development and implementation of major health care...
TRANSCRIPT

Chris van Weel
Emeritus Professor of General Practice RU Nijmegen
Professor of Primary Health Care Research ANU
The community is the laboratory of primary care – every community and at all times
Development and implementation of major
health care reforms in the Netherlands
March 10, 2015, NHPA

Contents of this presentation
Introduction:
Context: health care in Europe and concepts of success
The Netherlands healthcare and history of PHC
Case Studies
o GPs out-of-hours care (NL)
o Emergency care in social context (NL)
o Comprehensive community care (B)
o Scaling-up working with migrants (EU)
Reflections, conclusions
Bottom line:
• PHC key function of any health care system
• Function can not be executed in isolation
• All incentives are at the end of the day perverse
• How to award the entire health care system to create
health, not health care
2

European Healthcare Systems
• National States’ responsibility – No EU Healthcare policy
• Diversity in history, culture and values
– Common concerns of equity, sustainability, safety
• Area of increasing interest
– European Forum of Primary Care • http://www.euprimarycare.org/
– Comparative outcome studies • http://www.nivel.nl/sites/default/files/bestanden/Proefschrift-Dionne-Kringos-The-
strength-of-primary-care.pdf (be aware: 336 pages!)
• http://www.nivel.nl/en/qualicopc
• http://www.nivel.nl/en
3

Where it all started for Europe
More primary care
• Better health population, lower
healthcare costs
• Higher life expectancy
• Better diagnosis, treatment
diseases that matter
Illness - person with illness -
population
4
Barbara Starfield
Is Primary Care Essential?
Lancet 1994

Three ‘Prototypes’
5
* White et all, NEJM 1961
Green et all, NEJM 2001
Free Access
Gatekeeping through PHC
Gatekeeping through PHC
Personal GP

6
Two Facts of Real-life Health Care
Disease - person with disease -
population
POPULATION
ECOLOGY OF MEDICAL CARE*
REPORT SYMPTOMS
CONSIDER MEDICAL CARE
VISIT GP
VISIT
HOSPITAL
OUT-
PATIENT
HOSPITAL
TEACHING
HOSPITAL
White et all, NEJM 1961
Green et all, NEJM 2001
Most health problems community based
Primary health care
matters:
More primary care:
Better population health
Higher life expectancy
Lower healthcare costs

Clash of Concepts:
• PHC
• Individuals and Populations
• Social Context
• Co-morbidity - Multimorbidity
• Evidence-based Health Policy
• Health Systems, Education, Research
• Disease-specificity in diagnosis and
management
7

Dutch health care system
• Access to health care through general practice
• Primary care the link community - health care
system
• Gate keeper, navigator function
• Specialists, hospital, after GP referral only
• Personal listing with a practice, GP
• Practice population defined, and ‘known’
• Primary care the link to society: governance,
societal impact
8

• 1941 Sick Fund Decree
• universal coverage, primary care lead, patients’ lists and capitation payment
• 1956 Founding Dutch College of General Practitioners (DCGP)
• start of academic development
• university departments, teaching, training, research
• 1973 Introduction residency training
• GP Specialist register, re-accreditation since 1975
• 1989 DCGP Quality initiative • Development, implementation guidelines most common health problems
• 2006 Individual health care based private insurance
Landmarks Dutch Health Care

The 2006 Dutch health care reform
limited financial resources – struggle to contain costs
limited health returns on care investment
(initial) political solution:
Private insurance system market to regulate care and costing
private insurers as advocates for their insurees/patients

Motives for health care reform 2006
• Political:
– EU policy, requiring competition EU region for private investments; no
protection national market (dual public – private insurance)
– Era of privatization (Dutch Rail, Dutch Mail)
– Belief of the Market solving problems, the public sector could not
• Financial:
– Increase in health care costs (‘Dutch health care the best, most expensive’)
• Public Health:
– Decreasing returns on investment (life expectancy, in particular men)
– Under-utilization of prevention
11
Notion of Putting Health Care Back on Track
Look of innovative solutions – ‘All rules off the table’

The Insurance: structure and coverage http://www.civitas.org.uk/nhs/download/netherlands.pdf
• Legal obligation to be insured - Individual or Collective schemes
– Collective scheme for those on social benefits and unemployed
• Levels of health care coverage (3):
1. Chronic care Exceptional Medical Expenses Act (1968)
• Eligibility independent financial situation; payment by taxation (12.55% taxable income)
2. Universally compulsory Social health Insurance scheme
• Basic has to be delivered by insurer, open enrolment: General practice; community nursing;
hospital and medical specialist care, medication, midwifry, dental care <18 y.
3. Supplementary part (insurer may exclude insure)
• Dental care, complementary medicine; physiotherapy, cosmetic surgery
• Tax rebates to level-off impact of costs.
– healthcare allowance
12
Simplicity on Paper:
Complex reality

Roles and responsibilities
– Government National Level
• Secure proper functioning of system, define framework criteria (financial, societal)
• Monitoring health care expenditure
• Revisit framework criteria (financial, societal)
– Insurers, the public
• Advocate for the best care against the lowest price
– Professional field
• Demonstrate quality and cost-effectiveness
• Develop, present, secure innovative solutions
– Government Municipal level
• No direct responsibility for health care
• But: more and more responsibility for social welfare and societal participation
(unemployment benefits)
• De facto more and more interaction with health care
13

Evolving government framework (I)
– Initially: making sure that the market would govern
• Allow health insurers to lead and stimulate the field to work with insurers
• Expected outcomes: lower costs, higher quality - Actual outcome: higher costs, same care
– During implementation: equity and access
• Strict regulation on obligatory insurance and unrestricted eligibility of (basic) insurance
• Retaining role of PHC/GP: patients registrars, gate keeping, capitation payment
• Provisions for undocumented migrants to secure access to high quality care through PHC
14

The 2006 health care reform: from design to
implementation
Policy intentions
•Market: best care, lowest price
• Patients’, insurers’ choice
• Active role insurers contract care
• All rules off the table
•Primary care to earn its position
• Market promote prevention
15
System implementation
• Health policy to contain ‘market’
• Return to ‘relevant’ care
• Passive role insurers
• Market regulation
• Primary care: keep system operational
• Market ignores prevention
Positive: possibility of money following innovative initiatives
health promotion, high risk groups
community based planning health and wellbeing
Problematic: restrict trivial hospital care
emergency department as revolving door of care
fancy outpatient departments

Case Study I: out of hours care, GPs and hospital emergency departments
• Objective:
– Secure access to health care 24/7, guarantee access, retain PHC structure
• Local consortia of general practices:
– Shared care for community, GPs and receptionists/practice nurses out-of hours
– Advice, GP-consultations and -home visits which can not wait till regular hours
– Triage function, access to patients’ EMR
• Outcome:
– Retaining older GPs in system; satisfaction patients; professionalization out-of-
hours
• Development since 2006:
– Initially ‘ dual system’ with hospitals’ ED (‘market share of the hospital’)
– Costs generating effects of ED did lead to cap on payment, which forced PHC-
hospital alignment for out-of-hours care
16
Determinants of success: PHC investments before 2006; Insurer money as seeding money, reallocation available resources

Case Study II:
emergency care intimate partner violence
• Objective:
– Comprehensive approach intervention, prevention and legal protection
victims of intimate partner violence
• Projected outcome:
– Prevention of repeat-episodes; promotion self-efficacy; lower ED use/costs
• Local consortium stakeholders:
– Patients and their ‘advocates’, Emergency department, PHC, Police
• Procedure:
– PHC consultant in ED; victims provided with treatment, planning follow-up,
legal protection within
• Funding:
– Insurer (additional costs ED), Reallocation regular costs PHC, police
17
Determinants of success: PHC investments before 2006; Insurer money as seeding money, reallocation available resources

Reflections health system reform in the Netherlands:
what changed and what remained the same
• The initial concept challenged all roles and functions (‘the market’)
– Empirical wisdom reconfirmed critical role of the PHC function
• Insight in costs and money flows has pointed to critical problems
– Hospital, (sub)specialist sector under financial pressure (market management)
– Reduce waste and combine, better use available resources
• Health reform is integral approach, not restricted to single functions
– Failure of the 1990, need of better interactions (in PHC, with hospital, public health sector
and inter-sectorial)
• Rethinking values and ways to award performance
– Societies need less hospital, more PHC – yet importance of specialist expertise
18
Key question in payment:
How to award professionals to make patients, populations healthy?

* In 2013 almost no increase (0.1%) in percentage of GDP (NL National Statistics Institute )
Development health care costs
Percentage increase of expenditures per
year

Experiences before 2006
• Since 1941 ‘PHC-led health system’ based on lists,
capitation fee
• Long tradition reasonably good access and care, decent
price
• Protection against ‘dehumanization’ of medicine
– Listing encouraged the bonding and trust between patients and GPs
– Capitation payment encouraged GPs to act in best interest of patients
• There was a ‘structure’ to stimulate
– Teaching, training, education since 1973
– Research, quality assurance since 1986
20
Pay Back:
Evidence based clinical practice through PHC 1989
PHC main function for health problems (> 90% => > 96%)
Case Study III Community health centre ‘Botermarkt’ Ghent, Belgium http://www.wgcbotermarkt.be/eng/?q=node/1
http://www.who.int/social_determinants/resources/isa_multilevel_contribution_bel.pdf
• Multidisciplinary centre in a socially disadvantaged area
• Private non-for-profit initiative professionals, University
• Intersectorial action, directed social determinants health
• An example: Childhood obesity
• Problem analysis: lack of physical activity
• Problem reflection: lack of safe facilities play, recreation
• Societal action to build and community-govern facilities
• Outcome: where was the first effect spotted?
21
http://www.euprimarycare.org/sites/default/files/2013%20Alma%20Ata%20-%20EngelsJDM.pdf

Case Study III Community health centre ‘Botermarkt’ Ghent, Belgium http://www.wgcbotermarkt.be/eng/?q=node/1
http://www.who.int/social_determinants/resources/isa_multilevel_contribution_bel.pdf
• Multidisciplinary centre in a socially disadvantaged area
• Private non-for-profit initiative professionals, University
• Intersectorial action, directed social determinants health
• An example: Childhood obesity
• Problem analysis: lack of physical activity
• Problem reflection: lack of safe facilities play, recreation
• Societal action to build and community-govern facilities
• Outcome: drop in crime rate, improved safety street
22
Case Study IV Implementing PHC through Europe: RESTORE program
• Background and aim:
– Migrants form a substantial part ‘European PHC population’
– Communication key determinant of outcome of care, some professional guidelines
– Poor uptake, developed for, but not with migrant service users
• Approach:
– Built upon successful study in Ireland to engage difficult-to-reach migrants
– Use of migrants as co-designers, to plan service design with difficult-to-reach migrants
– Application state-of-the-art methods (NPT/PLA)
• Context:
– Example of a ‘Scaling-up’ approach
– Priority setting national scale: heterogeneity of health systems, migrant populations
• First experiences:
– Availability of resources, but a need to test these in different settings
– Methods to engage the hardest-to-reach migrants works throughout the EU region
– Importance of flexibility to fit the system (for example professional translators in NL)
23
RESTORE: Research into implementationSTrategies to support patients of different Origins and language background in a variety of European primary care settings
MacFarlane et al. Implementation Science 2012, 7:111
http://www.implementationscience.com/content/7/1/111ropean Study
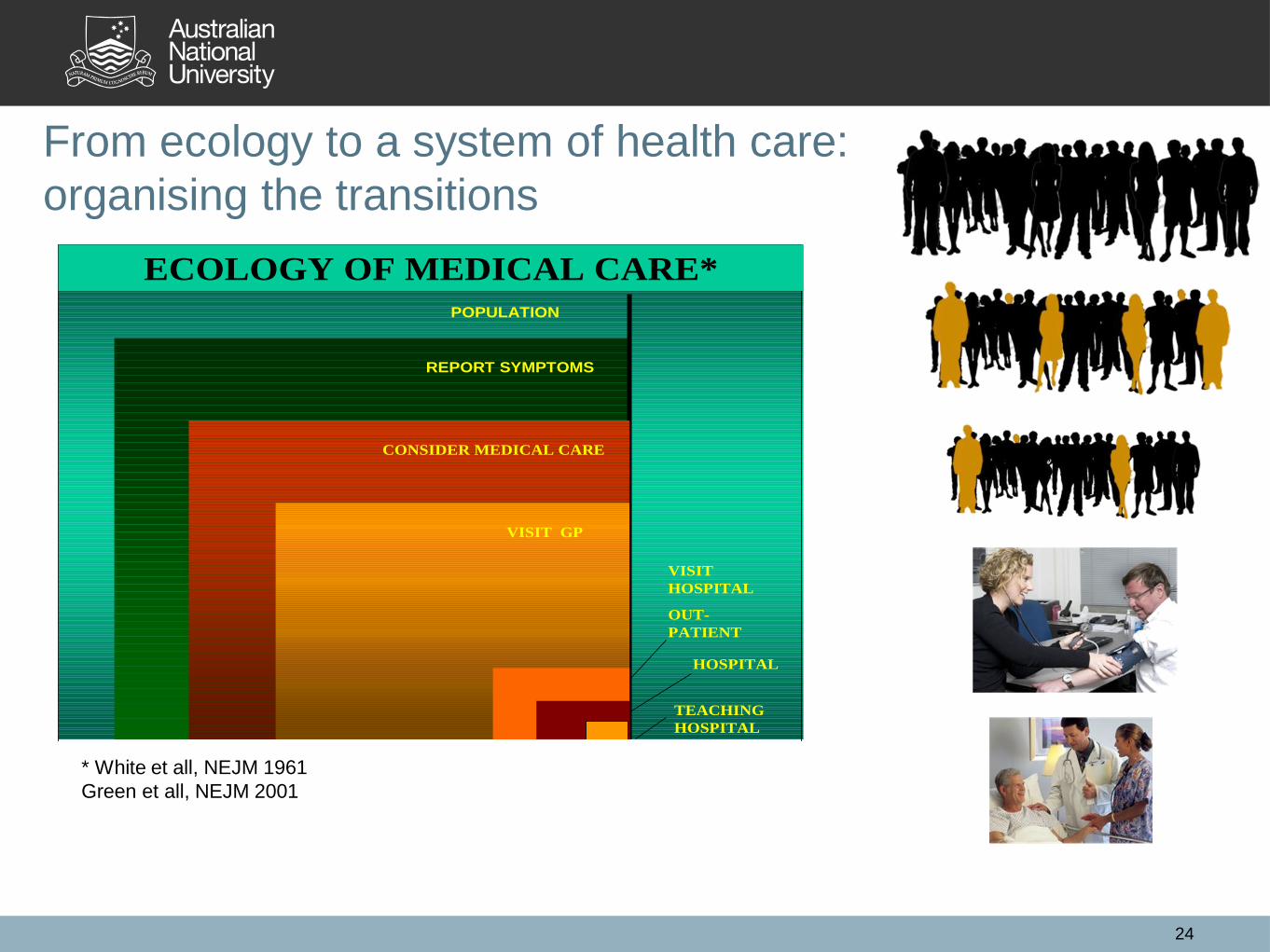
From ecology to a system of health care:
organising the transitions
24
POPULATION
ECOLOGY OF MEDICAL CARE*
REPORT SYMPTOMS
CONSIDER MEDICAL CARE
VISIT GP
VISIT
HOSPITAL
OUT-
PATIENT
HOSPITAL
TEACHING
HOSPITAL
* White et all, NEJM 1961
Green et all, NEJM 2001

Reflections, conclusions
Best outcomes in systems with PHC structure
Relation of trust between GP practice – patient critical
Registration – practice lists – rostering
Leadership of professionals critical driver of success
All PHC professionals,
Payment be directed at care for the patient with the health
problem, rather than at the health problem the patient has
Value of capitation payment
Challenges remain in the further integration of PHC with
Social welfare and public health
Hospital care and specialists
Impact of PHC is broader than health and health care
25