pdt slide english
DESCRIPTION
its all about PDT anaesthesiologyTRANSCRIPT
Fatal complications of percutaneous dilatational
tracheostomy Peter Gilbey, MDa,b,⁎
aThe Otolaryngology, Head and Neck Surgery Unit, Ziv Medical Center, Zefat, Israel bBar-Ilan University Faculty of Medicine in the Galilee, Israel
Received 19 June 2012
Tutor : dr.Erica Gilda Simanjuntak,SpAnPresentated by : Astri Marsa Zulkarnaen,S.Ked

Abstract
Objectives
Fatal complications of percutaneous dilatational tracheostomy (PDT) are rare and intraoperative fatal complications of PDT even more so.
Methods
A review of all previously reported fatal complications of PDT was conducted in order to :
•examine the prevalent causes of death
•to attempt to recommend measures designed to prevent similar fatal complications in the future
Results
•Cases of death during or following PDT in which the technique is related to the cause of death have only been reported in a small number of cases.
•Almost all fatal complications of PDT result from vascular injury.

Conclusions
Any vascular pulsation palpated over the tracheostomy site mandates preoperative ultrasound or conversion to open surgical tracheostomy.
History of previous neck surgery, radiotherapy or unclear surgical anatomy should be regarded with caution.

If a difficult intubation or procedure is anticipated it may be preferable not to attempt PDT with a plan to convert to surgical tracheostomy if necessary but instead to perform surgical tracheostomy without attempting PDT.

Introduction
Percutaneous dilatational tracheostomy (PDT), first described by Ciaglia et al in 1985, is the placement of a tracheostomy tube without direct visualization of the trachea.
It is considered to be a minimally invasive procedure that is performed in the intensive care unit or at the patient's bedside.

Andvantages of PDT
The time required for performing bedside PDT is considerably shorter than that required for performing an open tracheostomy
eradication of scheduling difficulty associated with the operating room and anesthesiology teams.

Bedside PDT also prevents the necessity to transport critically ill patients requiring intensive monitoring to the operating room.
The cost of PDT is roughly half that of performing open surgical tracheostomy.
A meta-analysis of five studies comparing PDT with
surgical tracheostomy found similar overall complication
rates in the 2 groups.

Early Late
Bleeding development of granulation tissue resulting in airway stenosis
infection failure to decannulate or upper airway obstruction with respiratory
failure after decannulation
Pneumothorax tracheoesophageal fistula
technical failures and perioperative hypoxia due to tube obstruction or accidental
decannulation
tracheomalacia
tracheal stenosis
tracheoinnominate artery fistula (TIF)

Case report
Name : Mrs.K
Age : 64th
Chief complaint : > left abdominal pain
> left flank pain
> dyspnea
on going disease : She was diagnosed as suffering from left pneumonia and treated with intravenous antibiotics
Medical History : morbid obesity and elephantiasis of the lower limbs
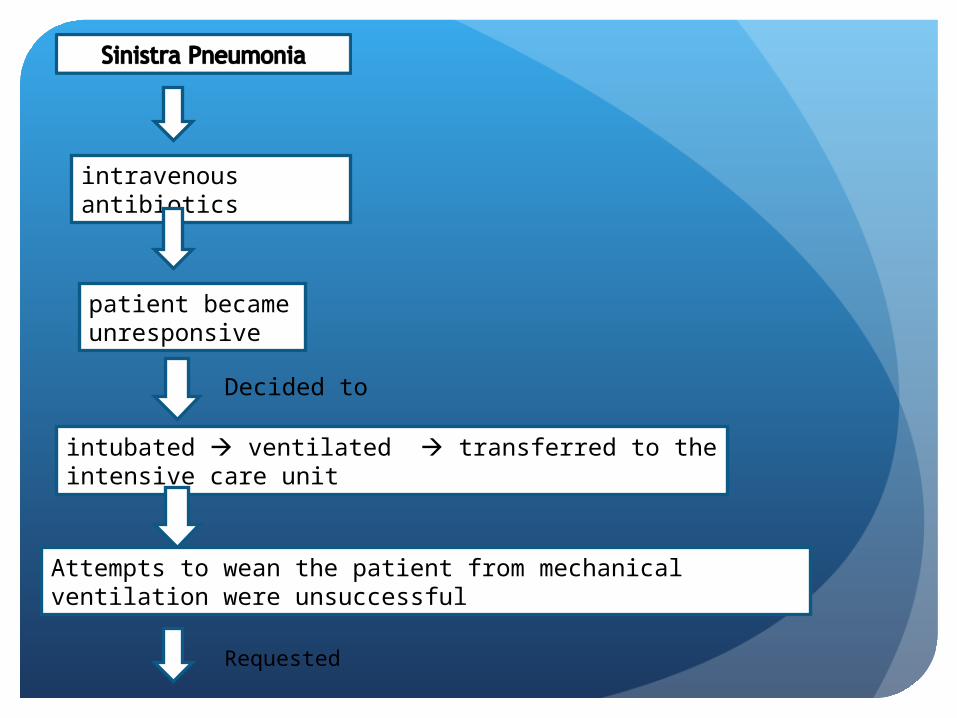
intravenous antibiotics
patient became unresponsive
Decided to
intubated ventilated transferred to the intensive care unit
Attempts to wean the patient from mechanical ventilation were unsuccessful
Requested

an elective tracheostomy
Due to the fact that the patient was morbidly obese with a short neck, a joint decision by the Intensive Care unit and the Otolaryngology, Head and Neck Surgery unit was made
transfer the patient to the operating room and not to perform a bedside procedure
in the operating room, the patient was re-evaluated by an otolaryngologist and an anesthesiologist
Despite the short neck the cricoid cartilage was palpated and a decision was made

to increase airway safety, a Cook Airway Exchange Catheter (Cook Critical Care. Bloomington, IN) was inserted into the trachea through the lumen of the endotracheal tube via a swivel connector
Attempt PDT
unsuccessful
Efficient jet ventilation through the airway exchange catheter was demonstrated
Attempts to reintubate over the tube exchanger ≠ berhasil
unsuccessful

further attempts to reintubate the patient and to ventilate with a laryngeal mask airway were ineffective
Final decision
attempt to perform an emergency cricothyroidotomy
via the opening in the anterior neck were not observed at any time during the procedure
The patient subsequently desaturated and expired
Post mortem examination was requested but refused by the family.

Discussion
In a recent survey of the membership of the American Academy of Otolaryngology, Head and Neck Surgery ,reported the number of catastrophic tracheostomy complications they had experienced during their career and the number of complications leading to death or permanent disability
55% of respondents reported caring for at least one patient with a catastrophic event related to a tracheostomy, accidental decannulation (34.3%) or bleeding (31.6%).

complication rates were

The most common Complications

Bleeding was the only early (within 1 week of the procedure) complication found to be significantly higher in the group of patients undergoing percutaneous tracheostomy

Minor bleeding during the performance of PDT has been reported to occur in fewer than 20% of cases.
Major bleeding occurred in fewer than 5% of cases and was usually venous.
Catastrophic hemorrhage is rare, usually delayed and in most cases is the result of a TIF

Fatal complications of PDT have only been reported in a small number of cases and fatal intraoperative complications of PDT are even less common.
Almost all result from vascular injury.
One case of intraoperative death during PDT resulting from loss of airway has been included in a national US survey of tracheostomy-related catastrophic events.

Ultrasound (US)
improve the safety profile of PDT
to identify the tracheal midline and the levels of the tracheal cartilages and is also of benefit in identifying overlying or vulnerable adjacent structures such as the thyroid gland and isthmus and blood vessels
Intraoperative tracheal endoscopy
can reduce the possibility of
paramedian or extratracheal
placement of the seeker needle
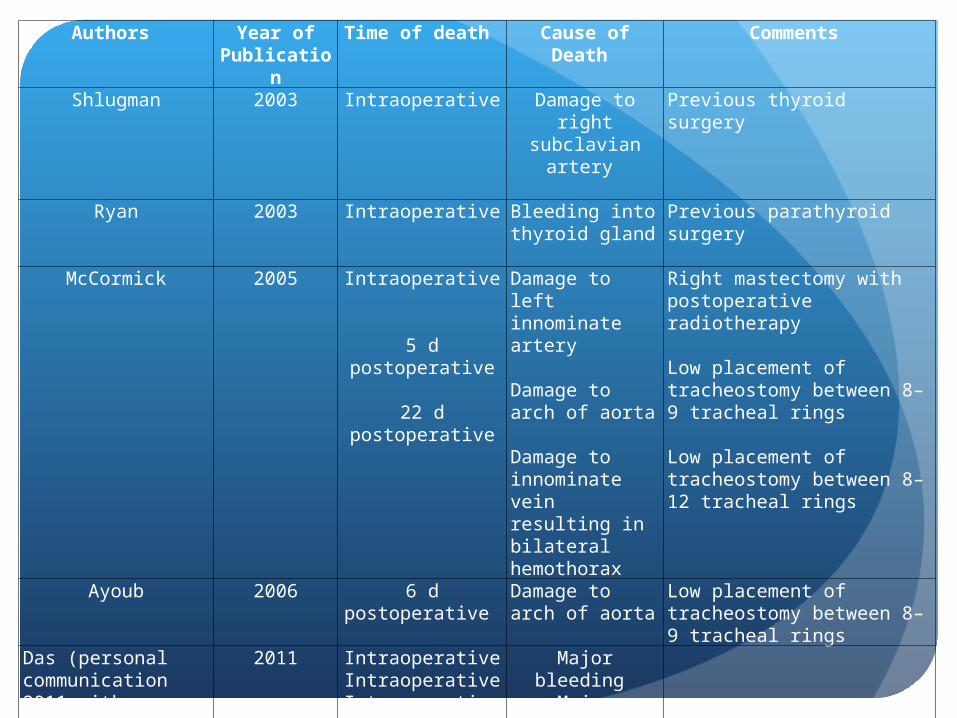
Authors Year of Publication
Time of death Cause of Death Comments
Shlugman 2003 Intraoperative Damage to right subclavian artery
Previous thyroid surgery
Ryan 2003 Intraoperative Bleeding into thyroid gland
Previous parathyroid surgery
McCormick 2005 Intraoperative
5 d postoperative
22 d postoperative
Damage to left innominate artery
Damage to arch of aorta
Damage to innominate vein resulting in bilateral hemothorax
Right mastectomy with postoperative radiotherapy
Low placement of tracheostomy between 8–9 tracheal rings
Low placement of tracheostomy between 8–12 tracheal rings
Ayoub 2006 6 d postoperative Damage to arch of aorta
Low placement of tracheostomy between 8–9 tracheal rings
Das (personal communication 2011 with author)
2011 Intraoperative IntraoperativeIntraoperative
Major bleeding Major bleeding
Airway loss
Present study 2012 Intraoperative Airway loss

Conclusion
Fatal complication of PDT is very rare
Fatal complications of PDT are extremely rare and usually result from vascular injury
US and/or intraoperative tracheal endoscopy seem to improve the safety profile of the procedure but are logistically demanding and probably not routinely required in all patients
Case selection is of great importance and patients with previous neck surgery or radiotherapy
if a difficult intubation or a difficult procedure are anticipated, it may be preferable not to attempt PDT with a plan to convert to surgical tracheostomy if necessary, but instead to perform surgical tracheostomy without attempting PDT
