxemia (saO2>96 %)
• Normoglycemia (BS=110-150 mg/dl)
• Normothermia (T=36-37 °C)
Treatment Goals in TBIBasic Measures
ICP < 20-25 mmHg and CPP (50) 60-70 mmHg
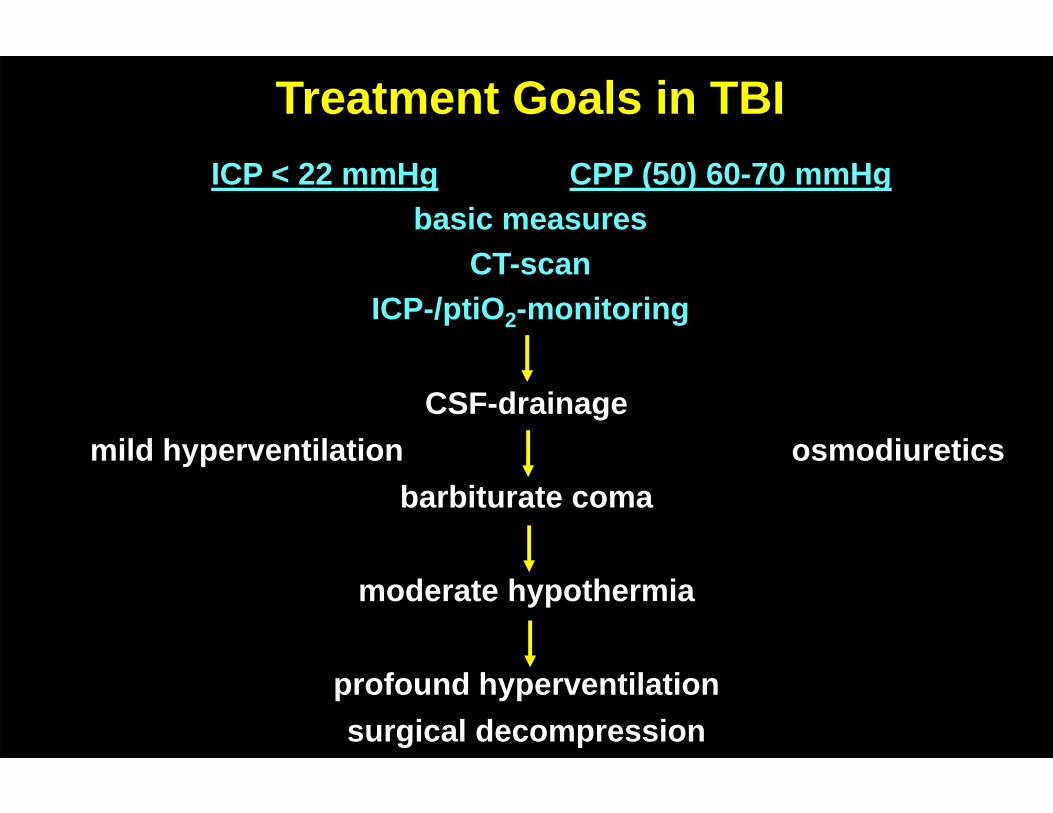
Treatment Goals in TBI
CSF-drainagemild hyperventilation osmodiuretics
barbiturate coma
moderate hypothermia
profound hyperventilationsurgical decompression
ICP < 22 mmHg CPP (50) 60-70 mmHgbasic measures
CT-scan ICP-/ptiO2-monitoring
