pdf (1.711 mb)
TRANSCRIPT

40
Upper canines and incisors: how a better knowledge of their morphology can help us to optimise their function
Amine EL ZOGHBY, Jean-Philippe RÉ, Christophe PEREZ,
Anne GIRAUDEAU, Jean-Daniel ORTHLIEB
Address for correspondence:A. EL ZOGHBY,rue de Damas,B.P. 11-5076Riad el-Solh1107 2180 [email protected]
ABSTRACT
Biometric study of contemporary human maxillary incisors and canine coronalmorphologyThe orthodontic alignment or prosthetic rehabilitation of the upper anterior sector is
based on available biometric data.The aim of this study is to measure the angle formed between the functional lingual sur-
face of the canine and central incisor and the axial-orbital plane.Materials and methodsThis retrospective study is based on an analysis of documents of young dental students.The measurements were made on 49 silicone models of healthy, natural, functional
teeth, in class I occlusion for the maxillary anterior group.ResultsThe values of slope angulations of the lingual surfaces relative to the axial-orbital plane
clearly decrease by 10° from the central incisor (57°) to the canine (47°).If there is stability in buccal morphology, there is variability in anterior lingual morphology,
particularly of the canine.These variations in an essential zone on the functional level are marked enough to war-
rant being taken into account in clinical practice.
KEYWORDS
BiometricIncisal guidanceCanine guidance Coronal morphology IncisorCanine.
J Dentofacial Anom Orthod 2010;13:40-54© RODF / EDP Sciences
DOI: 10.1051/odfen/2010105
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2010105

J Dentofacial Anom Orthod 2010;13:40-54. 41
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
Fifteen years ago, an emeritusclinician, Harold Shavell22 wrote: “Ina stable occlusion (inter-arch inter-cuspation) dental treatment mustreflect absolute and faultless sub-mission to the morphological struc-tural data. Morphology is the destinyof dentistry.”
Dentists often use specificdevices and protocols to repositionor rehabilitate the maxillary anteriorteeth in order to improve theirachieving aesthetic alignment.Although the labial surfaces of theseteeth usually display similar convexshapes, the lingual morphology ofthe upper incisors and caninesvaries greatly (fig. 1 and 2). And it is
precisely these lingual surfaces thatplay an essential role in masticatoryfunction8.
1 - BIOMETRIC STUDY OF THE CORONAL MORPHOLOGY OF UPPER INCISORS AND CANINES IN MODERN HUMANS
1 - 1 - Introduction
Figure 1Upper left upper: labial, mesial and lingualviews. The position in space and slope ofgenetically predetermined dental mor-phology will influence mandibular aes-thetics and kinematics.
Figure 2An inspection of its facial surfacealone can not provide any informa-tion about a tooth’s lingual mor-phology.
1 - 2 - Morphology induces the occlusal guidancefunction
Very often, orthodontists set andachieve a goal in treatment of adultsof altering anterior guidance function.While as yet there is no formal proofof its efficacy, dentists usually estab-lish a therapeutic plan designed toachieve immediate posterior disocclu-sion in mandibular translation move-ments. This total disocclusion, whichis scarcely physiological but easy for

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function42
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
dentists to obtain technically, is quiteopposed to the notion of a balanced“equilibrated” occlusion that wouldbe characterised by the simultaneouspresence of anterior and posteriorocclusal contacts in mandibularpropulsive and lateral excursion move-ments5.
Because no one has so far pre-sented adequate scientific evidenceto show which is most effective,dentists have to rely on clinical con-clusions and the scanty factual datanow available, to establish theirtreatment plans. But there is gener-al agreement among practitionersworking in the field that a canineprotected occlusion may be themost acceptable as Rinchuse et al.,reported in a review that found theliterature to be replete with sectar -ian and rather vague conclusions19.We feel, therefore, it is essential forus to explain why we believe thetherapeutic design of canine protec-tion appears to be valid:
– the therapeutic creation of caninefunction through orthodontics or pros-thetic treatment is easier to obtainthan group function;
– a pathogenic outcome of canineprotection has never been shown, butthe case for posterior occlusal inter-ference leading to harmful effectsseems much more likely.
We want to make it clear that ourbelief in the therapeutic value ofcanine guidance is only an opinion. Inview of the fragile nature of the avail-able scientific data17, no reasonableperson could dignify an interpretationof the status of the debate on group,canine, or any occlusal function assomething more solid than that; it isjust an opinion.
Mandibular kinematics depends
on the functioning of occlusal guid-ance. In the last phase of excursivemovement, the tooth guidance sur-faces pilot the developing mandibu-lar elevation by anticipation, rather inthe way of an access cone movingdirectly towards a target which ismaximal intercuspation in occlusion(MIO). This target must be accurateand unique. This guidance avoidsobstacles Into a position of maximalinter-cuspation, in the way an accesscone gives a path to a target. Thisocclusal target must be precise andunique, avoiding occlusal obstacles.It is essential that we understandwhat is meant by “occlusal interfer-ence”, guidance surfaces, andocclusal contacts.
– Occlusal interference is definedas dental obstacles generating limita-tion and/or deviation of horizontalmandibular trajectories in propulsiveor lateral excursions15.
– Posterior occlusal interference ischaracterised during a propulsive orlateral excursion translation move-ment by occlusal contact on a multi-cusp tooth without simultaneousanterior occlusal contact. In otherwords, “a posterior tooth releases theanterior teeth during translation”10.
Remarks concerning group function:Guidance only by the canine (caninefunction) or with the participation ofother teeth contiguous to the canine(more or less extensive group function)are functional guides, because there isno interference. Group function is a formof guidance which is effective in masti-cation at the cost of eroding tooth sur-faces.
– Anterior occlusal interferencemight be thought of as over guidance,blocking mandibular translation. In apropulsion movement, isolated con-

J Dentofacial Anom Orthod 2010;13:40-54. 43
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
tact on the mandibular teeth mustmove in accordance with the lineartrajectories on the maxillary guidancesurfaces. Anterior interference resultsfrom an excessively vertical guidanceslope. It is revealed by the presenceof reversed guidance zones: linear onthe labial surfaces of the mandibularincisors or canines and at discretepoints on the maxillary anterior teeth.
By promoting simple, direct move -ments, the slight predominance of anterior contacts facilitates neuro-muscular action25 while minimizingerosion of enamel. From the masti-cation point of view, harmoniousocclusal curves and dominant but mild canine slopes promotehomogeneous, symmetrical contactbetween the occlusal tables andoptimise grinding of foodstuffs. Inparafunctional activities like bruxismand gum chewing, during lateralexcursion the proximity of antagonis-tic posterior occlusal tables acts asan occlusal parapet, protecting theTMJs during strong activation of theelevators. On the other hand, wherecanine guidance is overly steep, thisprotection is absent and the anteriorblockage it causes will prevent trans-lation movements which generatemandibular retro-function and/or lat-eral function. This makes themandible operate in opposition to thenatural direction of anatomico-physi-ological function of the Temporo -mandibular joints (TMJ).
This proprioceptive guidance,working by anticipation, depends onthe organization of the anterior teethwhich display architectural and mor-phological aspects specific to ourhuman lineage14. The lack of prema-ture wear in the dental system in
modern populations accentuates thefunctional role played by dental mor-phology21.
1 - 3 - Reference plane
Figure 3The different reference planes in sagittal view
meatus) and left infraorbital point. Itcorresponds to the position of thehead of a person looking at the hori-zon, in an orthostatic position.Clinically, dentists use a cutaneousFrankfurt plane defined as passingthrough the Tragions (upper edge ofthe tragus) and the left cutaneousInfraorbital point (antero-inferioredge of the orbit)15.
Any evaluation of occlusal func-tions requires a non-dental horizon-tal baseline. The traditionalanthropological reference, theFrankfurt plane, accepted at theInternational Anthropology Confer -ence at Frankfurt in 1884, is a planein bone passing through the Porions(upper edge of the external auditory

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function44
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
It is a common error to think thatthe Frankfurt plane is the horizontalreference plane for mounting modelson articulators, particularly when atransfer arch with auricular end-pieceis used. In fact, the great majority ofarticulator systems employ the Axial-Orbital Plane (AOP), directly or byapproximation.
It passes through the Condylicuspoints (cutaneous or bony) and theleft Infraorbital point3. The posteriorreference is, indeed, at the level ofthe bi-condylar rotation axis (thisdetail was provided by Mc Collum in1924 and Stuart in 195518. The meandifferential angle (fig. 3) between theFrankfurt plane and the AOP is around7° (Standard deviation 2° out of 46measurements)16.
Data can be superposed andduplicated on different articulatorswith the AOP, as well as in cephalo-metric analyses and axiographicrecordings. The AOP also provides aset-up of dental arches which arespatially correct or at least close tothe horizontal baseline linked to thesemi-circular canals4.
pre-determined labio-lingual inclina-tion of the lingual convexities of upperanterior teeth during treatment.
Many statistical studies usingcephalometry on the bucco-lingualslopes of the incisors have providedreference data which orthodontistscan use to obtain optimal axial posi -tioning of teeth in conformity withskeletal types and aesthetic criteria.
In assessing tooth morphologyorthodontists can refer to dentalanatomy manuals that give an aca-demic reference model for each typeof tooth. But these models are onlygeneralisations that do not take indi-vidual differentiations into account.The biometric data in the literatureon the morphology of modernhuman upper anterior teeth is scantyand what there is applies primarily toincisors11. Both common sense andavailable studies caution us, as is thecase for all biological data, that vari-ation between individuals is great,and, for anterior teeth is concentrat-ed in the functional zone, the lingualsurfaces.
So we have decided it would beuseful to study the morphological vari-ability of upper incisor and caninecrowns to derive a theoretical set ofmean values that could helporthodontists to decide whether eachclinical situation requires a cus-tomised individual plan or whetherthey can use mean values to treatspecific cases.
This study proposes to furnish bio-metric, quantitative bucco-lingual dataabout anterior-maxillary teeth, bycomparing the morphology of theupper central incisor and canine teethof a group of modern humans.
1 - 4 - The variability of dental morphology
During the life of the natural denti-tion, the guidance slope adapts it toenvironmental pressures and com-pensates for skeletal deviations, eventhough nature dictates tooth morphol-ogy. The lingual morphology of maxil-lary anterior teeth clearly plays amajor part in guidance functionthrough the location of anatomicalrelief6,12,24. Accordingly, orthodon-tists should evaluate the extent of the

J Dentofacial Anom Orthod 2010;13:40-54. 45
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
This is a retrospective study ofeducational documents includinginformation obtained during the initialdental student clinical training period.In their program dental students fillout questionnaires, examine eachother clinically, take impressions ofeach other’s teeth, and prepare mor-phological analyses of their teeth inrelation to a horizontal referenceplane derived from a face bow. Weaccumulated our data by analysingthe data provided by the question-naires and the clinical examinationreports. We selected 49 consecutivefiles of 27 male and 22 female stu-dents whose average age was 22.
Criteria for selection:– young subjects between 22 and
25 years of age whose teeth wouldnot yet have suffered much dentalerosion;
– natural healthy dental arches;
– class I Angle occlusion with anterior contacts at maximal intercus-pation.
Criteria for exclusion from the study:– history of dysfunction of the
masticatory apparatus;– orthodontic treatment in
progress or completed;– dental reconstruction of the lin-
gual part of an anterior tooth;– significant malocclusion;– guidance anomaly: posterior
interference, anterior open bite.
2 - MATERIALS AND METHOD
2 - 1 - Sample
Figure 4Orthogonal support - class I Angleocclusion with anterior contacts atmaximal intercuspation.
Figure 5The orthogonal support, lined with silicone,fixed to the Quick® Axiograph, records the mor-phology of the anterior-maxillary teeth refer-enced in the Axial-orbital plane.
2 - 2 - Method
For each subject, we constructed asilicone model of the upper anteriorteeth mounted correctly in space onthe articulator by means of an ear-bowarbitrary face-bow transfer instrumentwhose horizontal and frontal position-ing we checked clinically as we pro-ceeded. By means of a right angle

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function46
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
support to the transfer arch plane weregisted the horizontal referenceplane, the Axio Orbital plane, and atthe same time the morphology of theupper anterior group of teeth (fig. 4and 5). In this way the modeling can be done directly in the mouthwith a silicone elastomere key (Elite®
H-D+.Zhermack).
Each silicone core is sectioned per-pendicular to e reference plane at twolevels for each canine and centralincisor (fig. 6). The sections are in themiddle of the tooth (central section -C) and at the main point of contact inmaximum intercuspation occlusion(MIO), usually on a proximal crest(Proximal section - P).
Figure 6Location of section illustrated of an upperleft central incisor: Central section (C) andproximal section (P).
Figure 7Vertical, orthogonal sections are cut alongthe previously defined cutting levels.
Figure 8Definition of labio-lingualbiometric parameters: (S:lingual slope, V: vestibularslope, AC: coronal axis,AOP: transposition of theAxial-orbital plane).
Figure 9Each section of the siliconecore is numbered (the lowerpart of the silicone representsthe reference plane and the 10mm scale). The biometricparameters will be quantifiedon each section.
Figure 10Screen view obtained after enter-ing the details of a proximal sectionof a 21 (all the values are expressedin degrees or millimetres).
Standarddeviation
J Dentofacial Anom Orthod 2010;13:40-54. 47
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
The different sections are num-bered by standard photographs thenquantified using software speciallydeveloped for the purpose (fig. 9).The reference dimension is given bythe length of the impression forksupport.
The slopes between the differentaxes are evaluated relative to theanatomical points noted (fig. 8 and 9)(labial and lingual cervical point, lin-gual contact point, labial and lingualcurvatures, point of labial and lingualfree edge).
We focused on studying four values:
S/V
S/AOP
V/AOP
S/CA
Lingual labial angle: between the lingual surface (S) and thelabial surface (V)
Guidance slope: slope between the lingual surface (S) and thereference plane (PAO)
Labial angle: slope between the labial surface (V) and the refe-rence plane (PAO)
Lingual-Axial surface angle: slope between the lingual surface(S) and the coronal axis (CA)
We evaluated these values inrelation to the Frankfurt planebecause the fork is parallel to the lateral arms of the face bow. To facil-itate comparison of the measure-
ments with other published studies,we added a corrective angle of 7° torelate them to the Axial-orbital plan,which is the one most commonlyutilised.
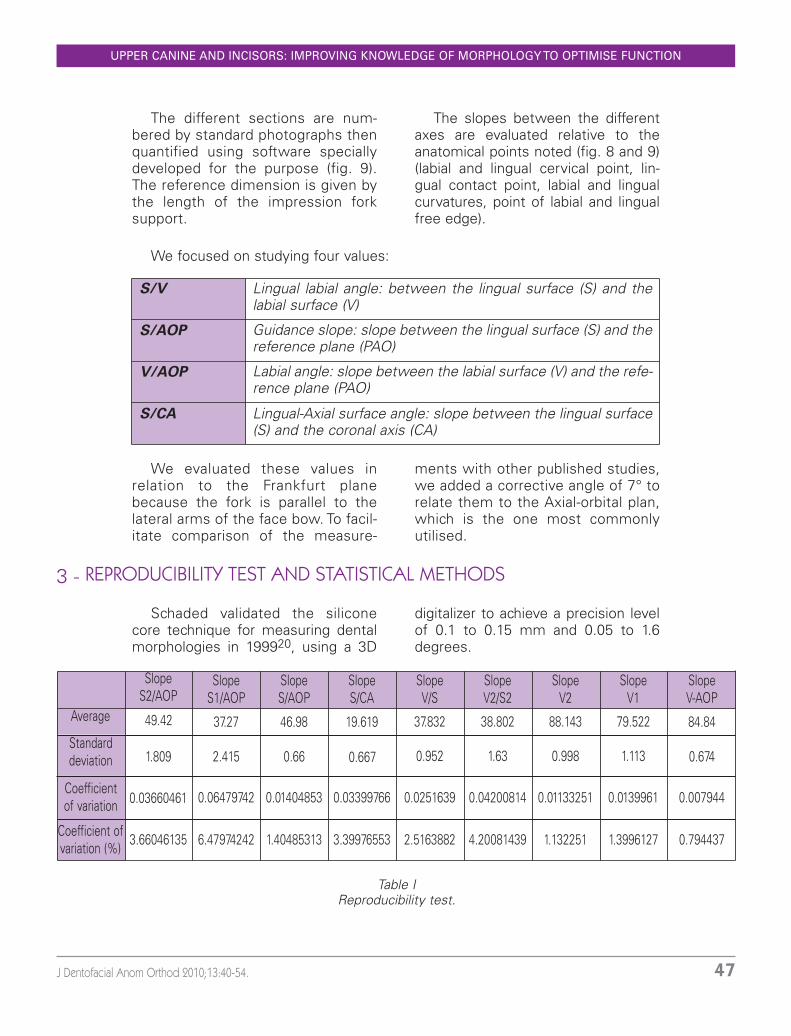
3 - REPRODUCIBILITY TEST AND STATISTICAL METHODS
Schaded validated the silicone core technique for measuring dentalmorphologies in 199920, using a 3D
digitalizer to achieve a precision levelof 0.1 to 0.15 mm and 0.05 to 1.6degrees.
Average
Coefficient of variation
Coefficient ofvariation (%)
SlopeS2/AOP
49.42
1.809
0.03660461
3.66046135
SlopeS1/AOP
37.27
2.415
0.06479742
6.47974242
Slope S/AOP
46.98
0.66
0.01404853
1.40485313
Slope S/CA
19.619
0.667
0.03399766
3.39976553
Slope V/S
37.832
0.952
0.0251639
2.5163882
Slope V2/S2
38.802
1.63
0.04200814
4.20081439
SlopeV2
88.143
0.998
0.01133251
1.132251
SlopeV1
79.522
1.113
0.0139961
1.3996127
Slope V-AOP
84.84
0.674
0.007944
0.794437
Table IReproducibility test.

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function48
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
To test the reproducibility of theacquisition software, the sameoperator repeated computer inputfor the same section of a centralincisor. The low coefficients of vari-ation in these measurements (witha mean error of 3%) indicate thatthis measurement can be consid-ered to be reproducible and accu-rate (table I).
The descriptive statistical study(Stata 8.0® software) deals with fourangular values characterising crownmorphology. We used the t-test to com-pare the means of the continuousnumerical variables, the chi² test to com-pare the nominal or qualitative variables,and the correlation test for the linksbetween quantitative variables. The sig-nificance threshold a was set at 5%.
4 - RESULTS
The quantification of angles (S/V,S/RP, V/RP and S/CA) performed onour sample did not show any signifi-cant difference between men andwomen. This allowed us to groupthem in a homogeneous series of 49subjects. But we used only the righthand side because of slightly signifi-
cant differences between the twosides.
For each case, we analysed the cen-tral and proximal sections. Consideringthe low significance of the differences,we used only the proximal sections forthis study because they were closer tothe functional zone (tables II, III, IV and V).
Lingual surface / coronal axis (S-CA)
Lingual-labial angle (V-S)
Lingual angle / Reference plane (S-RP)
Labial angle / Reference plane (V-RP)
N
49
49
49
49
m
17.78
37.97
57.29
88.83
sd
2.66
5.23
8.69
7.9
Table IIRight central incisor: proximal section (N: number of subjects, m: mean value in degrees,sd: standard deviation).
Lingual surface / coronal axis (S-CA)
Lingual-labial angle (V-S)
Lingual angle / Reference plane (S-RP)
Labial angle / Reference plane (V-RP)
N
49
49
49
49
m
29.29
55.93
47.43
93.18
sd
4.07
6.89
10.33
8
Table IIIRight canine: proximal section (N: number of subjects, m: mean value in degrees, sd:standard deviation).

J Dentofacial Anom Orthod 2010;13:40-54. 49
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
The correlation study (table V)between the two parametric variablesshowed that there is a high r coeffi-cient (approx. 0.8) between the maxil-
lary central incisor’s labial and lingualsurfaces but a very low one for thecanine’s buccal and lingual surfaces (r coefficient 0.01).
Table IVComparison of mean values between canine (red) and central incisor (blue): slopes of lin-gual coronal axis (S-CA) and labial (V) surfaces on the reference plane (RP) or the maincoronal axis (CA).
Tooth
11
13
Observation
49
49
Correlation factor
0.8
-0.093
p
0.000
0.51
Table VCorrelation between the labial angle on the Reference plane (V-RP) and the lingual angleon the Reference plane (S-RP).
5 - DISCUSSION
Despite the limitations of thisstudy, in relatively low sample sizeand single geographic location of thepopulation, it nevertheless providesoriginal biometric data that quantifiesthe biometric variability of maxillaryanterior teeth.
Relative to the Axial-orbital plane,the values of the guidance slope tilt (S)on the lingual surface (S/AOP) fall distinctly (approx. 10°) between the
5 - 1 - Guidance slope in the AOP

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function50
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
central incisor (57°) and the canine(47°).
Slavicek, in 198323 was the first tosuggest this analytical method, with astudy of the upper central incisorinvolving more than 1000 cases. Hisdescription of the lingual surface (fig.11) includes 3 measurement planes:S1 (1/3 cingular), S2 (1/3 occlusal) andS (median plane). The measurementsrevealed an incisor slope (S2) of about60°, confirmed by Orthlieb in 199016
with an angle of 61.35° (n=229,sd=12.4).
Kulmer also confirmed theseresults in 1999 on 34 youngAustrians13. Celar reports slightlylower values for a Japanese popula-tion of 82 young subjects: centralincisor: 51.5 (sd: 11.4), canine 44.2:(sd: 10.2)². Hobo7 found the samelevel of dispersion for the incisorslope.
The mean values we obtained inour study therefore confirmed theprevious work. They underline theneed to achieve a canine slope ofaround 45°, about 10° less than theincisor slope.
The mean slopes found are closeto a right angle.
Comparison between the incisorand the canine shows that the buccalsurface of the canine is slightly tiltedbuccally (94°) whereas the incisor‘sinclination (88°) is more lingual. Thecurvature of the canine is slightlymore accentuated.
Figure 11Different angles measured by Slavicek in 1983: S1: Cingular plane, S2: 2/3 occlusal, S:mean lingual slope.
5 - 2 - Labial surface slope in the AOP
5 - 3 - Angle of slope on lingual / coronal axis / labial surface
We start from the principle that thecoronal axis in humans is similar tothe crown-root axis. The anglebetween the labial surface and thecoronal axis does not show any par-ticular variations. It is lingually, on thehidden surface of maxillary anteriorteeth, that morphological variabilitycan be found.

J Dentofacial Anom Orthod 2010;13:40-54. 51
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
The angle between the lingualslope and the coronal axis (S/CA)increases between the centralincisor (18°) and the canine (29°).Slavicek23 reports a mean value of23° for S/CA for the canine. Thisunderscores the thicker labio-lingualshape of the canine with its highlyconvex lingual surface. It seems tous important to emphasise thevariability of this angle inorthodontics. While the anglebetween the labial surface and thelingual surface (V/S) has a stan-dard deviation of 7° for the canine,it is only 5° for the incisor.Slavicek23 reports standard devia-tions of 10°.
Therefore, by using the vertical ori-entation of the labial surface of thecanine as a reference, the guidanceslopes may vary by 15° to 20°.Functionally speaking, this variationcould be important when lateral excur-
sion operates to obtain minimal disoc-clusion posterior to the canine withoutinterference. It may be noted that thelack of correlation between the labialand lingual slopes of the canine showsthat by observing only the labial sur-face slope an orthodontists cannot dis-cern any information about the canineguidance slope.
Table VIComparative anatomy: comparison of incisors and canines (S/RP: lingual slope on refer-ence plane, S/CA: guidance slope on coronal axis).
5 - 4 - Evolution and comparativeanatomy
At the anthropology laboratory inthe Marseille Faculty of Medicine, acomparative anatomy study of anteriorteeth in a dry skull was carried outusing an identical protocol. In 2001, K.Illouz compared the incisors of 10large ape skulls, 27 prehistoric men,15 medieval men, and 35 modern sub-jects9 in vivo. In 2003, F. Bukiet com-pared the canines of 10 large apes, 14

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function52
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
prehistoric men, 40 medieval men,and 21 modern subjects1 in vivo.
Table VI summarises these studiesand leads to several observations.
– The lingual slope of the incisor isdistinctly increasing whereas the lin-gual slope of the canine is decreasing.
– Verticalisation of the incisors iscoherent with the increase in incisalover-bite.
– Reduction of the lingual slope ofthe canine.
– The angles between the lingualslope and the coronal slope (S/CA) arevirtually constant, which indicatesvery few morphological modifications.
– The values for current popula-tions harmonise with the results ofthe study presented.
– Because of the size of the sam-ples, it is difficult to attribute the slightdifferences noted to an ethnic varia-tion between the south of France andLebanon.
6 - CONCLUSION
Our study provides biometric dataabout maxillary canines and centralincisors in modern humans. Thesedata are intended to be used for pros-thetic or orthodontic treatment.This work confirms the thicker, morecurved configuration of the maxillarycanine compared to the central incisorand also its shallower lingual slope.The mean values that we report in ourstudy underline the benefit of target-ing a canine slope of around 45°,which is about 10° less than theincisor slope. On the other hand, it islogical to think that our treatmentsmust not lead to:
– a canine slope of more than 60°;– a canine slope which is steeper
than the incisor slope.Although distinct stability is noted
in labial and buccal morphology, thereis variation in lingual morphology, par-ticularly of the canine.
These variations in a functionallycritical zone are great enough to affectthe orthodontist’s choice of pre-torqued, pre-angulated brackets. It isconceivable that as studies in this
area flourish, that 3 or 4 classes oflabio-lingual angles may be defined toaid in such a selection.
The limitations of this work requirethat our conclusions be used only ashypotheses that deserve future indepth investigations with larger sam-ple sizes and the introduction ethnicvariations as well as typological cate-gories.
Figure 12Example of the close of orthodontic treat-ment: the maxillary canines, with theirstrong lingual inclination side, have slopesthat are steeper than those of the incisors.This is the opposite of what should havebeen obtained.

J Dentofacial Anom Orthod 2010;13:40-54. 53
UPPER CANINE AND INCISORS: IMPROVING KNOWLEDGE OF MORPHOLOGY TO OPTIMISE FUNCTION
1. Bukiet F. Etude biométrique de la canine maxillaire permanente les hominidés. Mémoire deD.E.A Laboratoire d’Anthropologie «Quaternaire», Faculté de médecine. Marseille : Universitéde la Méditerranée, 2003.
2. Celar A, Kubota M, Akimoto S, Sato S, Slavicek R, Hennerbichler E. Inclines of occlusal gui-dance,wear facets,and hinge axis path considering sequential guidance with canine domi-nance. Bulletin of Kanagawa dental college 1997;25(1):3-9.
3. Celenza FV. An analysis of articulators. Dent Clin North Am 1979;23:305-26.4. Delattre A, Fenart R. Otospongiosis and cranio-labyrinthine rotation. J C R Hebd Seances
Acad Sci 1960 Oct 10;251:1563-4.5. Espinosa de la Sierra R. Development of organic occlusion. J Gnathology 1985;4:87-115.6. Feuillerat C, Simon J, Orthlieb JD. Morphologie fonctionnelle des incisives maxillaires.
Cahiers Prothèse 1988;63:83-97.7. Hobo, 1997.8. Horris WH MC. The importance of anterior teeth. J Gnathology 1982;1:19-36.9. Illouz K. Anatomie comparée de l’incisive médiale maxillaire chez les Hominidés. Mémoire
de D.E.A Laboratoire d’Anthropologie «Quaternaire», Faculté de médecine. Marseille : Univde la Méditerranée, 2001.
10. Ingervall B. Tooth contacts on the functionnal and non functionnal side in children and youngsadults. Arch Oral Biol 1972;17:191-5.
11. Kiezer JA, Groeneveld HT. The reliability of human odontometric data. J Dent Assoc S Afr1991;46(5):267-70.
12. Kubein-Meesenburg D et al. Individual reconstruction of palatal concavities. J Prosth Dent1988;60(6):662-72.
13. Kulmer S, Ruzicka B, Niederwanger A, Moshen I. Incline and length of guiding elements inuntreated naturally grown dentition. J Oral Rehabil 1999;26(8):650-60.
14. Lacroix P. Le surplomb et le recouvrement incisif et canin dans l’évolution du guide antérieur.Mémoire de D.E.A «Quaternaire», Faculté de médecine. Marseille : Univ de la Méditerranée,1998.
15. Lexique d’occlusodontologie, College national d’occlusodontologie, Quintessence, 2001.16. Orthlieb JD. Diagnostic occluso-céphalométrique assisté par ordinateur (Occluso-cephalo-
metric computerised diagnosis). Doctorat d’Université. Marseille : Univ de la Méditerranée,1990.
17. Orthlieb JD, El Zoghby A, Kordi M, Perez C. La fonction de guidage : un modèle biomécaniquepour un concept thérapeutique. Cahiers Prothèse 2004;128:43-54.
18. Pitchford JH. A reevaluation of the axis-orbital plane and the use of orbital in a face bow trans-fer record. J Prosthet Dent 1991 Sep;66(3):349-55.
19. Rinchuse D, Kandasamy S and Sciote J. A contemporary and evidence-based view of canineprotected occlusion. Am J Orthod Dentofacial Orthop 2007;132(1):90-102.
20. Schaden G, Kulmer S, Dumfahrt H. Untersuchung der individuellen frontzahnfuhrung einmethodenvergleich. IOK 1995;27(1):7-13.
21. Seligman DA, Pullinger AG. Analysis of occlusal variables dental attrition, and age for distin-guishing healthy controls from female patients with intracapsular temporomandibular disor-ders. J Prosthet Dent 2000;84(1):114-5.
22. Shavell HM. Amalgocclusion: de la creation artistique d’une anatomie dentaire fonctionnellegrâce à l’amalgame d’argent. Réalités cliniques 1993;4:119-32.
BIBLIOGRAPHY

El Zoghby A, Ré JP, Perez C, Giraudeau A, Orthlieb JD. Upper canine and incisors: improving knowledge of morphology to optimise function54
AMINE EL ZOGHBY, JEAN-PHILIPPE RE, CHRISTOPHE PEREZ, ANNE GIRAUDEAU, JEAN-DANIEL ORTHLIEB
23. Slavicek R. Les principes de l’occlusion. Rev Orthop Dento Faciale 1983;17:449-90,533-43.24. Valentin.C. Le guidage antérieur en denture naturelle. C.N.O. 3es journées du collège natio-
nal d’occlusodontologie. Reims, 14-15 mars 1986.25. Williamson EH, Lundquist DO. Anterior guidance: its effect on EMG activity of the temporal
and masseter muscles. J Prosthet Dent 1983;49:816-22.