lipoprotein metabolism - srm universityendogenous lipid transport) t1/2 vldl= 15-60min catabolism of...
TRANSCRIPT
Lipoprotein metabolism

LIPOPROTEINS
Spherical macromolecular complexes which help in the transport of TGL and cholesterol through blood stream between various tissues.
The lipoproteins consist of a core of hydrophobic lipids (cholesterol ester & TGL) surrounded by a shell of amphipathic lipids (PL & free cholesterol) along with proteins (apolipoproteins).


Lipoproteins in plasmaLipoproteins Source Diameter
(nm) Density(g/ml)
CompositionProtein% Lipid %
Main lipids
Apo
Chylomicrons Intestine 90-1000 <0.95 1-2 98-99 TGL B-48, A, C, E
VLDL Liver 30-90 0.95-1.006
7-10 90-93 TGL B-100, C-I, C-II
IDL VLDL 25-35 1.006-1.019
11 89 TGL, C B-100, E
LDL VLDL 20-25 1.019-1.063
21 79 C B-100
HDL Liver, intestineCM,VLDL
5-12 1.063-1.210
55 45 PL, C A-I, A-II, C-I, C-II, D, E
Cholesterol rich lipoproteins:LDLHDL
TGL rich lipoproteins:ChylomicronsVLDL

Apolipoproteins
• Integral : Apo B100, Apo B48• Peripheral : Apo AI, Apo AII, Apo CI,
Apo CII, Apo E
Functions of apolipoproteins
• Activates many enzymes in the lipoprotein metabolic pathways.
• Maintain the structural integrity of lipoprotein complex.• Facilitate the uptake of lipoproteins in cells through their
recognition by specific cell surface receptors.• Can act as lipid transfer proteins.• Apoproteins are amphipathic helices. Charged amino
acids on one side of α-helix and neutral amino acids on the other. (Neutral side interacts with lipid).

Key enzymes of lipid transport• Lipoprotein lipase: synthesized by adipose tissue and
striated muscle. Produced by parenchymal cells, secreted and transported to the endothelial surface of blood capillaries where it is bound to heparan sulfate. Hydrolyzes TGL rich lipoproteins.
• Hepatic lipase: formed in hepatocytes, transported to hepatic endothelial cells. Acts on TGL in IDL. Also on PL & TGL in HDL.
• LCAT: synthesized by liver and attached to HDL in blood. Concerned with removal of excess cholesterol from peripheral tissues.

Key Receptors in Lipoprotein Metabolism
• LDL receptor: catabolism of LDL, apoB ligand
• ATP-binding cassette transporter A1 (ABCA1) : transports excess cholesterol from cells to poorly lipidated preβ-HDL or apo-A1.
• Scavenger receptor A1 (SR-A1): uptake of oxidized and modified LDL by macrophages
• SR-B1 receptor: selective uptake of excess cholesterol from tissues into HDL as well as from HDL when it reaches liver.

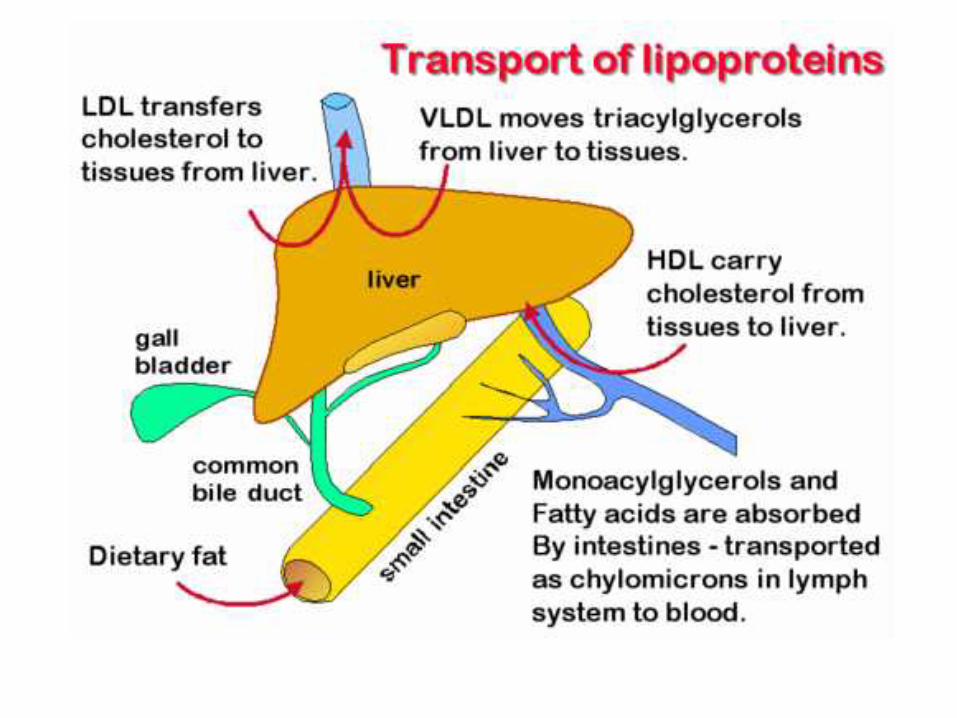
Lipid transport
• Exogenous lipid transport: involves chylomicron metabolism, aided by HDL
• Endogenous lipid transport: involves metabolism of VLDL and HDL.


Chylomicrons metabolism(Exogenous lipid transport)


Formation of chylomicrons
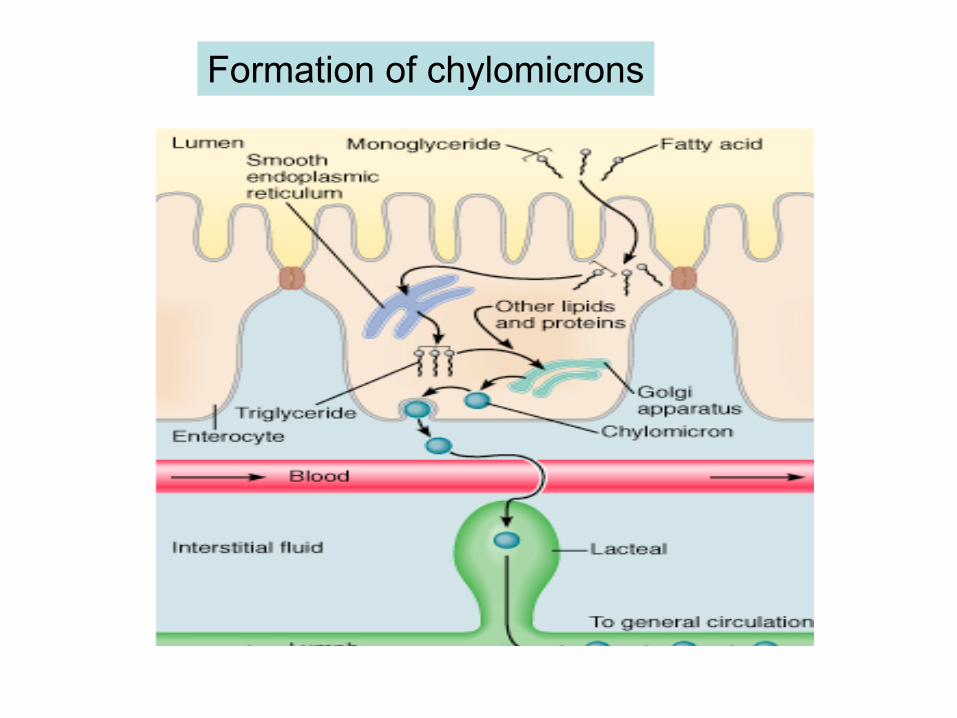
Formation of chylomicrons



Mature
Catabolism of chylomicronst1/2=5-10min
Skeletal muscle & adipose tissue

Chylomicron metabolism
• CM are assembled in the intestinal mucosa as a means to transport dietary cholesterol and TGL(exogenous lipids) to the rest of the body.
• The apolipoproteins that predominate before the CM enter the circulation include apoB-48 and apoA-I, -A-II and IV.
• CM leave the intestine via the lymphatic system and enter the circulation at the left subclavian vein.

Chylomicron metabolism
• In the bloodstream, CM acquire apoC-II and apoE from plasma HDLs.
• In the capillaries of adipose tissue and muscle, the fatty acids of CM are removed from the TGL by action of LPL.
• The apoC-II in the chylomicrons activates LPL in the presence of phospholipid.
• The FFA are then absorbed by the tissues. Glycerol is returned, via the blood, to the liver and kidneys to take part in gluconeogenesis.
Chylomicron metabolism
• During the removal of FA, a substantial portion of PL, apoA and apoC is transferred to HDLs.
• The loss of apoC-II prevents LPL from further degrading the CM remnants.
• CM remnants containing primarily cholesterol, apoE and apoB-48 are taken up by the liver through interaction with the CM remnant receptor.
• The recognition of CM remnants by the hepatic remnant receptor requires apoE.
• CM functions to deliver dietary TGL to adipose tissue and muscle and dietary cholesterol to the liver.
VLDL, LDL metabolismHDL metabolism
(Endogenous lipid transport)


Catabolism of VLDLt1/2 VLDL= 15-60minLDL= 3 days

VLDL
• The dietary intake of both fat and carbohydrate, in excess of the needs of the body, leads to their conversion into TGL in the liver. TGL are packaged into VLDL and released into the circulation for delivery to the various tissues (primarily muscle and adipose tissue) for storage or production of energy through oxidation.
• VLDL are, therefore, the molecules formed to transport endogenously derived TGL to extra-hepatic tissues.
• Nascent VLDL acquire apo-C and apo-E from circulating HDL. Lipoprotein lipase hydrolyzes TGL.
• The apo-C are transferred to HDL, thus converting VLDL to IDL. The predominant remaining proteins are apoB-100 and apoE. Further loss of TGL converts IDL to LDL.

IDL
• The fate of IDL is either conversion to LDL or direct uptake by the liver.
• Conversion of IDL to LDL occurs as more TGL are removed by the action of hepatic lipase.
• The liver takes up IDL after they have interacted with the LDL receptor to form a complex, which is endocytosed.
• For LDL receptors in the liver to recognize IDL requires the presence of both apoB-100 and apoE (the LDL receptor is also called the apoB-100/apoE receptor).



LDL• LDL are the primary plasma carriers of Cholesterol for delivery
to all tissues. The exclusive apolipoprotein of LDL is apoB-100.• Taken up by cells via LDL R-mediated endocytosis; requires the
presence of apoB-100. • Uptake occurs predominantly in liver (75%), adrenals & adipose
tissue. • The endocytosed membrane vesicles (endosomes) fuse with
lysosomes, in which the apoproteins are degraded and the CE are hydrolyzed to yield free C. ATP-dependent proton pumps lower the pH in the endosomes, which results in dissociation of the LDL from R.
• The portion of the endosomal membranes harboring the receptor are then recycled to the plasma membrane and the LDL-containing endosomes fuse with lysosomes.
• Acid hydrolases of the lysosomes degrade the apoproteins and release FFA & C. C is then incorporated into the plasma membranes as necessary.
• Excess intracellular C is re-esterified by acyl-CoA-cholesterol acyltransferase (ACAT), for intracellular storage. The activity of ACAT is enhanced by the presence of intracellular C.


LDL-Receptors
Endosome LysosomeAminoacids
CholesterolLDL
Cholesteryl ester(storage)LDL
Receptors
HMG-CoAreductase
LDL
LDL Receptor (apoB-E receptor)Receptor mediated endocytosis
ACAT
Regulates cholesterol synthesis and plasma cholesterol levels
LDL binding Internalization Lysosomal hydrolysis Regulatory actions
Uptake of LDL
• Insulin and tri-iodothyronine (T3) increase the binding of LDLs to liver cells, whereas glucocorticoids (e.g., dexamethasone) have the opposite effect.
• The effects of insulin and T3 on hepatic LDL binding may explain the hypercholesterolemia and increased risk of atherosclerosis that have been shown to be associated with uncontrolled diabetes or hypothyroidism.
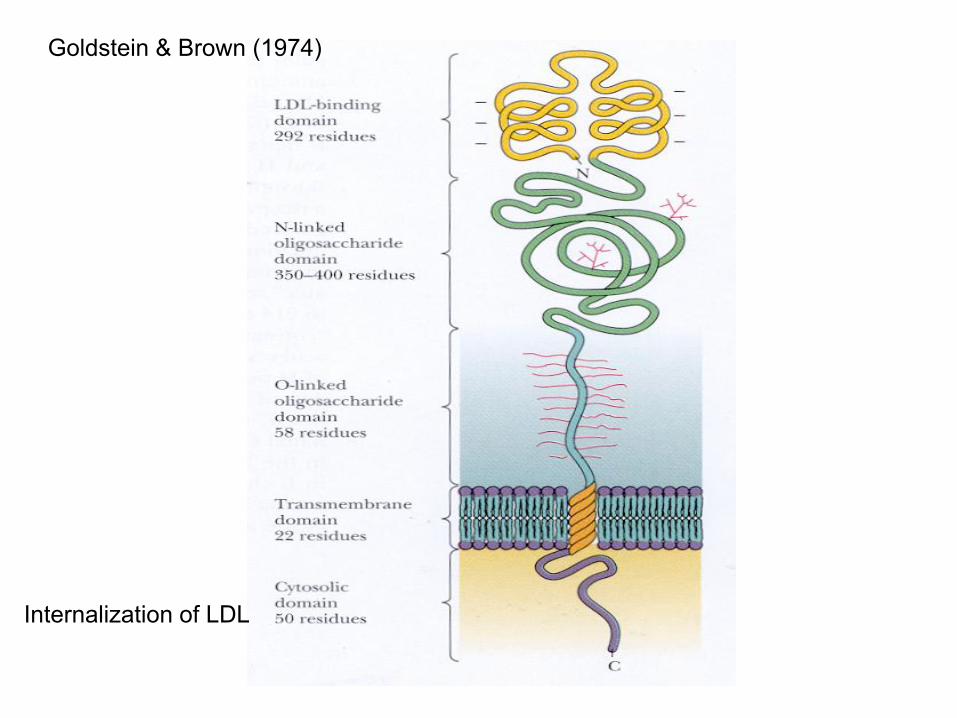
Internalization of LDL
Goldstein & Brown (1974)

Receptor-mediated clearance
• Saturability• High affinity• High degree of specificity
Fatty liver

What is Fatty Liver?• Collection of excessive amounts of fat
inside liver cells- steatosis. Occurs when lipid accumulation exceeds the normal 5% of liver weight.
• Fat in the liver usually causes no damage by itself. Indicator of the presence of a disease.
• Fatty liver may be associated with or may lead to inflammation of the liver-causing scarring and hardening of the liver. When scarring becomes extensive, it is called cirrhosis, and this is a very serious condition.


Causes of Fatty Liver• Obesity • Diabetes mellitus• Chemicals and drugs (such as alcohol, corticosteroids,
tetracyclines, valproate, methotrexate, CCl4, & yellow P) • Malnutrition, low-protein diet • Pregnancy • Vitamin A toxicity • Bypass surgery of the small intestine • Cystic fibrosis (most likely accompanied by malnutrition) • Hereditary defects in glycogen, galactose, tyrosine, or
homocystine metabolism • Medium-chain acyl CoA dehydrogenase deficiency • Cholesterol esterase deficiency • Phytanic acid storage disease (Refsum's disease) • Abetalipoproteinemia • Reye's syndrome

Two main categories1) Associated with raised levels of plasma fatty acids:
• Starvation decreased insulin, decreased protein synthesis• Feeding high-fat diet• DM• Alcoholism
2) Metabolic block in the production of plasma lipoproteins:
• Decreased apoprotein synthesis• Essential fatty acid deficiency decreased PL synthesis• Defect in incorporation of lipids and apoproteins• Defective secretory mechanism• Choline deficiency

Alcoholic fatty liver
• Ethanol is metabolised by the liver hepatocytes to acetaldehyde and acetate.
• The major route of ethanol oxidation is via alcohol-dehydrogenase, an NAD-dependent enzyme
• Both pathways result in an increased NADH/NAD ratio, whereby the fatty acid oxidation is reduced; but increased FA synthesis.
• Increased NADH/NAD increased pyruvate to lactate-Lactic acidosis.

Symptoms and Diagnosis• Usually no symptoms • Diagnosed during a routine physical examination. • There may be a rise in certain liver enzymes found in the
blood, and sometimes the liver is slightly enlarged. • To be certain of a diagnosis of fatty liver, the physician
may recommend a liver biopsy.
Treatment• Control the underlying conditions: reduction of
high blood TGL, glucose in DM, avoid alcohol & weight reduction in obesity.
• Currently, studies are underway on certain drugs such as Actigall. This drug appears to reduce liver damage in cases of steatohepatitis.
• Liver transplant.
Lipotropic factors
• Factors which prevent the formation of fatty liver– Choline– Betaine– Methionine