penwnl edsigatilhnciad vwdpyggiwhdfiwh ed … edsigatilhnciad vwdpyggiwhdfiwh ed or2iancia ... tin...
TRANSCRIPT

Earn
2 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
Clinical Perspectives on Current Dental AdhesivesA Peer-Reviewed Publication Written by Mark A. Latta, DMD, MS
PennWell designates this activity for 2 Continuing Educational Credits
Publication date: April 2008Review date: April 2011Expiry date: March 2014
Go Green, Go Online to take your course
This course has been made possible through an unrestricted educational grant. The cost of this CE course is $49.00 for 2 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.

2 www.ineedce.com
Educational ObjectivesUpon completion of this course, the clinician will be able to do the following:1. List and describe the types of dental adhesive systems
available.2. Describe the clinical application of etch-and-rinse
dental adhesives and the types of cases for which these are best suited.
3. Describe the clinical application of self-etch dental adhesives and the types of cases for which these are best suited.
4. Describe the newer adhesives that have been devel-oped and their benefits.
AbstractMost of the commonly performed tasks in dentistry have benefited from the development of modern dental ad-hesives, which are used for a wide range of applications. Dental adhesives enable minimally invasive dentistry. It is believed that dental adhesives can reinforce weakened den-tin or enamel, reduce marginal staining, reduce microleak-age, and may also reduce postoperative sensitivity when used appropriately. The resin-based adhesive systems developed to date can be categorized as one of two types: etch-and-rinse (total-etch) adhesive systems and “self-etch” adhesive systems. Both systems result in a unique interface at the juncture of tooth surface and adhesive. In the last decade, most new developments in dental adhesives have been focused on simplifying the components required for the bonding systems and improving performance of the resulting self-etching adhesives. Enamel bonding is supe-rior with etch-and-rinse adhesive systems, while self-etch systems may be more suitable for restorations with large areas of dentin. Careful consideration of several factors is essential in selecting an adhesive system.
IntroductionModern dental adhesives are used for a wide range of ap-plications. Direct anterior and posterior composite resin restorations all require bonding, while amalgam restora-tions may (optionally) also be bonded. S i m i l a r l y, indirect resin inlays, onlays, and veneers require bonding and, depending on their design, crowns, bridges, and posts and cores may also either require and/or benefit from the use of dental adhesives in conjunction with resin luting materials. In addition, dental adhesive technology is used in pit-and-fissure sealants, some endodontic obturation materials, fixed orthodontic appliances, and dentinal hy-persensitivity treatments. In total, most of the commonly performed tasks in dentistry have benefited from the de-velopment of dental adhesives.
Dental adhesives were originally developed as an ex-tension of industrial adhesives used to help paint and resin coatings bond to metal.1 Dr. Michael Buonocore is widely
considered to be the first person to propose the application of adhesion technology in dentistry. His groundbreak-ing research in 1955 demonstrated for the first time that acid-etching of enamel could provide a surface suitable for bonding with resins.2 By the mid-1960s, the first com-mercially available pit-and-fissure sealants and composite resin materials utilizing this new adhesive technology were used clinically.3 Buonocore theorized that resin tags filling the defects created by the etchant were responsible for enamel adhesion, and by the late 1960s, he also proposed that bonding to dentin was possible.4 Since then, dental adhesives have been developed that provide numerically higher bond strengths and more substantive bonded inter-faces to both enamel and dentin. By the 1980s, etch-and-rinse adhesives had gained widespread acceptability. By the 1990s, the concept of the “hybrid layer” was accepted, and both multi-step and single-step adhesives were avail-able (Table 1).
Table 1. Development of dental adhesives
1955 Proposed dental application of adhesive technology
mid-1960s
Commercially available pit-and-fissure sealants and composite resins utilizing bonding
late 1960s Proposed bonding of dentin
1980s Widespread acceptability of etch-and-rinse adhesives
1990s Acceptance of the “hybrid layer” concept Availability of multi-step and single-step adhesives
Dental adhesives promote conservation of tooth struc-ture and enable minimally invasive dentistry. For example, bonded bridges are based on the concept of minimal tooth preparation, by taking advantage of the adhesion of the “wings” of the bridge to abutment teeth. Chemical retention, either alone or in combination with mechanical retention (depending on the preparation’s configuration), has been demonstrated in various laboratory tests. Thus, it is believed that dental adhesives can reinforce weakened dentin or enamel, reduce marginal staining, reduce mi-croleakage,5 and may also reduce postoperative sensitivity when used appropriately (Table 2).6
Table 2. Potential effects of dental adhesives
Promotion of tooth structure conservation
Reinforcement of weakened dentin and enamel
Reduction of microleakage
Reduction of marginal staining
Reduction of postoperative sensitivity
www.ineedce.com 3
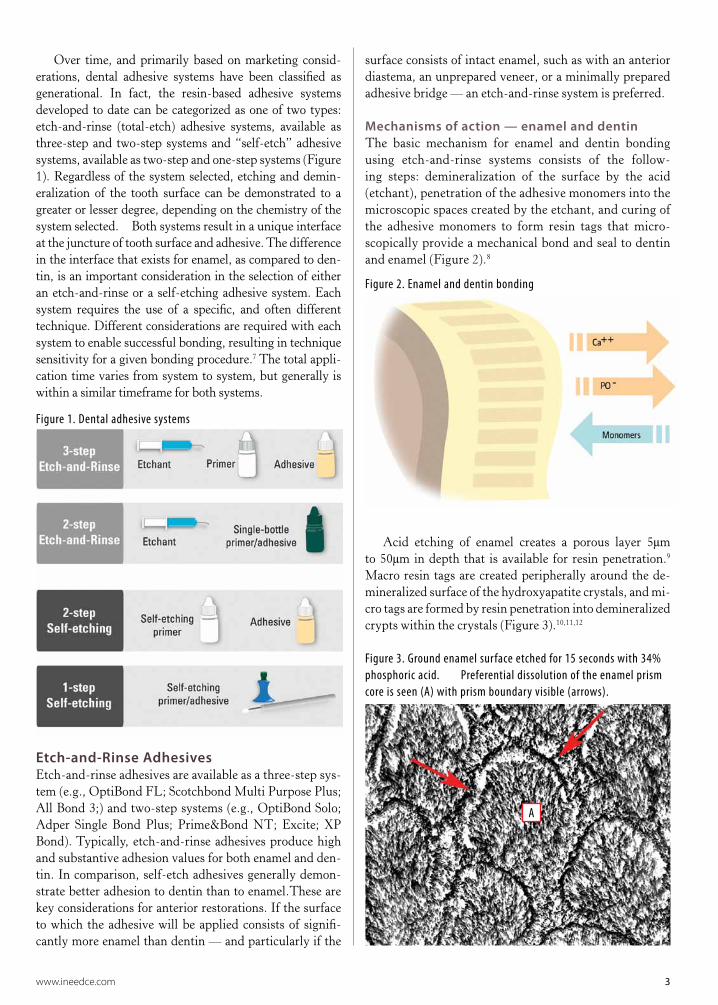
Over time, and primarily based on marketing consid-erations, dental adhesive systems have been classified as generational. In fact, the resin-based adhesive systems developed to date can be categorized as one of two types: etch-and-rinse (total-etch) adhesive systems, available as three-step and two-step systems and “self-etch” adhesive systems, available as two-step and one-step systems (Figure 1). Regardless of the system selected, etching and demin-eralization of the tooth surface can be demonstrated to a greater or lesser degree, depending on the chemistry of the system selected. Both systems result in a unique interface at the juncture of tooth surface and adhesive. The difference in the interface that exists for enamel, as compared to den-tin, is an important consideration in the selection of either an etch-and-rinse or a self-etching adhesive system. Each system requires the use of a specific, and often different technique. Different considerations are required with each system to enable successful bonding, resulting in technique sensitivity for a given bonding procedure.7 The total appli-cation time varies from system to system, but generally is within a similar timeframe for both systems.
Figure 1. Dental adhesive systems
Etch-and-Rinse AdhesivesEtch-and-rinse adhesives are available as a three-step sys-tem (e.g., OptiBond FL; Scotchbond Multi Purpose Plus; All Bond 3;) and two-step systems (e.g., OptiBond Solo; Adper Single Bond Plus; Prime&Bond NT; Excite; XP Bond). Typically, etch-and-rinse adhesives produce high and substantive adhesion values for both enamel and den-tin. In comparison, self-etch adhesives generally demon-strate better adhesion to dentin than to enamel.These are key considerations for anterior restorations. If the surface to which the adhesive will be applied consists of signifi-cantly more enamel than dentin — and particularly if the
surface consists of intact enamel, such as with an anterior diastema, an unprepared veneer, or a minimally prepared adhesive bridge — an etch-and-rinse system is preferred.
Mechanisms of action — enamel and dentinThe basic mechanism for enamel and dentin bonding using etch-and-rinse systems consists of the follow-ing steps: demineralization of the surface by the acid (etchant), penetration of the adhesive monomers into the microscopic spaces created by the etchant, and curing of the adhesive monomers to form resin tags that micro-scopically provide a mechanical bond and seal to dentin and enamel (Figure 2).8
Figure 2. Enamel and dentin bonding
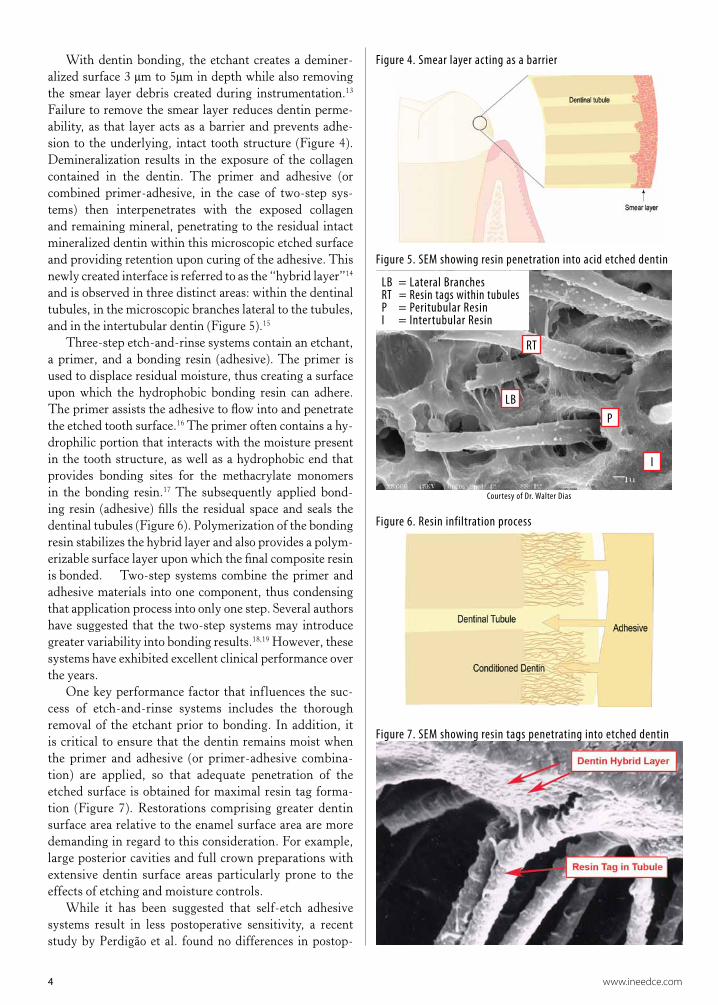
Acid etching of enamel creates a porous layer 5μm to 50μm in depth that is available for resin penetration.9 Macro resin tags are created peripherally around the de-mineralized surface of the hydroxyapatite crystals, and mi-cro tags are formed by resin penetration into demineralized crypts within the crystals (Figure 3).10,11,12
Figure 3. Ground enamel surface etched for 15 seconds with 34% phosphoric acid. Preferential dissolution of the enamel prism core is seen (A) with prism boundary visible (arrows).
A
4 www.ineedce.com
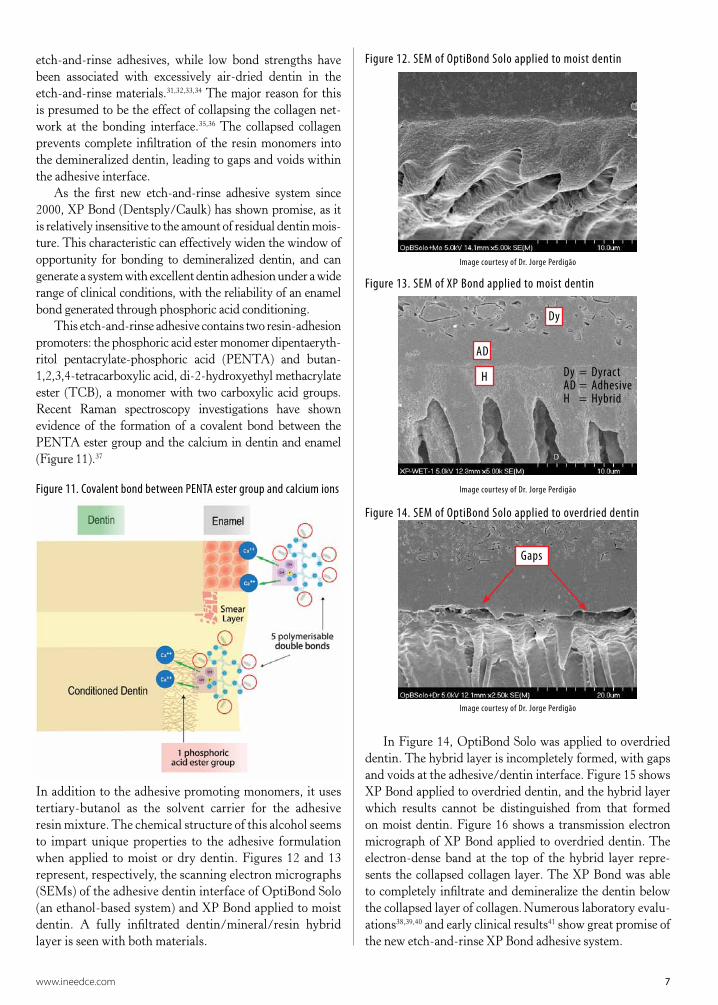
With dentin bonding, the etchant creates a deminer-alized surface 3 μm to 5μm in depth while also removing the smear layer debris created during instrumentation.13 Failure to remove the smear layer reduces dentin perme-ability, as that layer acts as a barrier and prevents adhe-sion to the underlying, intact tooth structure (Figure 4).
Demineralization results in the exposure of the collagen contained in the dentin. The primer and adhesive (or combined primer-adhesive, in the case of two-step sys-tems) then interpenetrates with the exposed collagen and remaining mineral, penetrating to the residual intact mineralized dentin within this microscopic etched surface and providing retention upon curing of the adhesive. This newly created interface is referred to as the “hybrid layer”14 and is observed in three distinct areas: within the dentinal tubules, in the microscopic branches lateral to the tubules, and in the intertubular dentin (Figure 5).15
Three-step etch-and-rinse systems contain an etchant, a primer, and a bonding resin (adhesive). The primer is used to displace residual moisture, thus creating a surface upon which the hydrophobic bonding resin can adhere. The primer assists the adhesive to flow into and penetrate the etched tooth surface.16 The primer often contains a hy-drophilic portion that interacts with the moisture present in the tooth structure, as well as a hydrophobic end that provides bonding sites for the methacrylate monomers in the bonding resin.17 The subsequently applied bond-ing resin (adhesive) fills the residual space and seals the dentinal tubules (Figure 6). Polymerization of the bonding resin stabilizes the hybrid layer and also provides a polym-erizable surface layer upon which the final composite resin is bonded. Two-step systems combine the primer and adhesive materials into one component, thus condensing that application process into only one step. Several authors have suggested that the two-step systems may introduce greater variability into bonding results.18,19 However, these systems have exhibited excellent clinical performance over the years.
One key performance factor that influences the suc-cess of etch-and-rinse systems includes the thorough removal of the etchant prior to bonding. In addition, it is critical to ensure that the dentin remains moist when the primer and adhesive (or primer-adhesive combina-tion) are applied, so that adequate penetration of the etched surface is obtained for maximal resin tag forma-tion (Figure 7). Restorations comprising greater dentin surface area relative to the enamel surface area are more demanding in regard to this consideration. For example, large posterior cavities and full crown preparations with extensive dentin surface areas particularly prone to the effects of etching and moisture controls.
While it has been suggested that self-etch adhesive systems result in less postoperative sensitivity, a recent study by Perdigão et al. found no differences in postop-
Figure 4. Smear layer acting as a barrier
Figure 5. SEM showing resin penetration into acid etched dentin
Courtesy of Dr. Walter Dias
Figure 6. Resin infiltration process
Figure 7. SEM showing resin tags penetrating into etched dentin
LB
RT
P
I
LB = Lateral BranchesRT = Resin tags within tubulesP = Peritubular ResinI = Intertubular Resin

www.ineedce.com 5
erative sensitivity between patients treated with self-etch adhesives and those treated with etch-and-rinse adhesives — nor have any differences been discovered in marginal integrity. It was concluded that restorative technique in-fluences postoperative sensitivity.20
There is proven long-term bond stability using etch-and-rinse systems with both enamel and dentin. Some studies have shown bonding to enamel is more consistent, with higher initial bond-strength values and less break-down at the enamel margin over time than with self-etch-ing adhesive systems.21 An important consideration when selecting between etch-and-rinse and self-etch systems is the condition of the enamel that will be bonded. If the enamel comprises mostly intact or uninstrumented enamel, the choice of an etch-and-rinse system is preferred (Figures 8a, 8b). If the tooth surface to be etched consists
mainly of dentin, self-etching systems may be a better choice in order to avoid the need to reinfiltrate the dentin after exposing the dentinal tubules with the etchant of the etch-and-rinse system (Figure 9).
Self-etching AdhesivesSelf-etch adhesives are available as one-step systems and two-step systems. They offer an advantage over etch-and-rinse systems: they do not require a separate etching procedure. Thus there is no need to rinse and then dry the preparation prior to application of the adhesive. In addi-tion, these systems are more tolerant of the presence of moisture on the preparation. Finally, the etching process proceeds in conjunction with the penetration of the adhe-sive, thus eliminating the potential for over-etching when treating dentin.
Techniques to maximize etch-and-rinse system performance
1) Etch the enamel first for at least 15 seconds, followed by etching the dentin for a maximum of 15 seconds. This will en-sure that the demineralized areas created during etching will be filled through capillary action, subsequently forming resin tags. Enamel should not be under-etched (less than 15 seconds) and dentin should not be over-etched (more than 15 seconds)—ei-ther of which could result in a reduced bond strength.22
2) Ensure that the dentin is slightly moist after rinsing-off the etchant and ‘drying’ the dentin. This “moist bonding”23 helps prevent exposed collagen from collapsing and forming a coagulate,24 which could prevent adhesive penetration into the dentin. Bonding is impaired if the dentin is either too dry or too moist.
3) Dispense the etch-and-rinse primer or primer-adhesive combination immediately prior to placement, so as to avoid evaporation of the solvents contained therein. Using a delivery system that results in simultaneous dispensing.
4) Apply an amount of adhesive sufficient to thoroughly coat and penetrate the entire etched surface. If using a two-step system, several layers of the primer-adhesive should be applied to ensure an adequately thick layer of adhesive — solvent pres-ent in the primer-adhesive can otherwise result in a layer that is too thin. Because etching dentin removes the smear layer, a larger surface area for adhesion is exposed, thus requiring more adhesive than is necessary for the etched enamel surface.
5) Thoroughly air-dry the adhesive to remove the ethanol, acetone, or hydrophilic solvent carrier, reducing the potential for interference with the polymerization process.
6) Ensure that the adhesive is thoroughly light-cured prior to composite restoration placement to avoid displacement of uncured adhesive during placement.
Figure 8a. Veneer preparation with surface consisting of enamel (pre-operative)
Figure 8b. Veneer case, prep
Figure 9. Molar preparation surface mainly of dentin for self-etch adhesive
Courtesy of Dr. Walter Dias

6 www.ineedce.com
Mechanisms of action — enamel and dentinSelf-etch adhesive systems are available in a range of acidi-ties, from low pH (<1) through mild pH (≥2) variants. As with etch-and-rinse adhesive systems, the mechanism of adhesion is thought to be a combination of mechanical and/or chemical retention. Low-pH self-etch systems result in a hybrid layer that mimics the hybrid later formed with etch-and-rinse adhesives, producing deep resin tags. Mild-pH self-etch adhesives have shallower resin tags — the hydroxy-apatite is not completely demineralized — and it is believed that retention may be partly due to a chemical interaction between the monomer and the hydroxyapatite crystal.25
As the self-etch adhesives are moisture forgiving, they are particularly useful in difficult-to-isolate areas or with difficult patients. However, self-etch adhesives generally contain water in addition to monomers in their formula-tion. This implies that it is more critical to ensure that the drying of the adhesive after application is effectively completed. In addition, the presence of moisture in the formulation requires special attention to shelf stability on the part of the manufacturers, making the stability of some products less certain than etch-and-rinse systems.26 Since self-etch adhesive systems demineralize and penetrate the dentin at the same time, there is no concern over incom-plete penetration and residual gaps within demineralized dentin. Due to the milder acidity of the self-etching adhe-sives, the removal of the smear layer is often less complete (Figure 10), so the dentinal tubules may not be as open as in the case of the etch-and-rinse systems. This is thought to reduce the risk of postoperative sensitivity, although the restorative technique is perhaps the key to reduced post-operative sensitivity. 27
Figure 10. Self-etch and etch-and-rinse adhesives
The main disadvantage of self-etch adhesive systems is that the enamel must be instrumented to provide an ef-fective etch. Self-etch adhesives typically do not provide as high an enamel bond compared to etch-and-rinse adhe-sives.28,29,30 In some cases, self-etch systems demonstrated a higher incidence of marginal staining on enamel margins, while the dentin margins were acceptable (e.g., posterior/more extensive preparations). Self-etch adhesives thus may be preferred over the etch-and-rinse adhesives if the
remaining enamel has been instrumented and if the surface area to be bonded consists mainly of dentin. They may also be a better choice if sustained isolation from oral fluids is likely to be a problem.
Newer Adhesive DevelopmentsIn the last decade, most new developments in dental adhesives have been focused on simplifying the components required for the bonding systems and improving performance of the resulting self-etching adhesives. The true one-bottle self-etch systems have now evolved to only one material which is ap-plied to the tooth, with no mixing required. Some of the newer systems have modified the self-etch ingredients so as to result in improvements in the products’ shelf lives, with diminished hydrolysis in the package. As noted above, while the quality of dentin adhesion with these self-etch systems is comparable to the etch-and-rinse adhesives, the enamel bonding of these systems still falls short of values for bond strengths achieved in the laboratory using a phosphoric acid etch system.
The self-etch systems remain popular due to the lack of concern regarding the technique used with moist dentin. The moist bonding technique has been repeatedly shown to augment bond strengths of ethanol- and acetone-based
Techniques to maximize self-etch adhesive performance
1) Enamel, if present, should be beveled to improve retention.
2) The surfaces to be bonded should be clean and debris-free to prevent contamination of the adhesive, since there is no rinsing step that would remove any contaminants.
3) If using a multidose, single-bottle adhesive, the amount required should be dispensed immediately prior to use in order to reduce the risk of solvent loss, which could potentially result in phase separation of monomer and water. Using a unit-dose package helps to avoid this problem and also provides an ap-propriate amount of adhesive for use.
4) Apply the self-etch adhesive to the enamel first, followed by application to the dentin. Some products recommend agitation of the adhesive to enhance its penetration.
5) Do not use a separate etchant on the dentin prior to using self-etch adhesives. While it may be believed that this would improve the bond to dentin, self-etch adhesives are not de-signed to work on etched dentin. The result would be clinically undesirable and could potentially result in catastrophic failure of the restoration. If using a separate etchant on enamel, great care must be taken to avoid its contact with dentin and to thor-oughly rinse it off prior to the use of self-etch adhesives.
6) If using a one-step self-etch adhesive, apply multiple appli-cations to help ensure adequate coating and penetration.
7) Thoroughly dry the adhesive (with a gentle stream of air) once it has been placed, to ensure removal of any volatile sol-vent and prevent interference with polymerization.
8) Light-cure the adhesive prior to placing the composite.
www.ineedce.com 7
etch-and-rinse adhesives, while low bond strengths have been associated with excessively air-dried dentin in the etch-and-rinse materials.31,32,33,34 The major reason for this is presumed to be the effect of collapsing the collagen net-work at the bonding interface.35,36 The collapsed collagen prevents complete infiltration of the resin monomers into the demineralized dentin, leading to gaps and voids within the adhesive interface.
As the first new etch-and-rinse adhesive system since 2000, XP Bond (Dentsply/Caulk) has shown promise, as it is relatively insensitive to the amount of residual dentin mois-ture. This characteristic can effectively widen the window of opportunity for bonding to demineralized dentin, and can generate a system with excellent dentin adhesion under a wide range of clinical conditions, with the reliability of an enamel bond generated through phosphoric acid conditioning.
This etch-and-rinse adhesive contains two resin-adhesion promoters: the phosphoric acid ester monomer dipentaeryth-ritol pentacrylate-phosphoric acid (PENTA) and butan-1,2,3,4-tetracarboxylic acid, di-2-hydroxyethyl methacrylate ester (TCB), a monomer with two carboxylic acid groups. Recent Raman spectroscopy investigations have shown evidence of the formation of a covalent bond between the PENTA ester group and the calcium in dentin and enamel (Figure 11).37
Figure 11. Covalent bond between PENTA ester group and calcium ions
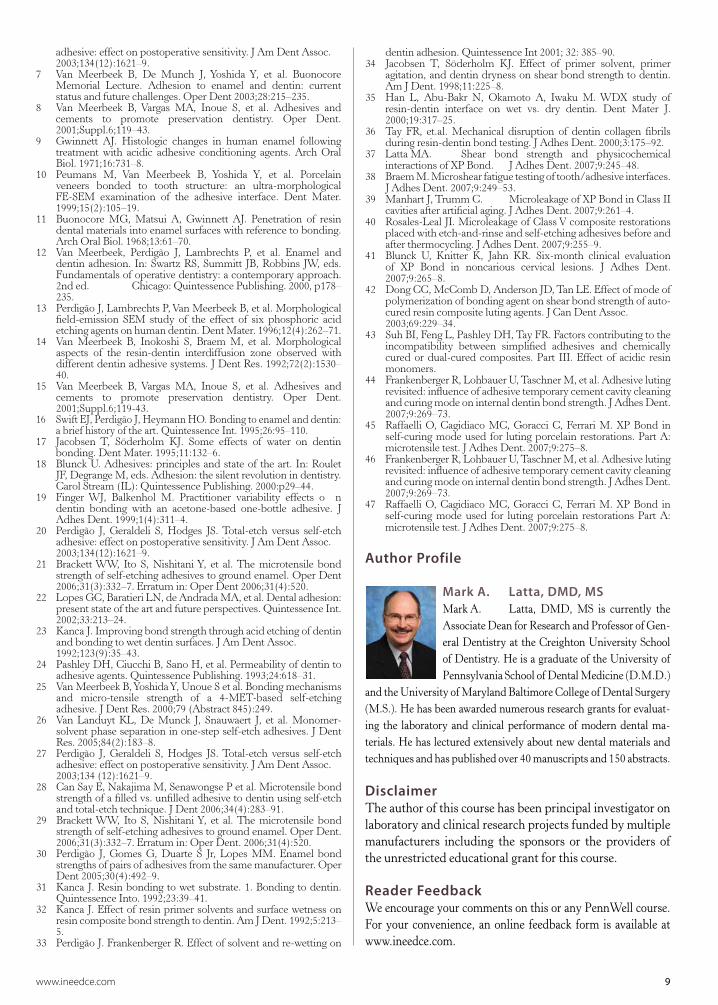
In addition to the adhesive promoting monomers, it uses tertiary-butanol as the solvent carrier for the adhesive resin mixture. The chemical structure of this alcohol seems to impart unique properties to the adhesive formulation when applied to moist or dry dentin. Figures 12 and 13 represent, respectively, the scanning electron micrographs (SEMs) of the adhesive dentin interface of OptiBond Solo (an ethanol-based system) and XP Bond applied to moist dentin. A fully infiltrated dentin/mineral/resin hybrid layer is seen with both materials.
In Figure 14, OptiBond Solo was applied to overdried dentin. The hybrid layer is incompletely formed, with gaps and voids at the adhesive/dentin interface. Figure 15 shows XP Bond applied to overdried dentin, and the hybrid layer which results cannot be distinguished from that formed on moist dentin. Figure 16 shows a transmission electron micrograph of XP Bond applied to overdried dentin. The electron-dense band at the top of the hybrid layer repre-sents the collapsed collagen layer. The XP Bond was able to completely infiltrate and demineralize the dentin below the collapsed layer of collagen. Numerous laboratory evalu-ations38,39,40 and early clinical results41 show great promise of the new etch-and-rinse XP Bond adhesive system.
Figure 12. SEM of OptiBond Solo applied to moist dentin
Image courtesy of Dr. Jorge Perdigão
Figure 13. SEM of XP Bond applied to moist dentin
Image courtesy of Dr. Jorge Perdigão
Figure 14. SEM of OptiBond Solo applied to overdried dentin
Image courtesy of Dr. Jorge Perdigão
Dy = DyractAD = AdhesiveH = Hybrid
AD
H
Dy
Gaps

8 www.ineedce.com
Use of Resin Adhesives with Resin CementsUse of resin adhesives is an important part of numer-ous clinical procedures when light-cured, self-cured, or dual-cured resin restoratives or cements are employed. The indications include cementing posts; resin core build-ups; and cementing ceramic veneers, inlays, and onlays as well as certain full-crown ceramics. If exclusively light-cured materials are used, such as when cementing a ceramic veneer, the resin adhesive can be light cured alone if a light cured-only resin cement base follows. However, there are known incompatibilities between some acid containing adhesives and self-cured and/or dual-cured resin cements or restoratives.42 It has been suggested that a small amount of residual acidic resin monomer can deactivate the tertiary amine that promotes the dark-cure polymerization of the resin cement or restorative.43 It is for this reason that it is suggested that, unless specifically designed for use with a dual and/or self-cure resin cement or restorative, self-etching adhesives should be avoided. In fact, even with etch-and-rinse adhesive systems, mixing different manu-facturers’ materials should be avoided to prevent incompat-ibility issues between the interface of the adhesive and the dual and/or self-cure restorative or cement material.
Several manufacturers provide a self-curing activator to be mixed with their respective adhesive (etch-and-rinse or
self-etch) to ensure full polymerization of a self- or dual-curing material. The primary function of these activators is not to promote the polymerization of the adhesive itself, but to provide a chemical environment at the interface between the adhesive and the self or dual-cured resin restorative ma-terial that promotes the curing of the interface, thus securely bonding the adhesive and restorative.
The new etch-and-rinse adhesive, when mixed with its specifically designed self-cure activator (SCA) in con-junction with Calibra cement, demonstrates some unique properties compared to other activated adhesives with their respective resin cements. When the self-cure-activated adhesive and the resin cement are light-cured (dual-cure mode for the Calibra), the enamel and dentin bond values are equal to or higher than those of other similar systems.44,45 However, even in the pure chemical self-cure mode (when no light is introduced), the self-cure-activated adhesive and self-cured cement form bond strengths to dentin that are higher than those achievable with similar dual-curing conventional systems.46,47
SummaryDental adhesives are used for a wide variety of applications. They are available as etch-and-rinse systems (also known as “total-etch” systems) and self-etch systems. Both systems result in etching of the tooth surface, and mechanical and/or chemical retention of the restoration or device upon curing of the adhesive. The adhesive system selected has implica-tions for the technique used as well as for the quality of the bonding. Enamel bonding is superior with etch-and-rinse adhesive systems, while self-etch systems may be more suitable for restorations with large areas of dentin. Careful consideration of several factors is essential in making the selection of an adhesive system. Mixing different manufac-turers’ materials (for example, adhesives and resin cements) should be avoided, as there are potential incompatibilities among the respective chemistries. Only adhesive systems specifically designed for the specific resin cement should be used. Recently, newer adhesives have been introduced that focus on simplifying and improving the performance of adhesive systems for bonding of both enamel and dentin.
References 1 Perdigão J, Lopes M. Dentin bonding — state of the art 1999.
CompendContinEducDent.1999Dec;20(12):1151–8,1160–2.2 BuonocoreMG.Asimplemethodofincreasingtheadhesionof
acrylicfillingmaterialstoenamelsurfaces.JDentRes.1955;34:849–53.
3 Cueto EI, Buonocore MG. Sealing of pits and fissures with anadhesiveresin:itsuseincariesprevention.JAmDentAssoc.1967;73:121–8.
4 Buonocore MG, Matsui A, Gwinnett AJ. Penetration of resindentalmaterialsintoenamelsurfaceswithreferencetobonding.ArchOralBiol.1968;13(1):61–70.
5 WiecskowskiG,YuXY,DavisEL,etal.Microleakageinvariousdentin bonding agent/composite resin systems. Oper Dent.1992;(Suppl.5):62–7.
6 Perdigão J, Geraldeli S, Hodges JS. Total-etch versus self-etch
Figure 15. SEM of XP Bond applied to overdried dentin
Image courtesy of Dr. Jorge Perdigão
Figure 16. Tranmission electron micrograph of XP Bond applied to overdried dentin
Image courtesy of Dr. Jorge Perdigão
Dy = DyractAD = AdhesiveH = HybridTag = Resin Tag
HH H
AD
Dy
Tag
www.ineedce.com 9
adhesive:effectonpostoperativesensitivity.JAmDentAssoc.2003;134(12):1621–9.
7 Van Meerbeek B, De Munch J, Yoshida Y, et al. BuonocoreMemorial Lecture. Adhesion to enamel and dentin: currentstatusandfuturechallenges.OperDent2003;28:215–235.
8 Van Meerbeek B, Vargas MA, Inoue S, et al. Adhesives andcements to promote preservation dentistry. Oper Dent.2001;Suppl.6;119–43.
9 Gwinnett AJ. Histologic changes in human enamel followingtreatment with acidic adhesive conditioning agents. Arch OralBiol.1971;16:731–8.
10 Peumans M, Van Meerbeek B, Yoshida Y, et al. Porcelainveneers bonded to tooth structure: an ultra-morphologicalFE-SEM examination of the adhesive interface. Dent Mater.1999;15(2):105–19.
11 Buonocore MG, Matsui A, Gwinnett AJ. Penetration of resindentalmaterialsintoenamelsurfaceswithreferencetobonding.ArchOralBiol.1968;13:61–70.
12 Van Meerbeek, Perdigão J, Lambrechts P, et al. Enamel anddentinadhesion. In:SwartzRS,Summitt JB,Robbins JW,eds.Fundamentalsofoperativedentistry:acontemporaryapproach.2nded. Chicago:QuintessencePublishing.2000,p178–235.
13 PerdigãoJ,LambrechtsP,VanMeerbeekB,etal.Morphologicalfield-emission SEM study of the effect of six phosphoric acidetchingagentsonhumandentin.DentMater.1996;12(4):262–71.
14 Van Meerbeek B, Inokoshi S, Braem M, et al. Morphologicalaspects of the resin-dentin interdiffusion zone observed withdifferentdentinadhesivesystems.JDentRes.1992;72(2):1530–40.
15 Van Meerbeek B, Vargas MA, Inoue S, et al. Adhesives andcements to promote preservation dentistry. Oper Dent.2001;Suppl.6;119-43.
16 SwiftEJ,PerdigãoJ,HeymannHO.Bondingtoenamelanddentin:abriefhistoryoftheart.QuintessenceInt.1995;26:95–110.
17 Jacobsen T, Söderholm KJ. Some effects of water on dentinbonding.DentMater.1995;11:132–6.
18 BlunckU.Adhesives:principlesandstateof theart. In:RouletJF,DegrangeM,eds.Adhesion:thesilentrevolutionindentistry.CarolStream(IL):QuintessencePublishing.2000:p29–44.
19 Finger WJ, Balkenhol M. Practitioner variability effects o ndentin bonding with an acetone-based one-bottle adhesive. JAdhesDent.1999;1(4):311–4.
20 Perdigão J, Geraldeli S, Hodges JS. Total-etch versus self-etchadhesive:effectonpostoperativesensitivity.JAmDentAssoc.2003;134(12):1621–9.
21 BrackettWW, Ito S, NishitaniY, et al.The microtensile bondstrengthofself-etchingadhesivestogroundenamel.OperDent2006;31(3):332–7.Erratumin:OperDent2006;31(4):520.
22 LopesGC,BaratieriLN,deAndradaMA,etal.Dentaladhesion:presentstateoftheartandfutureperspectives.QuintessenceInt.2002;33:213–24.
23 KancaJ.Improvingbondstrengththroughacidetchingofdentinandbondingtowetdentinsurfaces.JAmDentAssoc.1992;123(9):35–43.
24 PashleyDH,CiucchiB,SanoH,etal.Permeabilityofdentintoadhesiveagents.QuintessencePublishing.1993;24:618–31.
25 VanMeerbeekB,YoshidaY,UnoueSetal.Bondingmechanismsand micro-tensile strength of a 4-MET-based self-etchingadhesive.JDentRes.2000;79(Abstract845):249.
26 Van Landuyt KL, De Munck J, Snauwaert J, et al. Monomer-solventphaseseparationinone-stepself-etchadhesives.JDentRes.2005;84(2):183–8.
27 Perdigão J, Geraldeli S, Hodges JS. Total-etch versus self-etchadhesive:effectonpostoperativesensitivity.JAmDentAssoc.2003;134(12):1621–9.
28 CanSayE,NakajimaM,SenawongsePetal.Microtensilebondstrengthofafilledvs.unfilledadhesivetodentinusingself-etchandtotal-etchtechnique.JDent2006;34(4):283–91.
29 BrackettWW, Ito S, NishitaniY, et al.The microtensile bondstrengthofself-etchingadhesivestogroundenamel.OperDent.2006;31(3):332–7.Erratumin:OperDent.2006;31(4):520.
30 Perdigão J, Gomes G, Duarte S Jr, Lopes MM. Enamel bondstrengthsofpairsofadhesivesfromthesamemanufacturer.OperDent2005;30(4):492–9.
31 KancaJ.Resinbonding towetsubstrate.1.Bonding todentin.QuintessenceInto.1992;23:39–41.
32 KancaJ.Effectofresinprimersolventsandsurfacewetnessonresincompositebondstrengthtodentin.AmJDent.1992;5:213–5.
33 PerdigãoJ.FrankenbergerR.Effectofsolventandre-wettingon
dentinadhesion.QuintessenceInt2001;32:385–90.34 Jacobsen T, Söderholm KJ. Effect of primer solvent, primer
agitation,anddentindrynessonshearbondstrengthtodentin.AmJDent.1998;11:225–8.
35 Han L, Abu-Bakr N, Okamoto A, Iwaku M. WDX study ofresin-dentin interface on wet vs. dry dentin. Dent Mater J.2000;19:317–25.
36 Tay FR, et.al. Mechanical disruption of dentin collagen fibrilsduringresin-dentinbondtesting.JAdhesDent.2000;3:175–92.
37 LattaMA. Shear bond strength and physicochemicalinteractionsofXPBond. JAdhesDent.2007;9:245–48.
38 BraemM.Microshearfatiguetestingoftooth/adhesiveinterfaces.JAdhesDent.2007;9:249–53.
39 ManhartJ,TrummC. MicroleakageofXPBondinClassIIcavitiesafterartificialaging.JAdhesDent.2007;9:261–4.
40 Rosales-LealJI.MicroleakageofClassVcompositerestorationsplacedwithetch-and-rinseandself-etchingadhesivesbeforeandafterthermocycling.JAdhesDent.2007;9:255–9.
41 Blunck U, Knitter K, Jahn KR. Six-month clinical evaluationof XP Bond in noncarious cervical lesions. J Adhes Dent.2007;9:265–8.
42 DongCC,McCombD,AndersonJD,TanLE.Effectofmodeofpolymerizationofbondingagentonshearbondstrengthofauto-curedresincompositelutingagents.JCanDentAssoc.2003;69:229–34.
43 SuhBI,FengL,PashleyDH,TayFR.Factorscontributingtotheincompatibility between simplified adhesives and chemicallycured or dual-cured composites. Part III. Effect of acidic resinmonomers.
44 FrankenbergerR,LohbauerU,TaschnerM,etal.Adhesivelutingrevisited:influenceofadhesivetemporarycementcavitycleaningandcuringmodeoninternaldentinbondstrength.JAdhesDent.2007;9:269–73.
45 Raffaelli O, Cagidiaco MC, Goracci C, Ferrari M. XP Bond inself-curing mode used for luting porcelain restorations. Part A:microtensiletest.JAdhesDent.2007;9:275–8.
46 FrankenbergerR,LohbauerU,TaschnerM,etal.Adhesivelutingrevisited:influenceofadhesivetemporarycementcavitycleaningandcuringmodeoninternaldentinbondstrength.JAdhesDent.2007;9:269–73.
47 Raffaelli O, Cagidiaco MC, Goracci C, Ferrari M. XP Bond inself-curing mode used for luting porcelain restorations Part A:microtensiletest.JAdhesDent.2007;9:275–8.
Author Profile
Mark A. Latta, DMD, MSMark A. Latta, DMD, MS is currently the Associate Dean for Research and Professor of Gen-eral Dentistry at the Creighton University School of Dentistry. He is a graduate of the University of Pennsylvania School of Dental Medicine (D.M.D.)
and the University of Maryland Baltimore College of Dental Surgery (M.S.). He has been awarded numerous research grants for evaluat-ing the laboratory and clinical performance of modern dental ma-terials. He has lectured extensively about new dental materials and techniques and has published over 40 manuscripts and 150 abstracts.
DisclaimerThe author of this course has been principal investigator on laboratory and clinical research projects funded by multiple manufacturers including the sponsors or the providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.
10 www.ineedce.com
Questions1. _________ of the commonly performed
tasks in dentistry have benefited from the development of dental adhesives.a. Noneb. A fewc. Mostd. All
2. Dental adhesives were originally de-veloped as an extension of _________.a. industrial adhesives used to help paint and
resin coatings bond to plasticb. industrial adhesives used to help paint and
resin coatings bond to metalc. mining adhesives used to help fix explosives to
coal seamsd. none of the above
3. The first person to propose the applica-tion of adhesion technology in dentistry is widely considered to have been _____.a. Dr. Michael Buenavistab. Dr. Ian Flemingc. Dr. Michael Buonocored. none of the above
4. By the 1990s, _________.a. multi-step adhesives were available b. single-step adhesives were availablec. the concept of the “hybrid layer” was acceptedd. all of the above
5. It is believed that dental adhesives _________ when used appropriately.a. may reduce postoperative sensitivityb. can reduce marginal staining and microleakage c. can reinforce weakened dentin or enameld. all of the above
6. Both etch-and-rinse and self-etch adhe-sive systems result in a unique interface at the juncture of the _________.a. cementum surface and the etchantb. tooth surface and the etchantc. enamel surface and the etchantd. tooth surface and the adhesive
7. Etch-and-rinse adhesives are available as _________.a. one-, two- and three-step systemsb. two- and three-step systemsc. one- and three-step systemsd. all of the above
8. Dental adhesives promote _________ of tooth structure.a. corticationb. conservationc. destructiond. none of the above
9. The basic mechanism for enamel and dentin bonding using etch-and-rinse systems consists of _________.a. demineralization of the surface by the acid b. curing of the adhesive monomers to form
resin tags that microscopically provide a mechanical bond
c. penetration of the adhesive monomers into the microscopic spaces created by the etchant
d. all of the above10. Acid etching of enamel creates
_________ that is available for resin penetration. a. a porous layer 5 μm to 15 μm in depthb. a porous layer 5 μm to 25 μm in depthc. a porous layer 5 μm to 40 μm in depthd. a porous layer 5 μm to 50 μm in depth
11. Self-etch adhesives generally demonstrate _________ adhesion to enamel than/as to dentin.a. poorerb. the samec. betterd. none of the above
12. Acid etching of dentin bonding creates _________ that is available for adhesion.a. a demineralized surface 3 μm to 5 μm in depthb. a demineralized surface 5 μm to 15 μm in depthc. a demineralized surface 5 μm to 25 μm in depthd. a demineralized surface 10 μm to 15 μm in
depth13. Failure to remove the smear
layer _________.a. encourages resin adhesion b. reduces dentin permeabilityc. is immateriald. a and b
14. The primer in three-step etch-and-rinse systems is used to displace residual moisture, thus creating a surface to which the _________ bond-ing resin can adhere.a. Hydrophobicb. hydroponicc. hydrophilicd. none of the above
15. One key factor that influences the performance of etch-and-rinse systems includes _________.a. the use of phosphoric acid of at least
40% concentrationb. ensuring that the dentin is dry when applying
primer and adhesivec. the thorough removal of the etchant prior
to bondingd. all of the above
16. A recent study by _________ found no differences in postoperative sen-sitivity between patients treated with self-etch adhesives and those treated with etch-and-rinse adhesives. a. Bilbão et al.b. Persipany et al.c. Perdigão et al.d. none of the above
17. If the enamel to be etched comprises mostly intact or unin-strumented enamel, _________. a. the choice of a self-etch system is preferred b. the choice of an etch-and-rinse system
is preferredc. both adhesive systems are equald. none of the above
18. Self-etch adhesives are available as _________ systems.a. one-stepb. two-stepc. three-stepd. a and b
19. Self-etch adhesives _________.a. do not require a separate etching procedureb. are more tolerant of the presence of moisture
on the preparationc. eliminate the potential for over-etching when
treating dentind. all of the above
20. Low-pH self-etch systems result in a _________that mimics the _________ formed with etch-and-rinse adhesives, producing deep resin tags.a. uniform layerb. segregated areac. hybrid layerd. none of the above
21. Mild-pH self-etch adhesives have _________ resin tags.a. shallowerb. similarc. deeperd. none of the baove
22. With self-etch adhesive systems, _____.a. the dentinal tubules may not be as open as they
are with etch-and-rinse systemsb. demineralization and penetration of the dentin
occur at the same timec. the removal of the smear layer is often
less completed. all of the above
23. Self-etch adhesives typically provide a _________ enamel bond compared to etch-and-rinse adhesives.a. lowerb. similarc. higherd. none of the above
24. Use of a separate etchant on the den-tin prior to use of self-etch adhesives may _________ the bond to dentin.a. decreaseb. maintainc. improved. none of the above
25. In the last decade, most new develop-ments in dental adhesives have been focused on _________.a. increasing the concentration of etchant for
faster etching b. simplifying the components required for the
bonding systemsc. improving performance of the resulting
self-etching adhesivesd. b and c
26. Low bond strengths have been associated with _________ dentin in the etch-and-rinse materials.a. air-driedb. excessively air-driedc. excessive preparationd, none of the above
27. The primary function of self-activators that are mixed with their respective adhesive is to ________.a. provide a chemical environment at the interface
between the adhesive and the self or dual-cured resin restorative material that promotes the curing of the interface
b. provide a mechanical environment that secures the adhesive interface
c. reduce curing at the interface of the adhesive and tooth
d. none of the above28. Mixing different manufacturers’
materials when using resin adhesives _________.a. is of no consequence b. should be done to promote compatibility
between the interface of the adhesive and the dual and/or self-cure restorative or cement material
c. should be avoided to prevent incompat-ibility issues between the interface of the adhesive and the dual and/or self-cure restorative or cement material
d. none of the above29. The self-etch systems r _________
popular due to the lack of concern regarding the technique used with moist dentin.a. are no longerb. are more c. remaind. none of the above
30. The key to reduced postoperative sensitivity is perhaps the _________.a. preparation being maximizedb. restorative techniquec. pre-operative techniqued. a and c
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
Mailcompletedanswersheetto
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O.Box116,Chesterland,OH44026orfaxto:(440)845-3447
For immediate results, go to www.ineedce.com and click on the button “take tests Online.” answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
�Paymentof$49.00isenclosed.(Checks and credit cards are accepted.)
Ifpayingbycreditcard,pleasecompletethefollowing: MC Visa AmEx Discover
Acct.Number:______________________________
Exp.Date:_____________________
Charges on your statement will show up as PennWell
ANSWER SHEET
ClinicalPerspectivesonCurrentDentalAdhesives
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP:
Telephone:Home() Office()
Requirementsforsuccessfulcompletionofthecourseandtoobtaindentalcontinuingeducationcredits:1)Readtheentirecourse.2)Completeallinformationabove.3)Completeanswersheetsineitherpenorpencil.4)Markonlyoneanswerforeachquestion.5)Ascoreof70%onthistestwillearnyou2CEcredits.6)CompletetheCourseEvaluationbelow.7)MakecheckpayabletoPennWellCorp.For Questions Call 216.398.7822
Educational Objectives1. Listanddescribethetypesofdentaladhesivesystemsavailable.
2. Describetheclinicalapplicationofetch-and-rinsedentaladhesivesandthetypesofcasesforwhichtheseare
bestsuited.
3. Describetheclinicalapplicationofself-etchdentaladhesivesandthetypesofcasesforwhichthesearebestsuited.
4. Describetheneweradhesivesthathavebeendevelopedandtheirbenefits.
Course EvaluationPleaseevaluatethiscoursebyrespondingtothefollowingstatements,usingascaleofExcellent=5toPoor=0.
1.Weretheindividualcourseobjectivesmet? Objective#1:YesNo Objective#3:YesNo
Objective#2:YesNo Objective#4:YesNo
2.Towhatextentwerethecourseobjectivesaccomplishedoverall? 5 4 3 2 1 0
3.Pleaserateyourpersonalmasteryofthecourseobjectives. 5 4 3 2 1 0
4.Howwouldyouratetheobjectivesandeducationalmethods? 5 4 3 2 1 0
5.Howdoyouratetheauthor’sgraspofthetopic? 5 4 3 2 1 0
6.Pleaseratetheinstructor’seffectiveness. 5 4 3 2 1 0
7.Wastheoveralladministrationofthecourseeffective? 5 4 3 2 1 0
8.Doyoufeelthatthereferenceswereadequate? Yes No
9.Wouldyouparticipateinasimilarprogramonadifferenttopic? Yes No
10.Ifanyofthecontinuingeducationquestionswereunclearorambiguous,pleaselistthem.
___________________________________________________________________
11.Wasthereanysubjectmatteryoufoundconfusing?Pleasedescribe.
___________________________________________________________________
___________________________________________________________________
12.Whatadditionalcontinuingdentaleducationtopicswouldyouliketosee?
___________________________________________________________________
___________________________________________________________________
AUTHOR DISCLAIMERThe author of this course has been principal investigator on laboratory and clinical research projects funded by the sponsors or the providers of the unrestricted educational grant for this course.
SPONSOR/PROVIDERThis course was made possible by an educational grant from DENTSPLY Caulk. No manufacturer or third party has had any input into the development of course content. All content has been derived from references listed, and or the opinions of clinicians. Please direct all questions pertaining to PennWell or the administration of this course to Machele Galloway, 1421 S. Sheridan Rd., Tulsa, OK 74112 or [email protected].
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification forms will be mailed within two weeks after taking an examination.
EDUCATIONAL DISCLAIMERThe opinions of efficacy or perceived value of any products or companies mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of PennWell.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 2 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $49.00 to $110.00.
Many PennWell self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB) and can be used by dental assistants who are DANB Certified to meet DANB’s annual continuing education requirements. To find out if this course or any other PennWell course has been approved by DANB, please contact DANB’s Recertification Department at 1-800-FOR-DANB, ext. 445.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2008 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
AGD Code 017
11 Customer Service 216.398.7822 www.ineedce.com