periodontology bartolucci one
TRANSCRIPT

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 1/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 2/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 3/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 4/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 5/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 6/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 7/333
Chapter 1
The mechanis mof periodonta l
destruction

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 8/333
THE MECHANISM OF PERIODONTAL DESTRUCTIO N
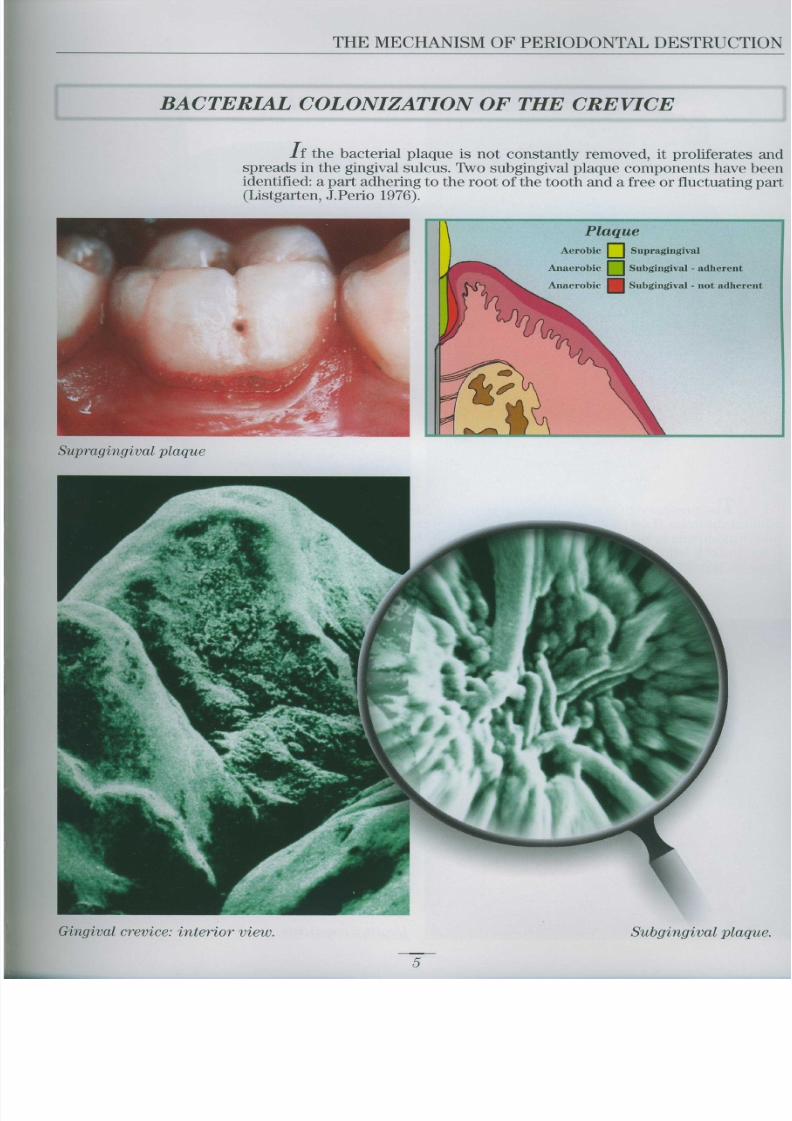
The term periodontal disease describes a group of diseases initiatin gin and remaining confined to the periodontal tissue . The m ajority are inflam-matory lesions caused by microorganisms accumulating in the pericrevicula rarea
Periodontal disease can be divided into
GINGIVITIS : the inflamma tory lesion is confined to the gingival tissue
PERIODONTITIS : the inflammatory lesion extends to the tooth support tis -
sues
Although more than 350 species of bacteria have been isolated in the mouth human periodontal infections are apparently caused by a specific microbia linfection . Less than 5% of microbial flora is, in fact, associated with disease .
--------------------------
Epithelial
attachment
0 .97 mm
Biologi c
width
.04 m i
Ideal gingival morphology and diagrammatic representation : pink colour, scalloped margin orange peel appearance, papillae in the interdental spaces, adequate band of keratinized gingiva .
The gingival sulcus is shallow (0 .69 mm), the epithelial attachment is located on the enamel (0 .97 mm)
the connective attachment is inserted in the root cementum (1 .07 mm) .The distance from the bottom of the sulcus to the osseous crest is known as the biological width (2 .04 mm) .
3

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 9/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 10/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 11/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 12/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 13/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 14/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 15/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 16/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 17/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 18/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 19/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 20/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 21/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 22/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 23/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 24/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 25/333
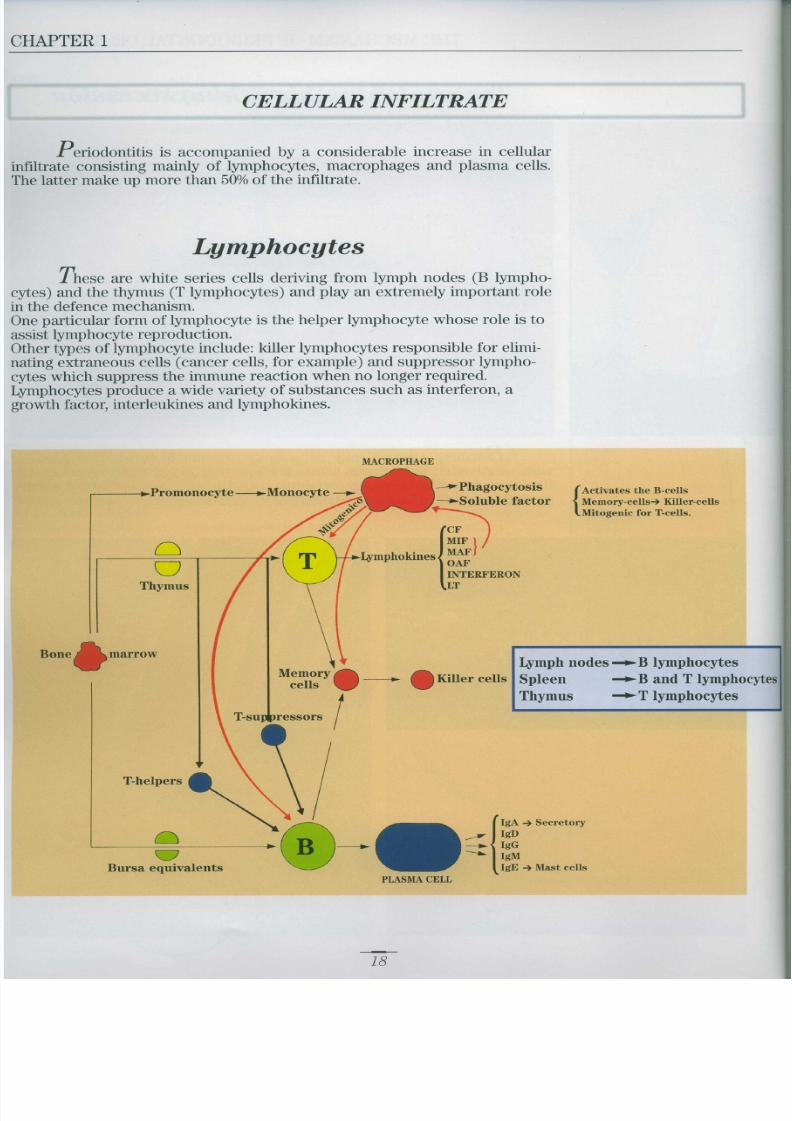
M acrophage s
These monocyte-derived cells have varied and extremely important func-acting as phagocytes, B lymphocyte activators and T lymphocyte mitogen s
the disease (gingivi-hydrolytic enzymes produced by th es, reducing cell damage . They also phagocyte the altered cells of the con-
of the disease (peri -
strategic position to identify and neutralise large quantities of antigens.ever, they are above all important for the interaction with the lymp hocyte T -
: this helps production o feukin-2 (IL2) which stimulates the T-helpers and T-killers to reproduce, trig -
lymphokine cascade .
Macrophages
20

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 26/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 27/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 28/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 29/333
CHAPTER 1
L ym p hok ine cascad e
1) A macrophage phagocytes a microorganis m
The M-T-helper complex secretes IL-1 (interleukin-1) . This activates T helpers to produce IL-2 (interleukin-2) which stimulates the reproduc
tion of T-helpers and T-killers
T-helpers produce B-cell growth factor which stimulates the cells t oreproduce and produce antibodies .
6) T-helpers produce gam ma-interferon
* activates killer T-cell s
* stimulates B-cell s* stimulates the M-T complex
Microorganism
s
2) Activation of the T-helper an d
bonding with a macrophag e
THE LYMPHOKINE CASCADE 6) Interferon

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 30/333
THE MECHANISM OF PERIODONTAL DESTRUCTION
Rosette formation : macrophage surrounde dby lymphocytes (which appear) adhering t othe surface and about to be phagocytized .When the lymphocytes have concluded theirtask, they are, in fact, eliminated .
25

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 31/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 32/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 33/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 34/333
THE MECHANISM OF PERIODONTAL DESTRUCTIO N
Plasma cells make up more than 50% of th e
tissue infiltrate and are also present in thecrevicular fluid .
Activation of a plasma cell wit hproduction of immunoglobuli n
antibodies
Plasma cell
Antibodies

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 35/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 36/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 37/333
CHAPTER 1
Pathogenesis of periodontal disease
Diagram of the succession of ev ents in the development of periodontitis
This condition, if not interrupted, tends to be self perpetuating with a poussez evolution
Productionof enzymes
Destructionof ground
substance
Passage of
plaqueproducts int o
the gingiva
FORMATION O FPLAQUE IN TH E
SULCUS
Onset o f
inflammation
Destructionof gingival
collagen
preading of
inflammation to
deep tissue sthrough the
vascular system
Formationof granulation
tissue
Proliferation
of junctionalepithelium

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 38/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 39/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 40/333
THE MECHANISM OF PERIODONTAL DESTRUCTION
The infection responsible for destruction of periodontal tissue occursin one or more sites and may last a variable period of time. The phenomenonmay die down spontaneously or as a result of treatment .
The host-parasite balance will remain stable until the same infection is re-acti -vated or a new one commences
ChronicSevere (SAP
Refractory (RE F
Periodontal diseases
Gingiviti s
Periodontitis
Juvenile Early onset (EOP )
Pre-pubera l
Localized (LIP )Generalized (JP)
35

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 41/333
CHAPTER 1
Periodontitis can be defined as a group of diseases associated with asubgingival microbial flora varying considerably in quantity and quality fro mdisease to disease . Strong evidence now exists to suggest that Actinobacillu s
Actinomicetemcomitans and Porphiromonas Gingivalis are exogenous form s
and represent the infective agents of periodontal diseases
Bacterial species associated with periodontitis
(Loesche et al. 1985; Slots and Rams 1990; Van Steenberger 1991
Bone reabsorption in chronic adult periodontitis .
Microbial species Clinical forms of periodontitis
LJP JP EOP SAP REF
A. Actinomicetemcomitans • • • • • • • • • • •
P. Gingivalis • • • • • • • • •
P. Intermedi a
B . Forsythus • • • • • • • • •
Fusobacterium spp
Peptostreptococcus spp
Campylobacter rectus • • • • •
Spirochetes • • • • • • • • • • • •

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 42/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 43/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 44/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 45/333
2
EXAMINATION OF THE PATIENT
M edical and stom atologic historyTo obtain a standardized assessment of the condition of organs o r
influencing the defini-
pharmaceutical or surgical treatment, a questionnaire is submitted t o
M edical history
N OES N OE SHave you ever had :
Hepatitis or liver problem s
Prolonged bleeding
Rh /1ma tie fever
Heart murmu r
High/low pressure
Chest/shoulder pain
Glaucoma
Contact lenses
Kidney problem s
Diabetes
TB
Emphysema/asthm a
Ulcer
Cancer
Epileps y
Venereal disease
Anaemi a
Blisters in the mouth
Ulcers in the mouth
Are you taking or have you YES N O
taken drugs such as :
Antibiotics
Aspirin
Anticoagulant s
Cortisone
ve drug s
Have you ever suffere d
adverse reactions to drugs ?
Which ones ?
Do you suffer from allergies ?
To what ?
If you are female :
Are you pregnant ?Are you taking contraceptives ?
Are you taking other
What kind of toothbrus h
Do you use a w ater pick ?
Do your gums bleed ?
Do you breath wit h
Do you grind you r
teeth at night ?
Do you have bad breath ?
Is your mouth painfu l
when you wake ?
Othe r
hormonal drugs?
Are you in the menopause ?
If yes, specify
iene treatment ?
dd any other° information you think m ight be important
Example of questionnaire to be submitted to the patient for correct compilation of medical history .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 46/333
DISEASE DIAGNOSI S
Clinical examinatio n
The aim of the clinical examination is to identify signs of possible disease The signs to look for include : colour, shape, consistency and height of the gin-giva and other oral structures such as the lips, mucosa, tongue, oropharynx floor of the mouth, hard palate and soft palate
It is important to examine both the general aspect of these structures and als oany possible localized alteration The gingiva are assessed on the basis of the following parameters
Marginal Festoonea Altered festonatio n
Edematous - FibrousFibroedematous
Flat - Glossy - Stipplin gdisappears
More coronal - More apica ljunction
PARAMETERS
Colour
Contours
43

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 47/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 48/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 49/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 50/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 51/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 52/333
Vitamin C deficiencyAscorbic acid (vitamin C) deficiency cause
sscurvy, a systemic disease cha racterized b yaccentuated weakness, anaemia, capillary dis -
ease and a tendency for both the skin an dmucosa (gingiva) to bleed, with the appearanc e
of petechiae on the limbs .
49
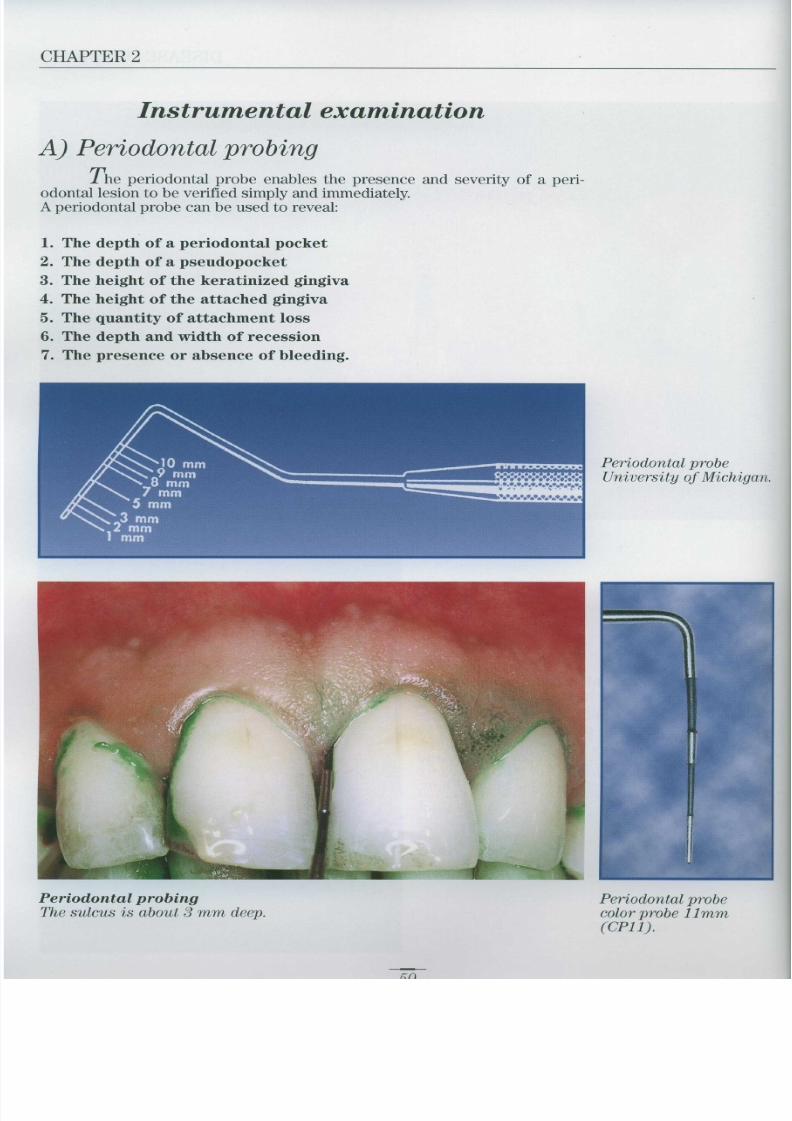
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 53/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 54/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 55/333
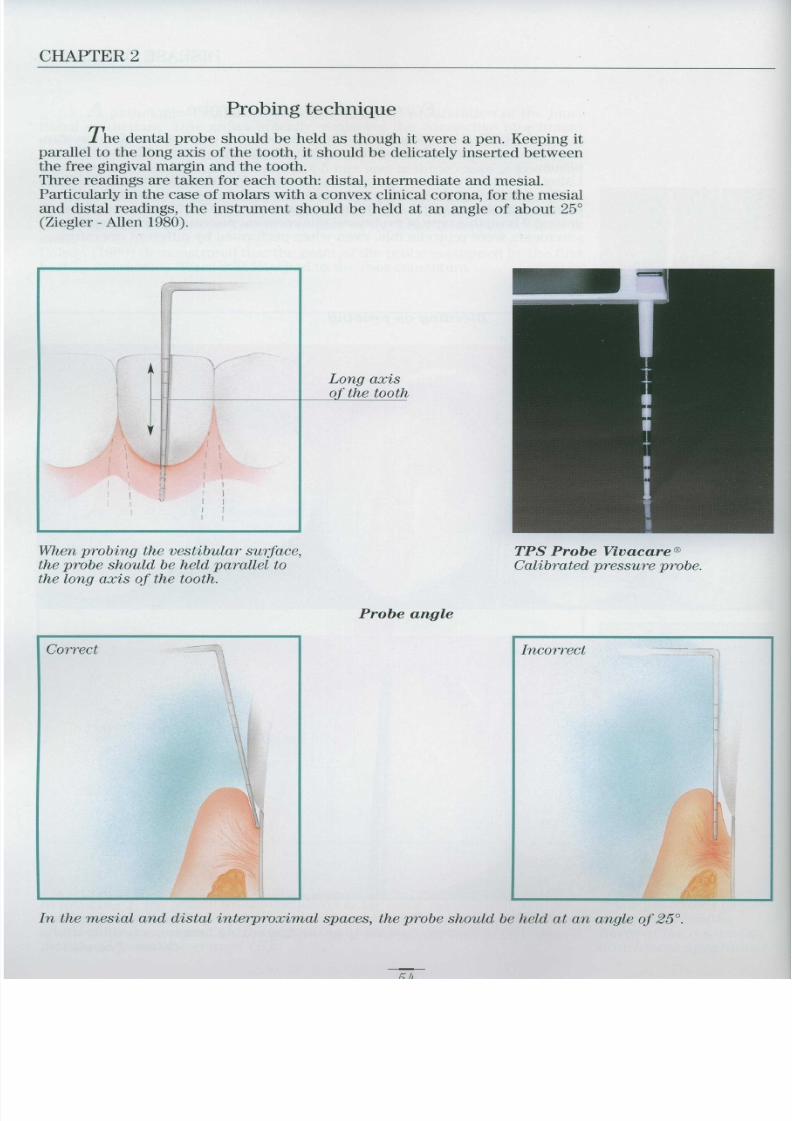
CHAPTER 2
pathological condition is known to cause proliferation of the junc-tional epithelium . This grows apically, replacing the connective attachmen tdestroyed by the disease, interposing between the gingival connective tissu eand the root surface, where it attaches itself
The epithelium m ay reach a length of 4-5 mm and in these cases is known a slong junctional epithelium (Listgarten - Rosenberg, 1979) .In the presence of inflammation, the probing depth w ill differ from the histo logic pocket depth . The probe penetrates the inflamed epithelial attachmen teasily, coming to a halt in the coronal part of the healthy connective attach
ment
Poison (1990) demonstrated that the point of the probe is stopped by the firs thealthy connective fibres still attached to the root cementum
Long junctiona l
epitheliu mNote the proliferation of
the junctional epitheli-
um as far as the roo t
cementum .
Junctional epitheliumDiagrammatic representation of the structure of the junctional epithelium
adhering to the surface of the enamel via hemidesmosomes .In drawing 1, the yellow line corresponds to the basal lamina and denta l
cuticle . In drawing 2, note the cemento-enamel junction with a small are aof afibrillar cementum (A), the beginning of the root cementum (C), th edentine (D) and the enamel (E)
Probing depthIn the presence ofinflammation, the
probe penetrates as faras the first health yfibres of the connectiveattachment apparatus .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 56/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 57/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 58/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 59/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 60/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 61/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 62/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 63/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 64/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 65/333
CHAPTER 2
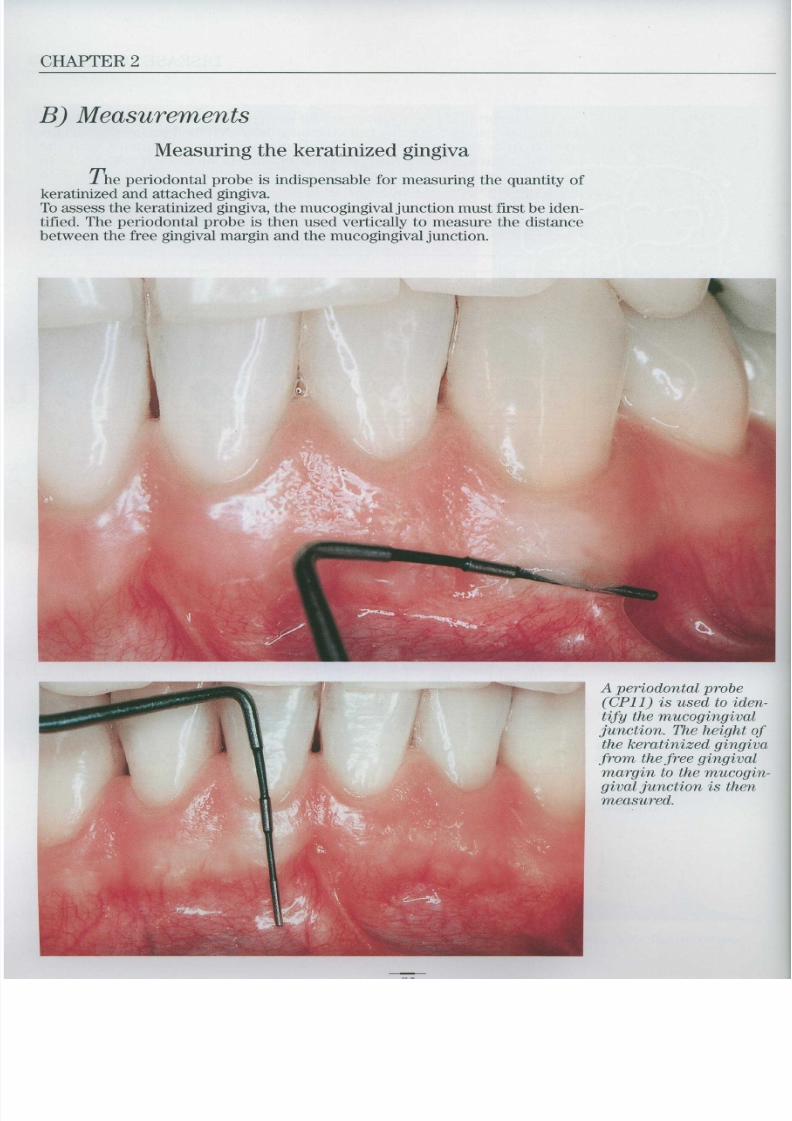
Measuring furcation involvement
Furcation involvement is diagnosed by probing with a special peri-odontal probe, the Nabers 2N
Classification
Degree Furcation involvemen t
Horizontal loss of bone tissue not exceeding 2-3 rum of the depth o f
the furcation
A: Horizontal loss of bone tissue for less than half the furcation
B: Horizontal loss of bone tissue for more than half the furcation
C: Almost complete horizontal loss of bone tissue
A small diaphragm remains
Total loss of interradicular bon e
otherwise known as a through-and-through furcation)
Nabers 2N probe .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 66/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 67/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 68/333
DISEASE DIAGNOSI S
Degree III
Total loss of interradicular bone .Degree III is also known as a
through-and-through furcation
65

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 69/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 70/333
DISEASE DIAGNOSIS
Orthodontic trauma
Mono-directional forces exerted on individual teeth produce pres-sure and tension fields within the periodontal space . As a result, the toothbecom es progressively more m obile and starts migrating in the direction of th eforce When the tooth leaves the influence of the trauma, the periodontium is reor-ganized and the tooth becomes stable in its new position
Tension zone
. 0 Stretched ligament .0 Bone apposition
. ©Dilated vessels .
reabsorption . 0 Torn periodontal fibres .
Occlusion traum a
Bone reabsorption caused by excessive occlusa l•
• accompanied by attachment loss
(Glossary of Periodontic terms . AmericanAcademy of Periodontology, 1986 )
Tooth mobility
Ingravescent:Presence of disease in progress
(Occlusion trauma)
(Inflammatory)Stabilized :
Poor bone support
67

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 71/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 72/333
DISEASE DIAGNOSI S
CLINICAL CASE
The clinical case illustrates a typical diagnostic and therefore thera-peutic error .A young patient (male, aged 15) presented mobility of the left upper latera lincisor and a diastema between the central and lateral incisors.The initial diagnosis wa s : occlusion damage and night grinding of the teeth forpsychological reasons .
Dental treatment consisted of selective grinding and construction of a resi n"bite" to wear at night . The youth (with divorced parents) was also referred t oa psychologist After a year o f psychotherapy , "bite" and selective grinding, the patient - still along way from being cured - was referred for a second opinion The diagnosis was : juvenile periodontitis The correct diagnosis was followed by suitable and successful treatment (se echapter 13)
The reddened an dcollapsed interdenta l
papilla is a symptom of
reabsorption of the
underlying bone .
69

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 73/333
CHAPTER 2
The clinical recordAll clinical and instrumental data and the patient's medical histor y
should be gathered together in a clinical record
Maxillary arch
• f t t • • • • I
f8 17 1 6• g 14 13 12 11 2123 24 25 6_ 37- 2S
32
Vestibular
Lingual
2
3
Mandibular arch
Vestibular
Lingua l
3
3
2

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 74/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 75/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 76/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 77/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 78/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 79/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 80/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 81/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 82/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 83/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 84/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 85/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 86/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 87/333
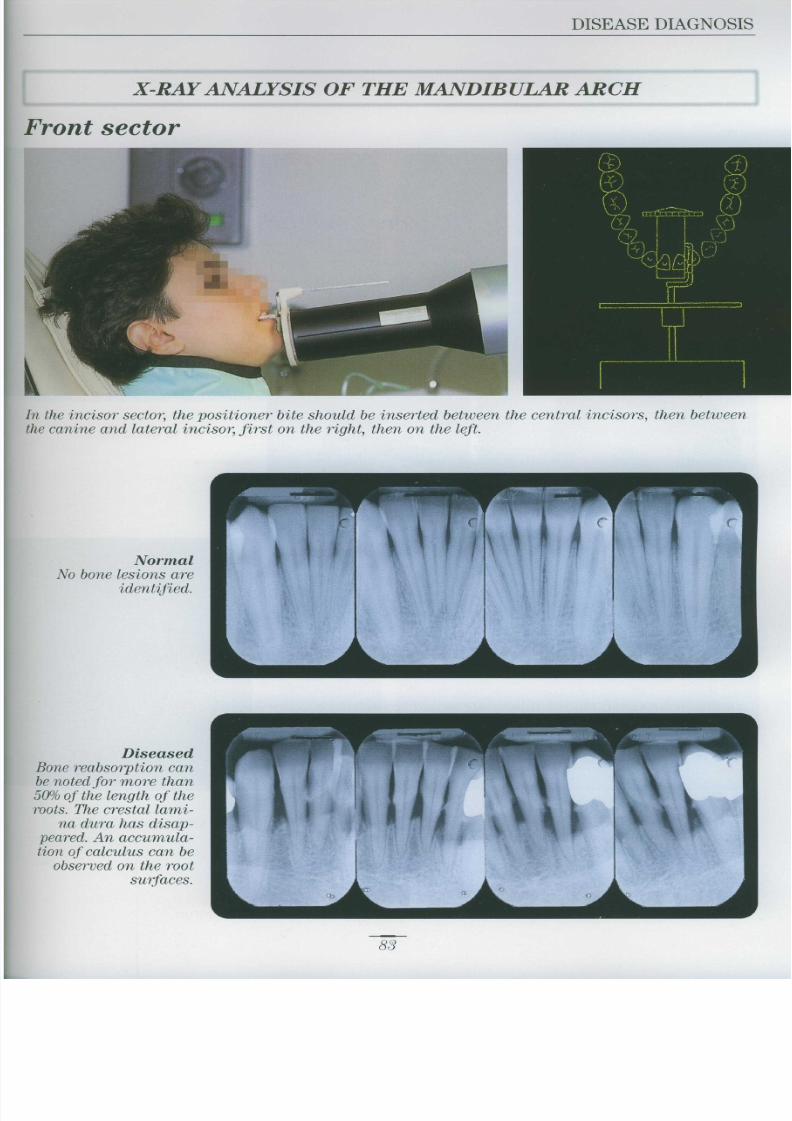
CHAPTER 2
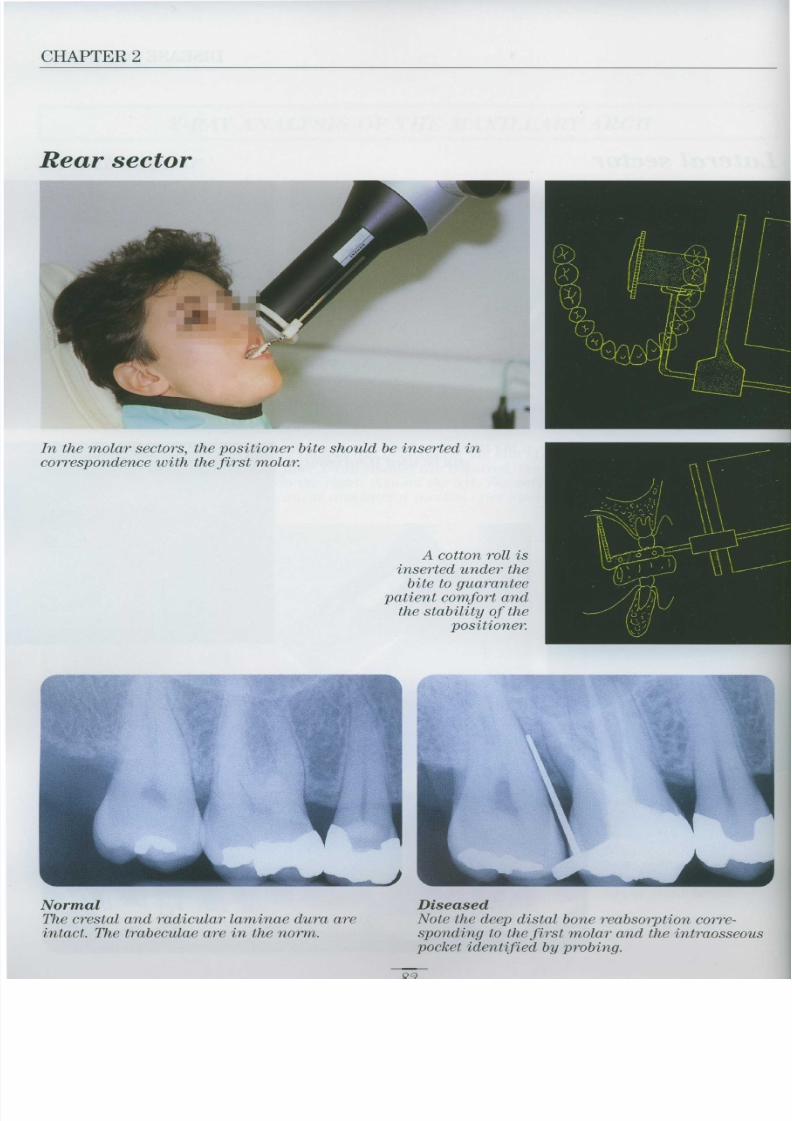
Lateral sector
In the premolar sector, the positioner bite should be inserte dbetween the two premolars, first on the right, then on the left .
In the molar sector, the positioner bite should be inserted between
the two molars, first on the right, then on the left . If a third molar
is present, the bite should be placed on the second molar .
O
84

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 88/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 89/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 90/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 91/333
CHAPTER 2
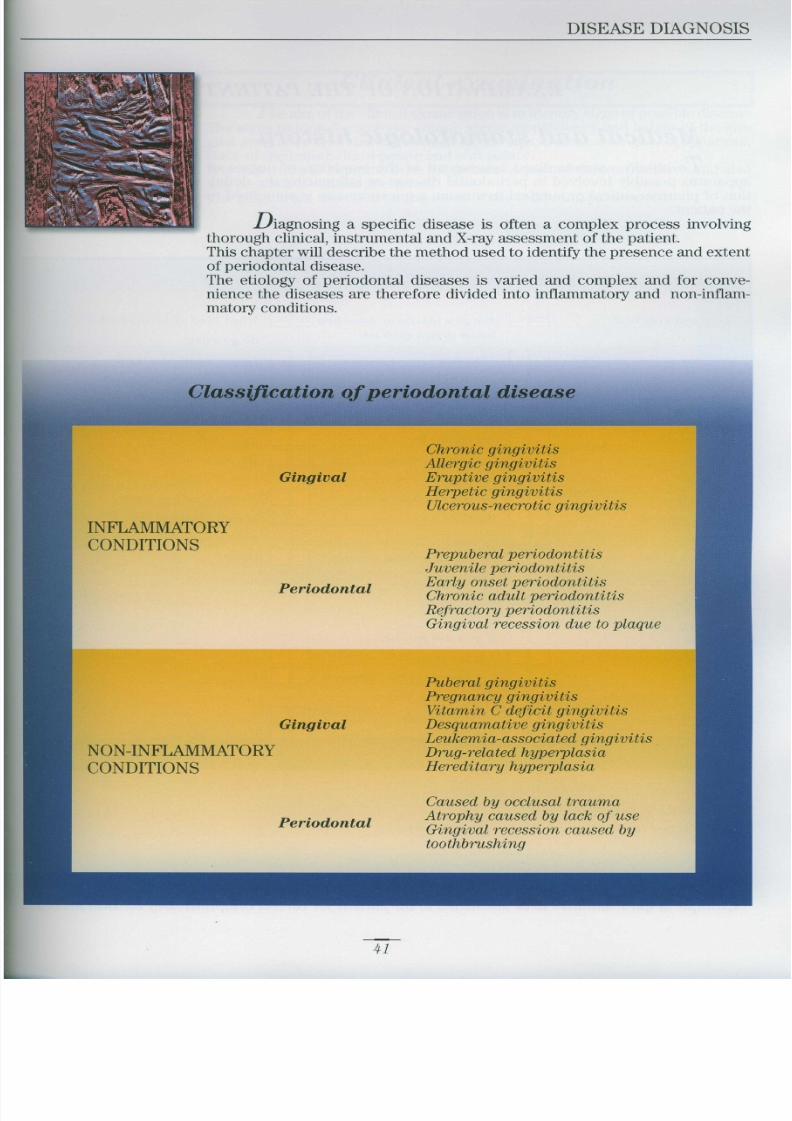
DISEASE DIAGNOSIS
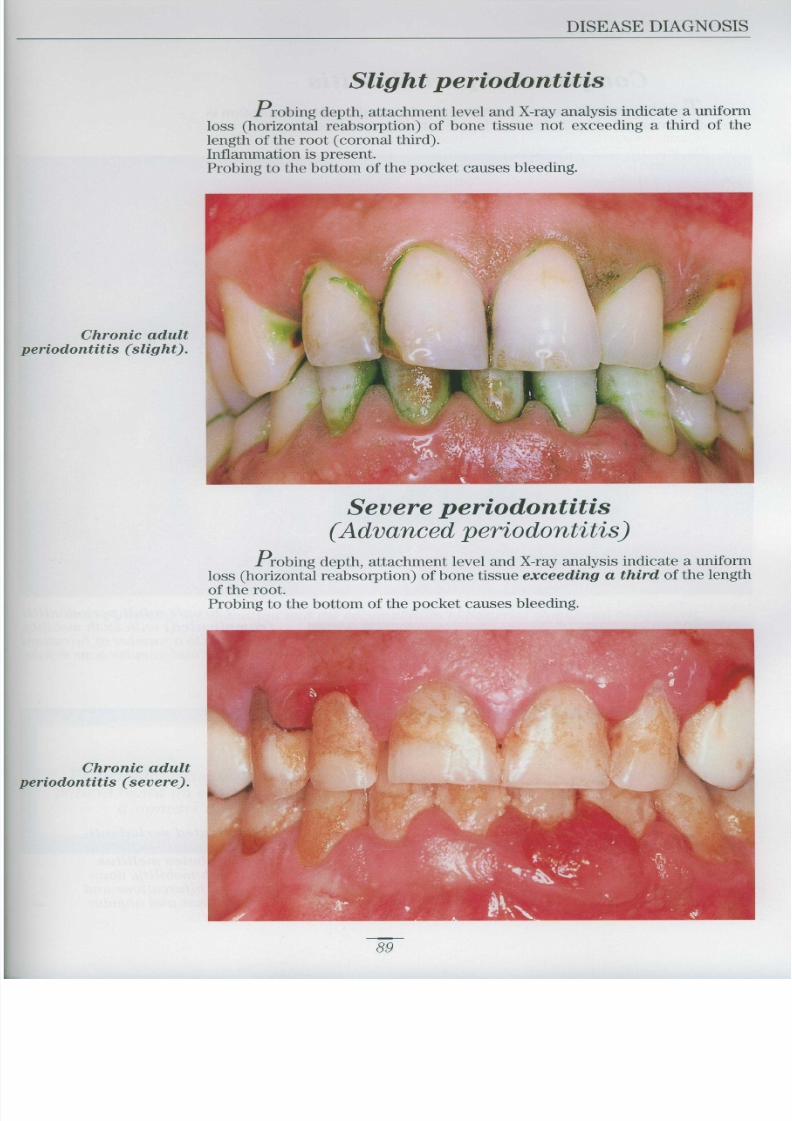
From a clinical point of view, periodontal diseases can be divided int ogingivitis and periodontitis . These are differentiated by loss of connectiv eattachment and bone reabsorption, two phenomena confined to periodontitis classifiable as slight, severe or com plicated according to the degree of dam ag eto anatomical structures
Periodontal diseases
DISEASE 'TYPE LESTnN SYMPTOM S
Inflammatory infiltrate Bleeding on probing
above the transseptal fibres No pocke t
Bone reabsorption limitedSlight to the coronal third of th e
root only
Bone reabsorption Bleeding on probin g
Periodontitis Severe extended beyond the Pocket
coronal third Possible tooth mobility
Angular bone reabsorption
Complicated and 2nd or 3rd degreefurcation involuement
Bleeding on probin g
Possible tooth mobility
Furcation involvement
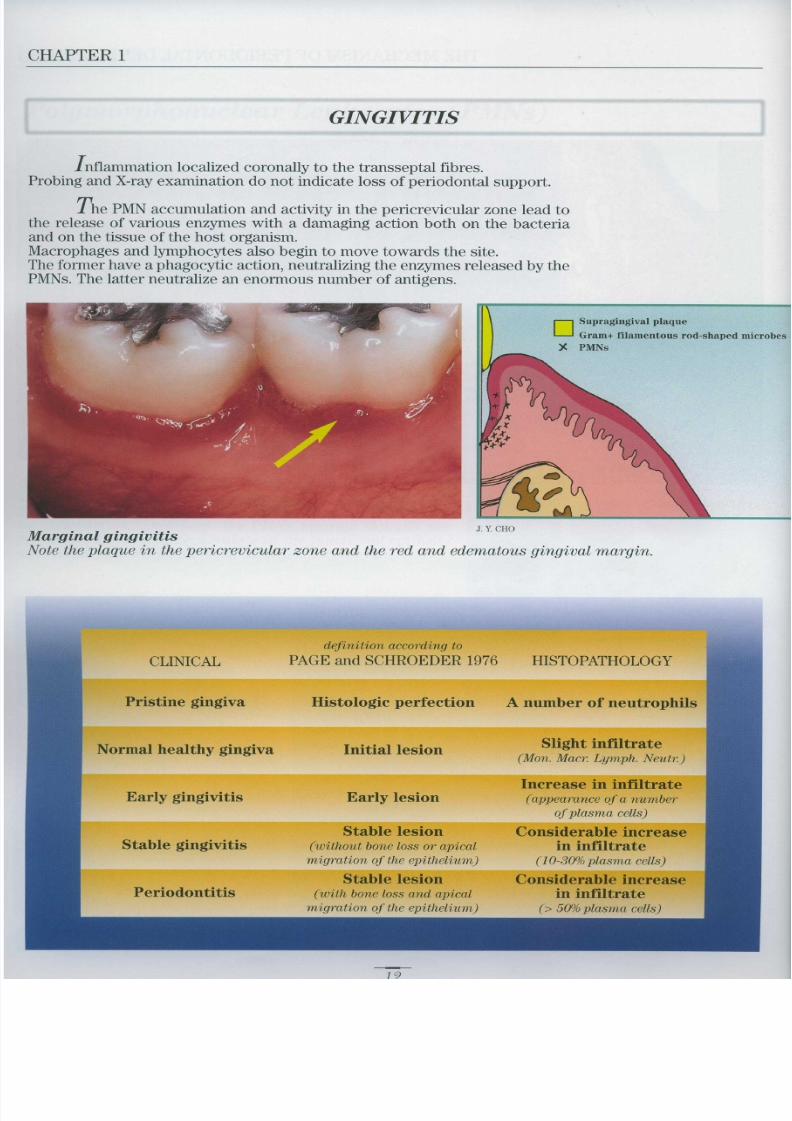
Gingivitis
Shis term is used to describe localized or generalized inflammation o fthe gingiva . The clinical system of this disease is bleeding on probingGingivitis is diagnosed in the absence of a periodontal pocket and when X-ra yexamination does not indicate bone reabsorption Pseudopockets may bepresent
Margina l
gingivitis
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 92/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 93/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 94/333
DISEASE DIAGNOSI S
Severe gingival inflammation and the accumulation of bacterial plaque can be observed .
CONCLUSIONS
Periodontal disease is diagnosed by means of a thorough assessment of th e
patient based on clinical, instrumental and radiographic data . Only a correc t
diagnosis can enable a suitable treatment plan to be drawn up
91

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 95/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 96/333
TREATMENT PLANNIN G
The treatment of a patient with periodontal disease consists of thre e
fundamental phases
1) Complete removal or at least control, of bacterial plaque, the etiologica lagent of the disease
2) Surgical correction of alterations to the soft and hard tissues caused by th e
disease . Restoration of functional form facilitates plaque control an dimproves aesthetics
3 Prevention of possible relapses with a personalized programme of follow -
up appointments
Chronic adult periodontitis .
95

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 97/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 98/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 99/333
CHAPTER 3
Reevaluatio n
A reasonable period of time (possibly several months) after the end o f
initial treatment, the patient undergoes a thorough examination to check th e
state of gingival inflammation which should have disappeared), periodonta lpocket depth and residual tooth mobility. The level of patient cooperation
must also be verified. The examination covers every tooth and the result sdetermine the choice of definitive treatment
Before initia ltreatment
At reevaluation
n

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 100/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 101/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 102/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 103/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 104/333
TREATMENT PLANNIN G
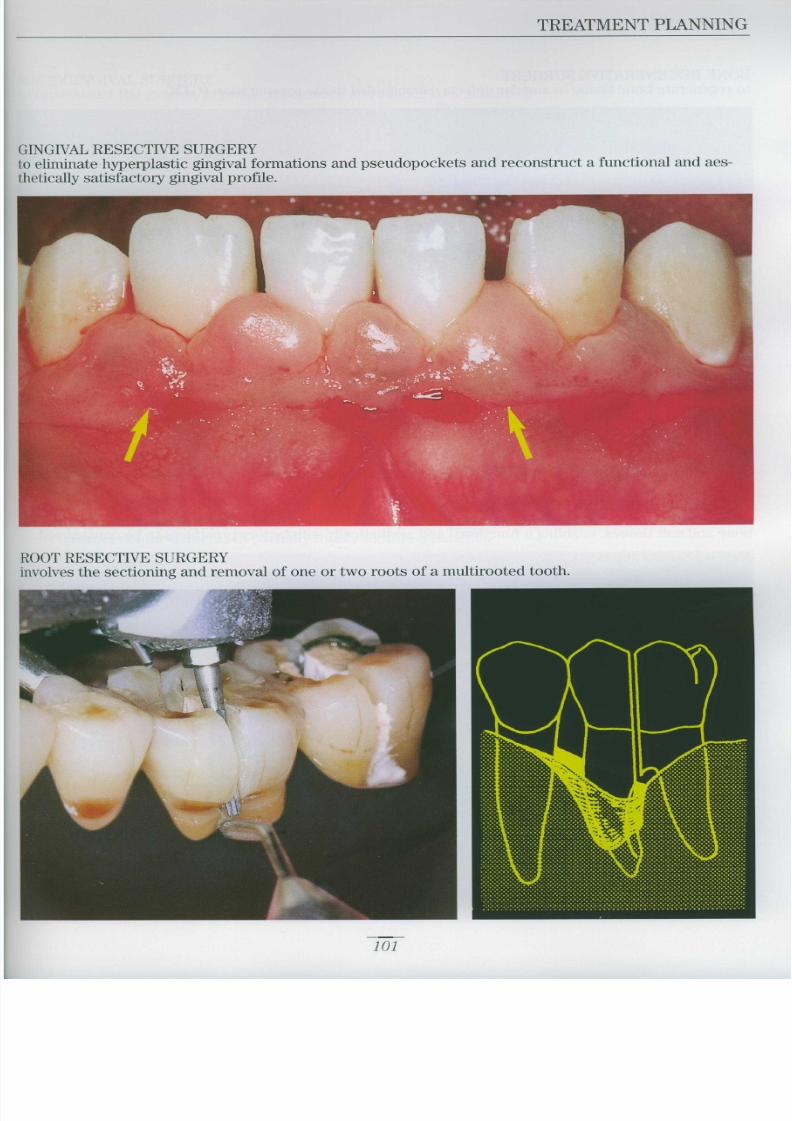
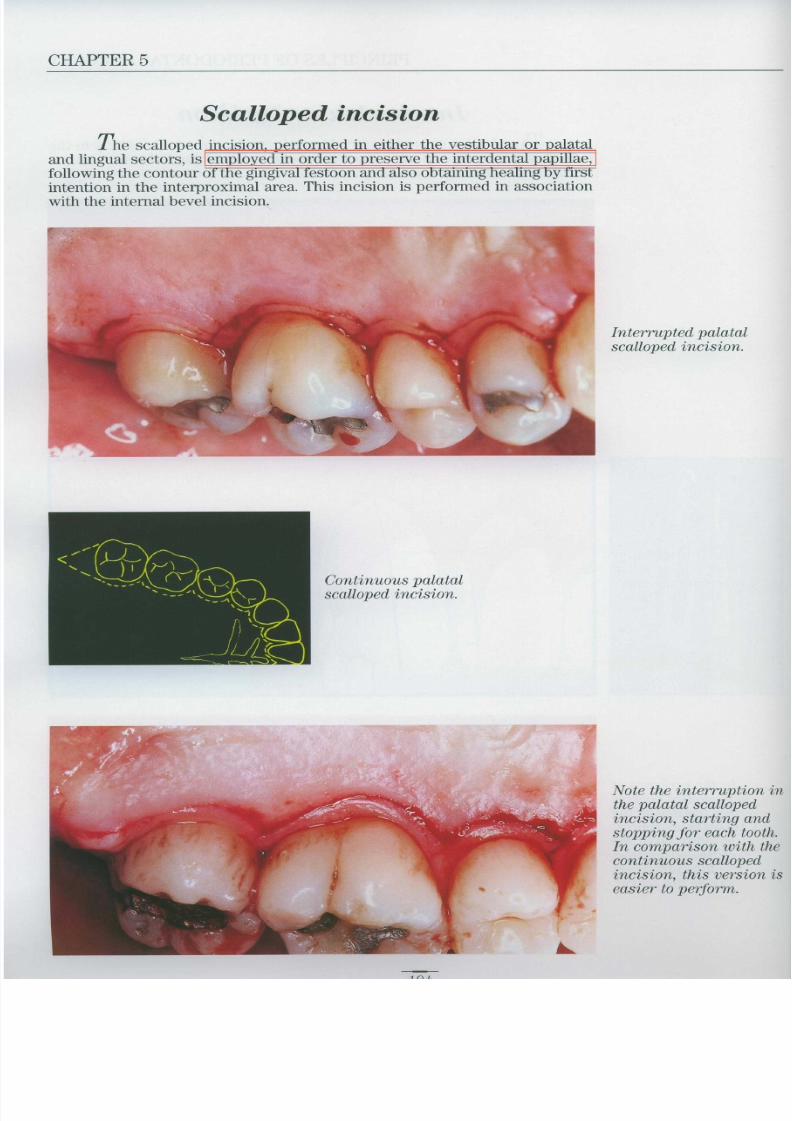
INGIVAL SURGERY
gingiva, improve appearance and reduce root sensitivity .
Y
103

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 105/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 106/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 107/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 108/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 109/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 110/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 111/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 112/333
ORAL HYGIENE REHABILITATIO N
The aim of Oral Hygiene Rehabilitation (OHR) is to eliminate bacteria lplaque infection by rem oving all local irritative stimuli . During this initial phaseof periodontal treatment, the patient must be motivated and instructed in th euse of home oral hygiene instruments . The patient must be made aware of theclose relationship between his or her active participation and the successfu loutcome of the treatment
Oral hygiene instruction
Motivation
Toothbrush (manual, electric, sonic, interdental
Dental floss (floss, tape, super floss
Toothpaste
Antiseptics (chlorhexidroe
Manual instruments (curettes, scalers
I-Iyposonic and ultrasonic instrument s
Rotary instruments
Alternating movement instrument s
113

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 113/333
CHAPTER 4
BACTERIAL PLAQUE CONTROL
Bacterial plaque must be controlled daily (2-3 times) by the patientusing a toothbrush and dental floss .
Toothbrush
None of the toothbrushes currently available on the market is better than th eothers . The best brush is probably the one used with the most effective tech-nique The advantages of electric toothbrushes over normal toothbrushes are con -fined to patients with reduced manual ability. Sonic toothbrushes (Sonicare 0 )supplement the electrical movement with cavitating vibration and a water jet
to facilitate removal of plaque and stains from the supragingival surface of th eteeth .
Conventional toothbrush

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 114/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 115/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 116/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 117/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 118/333
ORAL HYGIENE REHABILITATIO N
INAL GINGIVITI S
y.
LOUR PLAQUE DICLOSING AGEN T
Note the different gradation sof colour:the dark colouring identifiesless recently formed plaque .
N
The same clinical case as i n
the previous image treatedwith single colour plaqu e
detector. Recent plaque canno t
be distinguished from less
recent plaque .
TT
119

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 119/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 120/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 121/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 122/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 123/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 124/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 125/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 126/333
ORAL HYGIENE REHABILITATIO N
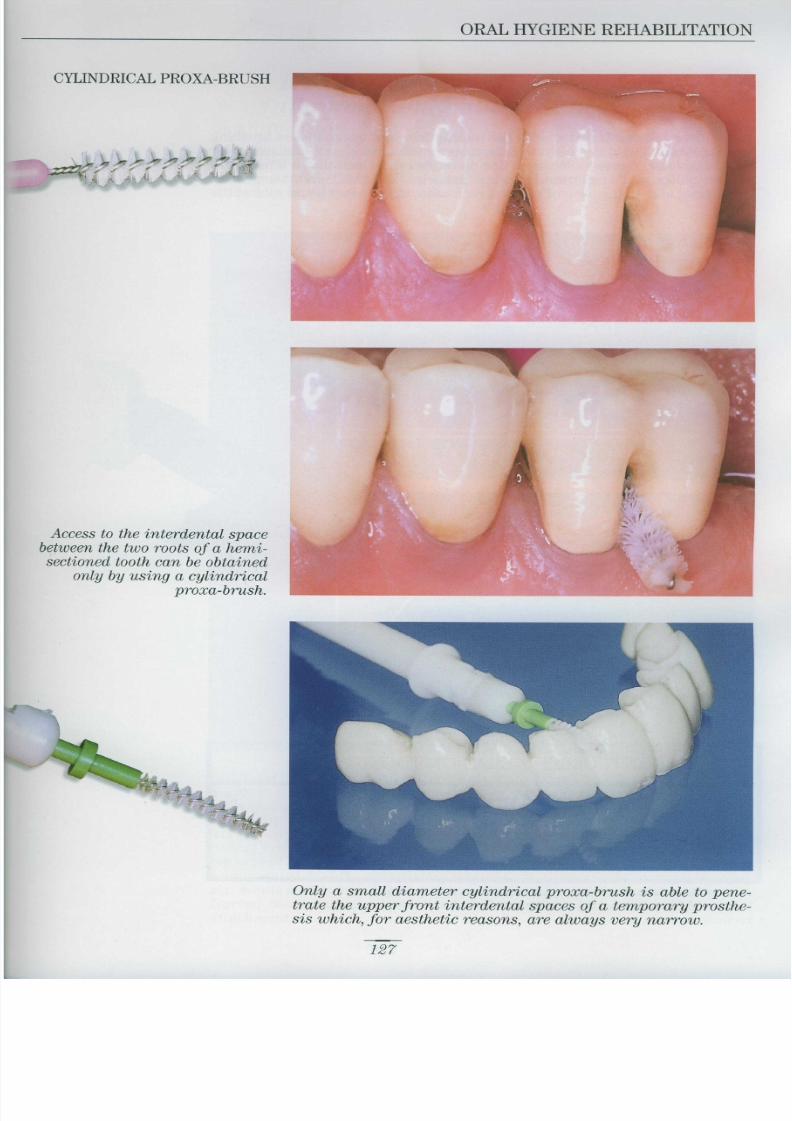
CYLINDRICAL PROXA-BRUS H
Access to the interdental spac ebetween the two roots of a hemi -sectioned tooth can be obtained
only by using a cylindrica l
proxa-brush .
Only a small diameter cylindrical proxa-brush is able to pene-
trate the upper front interdental spaces of a temporary prosthe-
sis which, for aesthetic reasons, are always very narrow
127

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 127/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 128/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 129/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 130/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 131/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 132/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 133/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 134/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 135/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 136/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 137/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 138/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 139/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 140/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 141/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 142/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 143/333
CHAPTER 4
Subgingival scaling and root planing are presented together as they are both performe d
at the same time .Subgingival work must be carefully targeted and performed under local anaestheticfollowing identification of pocket depths and the presence of subgingival deposits .
Subgingival scalingDefinition : removal of all accretions (plaque, calculus) from the sub
gingival surface of the teeth
Subgingival scaling may be performed using manual instruments curettes )and/or mechan ical instruments (sonic/hyposonic)
Note that the subgingival concretion of calculus has bee n
completely removed by the curette
During subgingival scaling, root planing is also completed
Subgingival curetteDeppeler M23 A Tl .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 144/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 145/333
CHAPTER 4
Subgingival scaling
and root planing
technique
Step 1
The pocket is probe d
and the solid concretio n
is identified
Step 2
The curette is reste don the tooth w ith th erounded back toward sthe gingiva .
Step 3
The curette i spushed under th egingiva, delicatel ymoving the gingiva l
tissue
If calculus i sencountered on theroot, the curette is
moved away fro mthe tooth, sh iftin g
the soft tissues unti lthe obstacle i s
passed
1h

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 146/333
ORAL HYGIENE REHABILITATIO N
Step 6When the sensation is of scrapin g
a hard, smooth surface, roo t
planing is complete .
Step 5
The apical-coronal movement o f
the curette is repeated a numbe r
of times to remove the softenedsurface of the root cementum .
Step 4
When the depth of th epocket has been
e
e
root cementum an d
moved with an apical
coronal movement
This operation remove s
the calculus and part o f
the root cementum
147

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 147/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 148/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 149/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 150/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 151/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 152/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 153/333
CHAPTER 4
Antibiotics in Oral Hygiene Rehabilitation
In the majority of cases, mechanical treatment is sufficient to eliminat ethe etiological agent of periodontal disease . In gingivitis, antibiotics are no t
prescribed. In adult periodontitis, mechanical treatment is normally sufficient However, in certain specific situations (progressive adult periodontitis, refrac-tory periodontitis, juvenile periodontitis), topical chemotherapy and topical o rsystemic antibiotics are administered to improve treatment efficacy .
Antibiotics should be prescribed only on completion of mechanical treatment.
Treating periodontal diseases
Mechanical Chemical
treatment treatment
Systemic Loca l
antibiotic antibiotic
treatment treatmen t
Adul t
periodontiti s
Advanced
- Progressive
Amoxycil .+Clay. Ac
Yes Yes Clindamycin Ye s
Ciprofloxaci n
Metronidazole
Yes Metronidazole+Amoxycil Ye s
Amoxycil.+Clay. Ac
C
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 154/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 155/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 156/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 157/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 158/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 159/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 160/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 161/333
CHAPTER 4
CLINICAL CASE 3 - Moderately severe periodontitis
Female patient aged 45
There are 4-5 mm deep periodontal pockets .
The image shows the case a year after completion of OHR. The patien t
refused surgical treatment and was included in a maintenance phasewith follow-up appointments every three months .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 162/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 163/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 164/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 165/333
CHAPTER 4
Step 2/B
Subgingival curette (M23A-TI) : sharpen using the same technique asdescribed for the supragingival curette . This curette has a rounded point
which must be respected during sharpening
Step 3The internal part of these instruments is curved and must therefore b e
finished with a cylindrical ceramic rod or Arkansas stone .
Protected back

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 166/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 167/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 168/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 169/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 170/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 171/333
SURGICAL
TREATMEN T
I CONTROLLABLI
I
YES NO
MAINTENANCE
CHAPTER 5
SURGICAL TREATMEN T
PATIENT SELECTION
FACTOR S
LOCAL BEHAVIOURAL SYSTEMI C
Oral access ComplianceChronic desquamative gingivitis Smokin g
Plaque contro l
The patient has concluded the hygienic phase of periodontal treatment and is ready for the surgical phc

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 172/333
PRINCIPLES OF PERIODONTAL SURGER Y
DECLARATION OF INFORMED CONSEN T
The undersignedconfirms that the following have been clearly explained :
The details of the surgical operation
The reasons for and objectives of the operation
The predictable consequences
The level of risk involved
The probability of success .
The possibility of a subsequent operation .
Possible alternative treatments .
He/she therefore consents to the proposed treatment and any othe r
action which may be held necessary during the operation itself
Date
175

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 173/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 174/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 175/333
CHAPTER 5
LOC L N STH SI
Two types of anaesthesia are used in periodontal surgery.
Infiltration anaesthesia
an anaesthetic solution (with or without adrenaline) is injected into the sof ttissues surrounding the site of the operation . The anaesthetic penetrate sthrough the cribrose structure of the bone tissue
Regional or nerve blocking anaesthesia
anaesthetic is injected near a nerve trunk, preferably near the bone entry o rexit point. In operations involving the lower molar sectors, both the lingua land buccal nerves must often be blocked
Instruments
Cook-Waite syringe
Aspirating syringe fo l
intraoral anaesthesia .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 176/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 177/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 178/333
PRINCIPLES OF PERIODONTAL SURGER Y
Mandibular arch
Lingual nerv e
ar
t
ed
.
181

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 179/333
CHAPTER 5
Blocking the inferior alveolar nerv e
The ramus of the mandible is held in the left hand in such a way tha tthe thumb is in the patient's mouth on the external oblique edge of th e
mandible about 1 cm above the occlusal plane. The syringe is held parallel tothe occlusal plane and brought into the mouth near the premolars of th eopposite side . The needle is inserted in the mucosa of the inner face of th eramus near the thumb of the left hand . The needle touches the bone almos timmediately . The syringe is rotated towards the left, then slowly inserted fo rabout 20 mm . The point of the needle should be near Spix's spine, in othe rwords, the point where the inferior alveolar nerve enters the mandibula rbone After testing aspiration, 2-3 ml of anaesthetic solution are injected This technique often blocks the neighbouring lingual and buccal nerves a swell Inferior alveolar nerve block is indicated for operations involving the mola rsector
Anaesthesia blocking
the inferior alveola rnerve.
Buccal nerve
Inferior alveolar nerve
Lingual nerve
R

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 180/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 181/333
CHAPTER 5
A naesthesia of the m ental foramen
To anaesthetisethe premolar and canine
region, after pulling th echeek aside, the needl eis introduced into th emucosa near the premo-lars. The point is pushe din for about 1 mm, inject-ing 1-2 ml of anaestheti csolution . For a completeeffect, anaesthesia mustalso be performed in thelingual sector
A naesthesia of the incisive nerve
To anaesthetisethe incisor region, a nee-dle is inserted in th eextreme surface of themucosa, injecting sever -
al millilitres of anaes-thetic between the righ tand left mental fora -
mens of the symphysis .The anaesthetic spreadsthrough the osseou spores into the bone tis -
sue as far as the nerve .
Anaesthesia of thi sregion must always b ecompleted by blockingthe mylohyoid nerve .
Infiltration anaesthesiaof the incisive nerve .
1 1

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 182/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 183/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 184/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 185/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 186/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 187/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 188/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 189/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 190/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 191/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 192/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 193/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 194/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 195/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 196/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 197/333
CHAPTER 5
Interproximal incisio n
This incision is performed with an interproximal scalpel (Orban' sscalpel no . 1-2 ; Buck's scalpel no. 5-6) and continues into the interproxima l
spaces to separate the col from the bone tissue. The triangular Buck's scalpe lis used in the narrowest interdental spaces (front sector) . The oval Orban'sscalpel is used in the widest interdental spaces (rear sector)
No . 1-2 Orban's scalpe lNo . 5-6 Buck's scalpe l
After elevating a vestibular flap and a palatal flap, an interproximal inci-
sion is performed on both sides of the col .
onn

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 198/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 199/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 200/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 201/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 202/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 203/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 204/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 205/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 206/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 207/333
CHAPTER 5
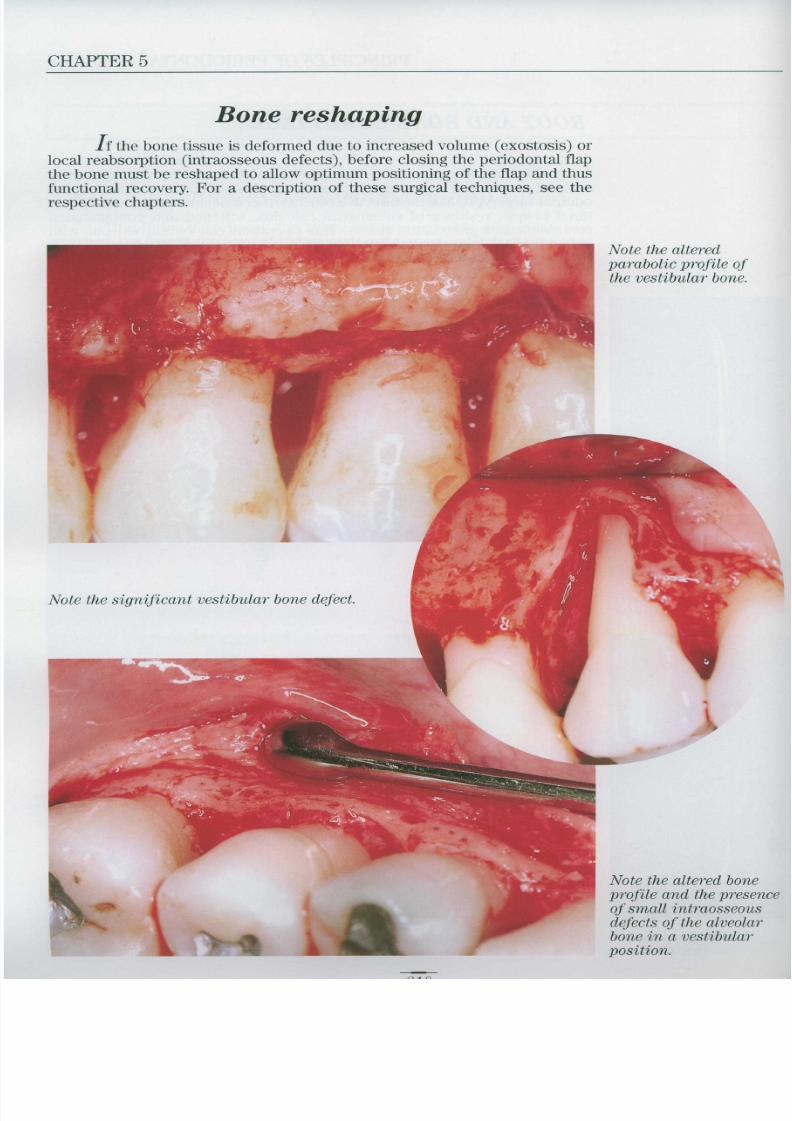
Bone reshaping
If the bone tissue is deformed due to increased volume (exostosis) o rlocal reabsorption (intraosseous defects), before closing the periodontal flap
the bone must be reshaped to allow optimum positioning of the flap and thu sfunctional recovery. For a description of these surgical techniques, see th erespective chapters
Note the alteredparabolic profile of
the vestibular bone .
Note the significant vestibular bone defect .
Note the altered boneprofile and the presence
of small intraosseou s
defects of the alveola r
bone in a vestibular
position .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 208/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 209/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 210/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 211/333
CHAPTER 5
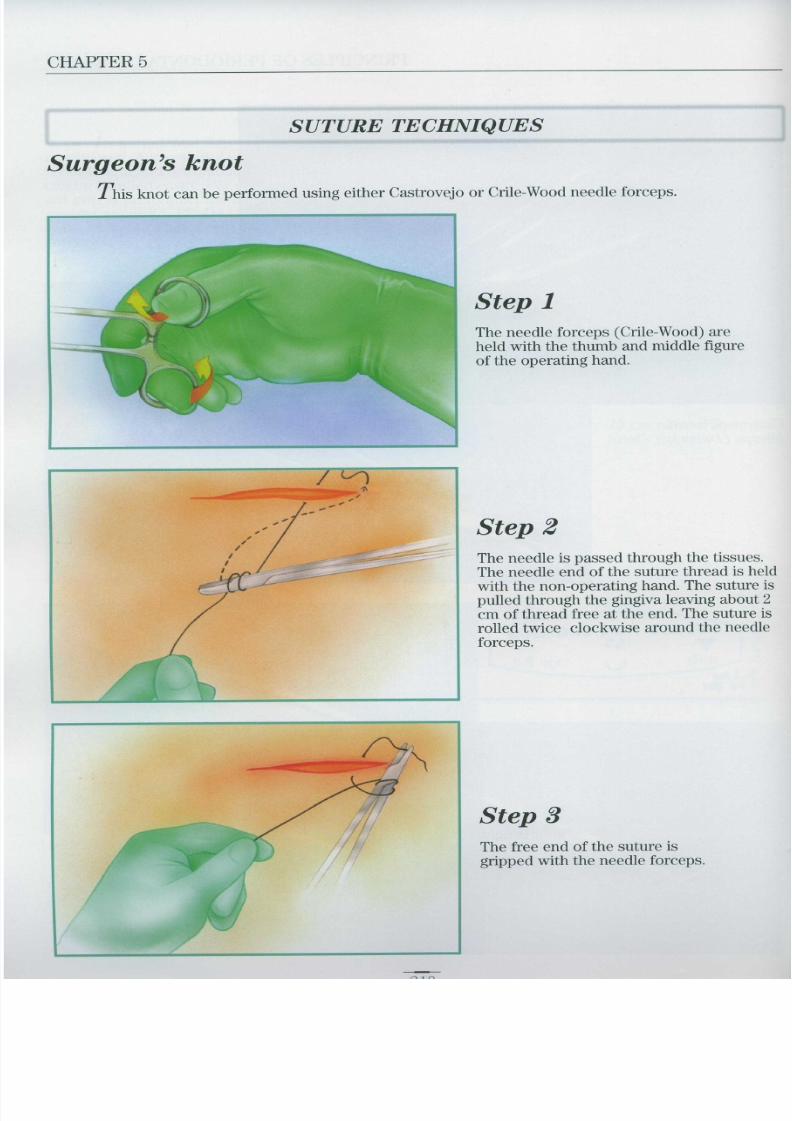
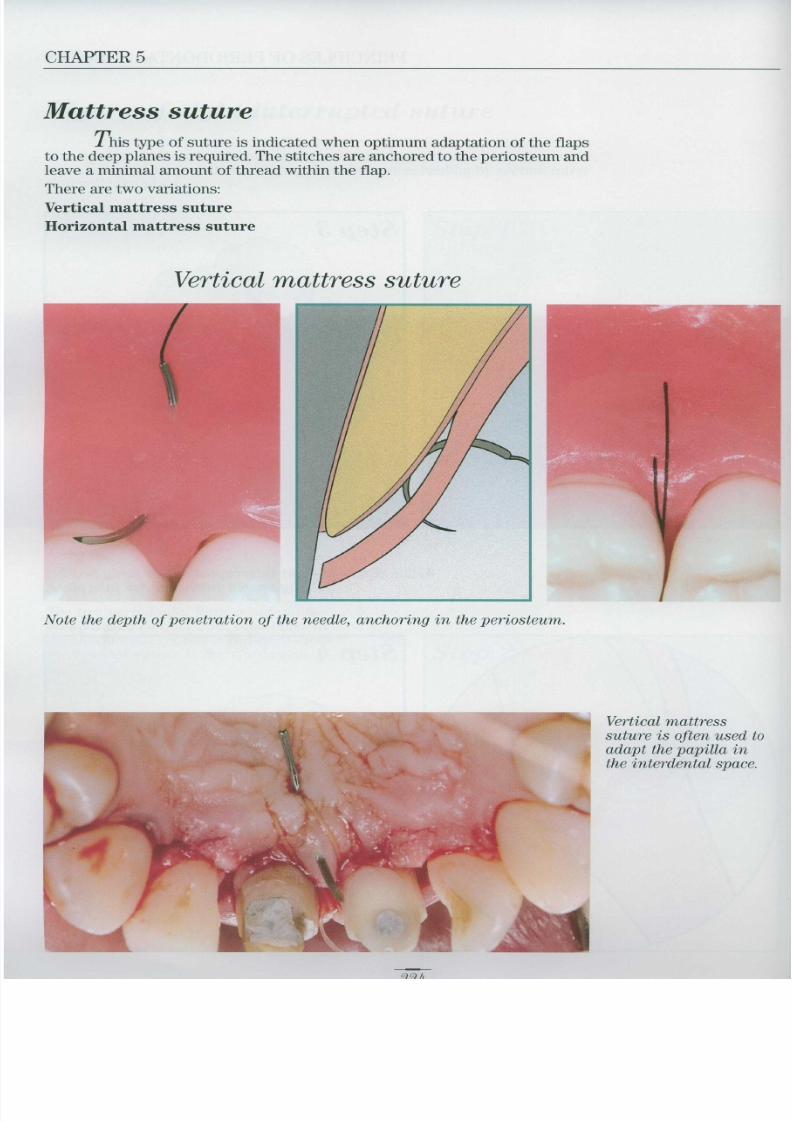
SUTURES
After positioning the flaps as planned, the wound is sutured . Th esutures should always be anchored in keratinized tissue . It is important to pre -vent tension thus avoiding possible localized necrosis and to use a sufficient(but not excessive) number of stitches
Circular 0 interrupted suture in black silk .
MaterialsVarious types of material and suture needles are used in general
surgery, only some of which are used in periodontal surgery
MATERIALS GAUGE NEEDL E
Silk 3 .0 - 4 .0 FS2v
Non- Dacron 5 .0 V5•
absorbable and PTFE (Gore-Tex") 5 .0 RTI6V
Ethibond ® (Exel) 5 .0 DA1 •
Simple catgut 4 .0 - 5 .0 FS2v P V
Chromic catgut 4 .0 FS2 V
Absorbable Polyglycolic acid (Dexon') 4 .0 - 5 .0 - 6 .0 T5• PRE2V CE2 v
Polyglactin (Vicryl ® ) 4 .0 FS2v
Poliglecaprone (Monocryl ® 5 .0 - 6 .0 DA10- P3v
• TAPERCUT NEEDLES v REVERSE CUTTING NEEDLES

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 212/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 213/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 214/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 215/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 216/333
PRINCIPLES OF PERIODONTAL SURGER Y
Step 4
The free end of the suture is pulle dwith the needle forceps
Step 5
The thread is rolled around the needl eforceps again in an anticlockwise
direction (opposite direction to step 2) The end of the thread is gripped with
the needle forceps
Step 6
The free end of the thread is pulled ,
keeping the needle forceps stationary until the second part of the surgeon' s
knot is tight.
219

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 217/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 218/333
PRINCIPLES OF PERIODONTAL SURGER Y
The circular interrupted suture will enable healing by first intention .
ep 3
221

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 219/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 220/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 221/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 222/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 223/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 224/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 225/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 226/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 227/333
CHAPTER 5
Continuous spiral suture
The spiral suture is used in apicectomies, in pre-prosthetic surgery, t osuture long incisions in edentulous crest, or in mucogingival surgery to suturethe site where the connective tissue graft has been taken from the palate. It i seasy and very quick to perform
Step 1The suture begins at one end of theincision with a circular stitch ,
performing a surgeon's knot .
Step 2It continues by passing the needleand thread about 3 mm away fro mthe first stitch . The needle re-emerge s
in a direction perpendicular to thesurgical wound
9 9n

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 228/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 229/333
CHAPTER 5
ontinuous blocked sutureThe indications for this type of suture are the same as for the continuou s
spiral suture . It is more demanding, but also more stable than the previous version
Step 1-2-3The first two steps are identical to thecontinuous spiral suture . The needle i sthen passed under the thread to block i tbefore performing another stitch about 3mm away from the first
Step 4-5The suture is continued, keeping th eend under tension . When the end of th eincision is reached, a surgeon's knot is
performed with the end of the threadand a slip knot with the last loop whic his not tightened

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 230/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 231/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 232/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 233/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 234/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 235/333
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 236/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 237/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 238/333
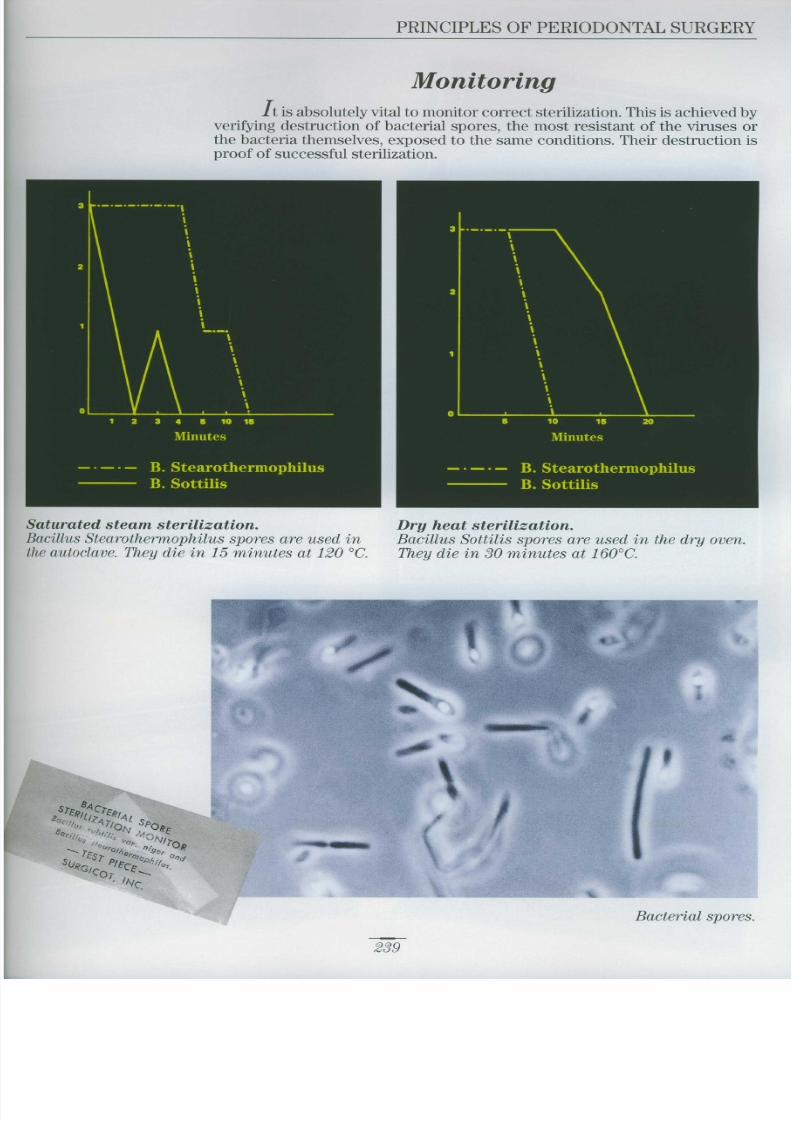
PRINCIPLES OF PERIODONTAL SURGER Y
L
L
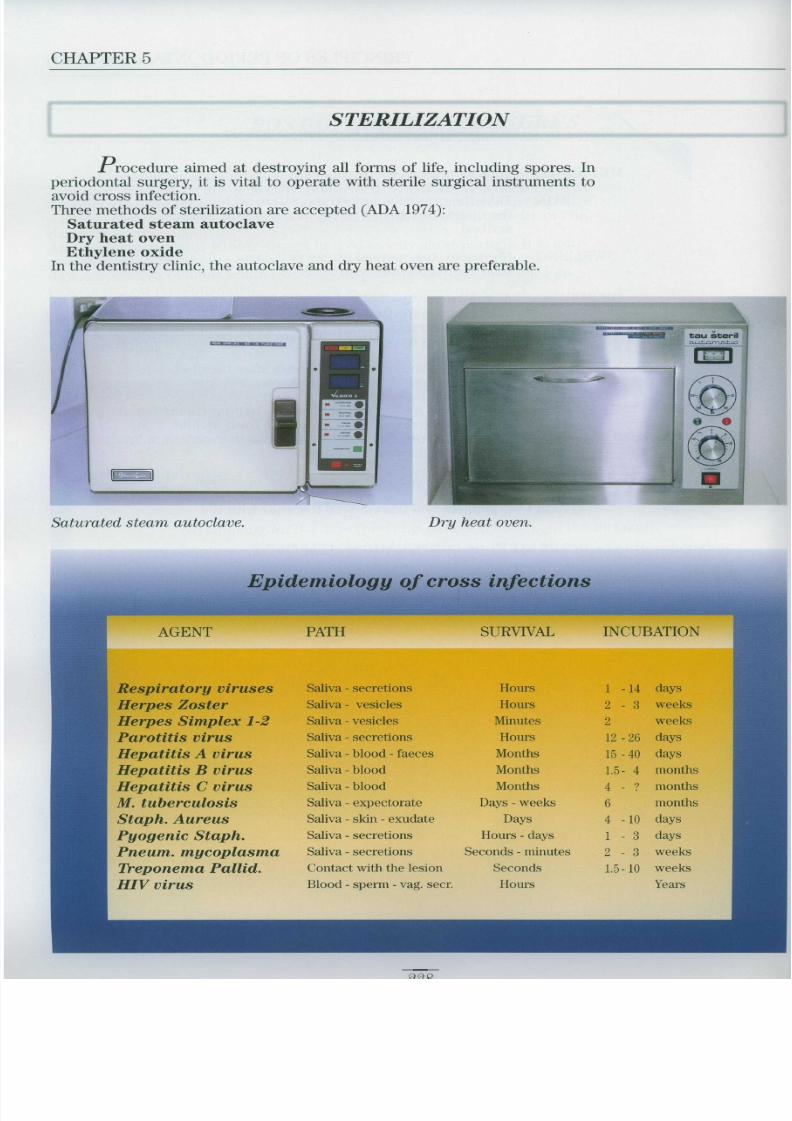
Monitoring with spores
241

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 239/333
Chapter 6
Per iodontal Flap
Surgery

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 240/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 241/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 242/333
PERIODONTAL FLAP SURGERY
Surgical instrumentsInstruments employed in periodontal flap surgery include :
Double-sided mirror to imp rove visibility CP12 graduated periodontal probe for measuring and probing
Straight round scalpel for incisions
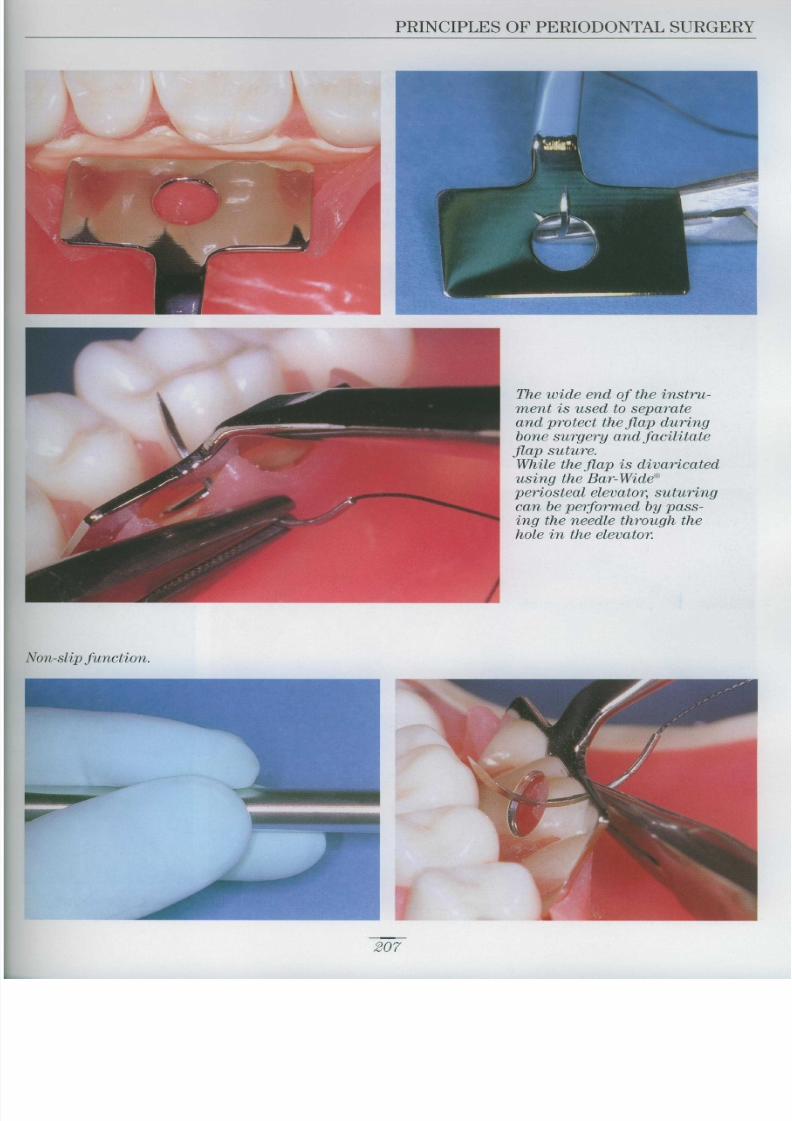
Bartolucci periosteal elevator Bar-Wide)
No 1/2 Orban interproximal scalpel for interproximal incisions
Universal curett e
to remove pieces of tissue and for the curettage of bone defects and roots
No . 36/37 Rodhes chisel
useful in bone surgery, the distal wedge procedure and to remove th e
periosteum
H3 curved Cocker Mosquito to remove pieces of tissue
Crile-Wood needle forceps 15 cm) for suturing
Dean scissors to cut the suture threads
Cook-Waite syringe for anaesthesia
Columbia retractors to retract cheek and lip
LaGrange scissors to finish the flaps
247

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 243/333
CHAPTER 6
A) Access flapDescribed for the first time by Kirkland in 1931, this flap is easy to per -
form . The aim is to obtain full access to root surfaces in order to complet e
mechanical treatment and perform any chemical treatment necessary
Indications :Indicated in chronic adult periodontitis to complete root planing and reducepocket depth
mwmmfwtmmwwmr
Surgical techniqu e
Step 1 : Incision, flap elevatio nand curettag e
The incision is performed vestibularly and palatally directly in the bot -tom of the pocket . The flaps are raised using a periosteal elevator, exposing
the bone and root surfaces which undergo thorough curettage
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 244/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 245/333
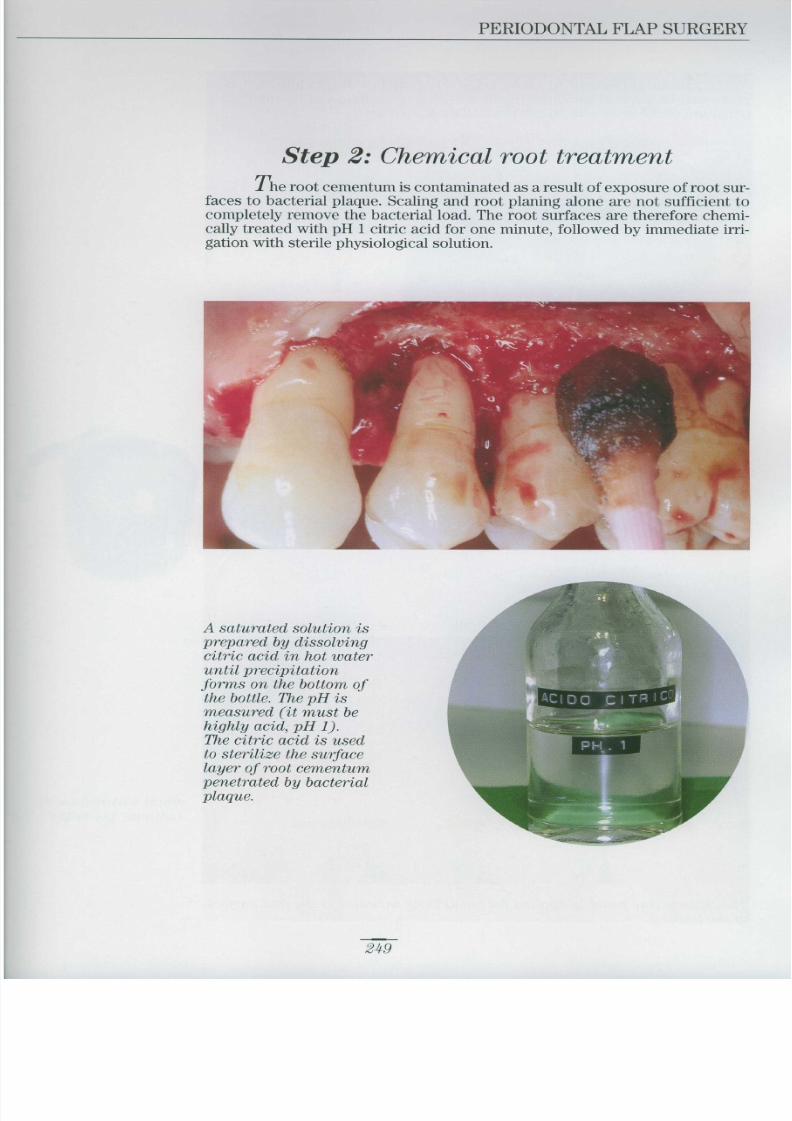
CHAPTER 6
As an alternative to citric acid, a tetracycline hydrochloride basedpaste can be applied for three minutes (Terranova), followed by immediat eirrigation of the area with sterile physiological solution
The tetracycline paste is applied for about three minutes to the root surfac e
of the teeth.
A capsule of Ambramycin ® is opene din a dappen and the contents ar e
diluted with sterile physiologica l
solution until a stiff paste i sobtained .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 246/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 247/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 248/333
PERIODONTAL FLAP SURGERY
Surgical technique
Step : Incisions
After administering local anaesthesia with an anaesthetic containin g:100,000), the incisions are performed using a Ba rd-Parker blad eo . 15) .
N
The first incision is made about 1 mm from the margin of the fre erallel to the longitudinal axis of the tooth
253

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 249/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 250/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 251/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 252/333
PERIODONTAL FLAP SURGERY
Step 4: Suture
. At the end of the surgical operation, the palatal and vestibular flaps arerepositioned and sutured in the pre-operative site . The suture is performe dwith silk thread or simple catgut .
Step 5: Periodontal pack
A pack is not required with the Widman flap, but if used, it should b eremoved after 3-4 days .
Post-operative image (after six months) .The incision performed several millimetres from the gingival margi n
has altered the final aesthetic result . Where aesthetics are a priority, th e
operation can be varied, making the first incision directly in the crevic-ular sulcus
257

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 253/333
CHAPTER 6
INTRACREVICULAR INCISIO N
Where aesthetics are a priority, the first incision is performed directlyin the crevicular sulcus as far as the osseous crest.
Post-operative image(after one month) .The final aesthetic result
is clearly better after an
intracrevicular incisio n
than after a margina lincision

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 254/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 255/333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 256/333
PERIODONTAL FLAP SURGERY
Elevating the flap :the flap is raised using a Pritchard periosteal elevator ; avoiding going beyond the mucogingiva ljunction. Root and bone curettage is carried out without reshaping the bone .
Suture :the vestibular and palatal flaps are repositioned in their pre-operative site and sutured with 4-0 blac k
silk and an FS2 needle using interrupted circular stitches .
261

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 257/333
CHAPTER 6
Post-operative phase : the case six months after the operation .Note the excellent healing and aesthetics
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 258/333
PERIODONTAL FLAP SURGERY
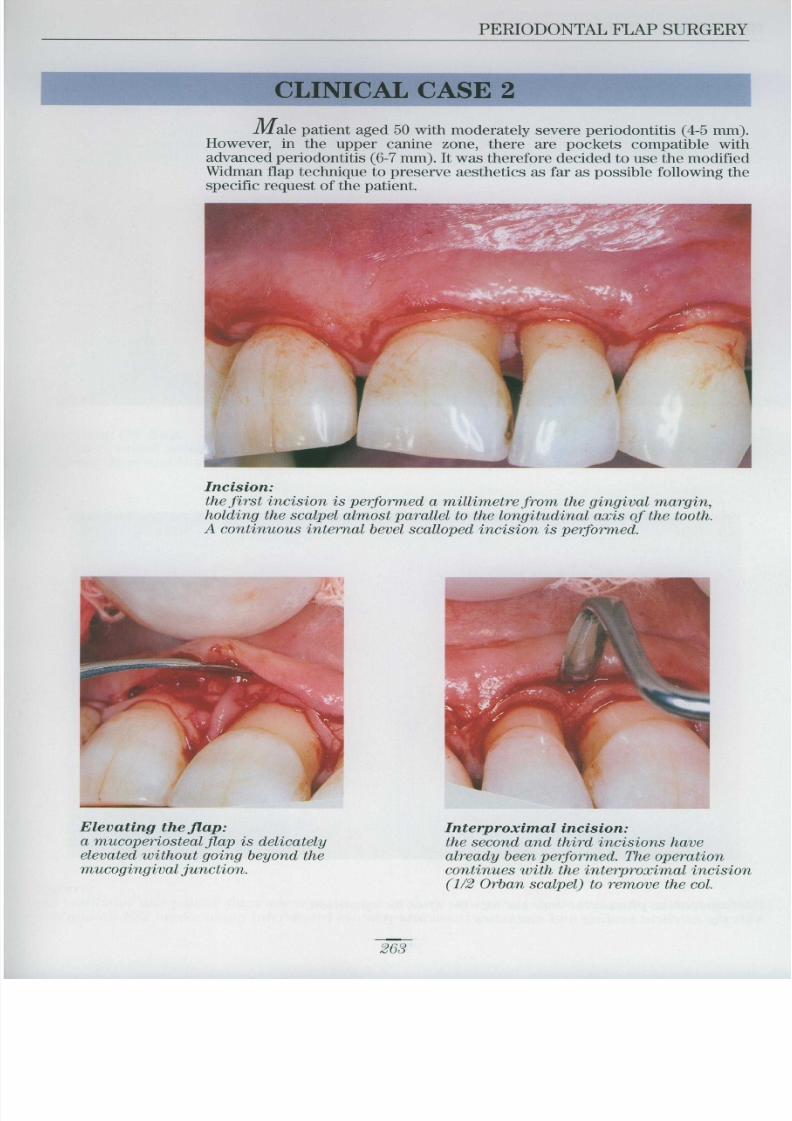
CLINICAL CASE 2
Male patient aged 50 with moderately severe periodontitis (4-5 mm) However, in the upper canine zone, there are pockets compatible wit hadvanced periodontitis (6-7 mm) . It was therefore decided to use the modifie d
Widman flap technique to preserve aesthetics as far as possible following th especific request of the patient .
Incision :the first incision is performed a millimetre from the gingival margin
holding the scalpel almost parallel to the longitudinal axis of the tooth .A continuous internal bevel scalloped incision is performed .
Interproximal incision :the second and third incisions hav ealready been performed. The operation
continues with the interproximal incision 1/2 Orban scalpel) to remove the col .
Elevating the flap :a mucoperiosteal flap is delicatel yelevated without going beyond themucogingival junction .
263

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 259/333
CHAPTER 6
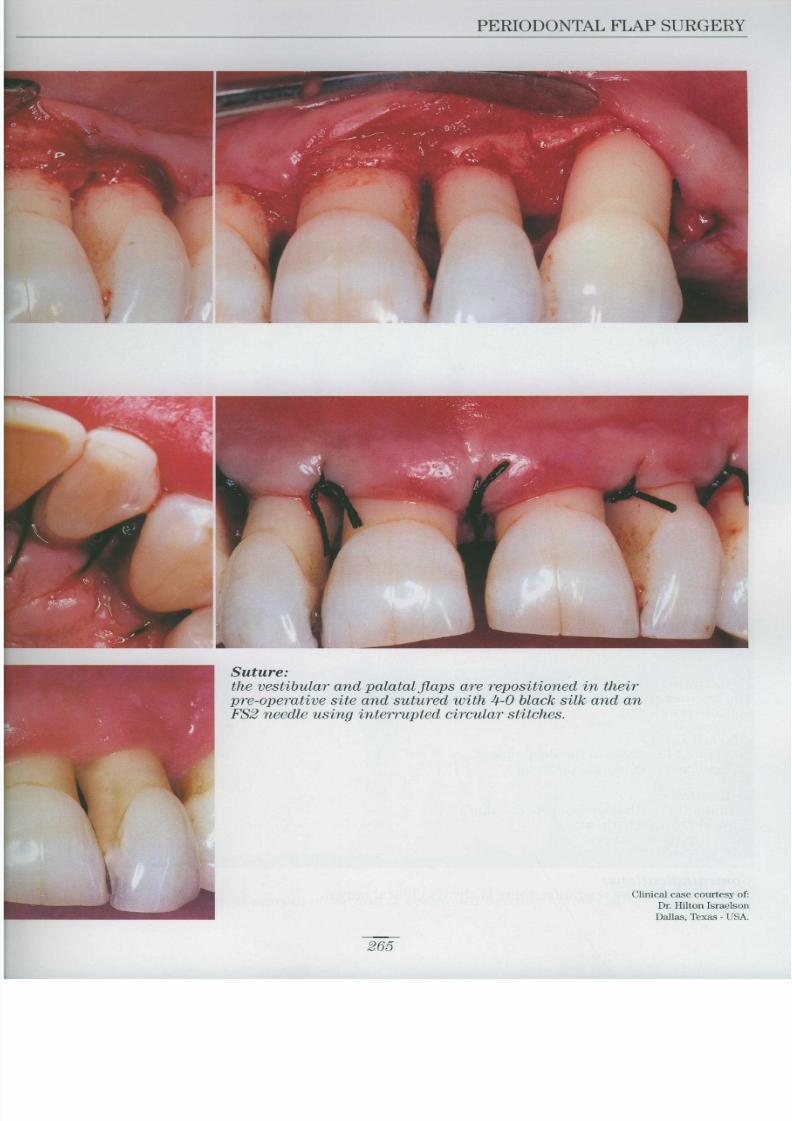
When the flap has been elevated, it can be seen that the vestibular sectors of the incisors are free fro m
bone reabsorption. However, in the vestibular sectors of the canines, there are small bone defects .Thorough curettage of these defects is performed, but without bone reshaping .
Post-operative phase :the case six months after the operation .
F
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 260/333
PERIODONTAL FLAP SURGERY
Suture
the vestibular and palatal flaps are repositioned in thei rpre-operative site and sutured with 4-0 black silk and a n
FS2 needle using interrupted circular stitches
Clinical case courtesy of :
Dr. llilton Israelson
Dallas, Texas - USA
265

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 261/333
CHAPTER 6
C Apically positioned flap
This flap was described for the first time by Nabers in 1954 . Later, i n1962, Friedmann called it the Apically Repositioned Flap , thus emphasisin g
the fact that the keratinized gingiva alveolar mucosa is moved in an apica ldirection after bone surgery. We will name this flap apically positioned because the gingival tissues are moved in a new position
An internal bevel incision is performed, the secondary flap is removed an dthe full thickness primary flap is elevated beyond the mucogingival junctio nand positioned apically to cover the osseous crest
Definition :
Mucoperiosteal flap, elevated beyond the mucogingival line an dapically positioned .
Objectives :To obtain full access to the deep planes To eradicate periodontal pockets .
Indications :Periodontitis with deep pockets (>6 mm)
Clinical crown lengthening
Resective bone surgery .
Pre-prosthetic bone surgery
Contraindications :
Aesthetic - after the operation, there is always clinical crownlengthening .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 262/333
PERIODONTAL FLAP SURGERY
phasepositioned at the cemento-enamel junction .
phasee
.
267

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 263/333
CHAPTER 6
Surgical technique
Pre-hygienic phas e
Note the edematous and reddenedgingival tissues
Post-hygienic phas e
At the end of the hygienic phase the edema and reddening of th e
gingiva have disappeared .The patient is being treated wit h0 .2% chlorhexidine .
Step 1Incision
An internal bevel sca lloped incisio nis performed at the gingival margin It is then deepened as far as th eosseous crest

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 264/333
PERIODONTAL FLAP SURGERY
Step 2Elevating the flap
Once the secondary flap and co lhave been removed, a mucope -
riosteal flap is elevated beyo nd th emucogingival junction to expos ethe osseous crest and any bon e
. If necessary, resec -tive bone surgery is performed
Step 3Suture
The vestibular and lingual flap sare positioned apically and
sutured to cover the osseous crestwith 4-0 black silk sutures and a n
FS2 needle
Step 4Stabilization
In the event of massive bonereabsorption with reversal of th ecrown/root ratio causing perma -
nent tooth mobility, stabilizatio nmay be indicated .
269

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 265/333
CHAPTER 6
CLINICAL CASE 1
Female patient aged 46 with advanced chronic periodontitis . Periodontal pockets, an average of 6-7 m m
deep, are present . At the end of the hygienic phase, a surgical operation is performed to eradicate th epockets
Pre-osseou s
Note the predominantly horizontal bone reabsorption .
Suture :the flaps are sutured a t
the osseous crest using asimple catgut suture .
Post-surgical phase :

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 266/333
PERIODONTAL FLAP SURGERY
. Conservative resective bon eavoid impairing the stability of the teeth which already have a reverse d
Post-osseous
Note the conservative nature of the bone resection to avoid worsening th ecrown/root ratio .
Suture :the flaps are sutured at theosseous crest using simpl e
catgut suture
.271
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 267/333
CHAPTER 6
CLINICAL CASE 2
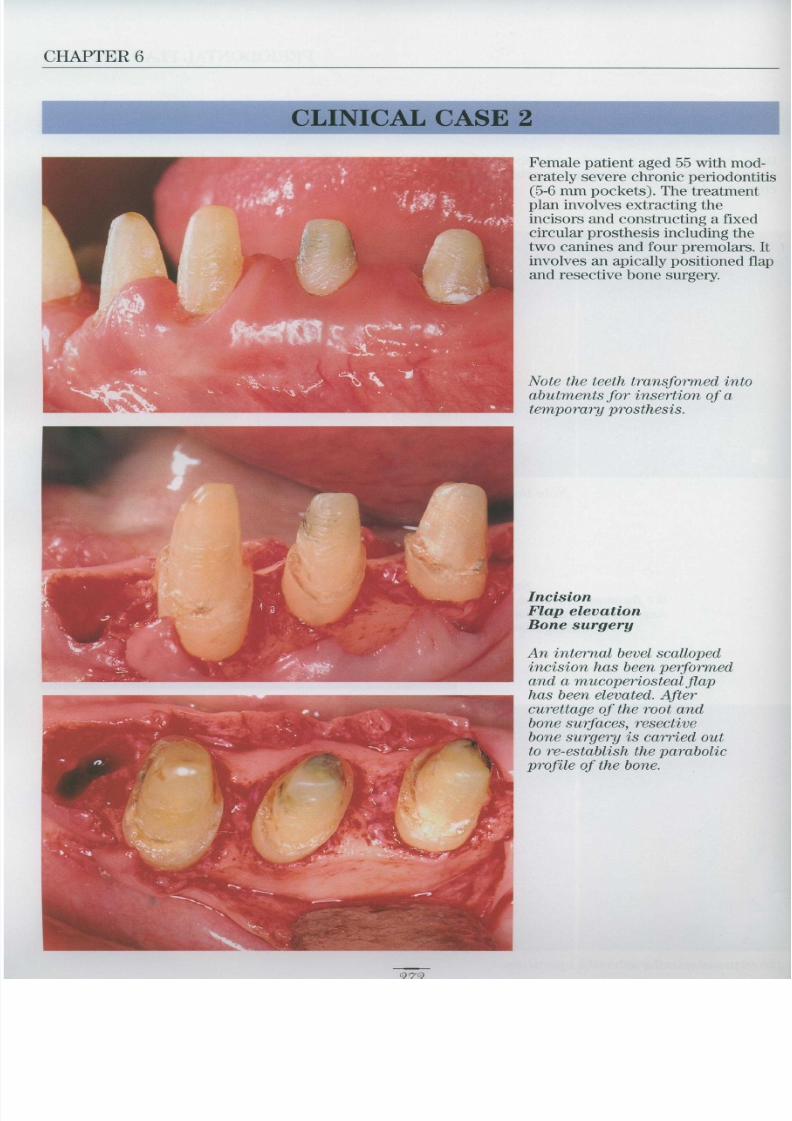
Female patient aged 55 with mod-erately severe chronic periodontiti s(5-6 mm pockets) . The treatmentplan involves extracting th eincisors and constructing a fixe dcircular prosthesis including th etwo canines and four premolars . Itinvolves an apically positioned flapand resective bone surgery.
Note the teeth transformed into
abutments for insertion of atemporary prosthesis .
IncisionFlap elevationBone surgery
An internal bevel scallope dincision has been performe dand a mucoperiosteal flap
has been elevated . Aftercurettage of the root an dbone surfaces, resective
bone surgery is carried ou t
to re-establish the paraboli cprofile of the bone.

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 268/333
PERIODONTAL FLAP SURGERY
Suture :
the flaps are positioned apically
and sutured at the crest with
dcircular stitches. Post-operativeimage on removal of the suture s
(12 days) .
Post-operative phase :
the case a month after th e
operation
The case three months after th e
operation with the temporary. The tissues are
mature and the case is ready fo r
preparation of the definitiv e
prosthesis .
273
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 269/333
CHAPTER 6
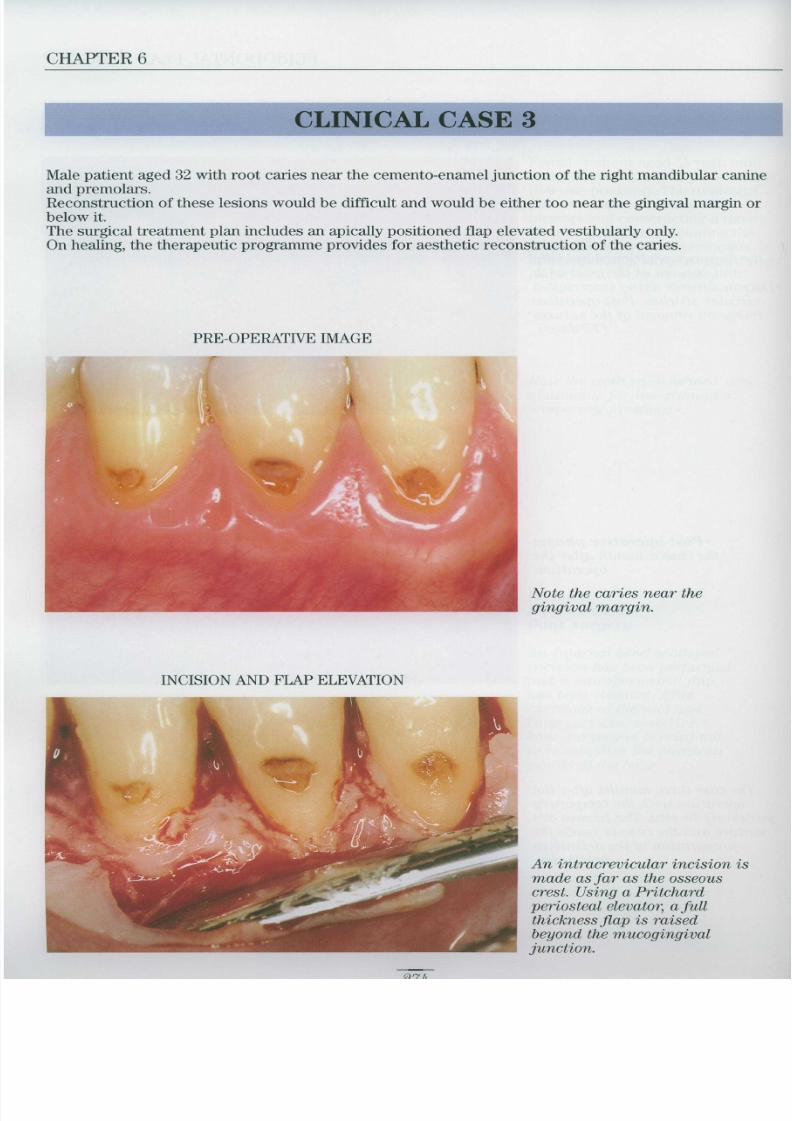
CLINICAL CASE 3
Male patient aged 32 with root caries near the cemento-enamel junction of the right mandibular canin eand premolars Reconstruction of these lesions would be difficult and would be either too near the gingival margin o rbelow it The surgical treatment plan includes an apically positioned flap elevated vestibularly only On healing, the therapeutic programme provides for aesthetic reconstruction of the caries
PRE-OPERATIVE IMAGE
Note the caries near thegingival margin
INCISION AND FLAP ELEVATION
An intracrevicular incision i smade as far as the osseous
crest . Using a Pritchardperiosteal elevator, a ful l
thickness flap is raisedbeyond the mucogingiva ljunction .
9 7 h

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 270/333
PERIODONTAL FLAP SURGERY
BONE SURGERY
Modest ostectomy and osteoplasty are performed, moving th e
bone margin vestibular to the caries apically by about 1-2 mm .
The dentine and softened cementum are removed and a tempo-
rary filling is performed .
POST-OPERATIVE IMAG E
The case three months after the operation. Note the perfectly
healed gingival tissue positioned apically to the caries .The case is ready for cosmetic reconstruction .
275

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 271/333
CHAPTER 6
D) Palatal FlapWhen an apically positioned flap is performed in the vestibular sec -
tion, once elevated beyond the m ucogingival junction, the tissue can usua lly b e
moved without difficulty. However, in the palatal sector where the flap con-sists exclusively of connective tissue, the lack of elasticity prevents it bein gapically positioned .
Definition :
The term palatal flap describes a particular surgical technique enabling th epalatal connective tissue to be incised, elevated, thinned and positione dapically .
Objectives :
To provide access to the root and bone surfaces.To obtain apical mobility of the palatal flap .
Indications :
Periodontitis Clinical crown lengthening
Resective bone surgery .
Pre-prosthetic surgery
Contraindications:
Too narrow and/or low a palate would make thinning of the flap difficult Care must be taken to avoid damaging the palatine artery.

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 272/333
PERIODONTAL FLAP SURGERY
Multiple bone reabsorption in the palatal secto r
CLINICAL CASE 1
In this clinical case i t
was necessary to posi -tion the vestibular and
palatal flaps apicallyfor prosthetic reasons
Note the short clinica lcrowns . With apicallypositioned flaps and
resective bone surgery
the clinical crowns are
engthened and prosthe -sis retention is thus
improved
PRE-OPERATIVE IMAGES
277

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 273/333
CHAPTER 6
Step 1 Intracrevicular incisio nThis is performed with a no . 15 Bard-Parker blade inserted directl yinto the crevicular sulcus as far as the osseous crest
Step 2: Flap elevation
A mucoperiosteal flap is elevated using a Pritchard periosteal elevator After exposing the bone tissue (for possible bone surgery) the length of the flap is measured .
Step 3 Paramarginal incision
An internal bevel incision is performed at a distance from th e
gingival margin determined by the need or otherwise t oshorten the flap
Step 4 : Thinning the f lap
If necessary, the flap is further thinned using a new blade
Step 5 S uturing the f lap
The flap is closed, covering the osseous crest, with acontinuous suspended suture or vertical/horizonta lmattress suture
Surgical technique
9 7

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 274/333
PERIODONTAL FLAP SURGERY
Note the intracrevicular andparamarginal incisions .
The incisions are also extended t othe retromolar region and th e
mesial edentulous ridge .
After removal of the secondary
flap and further thinning of th eprimary flap, the latter i s
positioned at the osseous cres t
(resective bone surgery is
performed) and sutured with
sand horizontal mattress stitches .he margins of the flap positioned
in correspondence with theedentulous ridge are sutured wit h
interrupted circular stitches .
After the operation, the clinica l. In this typ e
s
always indicated . It is removedafter about a week .
279

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 275/333
CHAPTER 6
CLINICAL CASE 2
Male patient aged 48 with chronic periodontitis . Pocket an average o f
6-7 mm deep and horizontal bone reabsorption are present . Probing performe dafter anaesthesia (bone sounding) revealed the need to shorten the palatal flapby about 3 mm
The first internal bevel incision (no . 15 B.P.) is performed about 3 mm from th e
gingival margin to thin and shorten the flap . The incision is extended to th e
retromolar area .
After elevating the primary flap, the secondary flap can be clearly seen .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 276/333
PERIODONTAL FLAP SURGERY
The secondary flap is removed after making a second incision in the sulcus (no . 1 5B.P.) and a third interproximal incision (no . 1/2 Orban) at the base of the col .Thorough root and bone curettage is performed together with bone reshaping .
Note the thinned palatal flap .
The palatal flap is adapted to the bone planes and held under compression) with agauze moistened with physiological solution for 2-3 minutes . This minimizes the fil m
of fibrin and encourages coagulation . Immediately afterwards, the flap is closed withcontinuous suspended suture using 4-0 black silk .
281

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 277/333
CHAPTER 6
CLINICAL CASE 3
Female patient aged 35 with amelogensis imperfecta . The crown enam-el is completely destroyed and the clinical crowns must therefore be length-ened to allow for prosthetic reconstruction of the teeth
After bone sounding, two incisions are performed, the firs t
intracrevicular to the osseous crest, the second 6-7 mm from the
gingival margin .
A full thickness primary flap is elevated . The secondary flap is then
removed and an ostectomy performed to obtain crown lengthening .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 278/333
PERIODONTAL FLAP SURGERY
s
. Now seeming considerably longer, the teeth are then prepared for optimum reception of firs t
the definitive prosthesis .
.
283

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 279/333
CHAPTER 6
E) The Distal W edg eThe retromolar gingival mucosa zone of the mandible and maxilla
often present variations - sometimes bulbous and keratinized, sometimes fla t
and without keratin In the majority of cases, there is a limited amount of keratin in this area .The treatment of any periodontal pockets in the distal sector of the last mola rmay be complicated by poor accessibility and the local anatomy.The operation to reduce retromolar pockets was described by Robinson i n1966 in his article, now a classic, "The D istal Wedge Ope ration" In the presence of a pocket in the retromolar zone together with completelykeratinized tissue, the pocket eradication operation consists of a simple gin-givectomy However, if the tissue consists of a keratinized zone and a zone of mucos aonly, and access to the deep planes (bone and root surface) is required, thepreferred operation is the distal wedge procedure
Definition :The term distal wedge is applied to a particular surgical technique employe dto eradicate retromolar pockets and reduce the extent of retromolar tissue
Objectives :
To eradicate retromolar pockets To reduce the volume of the retromolar area To create access to the deep planes
Indications :
Periodontal pockets Clinical crown lengthening Retromolar bone surgery Pre-prosthetic surgery
Contraindications:
None

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 280/333
PERIODONTAL FLAP SURGERY
Surgical techniqu e
The retromolar zone may be surgically reduced by means of
A) Gingivectomy
B) Distal wedge procedure .
GINGIVECTOM Y
This operation is indicated exclusively in the case of moderately sever egingival hyperplasia . In these cases, a section perpendicular to the axis o fthe tooth is sufficient to completely eradicate a pocket or the gingiva lhyperplasia.
285

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 281/333
CHAPTER 6
DISTAL WEDG E
The flap incisions to reduce the retromolar zone can be performed in thre edifferent ways
I) Triangular incisio n
II) Parallel incisions
III) Page incision
I) TRIANGULAR INCISION
A triangular incision ismade angled from themedian part towardsthe exterior so as t o
obtain a thinned flap .The incision is then
continued along theintracrevicular line a s
far as the interproxi-
mal space between th e
last two molars
Two full thickness flap s
are elevated, isolatingthe distal wedge w hic h
is removed by firs tgripping it with aCocker Mosquito an dthen detaching it from
the deep osseous planeswith an Ochsenbeinchisel
c

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 282/333
PERIODONTAL FLAP SURGERY
d-
ed with physiologica lolution. If there is an
intraosseous pocket
reated by mea ns-
tive or regenerative)
At the end of the operation, the flaps ar e
sutured with 4-0 black silk .Alternatively, an absorbable suturematerial can be used .
287

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 283/333
CHAPTER 6
II) PARALLEL INCISIONS
Pre-operative image .
Two parallel incisions are made in the keratinized retromolar gingiva ter-
minating in the mucosa . The incisions are undercut by sloping the scalpel .
The result is two thinned flaps . The incisions are then extended around th e
last two molars and may either be intracrevicular or 1-2 mm from the gin-
gival margin . This depends on whether epithelium needs to be remove d
from within the periodontal pocket .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 284/333
PERIODONTAL FLAP SURGERY
After elevating the two mucoperiosteal flaps, the block of intermediate tissu eis removed with the help of an Ochsenbein chisel .
The bone tissue and root surfaces of the two molars are exposed and curet -tage is performed . The area is then irrigated with physiological solutio n
and, if necessary, bone surgery (resective or regenerative) is performed .
The flaps are adapted accurately to the deep planes and sutured with inter -rupted circular stitches, using 4-0 black silk in order to obtain healing b yfirst intention .
289
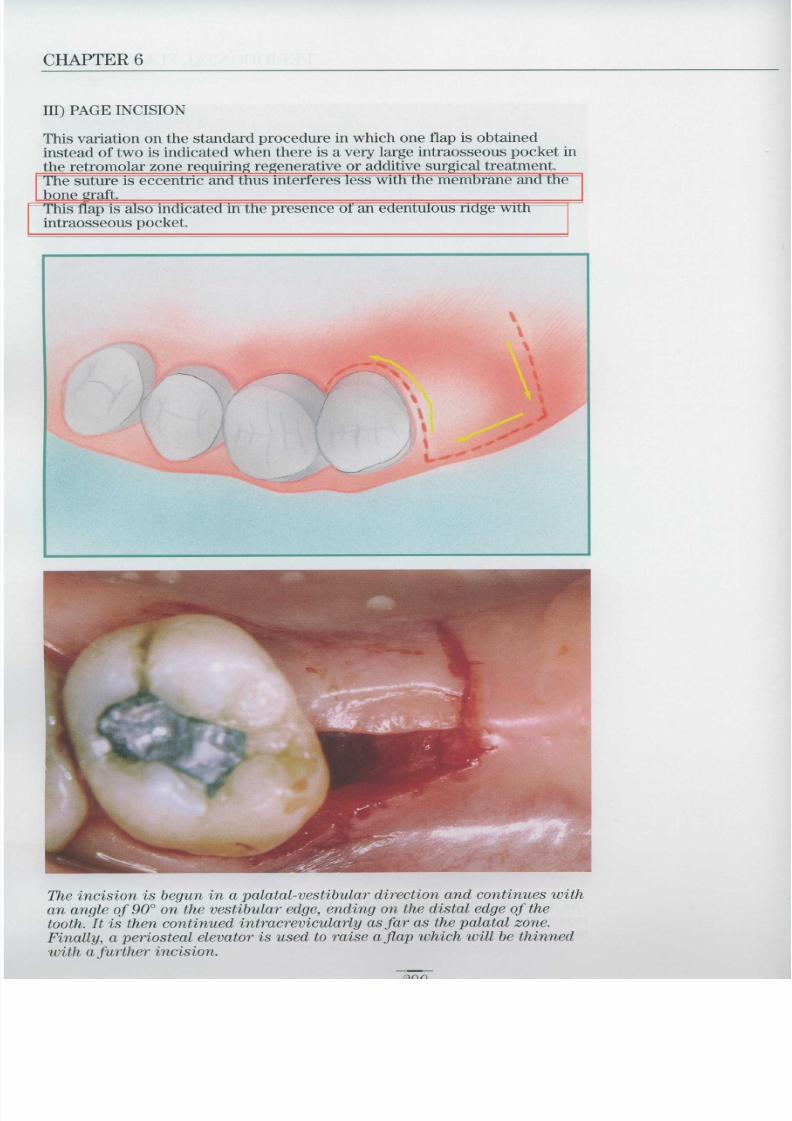
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 285/333
CHAPTER 6
III) PAGE INCISIO N
This variation on the standard procedure in which one flap is obtainedinstead of two is indicated when there is a very large intraosseous pocket in
the retromolar zone requiring regenerative or additive surgical treatment
The suture is eccentric and thus interferes less with the membrane and thebone graft This flap is also indicated in the presence of an edentulous ridge wit hintraosseous pocket
The incision is begun in a palatal-vestibular direction and continues wit han angle of 90° on the vestibular edge, ending on the distal edge of th e
tooth . It is then continued intracrevicularly as far as the palatal zone .Finally, a periosteal elevator is used to raise a flap which will be thinne d
with a further incision

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 286/333
PERIODONTAL FLAP SURGERY
Curettage of the root su7faces and bone defect is performed, followed b y
irrigation with physiological solution .If necessary, bone surgery (regenerative - additive) is performed
The flap is carefully adapted to the deep planes and sutured with inter-
rupted circular stitches .
291

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 287/333
CHAPTER 6
Sm oking and the outcom e
of treatmen t
Cigarette smoking is recognized as having a negativ einfluence on the outcome of surgical and non-surgica ltreatment (Kaldahl, 1996) . In addition, it had previouslybeen demonstrated (Bergstrom, 1987) that smoking had anegative effect on bone reabsorption, even in patient swith a high standard of hygiene
Reabsorption of alveolar bone height with respect to age : study carried out on smoker and non-smoker patients
Smoker patien tEighteen months previously the patient underwen t
periodontal flap surgery
The photographs were take n
during a routine professiona lscaling session (every thre emonths). Note the enormousquantity of black pigmentation(nicotine and tar and gingival inflammation .
292

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 288/333
PERIODONTAL FLAP SURGERY
H ealing of the operation site
Modified Widman flap
A) Curettage is performed on the bone which is then covered with the flap .
B) During the healing phase, bone reabsorption takes place together wit hbone regeneration widthways . A long junctional epithelium is interposedbetween the regenerated tissue and the root surface
C) During tissue maturation (6-12 months), moderate apical migration of th e
gingival margin occurs .
Apically positioned flap
A) Bone reshaping is performed and the flap is positioned at the crest
B) The bone continues to be reabsorbed and there is attachment loss .
C) During tissue maturation (6-12 months), a certain amount of regeneration o fthe bone and coronal attachment apparatus occurs
CONCLUSION S
Longitudinal studies have shown (1st European Workshop onPeriodontology, 1993) that the various surgical methods are equally effectiv e
in reducing periodontal pocket depth and controlling the progression o fchronic adult periodontitis
Post-operative control of bacterial plaque is, however, the most important fac -tor in determining the long term success of periodontal surgery, regardless of
the technique used .
These observations reduce the significance of the traditional differentiatio nbetween surgical techniques indicated to reduce pocket depth (access flap an d
modified Widman flap) and surgical techniques indicated to eliminate th epocket (apically positioned flap and gingivectomy) .
293

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 289/333
Chapter 7
Resectiv eBone Surgery

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 290/333
RESECTIVE BONE SURGERY
The term resective bone surgery is applied to all procedure semployed to eliminate craters and angular defects caused by the bone reab-sorption typical of periodontal disease . The principles of resective bonesurgery were set out by Schluger in 1949 and again by Goldman in 1950 .These authors described the direct relationship between the gingival profil eand the shape of the underlying bone . Elimination of craters and osseou sangular defects is therefore vital to obtaining an optimum gingival profileand maintaining shallow pockets after periodontal surgery .
Normal bone profil eNormal bone architecture consists of a festooned bone profile with into proximal septa locate d
coronally to the radicular bone . The bone and the cemento-enamel junction are about 2 mm apart .
297

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 291/333
CHAPTER 7
Almost normal bone profileNote the greater distance between the bone and the cemento-enamel junction, although the paraboli c
profile and shape of the interdental alveolar septa are conserved
Pathological bone profileNote the much greater distance between the bone and the cemento-enamel junction .
The parabolic profile and shape of the interdental alveolar septa are completely altered .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 292/333
RESECTIVE BONE SURGERY
Bone defects
Bone defects consist of localized reabsorption of the osseous alveolarcrest around the tooth . They are also known as intraosseous defects as the yare formed within the bone mass and are classified according to the number o fconstituent walls
Bone defects may occur in various sites around the same tooth and are usual-ly located in the interproximal space . However, they may also occur in th evestibular and/or palatal and lingual bone tissue If they occur in the bone tissue of a root furcation, there may also be som edegree of reabsorption between the roots, in the severest cases, establishingcommunication between the vestibular and palatal or lingual sectors
O ne wall hemiseptum
Two walls
299

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 293/333
CHAPTER 7
CraterA bone defect is defined as a crater whe n
the two surviving bone walls are th e
vestibular and lingual or palatal walls .
Three walls

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 294/333
RESECTIVE BONE SURGERY
Circumferential
Resective bone surgery is not indicated for very large bone defectswhich are m ore effectively treated by regenerative or additive bone surgery (o ra combination of both)
ADDITIVEBone grafts
Bone implants
REGENERATIVEGuided tissu e
regeneration (GTR )
301

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 295/333
CHAPTER 7
Resective Bone Surgery
OSTEOPLASTY
The term osteoplasty was introduced by Friedman in 1955 . The aim o fthis technique is to reshape the bone to create a physiological form withou tremoving the supporting bone (tissue connected to the tooth via periodonta lfibres)
Surgical techniqu e
After elevating a full thickness flap, osteoplasty is performed using mediu mgrain diamonds mounted on a turbine or micromotor The operation site must be abundantly irrigated with cold (4-5°C sterile salin esolution) Initially, the diamond is moved in a coronal-apical direction to reduce th ethickness of the bone . The surface is then finished with the same diamon dused with a brush-type movement in a mesial-distal direction During the operation, great care must be taken to avoid touching the root sur-faces with the rotating diamond.
INDICATIONS TECHNIQI IE CONTRAINDICATION S
Bon e
reshapingOsteoplasty Non e
Elimination of small Degree 2-3 toot hbone defects
Ostectomymobility
Creation of a Osteoplasty Bone reabsorption of >50%physiological p rofile Ostectomy Degree 2-3 tooth m obilit y
Diamonds forosteoplasty

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 296/333
RESECTIVE BONE SURGERY
A fter Osteoplasty
Before the Osteoplast y
Bone reabsorptioncaused by periodonta ldisease has modifie dthe bone a rchitecture .After elevating a ful l
thickness flap, it was
therefore decided toreshape the bon e
architecture byosteoplasty .
After osteoplasty, th e
rnd the ledge has bee n
eliminated withou t
removing thesupporting bone .
303

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 297/333
CHAPTER 7
OSTECTOMY
Ostectomy describes the surgical procedure employed to remove th esupporting bone tissue (bone connected to the tooth by means of periodonta lfibres) This technique is used to re-establish the physiological contour of bone tissu ealtered by periodontal disease
Before Ostectom y
After Ostectomy
The physiologica larchitecture of the bon e
has been completelyaltered by bon ereabsorption caused b yperiodontal disease .
Ostectomy (removal of
the supporting bone has been performed .
This operation hasrecreated the physiolog-ical architecture of thealveolar bone
The interproximal boneis now more taperedand located more coro-
nally to the radicular
bone . This type of con -tour is defined as `par-
abolic
ni
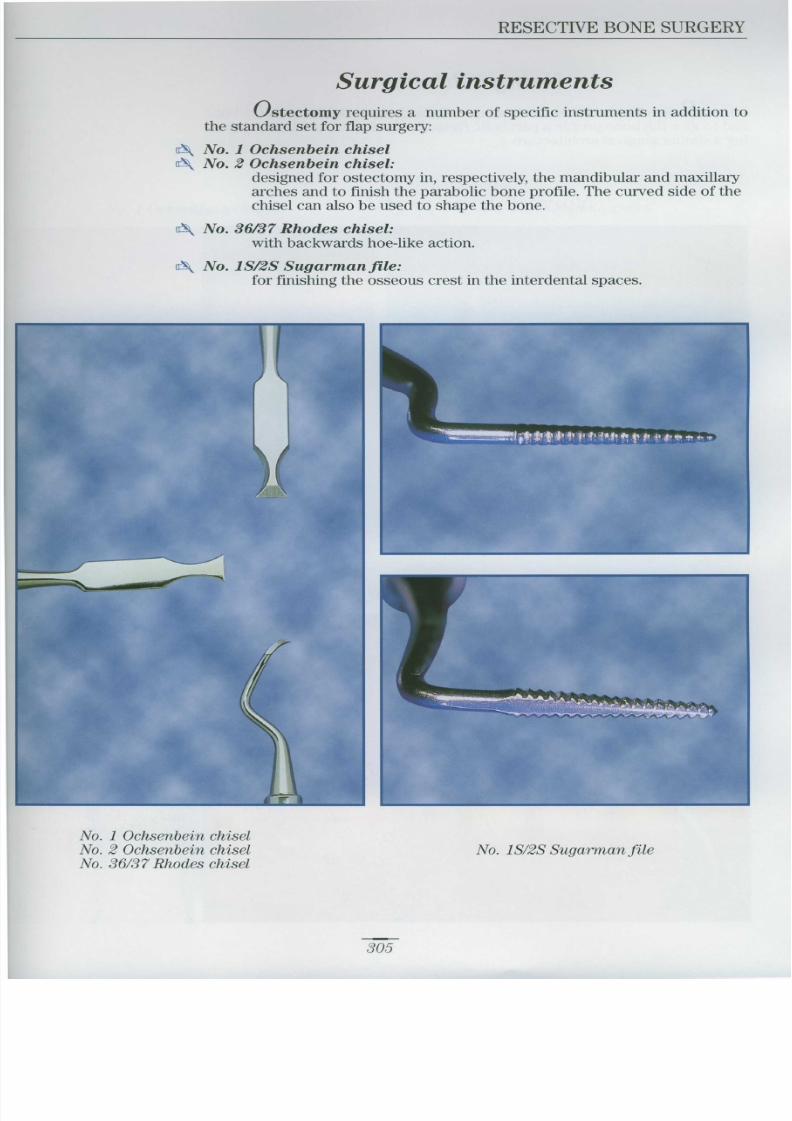
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 298/333
RESECTIVE BONE SURGERY
Surgical instrumentsOstectomy requires a number of specific instruments in addition t o
the standard set for flap surgery
No 1 Ochsenbein chise l
c No 2 Ochsenbein chisel:
designed for ostectomy in, respectively, the mandibular and maxillar yarches and to finish the parabolic bone profile . The curved side of th echisel can also be used to shape the bone
c No . 36/37 Rhodes chisel :
with backwards hoe-like action
No 1S/2S Sugarman file :
for finishing the osseous crest in the interdental spaces
No. 1 Ochsenbein chise lNo. 2 Ochsenbein chise l
No. 36/37 Rhodes chisel
No . IS/2S Sugarman file
305

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 299/333
CHAPTER 7
Using Chisels
Bone chisels are used to remove vestibular and palatal support bon eand to give the bone profile a parabolic (festooned) shape capable of support-
ing a similar gingival architecture
Normal bone profile
The vestibular boneprofile is paraboli cwith a physiologica l
architecture andinterdental peak s
positioned coronall yto the festoons
Pathological bone profile
Following periodonta ldisease, bone reabsoi p -tion has taken place .The bone profile hasbeen completely altered .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 300/333
RESECTIVE BONE SURGERY
To modify the bone profile, no . 1 and no. 2 Ochsenbein chisels and ano . 36/37 Rhodes chisel are used
No. 1 Ochsenbein chisel No . 2 Ochsenbein chisel
No . 36/37 Rhodes chisel

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 301/333
CHAPTER 7
Using files
Interdental files are used to remove small pieces of connective tissu efrom the interradicular bone while at the same time filing the surface . The
sides of the files are not sharp so as to avoid damaging the surface of the toothduring the operation
No . 1 S/2S file
The sides of the fil e
(Sugarman 1 S/2S) ar e
flat to avoid damagingthe root surface of theteeth during filing

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 302/333
RESECTIVE BONE SURGERY
SURGICAL CORRECTION OF INTERPROXIMAL CRATERS
The guided tissue regeneration technique can be used to treat dee pinterproximal craters Ostectomy is, however, the preferred treatment for craters no deeper than 3- 4
mm, especially if located in a vestibular position .To remove the vestibular wall or the bone walls of the defect, first medium -sized diamonds, then chisels and files are used as described previously
Pre-operative Post-operative
Pre-operative Post-operative
309

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 303/333
CHAPTER 7
RESECTIVE BONE SURGERY
Resective bone surgery uses both osteoplasty and ostectomy t oreshape the bone tissue The aim is to obtain bone architecture with a physiological parabolic shap ewith the interproximal septa positioned coronally to the festoons
Note the altered bone architecture
Phases of resective bone surgery
Step 1 : Preparation of vertical groove s
Step 2 : Preparation of festoons
Step 3 : Margin definitio n
Step 4 : Parabolization
Hunan maxilla : vestibular view
FUNDAMENTAL RULES OF BONE SURGERY
o Always elevate full thickness flaps
o The scalloping of the flap should anticipate the anatomy of the underlyingbone after surgery .
©Osteoplasty should always precede ostectomy
© If possible, surgery should always finish with positive bone architecture
©Micromotor or turbine mounted burs or diamonds must never come int ocontact with the teeth and must always be used under an abundant spra y
of cold water

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 304/333
RESECTIVE BONE SURGERY
SURGICAL TECHNIQUE - VESTIBULAR, SECTIO N
Step 1 : Preparation of vertical groovesAfter elevating a mucoperiosteal flap and exposing the bone surface, a
rounded bur (no. 8) is used to cut vertical grooves in the interdental spaces starting from the coronal part and extending apically These grooves indicate the quantity of bone to be removed
311

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 305/333
CHAPTER 7
Step 2 : Preparation of festoon sUsing the same bur with a horizontal brush movement, the grooves are
joined together, reducing the thickness of the bone at the margins to obtain a
physiological shape .
?1
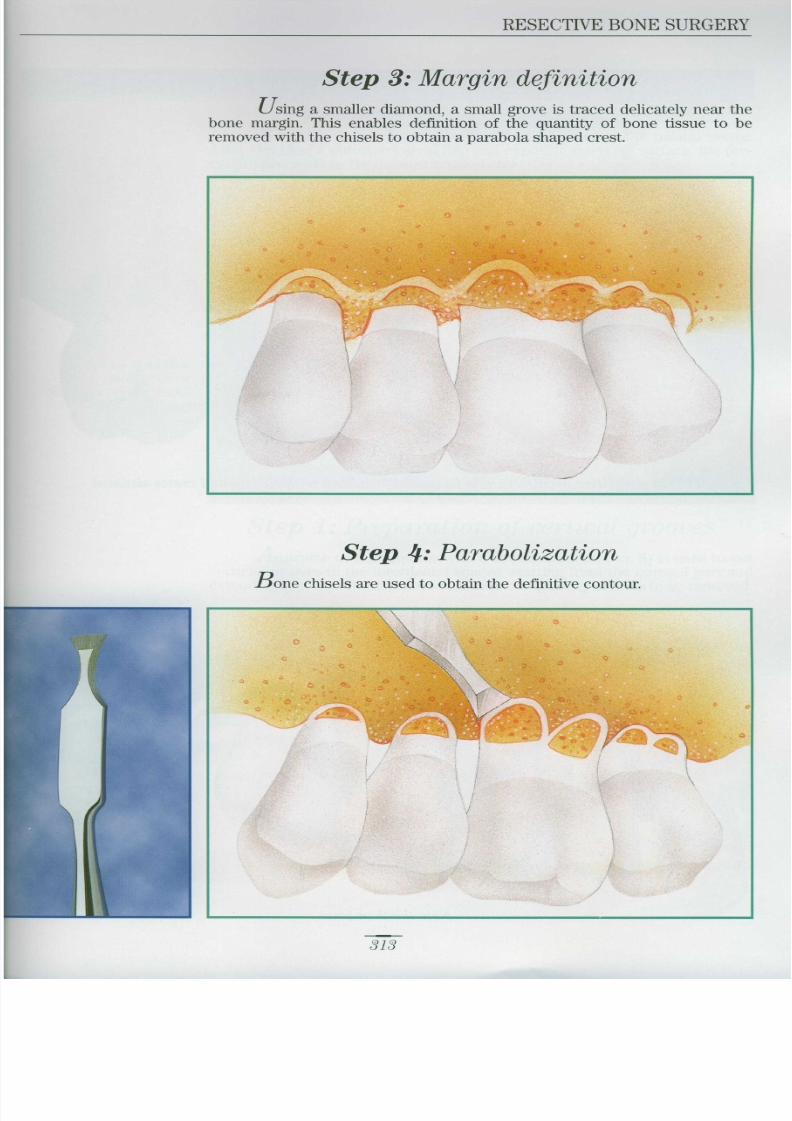
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 306/333
RESECTIVE BONE SURGERY
Step 3 : Margin definition
Using a smaller diamond, a small grove is traced delicately near th ebone margin . This enables definition of the quantity of bone tissue to b eremoved with the chisels to obtain a parabola shaped crest
Step 4 : Parabolization
Bone chisels are used to obtain the definitive contour
313
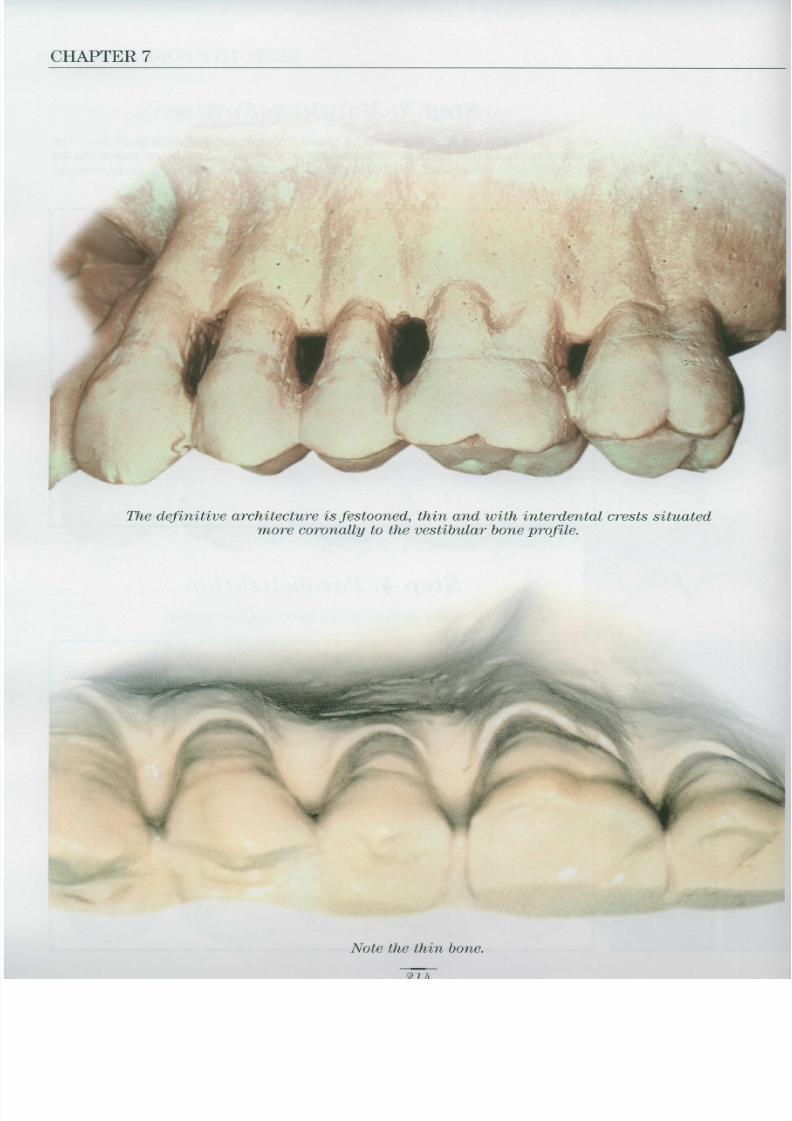
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 307/333
CHAPTER 7
The definitive architecture is festooned, thin and with interdental crests situate dmore coronally to the vestibular bone profile .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 308/333
RESECTIVE BONE SURGERY
SURGICAL TECHNIQUE - PALATAL SECTO R
Resective bone surgery can also be performed in the palatal sector After elevating a mucoperiosteal flap and exposing the bone surface, the pro-cedure proceeds as for the vestibular sector
Human maxilla :
palatal viewNote the perfect bone
architecture .
Step 1 : Preparation of vertical groove sA turbine or micromotor with a round diamond (no . 8) is used to cut
vertical grooves in the interdental spaces, starting from the coronal part an dextending apically. Th ese grooves indicate the quantity of bone to be rem oved
Vertical grooves hav eg
a round diamond
315

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 309/333
CHAPTER 7
Step 2 Preparation of festoon s
Using the same diamond with a horizontal brush movement, th egrooves are joined together, reducing the thickness of the bone at the margins
Step 3-4 Margin definitionParabolization
After defining the quantity of bone to be removed, bone chisels ar eused to obtain a parabolic contour as indicated for the vestibular sector .
The definitivearchitecture i s
festooned and th e
osseous crest i spositioned more
coronally to the
palatal profile .
16

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 310/333
RESECTIVE BONE SURGERY
CLINICAL CASE
Patient suffering from chronic adult periodontitisPremolar and molar periodontal pockets are present in the rear maxillary sec -tion with an average depth of 6-7 mm .
The hygienic phase reduces the depth of the pockets (average 5-6 mm) The surgical treatment involves elevation of a mucoperiosteal flap and reshap -
ing of the bone to eradicate the pockets and obtain an anatomy suitable fo rpatient maintenance of a healthy periodontium .
Before bone surgery
An internal beve l
incision has been
performed, a ful l
thickness flap hasbeen elevated and th e
secondary flap ha sbeen removed .
The physiologica l
bone contour hasbeen altered by bon e
reabsorption causedby the periodontitis .The alterations can
be corrected b yresective bone
surgery .
317

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 311/333
CHAPTER 7
A fter bone surgery
Note the festoonedprofile of the bonewith the interdenta lsectors positione dmore coronally to the
vestibular bone .
The vestibular and
palatal flaps will b epositioned so as t o
cover the osseous cres t
and sutured indepen-
dently with continuoussuspended suture .

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 312/333
RESECTIVE BONE SURGERY
Clinical case sixmonths after the
operation. Note theelegant architecture
of the gingival tis -sues, perfectly adapt -ed to the underlying
bone structure .
MaintenanceThis new architecture facilitates bacterial plaque control and thu s
maintenance of a healthy periodontium . The patient will be included in a cyc l eof regular follow-up appointments for professional prophylaxis
CONCLUSIONS
Resective bone surgery is by definition destructive and does not in itself cur eperiodontitis as this is an infectious disease
This type of surgery is performed exclusively in the case of minor alteration sin the bone architecture which, in association with periodontal pockets
facilitate the progression of periodontal disease .
319

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 313/333
Chapter 8
Resectiv e
G ingival Surgery
321

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 314/333
RESECTIVE GINGIVAL SURGER Y
Increases in gingival volume may be caused by a range of factors andcan be divided into two forms
Gingival hyperplasia abnormal multiplication or increase in the number ofcells in the gingival tissue, leading to an increase in the volume of the gingiva .
Gingival hypertrophy an increase in the volume of the cells in the gingiva leading to an increase in the volume of the gingiva
Gingival hypertrophy usually disappears if the etiological factor causing it is
treated. On the other hand, once p resent, gingival hyperplasia does not regress even if the etiological agent is eliminated
Resective Gingival Surgery is used above all to treat gingival hyperplasia
Gingival Enlargements
GENERALIZED LOCALIZE D
*Hereditary Gingival Fibromatosi s
MucopolysaccharidosisAspartylglycosaminuri a
Donahue's Syndrom e
Pfeiffer's Disease
*Fibroepithelial Epuli s
*Giant Cell Tumou r
*Hormonal EpulisSarcoidosis
Multiple Myelom a
Langerhans' Cell Tumour*Chronic Inflammatory H yperplasia
*Diseases treatable by resective gingival surgery
Angiokeratoma Corpori sMultiple Hamartoma
Sturge Weber's Angiomatosi s
Acute Myeloid Leukemia
PreleukemiaAplastic Anemi a
*Drug s(Diphenylhydantoin, Cyclosporin
Ca Channel Blockers)
323

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 315/333
CHAPTER 8
CHRONIC INFL MM TORY HYPERPLASIA
Bacterial plaque hyperplasia the accumulation of bacterial plaqu e
induces a chronic inflammatory condition which predisposes the patient liable
to gingival fibrosis
Open mouth breathing hyperplasia during the night, adenoida lpatients with labial incompetence breathe with their mouths open . The con-tinued alternation of damp and dry conditions on the surface of the gingiva lmucosa induces an inflammatory condition which predisposes the patient togingival fibrosis

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 316/333
RESECTIVE GINGIVAL SURGER Y
HORMONAL HYPERPLASIA
During puberty or pregnancy, hormonal alterations may cause local-ized hyperplasia
PREGNANCY EPULIS
325

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 317/333
CHAPTER 8
HEREDITARY FAMILIAR FIBROMATOSIS
HYPERPLASIA DURING DIABETES MELLITUS
In patients with juvenile diabetes there is often a hyperplastic gingiva lresponse resulting from suppression of the typical activity of the macrophage swhich normally phagocyte the damaged collagen fibres
i

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 318/333
RESECTIVE GINGIVAL SURGERY
Collagen fibres of the
gingival connectivetissue .
In diabetics, the gingival connective tissue tends to increase due to theabnormal stability of the mature collagen, insensible to normal turnover .
327

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 319/333
CHAPTER 8
D IP H EN Y L H Y D A N T O IN H Y P ER P L A SIA
common type of gingival hyperplasia frequently occurs during the chroni cassumption of certain drugs such as diphenylhydantoin, cyclosporin etc

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 320/333
RESECTIVE GINGIVAL SURGERY
Gingival Connective Tissue Serum
PATHOGENIC HYPOTHESIS
SalivaryGlands
The diphenylhydantoin taken by epileptics passes from the plasm a
serum to the salivary glands, building up in the bacterial plaque . It has beenshown (Steinberg A .D . et al, J .Perio Res . 1976) that bacterial plaque diphenyl-hydantoin is reabsorbed through the sulcular epithelium and deposited in th eunderlying connective tissues where it is added to the diphenylhydantoin o fhematic origin.
329

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 321/333
CHAPTER 8
SURGICAL JUSTIFICATION
In cases of gingival hyperplasia, surgery must be performed to elimi-nate the pseudopocket and re-establish a physiological contour
Pocke tConnective attachment loss with bon ereabsorption.
Pseudopocke tPocket caused by gingival hyperplasia withou t
connective attachment loss or bone reabsorption

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 322/333
RESECTIVE GINGIVAL SURGERY
Surgical instrumentsThe instruments used in Resective Gingival Surgery include
Double-sided mirror :
for improv ed v isibility
CP12 graduated periodontal probe :for measurements and probing
G'N Goldman-Fox right and left pocket marker:forceps to establish pseudopocket depth .
Straight round scalpel :
for excising the hyperplastic tissue
No . 15/16 Kirkland scalpel :for incising the hyperplastic tissue .
Universal curette :
for removing pieces of tissue and root planing
H3 curved Cocker Mosquito :for removing pieces of tissue .
Surgical Forceps
Columbia retractor:to retract cheeks and lips
Cook-Waite syringe for anaesthesi a
LaGrange scissors :to finish gingival tissue
v
331

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 323/333
CHAPTER 8
SURGICAL TREATMEN T
Step 1 : Measuring the pseudopocket sThe first surgical phase involves measuring the depth of th e
pseudopockets to establish the amplitude of the surgical excision.
A periodontal probe is used first to measure the pseudopocket and then t oreproduce the measurement externally with a bleeding point.Alternatively, this can be done using Goldman-Fox pocket marker forceps

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 324/333
RESECTIVE GINGIVAL SURGERY
inimum instruments necessar ygingivectom y
• CP 12 Periodontal Prob e
• no . 7/8 Younger-Good Curett e
• LaGrange Scissors
• no . 15/16 K irkland Scalpe l
• right and left Goldman-Fox Pocke t
Marker Forceps
.
333

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 325/333
CHAPTER 8
Step 2 IncisionThe initial incision is made slightly on the apical side of the bleedin g
points with a no . 15 Bard-Parker blade or a no. 15/16 Kirkland scalpel. The
instrument should slope in an apical-coronal direction and the incision shoul dreach the bottom of the pseudopocket
No . 15/16 Kirkland
scalpel
Step 3 Excisio nAfter the hyperplastic tissues have been incised, they are remove d
using a no . 1/2 Orban interproximal scalpel. The operation is completed withthe help of a curette
No . 5/6 Buckinterproximal scalpel
Qh

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 326/333
RESECTIVE GINGIVAL SURGERY
Step 4: Gingivoplasty
The definitive gingival profile and shape are obtained using LaGrangescissors. In some cases, a coarse grain turbine-mounted diamond may also b eused for gingivoplasty
Step 5 Hemostasis
The raw gingival surface is covered with a strip of Surgicel' to controlpost-operative hemorrhage and then with a soft periodontal pack . The pack isleft in situ for about a week
Surgicel
335

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 327/333
CHAPTER 8
Post-operative treatmen t
Once the periodontal pack has been removed, topical 0 .2% chlorhexi-dine treatment (gel) is continued for a week . At the same time, normal ora l
hygiene procedures are gradually resumed . Drug-induced gingival hyperplasiatends to reoccur. Post-operative treatment therefore involves a rigid pro -gramme of follow-up appointments (every three months) . During the profes-sional prophylactic sessions, the following operations are performed
1) Reinforcement of patient compliance 2) Scaling and polishing .
3) Minor and localized gingivectomy (if necessary) 4) Topical chemotherapy
Post-operative image(after two months) .Note the excellen t
aesthetic andfunctional results .
Post-operative image(after two years) .The patient continuesthe diphenylhydantoin
therapy. Note the mod-erate hyperplasia start-ing to re-form in corre-
spondence with the
interdental papillae
perhaps caused b yreduced plaque contro lby the patient
,`

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 328/333
RESECTIVE GINGIVAL SURGERY
Pre-operative image
Post-operative image (after two months) .
337

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 329/333
CHAPTER 8
CLINICAL CASE 1 Puberal Hormonal Hyperplasia
During puberty, hormonal alterations may induce localized gingiva lhyperplasia
Localized gingival hyperplasia in a femalepatient aged 13 .
The first incision is performed with a Kirklandscalpel sloping in an apical-coronal direction (4 ,
After excising th e
hyperplastic tissue
a gingivoplasty i sperformed .
A small quantity of
Avitene® is applied as ahemostatic .
00 0

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 330/333
RESECTIVE GINGIVAL SURGERY
Post-operative image(after one month) .
nreveals an epithelials
. The basa llayer is normal
339

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 331/333
CHAPTER 8
CLINICAL CASE 2 Diphenylhydantoin-induced hyperplasi a
Diphenylhydantoin-induced generalized gingival hyperplasia in anepileptic male patient aged 25, in an institution for many years . As a result ofpoor bacterial plaque control, the hyperplasia is associated with hypertrophycaused by local accumulation of fluids due to the inflammation present . Afte rcompleting the hygienic phase, gingivectomy was performed first in the max-illary arch and then in the mandibular arch
h n

7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 332/333
RESECTIVE GINGIVAL SURGERY
341
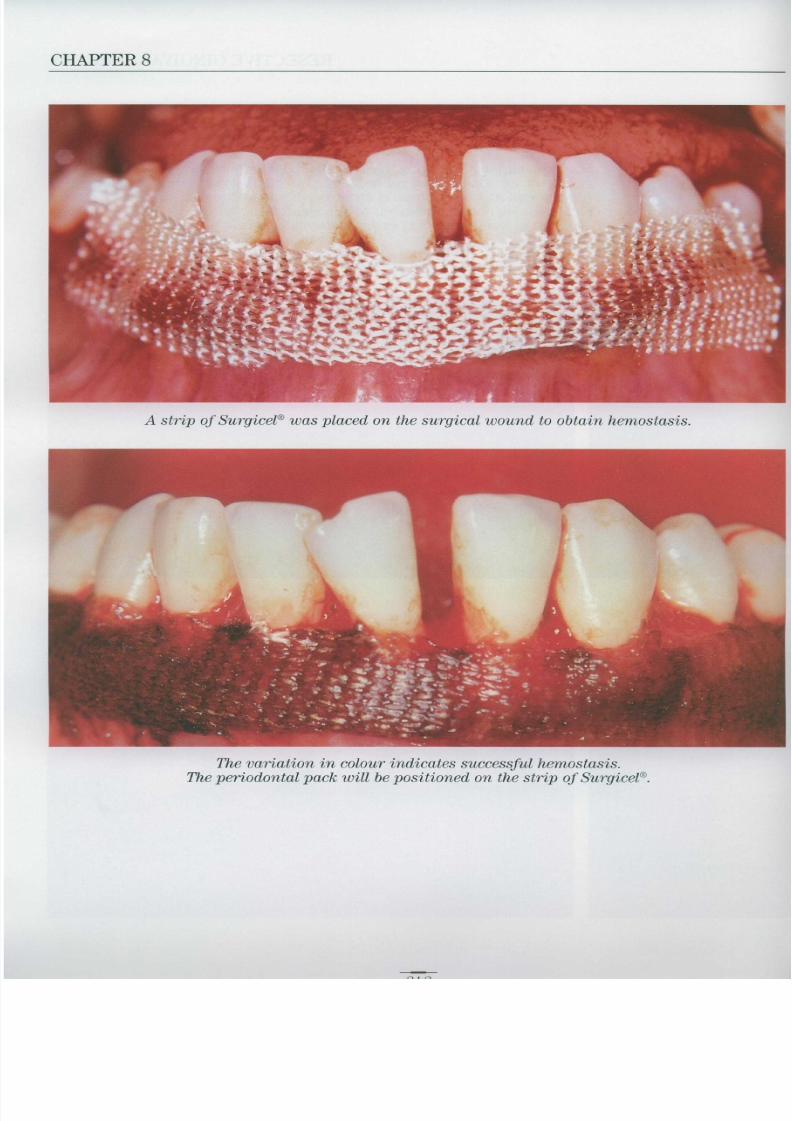
7/22/2019 Periodontology Bartolucci One
http://slidepdf.com/reader/full/periodontology-bartolucci-one 333/333
CHAPTER 8
A strip of Surgicel was placed on the surgical wound to obtain hemostasis
The variation in colour indicates successful hemostasis .The periodontal pack will be positioned on the strip of Surgicel