pcnp acute and chronic wounds - read-only
TRANSCRIPT

11/3/2017
1
Carol Calianno MSN CRNP, CWOCN11/3/17
If specific brands are mentioned or shown in photographs it is done because: There are unique characteristics of the product It is the only product in the category Within product categories, examples of multiple
dressings are shown to demonstrate product type/properties
I have no vested interest, financial or otherwise in any product discussed
Review of different types of wounds Discuss how mechanism of injury and systemic
disease affects treatment choices Review common and advanced wound care
treatment options for acute and chronic wounds
Mechanism of repair depends upon the tissue layers damaged
Partial Thickness - Epidermis and superficial dermal layer heal by regeneration. Does not form granulation tissue. No scarring.
Full Thickness - Deep dermis, appendages, hypodermis, muscle, tendons, ligaments, & bone heal by scar formation. If healing by second intention, granulation tissue is formed.
��������� ������
������ �������
���
��� ���������
����������������
��������� �����!��
"�����
"� � ���##�����
������������$������% ������&����&������������
Hemostasis Small vessels contact Platelets are activated and aggregate at damaged
vessels Coagulation cascade begins
Inflammation Neutrophils and monocytes begin clean up phase Macrophages are released to stimulate proliferative
phase Prolonged inflammation caused by Increased bacterial levels Repetitive trauma Contributes to hyper-proliferative scaring
(hypertrophic and keloid type scars)

11/3/2017
2
$����������� ����������� ���������'�������������������(��������
)�� �*� ������������� ���� +������� ������������������������������
����������������'���)��,��-������������#���������������� ����� ���'�.�����/�0�
� ����������� ���������#��������#����������'�����������'�������������������
� ��������% ���� ������#����00� ������������������ ���� ������#������'�������������#��" �����������������������
��� ����������������/��123 ������������������������
����#�����������������#���4������
Only pressure injuries are ‘Staged’
Not all wounds on a diabetic are ‘diabetic ulcers’
If unsure of etiology use terms partial or full thickness to describe wound
Chronic Wound Definitions Wounds, which have failed to proceed through an orderly and timely reparative
process to produce anatomic and functional integrity over a period of 3 months
A wound that does not decrease in size by 30% in 3 weeks or by 50% in 4-5 weeks. If a wound does not decrease in size by 50% in 4 weeks there is a 91% chance it will not be healed within 12 weeks
Terms Stalled Wound Maintenance Wound Non-healable Wound
Widergrow,A.D.(2012) Deconstructing the stalled wound. Wounds (24)3, 58-66
Surgical
Trauma
Cutaneous manifestations of systemic disease
Move rapidly and predictably through the repair process
Most surgical wounds are closed by sutures, staples, adhesive tapes or glue
Surgical Wound Classifications Class I – clean, uninfected. Close with primary closure Class II – clean/contaminated, GI or GU or respiratory tracts were
entered during the surgery. No evidence of infection. Close with primary closure
Class III – open wounds or surgeries with spillage from GI tract. Delayed primary closure ( tertiary intention)
Class IV – Dirty Infected, older wounds, contaminated. Heal by secondary intention
SSI account for 22% of all hospital acquired infections
Poor statistics on outpatient SSI rates Most statistics are for ambulatory care surgical centers Estimated rate for ‘low risk’ procedures 0.74% to 2.42%
Principles for management of surgical site infections: Open and drain the incision Debride necrotic tissue Remove foreign bodies Manage the open wound Fill dead space and allow for wicking of drainage Do not over pack Maintain a moist wound bed Perform serial debridement s as needed. Wet to dry dressings are not an
acceptable method of debridement

11/3/2017
3
Infectious Diseases Society of America (IDSA) Guidelines for Treatment of Surgical Site Infections*
Fever 1st 48hrs & up to 4 days Evaluate, culture, consider other causes, open wound, start penicillin
and clindamycin
Fever > 4 days Evaluate, check WBC, monitor temp, culture Clean wound trunk, head, neck – cefazolin or vancomycin until
MRSA is ruled out Perineal/GI tract wound –cephalosporin + metronidazole or
levofloxacin + metronidazole or carbapenem
*Stevens, D. L., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. C., Gorbach, S. L., & ... Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clinical Infectious Diseases: An Official Publication Of The Infectious Diseases Society Of America, 59(2), 147-159. doi:10.1093/cid/ciu296
There are very few controlled trials assessing the effect of topical agents or dressings on healing rates of surgical wounds left to heal by second intention
Foam dressing are the best studied and are preferred over gauze: less pain with dressing changes, better absorption and less frequent dressing changes
Silver impregnated dressings are being used more used often after sternotomy and joint replacement surgery
Classification of burns (1st - 3rd degree system replaced)
Superficial Superficial partial-thickness Deep partial-thickness Full-thickness
Types of burns Thermal – heat or cold Chemical – Alkali, Acid, Vesicant Electrical – Voltage injuries, Arc injuries Radiation Inhalation
Electrical burns are associated with compartment syndrome, neurologic symptoms, and delayed complications
Silver sulfadiazine (SSD) – is quickly deactivated in wounds, requires frequent dressing changes to maintain antibacterial property
A Cochrane review found “some evidence that a particular antibiotic (silver sulfadiazine) applied directly to the burn actually increases the rates of infections by 8% to 80%” *
Air bag burns are caused by sodium hydroxide in aerosol from deployment. SSD and silver dressings can cause semi-permanent staining. For face injuries consider mupirocin
Pruritis associated with burns caused by release of histamine & dry skin Oral antihistamines Cool or tepid baths Moisturizer
* Barajas-Nava LA, López-Alcalde J, Roqué i Figuls M, Solà I, Bonfill Cosp X. Antibiotic prophylaxis for preventing burn wound infection. Cochrane Database of Systematic Reviews 2013, Issue 6. Art. No.: CD008738. DOI: 10.1002/14651858.CD008738.pub2
Partial thickness> 10% BSA
Burns of face, hands, genitals, feet or major joints
All chemical, electrical and inhalation burns
Persons with additional co-morbidities or injuries
Children

11/3/2017
4
70-80% of all leg ulcers are venous but there are many atypical lesions that can be misdiagnosed. The following are just some of the atypical ulcers that are seen
1. martorell's ulcer2. cutaneous vasculitis3. antiphospholipid syndrome leg ulcer4. necrobiosis lipoidica diabeticorum5. porphyria cutanea tarda leg ulcers6. calciphylaxis7. pyoderma gangrenosum8. kaposi's sarcoma9. squamous cell ca10. basal cell ca
Poor circulation at site of wound Limited arterial
vascularization Edema
Lymphedema
Non-reversal of etiology Recurrent trauma Foreign body retention Elimination/reduction
pressure Edema management
Co-Morbidities
Non-compliance
Poor Nutritional state
Poor wound care choices
Infection/Biofilms
Most common chronic wounds are: Pressure ulcers Venous ulcers Neuropathic ulcers Ischemic ulcers
Reported Rates of Recurrence Pressure ulcers 23%- 40% Venous ulcers 24%- 57% Neuropathic ulcers ~60%
Evidence-based Management Strategies for Treatment of Chronic Wounds Eplasty. . 2009 Jun 4;9:e19. 9e19http://www.pubmedcentral.nih.gov/tocrender.fcgi?journal=527&action=archive
Acute Infection Pain Purulent drainage Odor Edema Erythema Induration Systemic S/S Fever Lethargy Elevated white count Tachycardia Changes in blood pressure Confusion
Chronic Wounds Delayed healing Discolored granulation
tissue Friable granulation tissue Pocketing Foul odor Wound breakdown Increasing pain
Increasing pain and wound breakdown demonstrated 100% specificity as indicator for infection in chronic wounds
Dominant organisms in chronic wounds are Staph Aureus and Pseudomonas
Pooled research showed Staph present 80-100% and Pseudomonas present 43-100%

11/3/2017
5
Mild erythema around a new wound is normal
Generally, erythema ≥ 3cm = infection
Diabetic full thickness wounds ≥ 4 months old suspect osteomyelitis
Any chronic wound ≥ 6 months old - Consider biopsy
Biofilm development is common in older wounds
60 year old wound
75 year old wound
90 year old wound
Pedestal Formation - Bacteria attach to and move on host cells connecting the bacteria to the cytoskeleton
Tele-sensing Actively probe for information by
releasing proteins to assess conditions beyond the cell surface
Changes in the probes enable the bacteria to mount a specific response.
Smart Parasite Tempering of virulence to avoid
massive host tissue death Recruits other organisms Cause of 80% of all infections
Resist Antibiotics Secrete enzymes to modify
the ABX to an inactive form
Use efflux pumps to expel antimicrobials
Use mutants to render target proteins resistant to ABX
Persister Cells - Specialized survivor cells that become dormant and temporarily tolerant of ABX and metal ions. Then re-awaken and re-seed the host again.
BioFilms
Treatment:Surgically remove the colonized surface
Mechanical injuries Skin tears Pressure ulcers
Arterial ulcers
Venous ulcers
Diabetic ulcers
International Skin Tear Advisory Panel [ISTAP] Classification System
Category 1 Linear tear or flap. Skin edges can be approximated
to within 1mm
Category 2 Partial flap loss that can not
cover the wound bed
Category 3 Complete skin loss, no
epidermal flap

11/3/2017
6
Cleanse the wound
Realign the flap
Classify, measure
Low adhesive dressing
Maintain moist ( not wet ) surface
Lift dressings gently when changing
For wounds with flaps, draw arrow indicating direction to remove dressing to avoid lifting off flap
National Pressure Ulcer Advisory Panel’s Guidelines for staging
Blanching – Reactive hyperemiaStage I:Intact skin with non-blanchableredness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area.
Further description:The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Stage I may be difficult to detect in individuals with dark skin tones. May indicate "at risk" persons
Stage II:Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled blister.
Further description:Presents as a shiny or dry shallow ulcer without slough or bruising.* This stage should not be used to describe skin tears, tape burns, perineal dermatitis, maceration or excoriation. *Bruising indicates suspected deep tissue injury
Stage III: Full thickness tissue loss. Subcutaneous fat may be visible but
bone, tendon or muscle are not exposed.
Slough may be present but does not obscure the depth of tissue loss.
May include undermining and tunneling.
Further description: The depth of a stage III pressure ulcer
varies by anatomical location. The bridge of the nose, ear, occiput
and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow.
Bone/tendon is not visible or directly palpable.

11/3/2017
7
Stage IV: Full thickness tissue loss with
exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling.
Further description: The depth of a stage IV pressure
ulcer varies by anatomical location.
The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow.
Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis
Suspected Deep Tissue Injury: Purple or maroon localized area of
discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear.
The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue.
Further description: Deep tissue injury may be difficult to
detect in individuals with dark skin tones.
Evolution may include a thin blister over a dark wound bed.
The wound may further evolve and become covered by thin eschar.
Evolution may be rapid exposing additional layers of tissue even with optimal treatment.
Unstageable presence of slough or
eschar obscures depth of wound
Treatment Reduce/Relieve Pressure Bed – mattress overlay Chair – consult to Rehab/PT for
seating evaluation and pressure reducing seat cushion
Refer to Wound Center or Specialist
Until seen consider non-occlusive low adhesive dressing
Maintain moist ( not wet ) surface
Change dressings daily until seen by specialist
It is estimated that 7 million people in the United States have LEVD .
Venous insufficiency is a long-term debilitating disease that accounts for approximately 70 - 90% of all leg ulcers.
Each case of LEVD can cost up to $40,000 in health care resources
The annual cost for the treatment of venous leg ulcers in the U.S. is estimated to be between $570 million and $1.4 billion.

11/3/2017
8
Typically on lower half of legs at gaiter area or medial malleolus
Wounds are large and shallow with diffuse edges
Throbbing pain with generalized edema
Slough is present with heavy exudate
Hemosiderosis and lipodermatosclerosis usually present
Usually have relief of throbbing pain with elevation
Leg pain and edema that are relieved with elevation
Ankle flaring
Dry flaky itchy skin
Complaints of heaviness and dull ache in the legs
The presence of varicosities
Firm brawny edema [lipodermatosclerosis]
Dull aching or severe leg pain and leg heaviness.
Hemosiderosis
Dry flaky itchy skin
Stasis dermatitis Eczematous changes Erythema Scaling
Weeping dermatitis
May develop as a result of:
Malnutrition
Immobility
Leg trauma – most common cause Mechanical – scratching, abrasion Thermal – use of heating pad Chemical injury – OTC or Rx topicals, household cleaning
agents, plants ( poison ivy)
Peak age 60 -80 years
Venous Ulcers account for 80-90% of all leg ulcers
Estimated 7 million have venous insufficiency world wide and 3 million will progress to ulceration
Recurrence rates range from 57% to 97%
Healing: Most within 40-120 days, 25% remain unhealed at 1 year
LEVD vs. Lymphedema

11/3/2017
9
Chronic disease - impaired flow of lymph fluid caused by damage to the transport system (common)
lymph node excision Radiation fibrosis long standing venous disease
The end result - compromised lymphatic return with progressive accumulation of protein rich fluid in the interstitial space leading to fibrosis in the soft tissue & greater lymphatic obstruction.
Frequently under treated
Long term management is critical
Primary: rare, caused by congenital defects Secondary:
Commonly caused malignancy and treatment Filariasis: most common cause worldwide parasitic
infection of lymph vessels and nodes. Transmitted by mosquitoes
Stage 0-1 Reversible pitting edema beginning at the foot Negative or borderline Stemmer sign No palpable fibrosis
Stage 2 Nonpitting edema not improved with elevation Positive Stemmer sign Pronounced fibrosis Hyperkeratosis Papillomatosis
Stage 3 Lymphostatic elephantiasis Progressive fibrosis, hyperkeratosis Ulcerations
LYMPHEDEMA VENOUS INSUFFICIENCY
Non-pitting edema Not limited to the lower
leg Can involve genitals Stemmer sign No response to diuretics
Pitting edema Limited to the lower leg Does not involve
genitals No Stemmer sign Can respond to diuretics
“Painful fat syndrome” Negative Stemmer sign Tissue is painful and
bruises easily Palpate hard nodules
under the skin Abnormal distribution of
fat in lower extremities Bilateral heavy hips, thighs Non pitting edema Swelling ends at the
ankles
11/3/2017
10
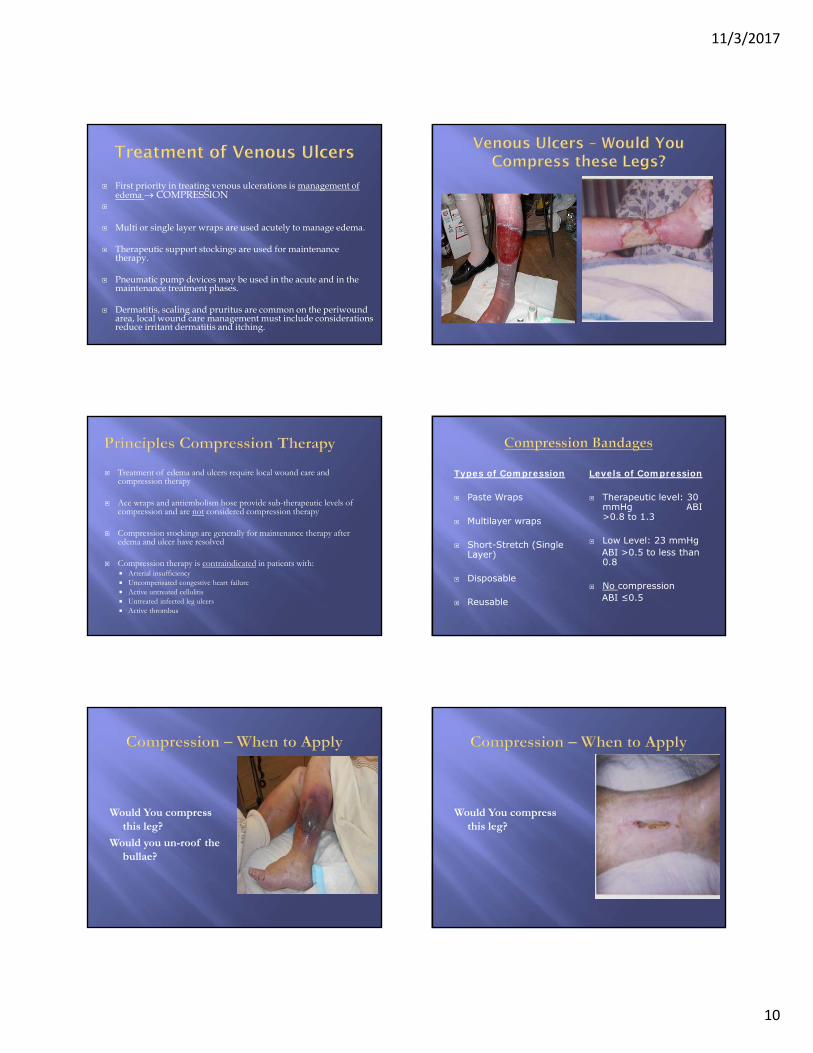
First priority in treating venous ulcerations is management of edema COMPRESSION
Multi or single layer wraps are used acutely to manage edema.
Therapeutic support stockings are used for maintenance therapy.
Pneumatic pump devices may be used in the acute and in the maintenance treatment phases.
Dermatitis, scaling and pruritus are common on the periwoundarea, local wound care management must include considerations reduce irritant dermatitis and itching.
Treatment of edema and ulcers require local wound care and compression therapy
Ace wraps and antiembolism hose provide sub-therapeutic levels of compression and are not considered compression therapy
Compression stockings are generally for maintenance therapy after edema and ulcer have resolved
Compression therapy is contraindicated in patients with: Arterial insufficiency Uncompensated congestive heart failure Active untreated cellulitis Untreated infected leg ulcers Active thrombus
Types of Compression
Paste Wraps
Multilayer wraps
Short-Stretch (Single Layer)
Disposable
Reusable
Levels of Compression
Therapeutic level: 30 mmHg ABI >0.8 to 1.3
Low Level: 23 mmHgABI >0.5 to less than 0.8
No compressionABI ≤0.5
Would You compress this leg?
Would you un-roof the bullae?
Would You compress this leg?

11/3/2017
11
Unstable heart failure/CHF Venous thrombosis ABI<0.6
Subfascial Ligation of Incompetent Perforator Veins
Subfascial Endoscopic Perforating Vein Surgery (SEPS)
Skin grafts
Bioengineered skin equivalents
NPWT
Electrical Stimulation
Limb Elevation
Weight Control
Sodium intake reduction
Exercise
Establish maintenance plan Follow-up Care Patient Education Prevention Exercise
Skin Changes Shiny, Taut, Thin Dry Skin Hair Loss Atrophy of Subcutaneous Tissue Dystrophic Nails Skin Temperature
Ischemic pain: Intermittent claudication: 70 % occlusion Nocturnal pain : 70 – 90% occlusion Rest pain: 90 % occlusion
Ankle-Brachial Index > 1.0 - 1.3 Normal < 0.9 LEAD 0.6 – 0.8 Borderline perfusion <0.5 Severe Ischemia < 0.4 Critical ischemia
Toe Brachial Index <0.64 indicates LEAD
Transcutaneous Oxygen Pressure <40mmHg indicates hypoxic limb, < 30 critical ischemia (predicts failure to heal)
Pulse Volume Recording (PVR) indicated if ABI is >1.3
Can occur on any part of the leg, commonly at or below the ankle at lateral malleolus or on the toes.
Usually small, with even or ‘cliff ’ wound edges
Often appear with dry necrotic wound bed
Deep, painful wounds with minimal or localized edema
Often pain increases with elevation Cramping, aching, fatigue/weakness Tingling, burning type pain Rest pain: constant deep aching pain

11/3/2017
12
Local wound care is determined by the perfusion state of the extremity.
Use dry dressing for dry stable eschar on non-infected arterial wounds
For moist or draining wounds, choose dressings that are changed daily
Generally, avoid dressings that are changed every 3-5 days such as hydrocolloid dressings
Limit use of debriding agents to selected situations & carefully monitor
Frequently monitor the wound if moist dressings are ordered, such as hydrogels
Monitor regularly for subtle signs of infection
Surgical Options to Improve perfusion Bypass Grafts Endovascular Procedure
Pharmacologic Therapy ACE Inhibitors – increase walking distances Cilostazol – antiplatelete agent, reduce walking pain Aspirin Pentoxifylline – second line, inconsistent results
Hyperbaric Oxygen Therapy Life style Changes
Causes of Neuropathy: Metabolic diseases - diabetes mellitus Autoimmune diseases - lupus erthematosis Organ failure Endocrine diseases - hypothyroidism Infections - Lyme disease, HIV, & Hanson’s disease Trauma - Spinal cord injury, frostbite Idiopathic – genetic or undetermined etiology
Types of Neuropathy Sensory - loss of protective sensation and altered
perception to temperature, pain and touch Autonomic Motor – foot deformities, abnormal weight bearing Automomic - decreased sweating, altered blood vessel
tone
83% of lower limb amputations occur in Diabetics
5 year survival rate after amputation ranges from 41-70%
85% of Diabetic Amputations are Preventable
Three major causes of neuropatic ulcers Poorly Fitted Shoes Repetitive Pressure Penetrating Injuries
Frostbite
Identify perfusion status – at lease 25% of those with neuropathic ulcers have LEAD as well
R/O osteomyelitis
Off load to reduce or eliminate pressure and shear stress
Debride avascular tissue if adequate perfusion.
Chose local wound care to optimize off-loading, absorb/provide moist healing environment, limit contamination opportunities
Consider need for HBO or skin grafting for stalled, non-infected wounds

11/3/2017
13
Primary and Adjunct Therapies Poor nutrition results in: Decreased wound tensile strength Decreased phagocytic activity Decreased T-cell function Increased morbidity & mortality in surgical and medical
patients
Injury Increases metabolic rate due to release of catecholamine at the
time of tissue damage. Caloric & protein needs increase If no additional insult occurs, metabolic needs return to
baseline within 10-14 days For a chronic wound metabolic needs remain high
Hepatic Proteins Serum albumin 3.5 - 5.0 g/dl Transferrin 230-390 mg/dl Pre-albumin 19.5-35.8 mg/dl
Correlate with overall prognosis, less indicative of actual nutritional status
Reflect conditions causing inflammation Trauma Infection Injury
Creatinine Indirect measurement of skeletal muscle mass Measure of long term protein status Requires normal renal function & urinary output
Hemoglobin Hematocrit B12 Folate Serum Iron Total Iron Binding Capacity [TOBC]
Protein Angiogenesis
Collagen remodeling
Wound contraction
Fat Responsible for development & stability of cell membranes
They participate actively in inflammatory response to injury
Carbohydrates Energy source, turns to glucose
Excessive levels result in impaired healing
Vitamin A - fat soluble; important in deposition of collagen, reverses effects of corticosteroids
Vitamin C - water soluble; cofactor in collagen formation; important to fibroblasts
Zinc - enzyme systems, immune competency & collagen formation
Iron - important in hemoglobin for transport of oxygen
Copper - deficiency results in weaker scar formation, decreased tensile strength

11/3/2017
14
Amino Acids
Arginine
Glutamine
Cystine
These are indispensible (essential) in conditions of intense stress – trauma, chronic disease, & wounds
Removal of necrotic tissue/foreign bodies Elimination and/or prevention of infection Eliminate dead space Absorption of exudate Maintenance of moist wound environment Thermal insulation Protecting the wound from trauma Protecting the surrounding tissue Adequate nutrition
Avoid use of cleansing agents/solutions that are intended for use on intact skin such as : Chlorhexadine gluconate 4%, povidone iodine
The following are not recommended for routine use: povidone iodine sodium hypochlorite solution (Dakin’s Solution) hydrogen peroxide acetic acid
2008 Cochrane Review concluded that tap water was as effective as saline in cleansing wounds
Hypochlorus Acid HOCI affects microbial cell permeability & kills by binding to critical cell membrane
components Ph 5.4 Reduces odor Breaks down surface debris in wound bed Stable 72 hours at room temperature and 14 days if refrigerated
• Controlled trials found no difference in incidence of post procedure infections for superficial surgical wounds with use of topical antibiotics or a petrolatum based ointment
• Contact dermatitis to neomycin and bacitracin ranges from 1.5% to 13.1% in patch testing
• Mupuricin 2% is effective against methicillin-resistant Staphylococcus [MRSA]. Avoid overuse for non-MRSA
• Hydrogen peroxide interferes with tissue migration and proliferation of fibroblasts, in surgical wounds irrigation with H2O2 has been associated with crepitus, subcutaneous tissue destruction and wound dehiscence
• Povidone-iodine interferes with tissue migration and proliferation of fibroblasts . Can lead to systemic allergic reactions if used on a full thickness wound. S/S include – flu like symptoms, renal failure and anaphylaxis
Tissue Debridement is key factor in the management of non-healing wounds.
All necrotic tissue should be debrided unless it is contraindicated No arterial blood flow to affected area
When only palliative care measures are desired by the patient/family
The patient can not tolerate anesthesia for extensive surgical debridement.
Mechanical - sharp/surgical Irrigation Autolytic - occlusive or semiocclusive dressing
(Transparent films, hydrocolloids, hydrogels, & dextranomers)
Enzymatic - proteolytic substances that breakdown necrotic tissue: collagenase
Biologic - Maggot Therapy Wet-to dry dressings – not recommended Whirlpool – not recommended

11/3/2017
15
Change dressings as frequently as needed to prevent strike through of drainage to outer dressing and maceration of periwound tissues.
Relieve causative factors if possible: Pressure reduction Remove allergens Edema reduction
Do not mix topical treatments unless the manufacturer stands behind the combination Could be a safety hazard for patient Could nullify the effectiveness Could have a negative interaction between dressing ingredients
Alginate* Antimicrobial* Collagen Composites* Contact layers* Copolymer
Foam* Gauze* Hydrocolloid Hydrogel* Hydrofiber/ Fiber Gelling Transparent Film*
* These are the most helpful to have in your clinic or office
Contact LayersTo reduce trauma to granular wound or exposed structures/organs
There are varying degrees of permeability.
Have little or no ability to absorb
Use occlusive dressings with caution
Vaseline gauze Telfa
MepitelAdaptic
Indications superficial wounds
(skin tears) cover IV sites protect intact skin
Contraindications moderate to heavily
draining wounds wounds with friable
surrounding skin cavity wounds wounds with sinus
tracts full thickness wounds
Designed to absorb small to moderate amounts of drainage
Occlusive or semiocclusive dressing composed of gelatin, pectin & carboxymethylcellulose
Indication – Primary or secondary dressing for Partial and full thickness wounds, light to moderate exudating ulcers
Autolytic debridement
Use with caution in wounds with limited perfusion
Contraindication – known sensitivity to carboxymethylcellulose, infected wounds and heavily exudating wounds
Dressings designed to absorb moderate to large amounts of drainage include: alginates, foams and sodium impregnated gauze Alginates Foams Sodium impregnated
gauze

11/3/2017
16
Derived from brown seaweed, absorbent and conform to wound shape
Interaction with wound fluid creates gelatinous appearance
Can absorb up to 20x in weight
Indications – Moderate to heavy exudatingwounds
Contraindication – dry wound
Absorbent, non-adherent layer that provides non-traumatic removal
Indication Moderate to heavily exudating wounds Primary dressing for absorption Secondary dressing for wounds with packing Protection of fragile skin
Absorbs drainage around tube
Contraindication - Eschar
Hydrofiber Composed of fibers of
carboxymethylcellulose, non-woven, white cotton like product
Quickly turns to gel when in contact with wound fluid Holds it shape for ease with
removal Absorbs 33% more than
alginate
Indication - Moderate to heavily exudating wounds
Contraindication - Known sensitivity to carboxymethylcellulose
Collagen
• Fibrous insoluble protein produced by fibroblasts
• Indication - Minimal to moderate exudatingulcers; non-infected wounds
• Contraindication - Necrotic ulcers, allergic to biomaterial source (bovine, porcine, sheep)
Combination of 2 or more products manufactured as a single dressing and performs multiple functions
Indication - Minimal to heavy exudate, healthy granulation tissue, necrotic tissue, or mixed ulcers
Contraindication - No border of intact skin for anchoring the dressing
Moisture retentive dressings helpful in maintaining a moist wound environment for wounds with little or no drainage.
Water or glycerin based hydrating dressings
Contraindication - Heavily exudating wounds
Three forms:1. Amorphous2. Impregnated gauze3. Sheet

11/3/2017
17
Iodine is a well know antimicrobial agent
0.9% iodine is carried in polysaccharide beads
Provides a slow sustained release of iodine in non-cytotoxic concentrations
High rate of absorption from exudating ulcers.
No documented cases of bacterial resistance.
Contraindicated in known iodine allergy, dyes or seafood
Reduces the activity of collagenase, should not be used together
Can break down biofilms
Broad spectrum including MRSA and VRE
Non-toxic, active and readily available
Antimicrobial and mild anti-inflammatory
Silver sulfadiazine Effective for gram positive & negative bacteria as well as anaerobes and yeast Prolonged use may delay re-epithealization Do not use on sulfa sensitive patients
Precautions/Contraindications Should not be used with collagenase Use with caution in children [silver toxicity] Should not be used within 24hours of MRI Should not be used during pregnancy or lactation Should not be used in persons with silver allergy
Effective for gram positive & negative bacteria, anaerobes, fungi, yeast, and viruses
Low incidence of sensitivity
In a moist environment, dressings impregnated with silver can release silver ions over several days
Available in many forms Elemental Organic Inorganic
Some silver dressings require the use of sterile water for wound cleansing, normal saline may inactivate silver ions
Contains active Leptospermum Honey
Indications: Debridement, lowers wound pH, can breakdown biofilm
Available: Gel, alginate, hydrocolloid
Contraindications – allergy to honey, no evidence that sensitivity to bee venom is a contraindication
Indications: malodorous wounds, fistulas
Absorbs drainage and toxins
Typically used in Palliative/Hospice Care
Topical debriding agent may be ordered for eschar or slough on the wound bed

11/3/2017
18
Preserve lifeSave limb or functionPrevent or control infectionEliminate or minimize pain and stressHeal the woundStabilize the wound if healing is not a realistic
goalPalliative management of symptoms for terminalpatients
Pressure Injuries – reduce/prevent further pressure
LEVD – manage edema Compression
LEAD – improve circulation Revascularize
LEND - prevent further pressure Offload