pathophysiology & management of acid base and common electrolyte imbalance in critically ill dr....
TRANSCRIPT

Pathophysiology & Management of Acid Base and Common Electrolyte Imbalance
in Critically ill
Dr. Shalini Saini
University College of Medical Sciences & GTB Hospital, Delhi

Acid Base Equilibrium
What is Acid Base Equilibrium About?
?Buffers?
Fixed Cation?
Base Excess/ Deficit?
Anion Gap?
Acid Base Equilibrium
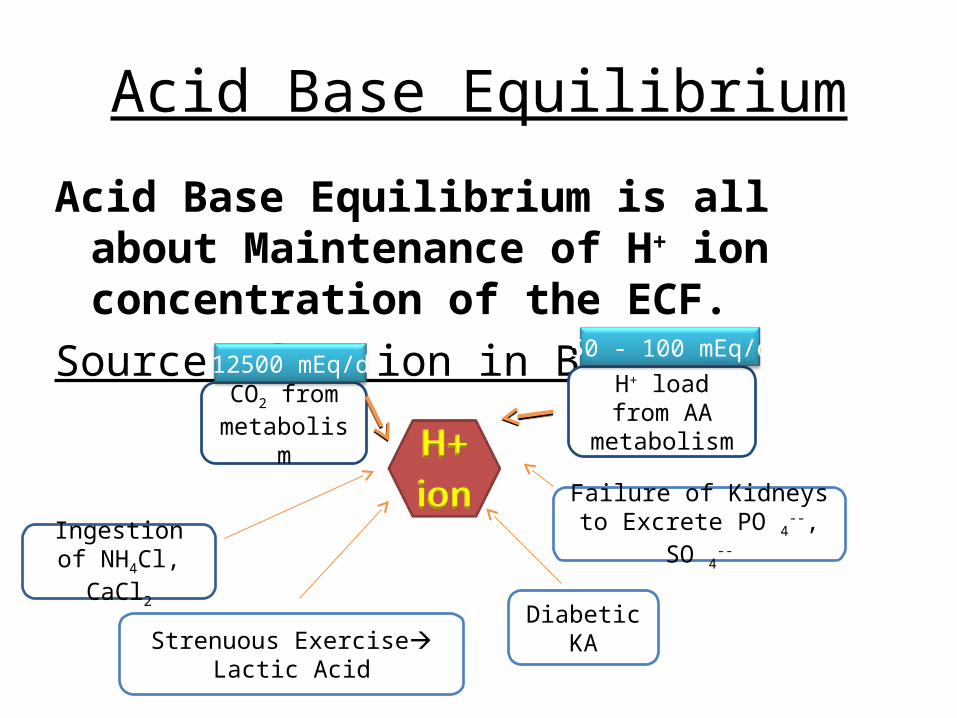
Acid Base Equilibrium is all about Maintenance of H+ ion concentration of the ECF.
Source of H+ ion in Body:
CO2 from metabolism
H+ load from AA metabolism
Strenuous Exercise Lactic AcidDiabetic KA
Ingestion of NH4Cl, CaCl2
Failure of Kidneys to Excrete PO 4
--, SO 4--
12500 mEq/d50 - 100 mEq/d

Some Basic Chemistry
Definitions:
Arrhenius(1903):– Acid: H+ Donor in Solution– Base: OH- Donor in Solution
Browsted and Lowry(1923):– Acid: Proton Donor– Base: Proton Acceptor

Some Basic Chemistry
pH (Potenz or Power of Hydrogen): Sorenson
Negative logarithm of H+ ion concentration to the base of 10
Why pH?• Normal H+ ion conc: 0.00004meq/L or 40nEq/L or 4x10-9 mol/L• pH converts decimal numbers & takes away negative sign.• Normal pH: 7.35-7.45• Normal H+ Conc: 0.00002mEq/L – 0.0001 mEq/L

Acid Base Equilibrium:
Solutions:
When substances are added to water, 3 simple rules have to be satisfied at all time:1. Electrical Neutrality2. Mass conservation3. Dissociation Equilibrium
Clinical Concepts:Base Excess: Amount of Acid or Alkali required to return plasma in vitro
to normal pH under standard conditions( pH 7.4, PCO2 40 , temp 37 C)
Standard BE: BE calculated for Anemic Blood (Hb = 6gm%).– Since Hb effectively buffers plasma & ECF to a large extent.
• Quantity of Acid or Alkali required to return plasma in-vivo to a normal pH under standard conditions
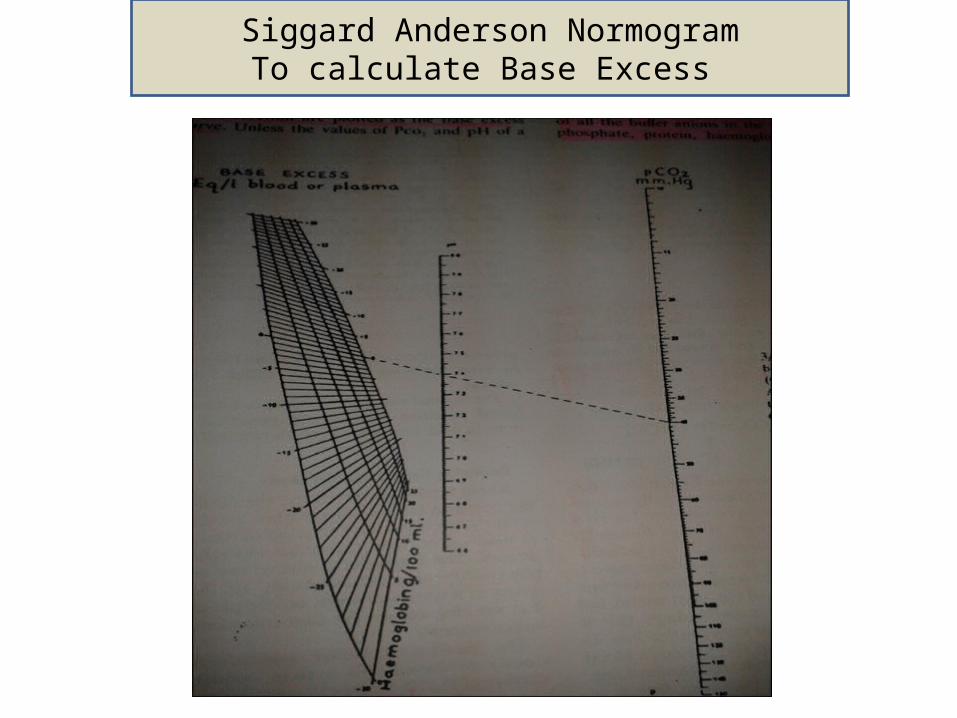
Siggard Anderson NormogramTo calculate Base Excess

Acid Base Equilibrium:The Henderson-Hasselbalch Equation:
H2 CO3 <====> H+ + HCO3-
=> Ka = [H+ ][HCO3 ]/ H2 CO3
Taking Logarithm on both sides & Rearranging: pH= pKa + log10[HCO3
-]/SX*PCO2
pKa = 6.1, S = 0.03(solubility coefficient), PCO2 = 40, HCO3 =25
On putting values & solving, pH = 7.4 Significance:• Includes components of both Metabolic & Respiratory Acid base disorders• Value of any one variable can be determined if other two known. Mostly HCO3
- is calculated
• pH determined by ratio of [HCO3-]/PCO2
• Increase=> alkalosis, Decrease => Acidosis

Anion Gap:• Estimate of relative abundance of unmeasured anions• Footprint of metabolic acidosis • UC & UA in electrochemical balance equation: Na + UC = (Cl + HCO 3 ) + UA
Rearranging equation : UA-UC (AG) = [Na+] - {[HCO3-] + [Cl-]}
• Normal Value: 8-12mEq/L• ↑ AG reflects ↑ Unmeasured Anion• Unmeasured Anions- Albumin,Phosphate, Sulphate, Organic acid.• 1mg/dl fall in Albumin, AG↓ by 3meq/l • High AG acidosis- Ketones, Lactate, Methanol.• Normal AG acidosis- Diarrhea.

Clinical Concepts:
Acid Base Equilibrium:• Elimination of Acid• Recovery/Regeneration of Base
Mechanisms that keep pH stable Buffering Compensation Correction
Clinical Concepts:
Buffers:
Definition: A substance that can bind or release H+ ions in solution, thus keeping the pH of the solution relatively constant despite addition of large amounts of acid or base.
For Buffer HA,HA <====>H+ + A-
pH = pKa + log [A-]/[HA]
– When [A-] = [HA], pH= pK, buffering capacity is maximum.
Clinical Concepts:
Most buffers are weak acids (H+ buffer) & their Na+ Salts (Na+ buffer)• Strong Acids Buffered by Na+ Buffer
• HCl + Na Buffer <====> H+ + Cl- +Na+ + Buffer <====> H Buffer + NaCl• Strong Bases Buffered by H+ buffer
• NaOH + H Buffer <====> Na+ + OH- + H+ + Buffer <====> Na Buffer + H2O
Buffer Effectiveness Depends on:• Quanitity
– H2CO3 /HCO3
- - Most important Extracellular Buffer– Protein Buffers – Most important Intracellular Buffer
• pKa
– Buffering capacity maximum when pH=pKa

Clinical Concepts:Buffers in ECF:• Carbonate-Bicarbonate Buffer 53%
– Plasma (35%)– Erythrocyte(18%)
• Hemoglobin 35%• Plasma Proteins 7%• Organic & Inorganic Phosphates 5%
Buffers in ICF:• Intracellular Proteins• H2PO4-HPO4
- system
Intracellular buffers are responsible for ~85% buffering in Met. Acidosis and ~35% in Met Alkalosis and almost complete buffering in Respiratory Acidosis and Alkalosis.

Clinical Concepts:
Bicarbonate Buffer:
• HCl + NaHCO3- <==>NaCl + H2CO3<==>NaCl + H2O + CO2
• Useful only for Metabolic Acidosis
Hb System:
• Both Respiratory & Metabolic Acidosis in ECF

Hemoglobin buffer
• Chloride Shift • Buffers H+ directly• HCO3 - diffuses out
• Cl diffuses in
Clinical Concepts:
Protein Buffer:• Predominant Intracellular Buffer – Large total concentration• pK = 7.4• AA have Acidic & Basic Free radicals
.COOH + OH- <====> COO- + H2O
.NH3OH + H+ <====> NH3 + H2O
Phosphate Buffer:• pK = 6.8• Predominantly Intracellular• Also in renal tubular
HCl + Na2HPO4 <====> NaH2PO4 + NaCl
NaOH + NaH2PO4 <====> Na2HPO4 + H2O
Clinical Concepts:
Compensation:Pulmonary Compensation
H+ + HCO3-<====> H2CO3 <====>CO2 + H2O
• H+ acts on medullary centres. – Metabolic Acidosis – Increased Ventilation– Metabolic Alkalosis – Depression of Ventilation• Minute ventilation increases 1-4l/min for every 1mmHg increase in
PaCO2
Clinical Concepts:
Renal Compensation:
Mechanisms:1. Reabsorption of filtered HCO 3
- (4000-5000 mEq/d)
2. Generation of fresh bicarbonate3. Formation of titrable acid – (1mEq/Kg/d)4. Excretion of NH4
+ in urine

PERITUBULAR BLOODPERITUBULAR BLOOD RENAL TUBULAR CELLRENAL TUBULAR CELL
GLOMULAR FILTRATEGLOMULAR FILTRATE
HCO3- + H+
CO2
HCO3- + H+
HCO3- + H+
HCO3- Na+ HPO4
2- Na+ NH3 Na+
H2CO3
CO2 + H2 O
H2O
H2PO4-
H2PO4-
NH4+
NH4+
1. NaHCO3
2. NaHCO3
3. NaHCO3
MAJOR RENAL MECHANISMS RESPONSIBLE FOR H+ EXCRETION/HCO3- RETENTIONMAJOR RENAL MECHANISMS RESPONSIBLE FOR H+ EXCRETION/HCO3- RETENTION
CO2 can be obtained from blood or the tubular fluidCO2 can be obtained from blood or the tubular fluid
Glutamine
CO2
CA

Acidemia or Acidosis? Alkalemia or Alkalosis?
Any condition that disturbs acid -base balance by increasing H+ through endogenous production,↓ buffering capaity, ↓ excretion, or exogenous addition is termed as ACIDOSIS Any condition that ↓ H+ is termed as ALKALOSIS
Acidemia or Alkalemia refer to net imbalance of H+ in blood.

Defining acid base disordersDisorder Primary change Compensatory
responseRespiratory AcidosisAlkalosis
↑PaCO2
↓PaCO2
↑HCO3
↓HCO3
MetabolicAcidosis Alkalosis
↓HCO3
↑HCO3
↓PaCO2
↑PaCO2

Normal reference range
pH 7.35-7.45
HCO3- 22-26meq/l
PaCO2 35-45mmHg
PaO2 80-100mmHg
Base excess/Deficit -2 to +2meq/l
Anion gap 8 to 12 meq/l
A-aO2 5-25mmHg
SaO2 96-100%

Prediction of Compensatory Responses on Simple Acid Base DisordersPrediction of Compensatory Responses on Simple Acid Base Disorders
Disorder Prediction of CompensationMetabolic Acidosis • For every 1mmol/l ↓ in HCO3
- → 1mm Hg ↓ in PaCO2
• Expected PaCO2 = 1.5 (HCO3- ) + 8
• PaCO2 should approach last two digits of pH
Metabolic Alkalosis For every 1 mmol/l ↑ in HCO3- ,↑ PaCO2 By 0.7mmHg
Respiratory Alkalosis
Acute [HCO3- ] will ↓ 2mmol/L per 10 mmHg ↓ in PaCO2
Chronic [HCO3- ] will ↓ 4mmol/L per 10 mmHg ↓ in PaCO2
Respiratory Acidosis
Acute [HCO3- ] will ↑ 1mmol/L per 10 mmHg ↑ in PaCO2
Chronic [HCO3- ] will ↑ 4mmol/L per 10 mmHg ↑ in PaCO2

General approach to acid-base disorder
pH
AcidemiapH <7.35
NormalpH7.35-7.45
AlkalemiapH> 7.45
Normal or mixed disorder↓HCO3 ↑PaCO2
Metabolic acidosis
Respiratory acidosis
↑HCO3 ↓PaCO2
Metabolic alkalosis
Respiratoryalkalosis

Diagnosis of acid base disturbance
Step -1: Is there an acid – base disturbance? look at PaCO 2 & HCO3 , whether in normal range. If normal range,
no acid-base disturbance or rule out mixed disorder. If abnormal, proceed to step 2. Step-2: Is there acidemia or alkalemia? Step-3: What is primary acid base disorder? Step-4: Calculate the expected compensation? Determine whether actual value matches with the expected compensation. Matching of both confirms diagnosis of primary disorder.
Step 5: Determine the presence of mixed acid-base • Check the direction of changes- As per ‘Rule of same direction’, in simple acid-base disorder PaCO2 & HCO3 changes from normal in same
direction. If changes occur in opposite direction; mixed disorder.• If expected compensation > or < than calculated compensation; mixed.• Check for anion gap :
i. If high AG , High AG metabolic acidosis.
ii. If normal AG , Non-AG metabolic acidosis.
• Case scenario: A 66 year old man seen in emergency room. He has had 8 days of severe diarrhea, abdominal pain, & decreased intake, but adequate intake of liquids. His medical history is significant for diabetes & hypertension. Presently on enalapril, aspirin, atenolol, metformin. Physical examination: B.P 105/70, Pulse 72/min, R.R 32. Lab report: Na 136, K 3.9, Cl 114, HCO3 13, creatinine 1.2, glucose 128
Urine: pH 6, Na 32, K 21, Cl 80 ABG: pH 7.27, PO2 90, PCO2 30
Which acid base disorder is present?

• pH low & ↓ HCO3 Metabolic acidosis.
• Respiratory compensation :
Expected PCO2 = 1.5 X 13 + 8 = 27.5 (Adequate)
• Anion Gap = 136– (114 + 13) = 9 (Normal)
Non-AG Metabolic Acidosis
Metabolic acidosis
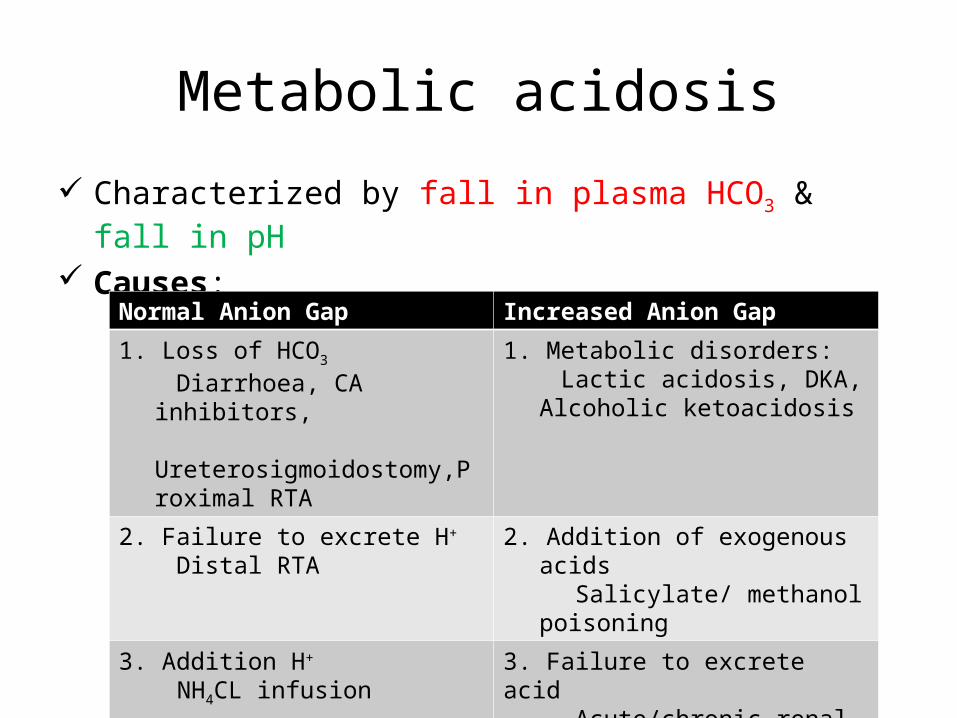
Characterized by fall in plasma HCO3 & fall in pH Causes:
Normal Anion Gap Increased Anion Gap
1. Loss of HCO3
Diarrhoea, CA inhibitors, Ureterosigmoidostomy,Proximal
RTA
1. Metabolic disorders: Lactic acidosis, DKA, Alcoholic
ketoacidosis
2. Failure to excrete H+ Distal RTA
2. Addition of exogenous acids Salicylate/ methanol poisoning
3. Addition H+
NH4CL infusion3. Failure to excrete acid Acute/chronic renal failure
Clinical manifestations:• Pulmonary changes- Kussmaul’s breathing( deep,regular,sighing respiration)• Cardiovascular changes- if severe (pH<7.2), ↑ susceptibility for cardiac arryhthmias, ↓ response to ionotropes & secondary hypotension.• Neurological changes- headache, confusion to coma.• Other- Renal failure
Diagnosis:• ABG values - ↓ HCO3 , ↓ pH, compensatory ↓ PaCO2

Treatment of Metabolic Acidosis:1. Specific management of underlying disorder
As a rule treat underlying disorder meticulously. It may be the only required treatment for mild to moderate acidosis & Non-AG acidosis.
2. Alkali therapy
Reserved only for selective patients with Severe Acidemia (controversial) & for Non-AG Acidosis Indications: pH<7.2 with sign of shock or myocardial irritability. HCO3 < 4meq/l
Severe Hyperchloremic acidemia Goal: To return pH to about 7.2 & HCO3 ↑ by 8-10meq/l.
Amount of HCO3 required= (Desired HCO3 – Actual HCO3 ) X0.3 X Bodywt.
Half of the correction is given f/b repeat ABG after sometime.

Case scenario: ABG of a patient with CHF on frusemidepH 7.48, HCO3 34 mEq/l, PaCO2 48 mmHg
• pH = alkalosis• HCO3 = s/o metabolic alkalosis
• PaCO2 = s/o compensation
• Rise in PaCO2 = 0.75 x rise in HCO3 = 0.75 x (34-24) = 7.5
Expected compensation = 40+7.5= 47.5 mmHg ~ actual PaCO2 s/o simple acid base disorderSo patient has primary metabolic alkalosis due to diuretics

Metabolic alkalosis
Characterized by ↑ HCO3 , ↑ pH,& compensatory ↑ in PaCO2
Occurs when there is excess of buffers present, raising systemic pH. Clinical features:• CNS- ↑ neuromuscular excitability leading to paresthesia, headache.• CVS- hypotension & arrythmias• Others- weakness, muscle cramps
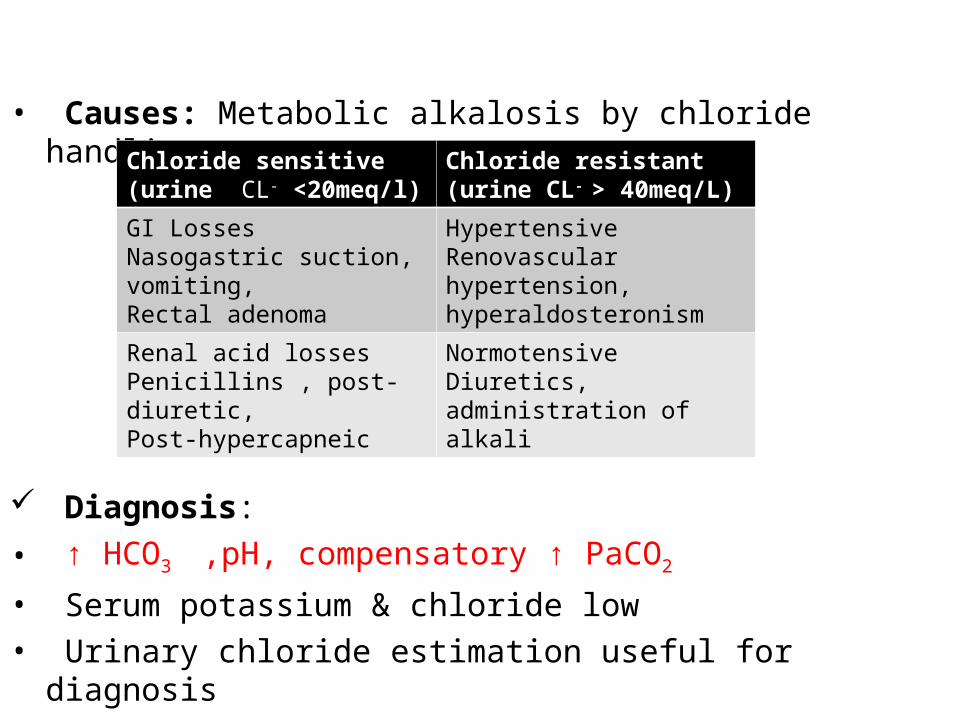
• Causes: Metabolic alkalosis by chloride handling
Diagnosis:• ↑ HCO3 ,pH, compensatory ↑ PaCO2
• Serum potassium & chloride low• Urinary chloride estimation useful for diagnosis
Chloride sensitive(urine CL- <20meq/l)
Chloride resistant(urine CL- > 40meq/L)
GI LossesNasogastric suction, vomiting,Rectal adenoma
Hypertensive Renovascular hypertension, hyperaldosteronism
Renal acid lossesPenicillins , post-diuretic,Post-hypercapneic
Normotensive Diuretics, administration of alkali
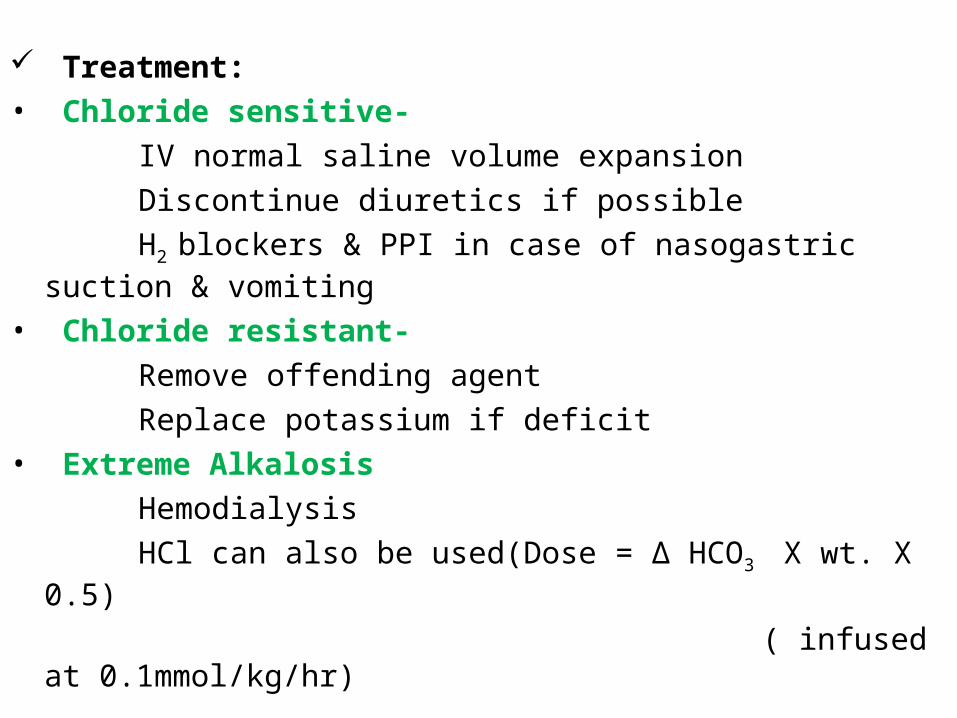
Treatment:• Chloride sensitive-
IV normal saline volume expansion Discontinue diuretics if possible H2 blockers & PPI in case of nasogastric suction & vomiting
• Chloride resistant-
Remove offending agent Replace potassium if deficit• Extreme Alkalosis
Hemodialysis HCl can also be used(Dose = ∆ HCO3 X wt. X 0.5)
( infused at 0.1mmol/kg/hr)

Case scenario: Following sleeping pill ingestion, patient presented in drowsy state with sluggish respiration with rate of 4/min
pH 7.1, HCO3 28 mEq/l, PaCO2 80 mmHg, PaO2 42 mmHg
• pH = acidosis
• PaCO2 = s/o respiratory acidosis
• PaO2 = moderate hypoxemia
• HCO3 = s/o compensation
• Rise in HCO3 = 0.1 x rise in PaCO2 = 0.1 x (80-40) = 4 mEq/l
Expected compensation = 28 mEq/l ~ actual PaCO2 s/o simple acid base disorder
So patient has primary respiratory acidosis due to respiratory failure, due to sleeping pills

Respiratory Acidosis
Characterised by ↑ PaCO2 , ↓ pH, & compensatory ↑ HCO3
Causes:• Airway obstruction- Foreign body,Aspiration, Obstructive sleep apnea, Laryngospasm or Brochospasm.• Neuromuscular disorders of respiration- Myasthenia gravis, Guillain-Barre syndrome, Tetanus, Botulism, Hypokalemia, Cervical spine injury, Obesity• Central respiratiory depression- Drugs(Opiates, sedatives),Brain trauma• Respiratory disorder- Severe Pulmonary edema, Asthma, ARDS, COPD, Pulmonary fibrosis.

Clinical presentation: Headache, confusion, irritability, delirium Severity relates with the rapidity of development of disturbance. Treatment:A. General measures 1. Major goal is to identify & treat underlying cause. 2. Establish patent airway & restore oxygenation. 3. If patient with chronic hypercapnia develops sudden ↑ PaCO2 , search for aggravating factor, vigrous treatment of pulmonary infection, brochodilator therapy, removal of secretions. B. Oxygen therapy 1. In Acute , major threat is hypoxia, so oxygen is supplemented. 2. In Chronic hypercapnia, oxygen therapy instituted carefully & in lowest possible concentration.

C. Mechanical Ventilatory Support 1. Patient selection: In acute acidosis, early use of ventilatory assistance advised. In chronic, a more conservative approach is advisable because of great difficulty in weaning. 2. Indications: • Unstable,symptomatic or progressively hypercapneic.• If signs of muscle fatigue• Refractory severe hypoxemia• Depression of respiratory centre3. Rate of correction PaCO2 should be gradual & target is usually patient’s prior stable level & in acute should be normal level.D. Alkali Therapy Avoid except in severe acidemia or severe bronchospasm.
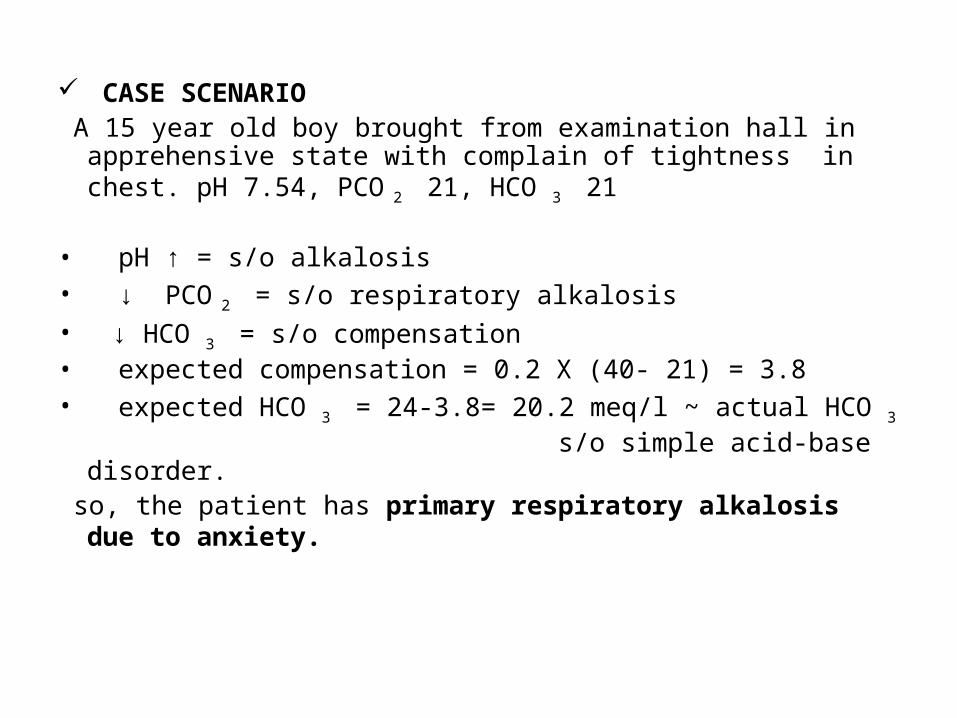
CASE SCENARIO A 15 year old boy brought from examination hall in apprehensive state
with complain of tightness in chest. pH 7.54, PCO 2 21, HCO 3 21
• pH ↑ = s/o alkalosis• ↓ PCO 2 = s/o respiratory alkalosis• ↓ HCO 3 = s/o compensation• expected compensation = 0.2 X (40- 21) = 3.8 • expected HCO 3 = 24-3.8= 20.2 meq/l ~ actual HCO 3 s/o simple acid-base disorder. so, the patient has primary respiratory alkalosis due to anxiety.

Respiratory Alkalosis
Characterised by ↓ PaCO2 due to hyperventilation & leads to ↑ pH.
Diagnosis: ↓ PaCO2 (<35mmHg), ↑ pH , compensatory ↓ HCO3
serum HCO3 does not fall below 15meq/l unless metabolic
acidosis is present. Causes:
1. Hypoxemia- Pulmonary disease( Pneumonia, Fibrosis, Edema,Emboli), CHF, Hypotension, Severe anemia, High altitude. 2. Direct stimulation of respiratory centre- Psychogenic or voluntray hyperventilation, Pain, Hepatic failure, Neurological disorder. Clinical features: Headache, arrythmias, tetany, seizures. Severity of hypocapnia constitutes grave prognosis.

Treatment• Vigrous treatment of the underlying cause• Mild alkalosis with few symptoms needs no treatment.• As hypoxemia is common cause, oxygen supplememtation is essential.

Case scenario
Known case of COPD develops severe vomiting pH 7.4, HCO3 36meq/l, PCO2 60mmHg
• pH normal = s/o either no acid –base disorder or mixed• ↑ PCO2 = s/o respiratory acidosis ( due to COPD)
• ↑ HCO3 = s/o metabolc alkalosis ( due to vomiting)
the patient has mixed disorder , respiratory acidosis & metabolic alkalosis.
Normal pH can be due to end result of opposite changes caused by primary disorder.
Mixed Acid Base Disorders
• Difficult to diagnose• Suspected whenever pH is normal or if apparent compensation is not adequate in a patient with known primary acid-base disorder.• Mixed metabolic & respiratory acidosis occurs when respiratory compensation is insufficient .• Gram- negative sepsis is a common cause of respiratory alkalosis & metabolic acidosis .
Summary:• Acid Base Homeostasis is all about maintenance of normal H+
concentration.• Changes in acid base status of ECF have profound and often
unpredicatable clinical and laboratory effects, more so during anaesthesia.
• pH scale is a negative logarithmic scale.• Anion gap must always be calculated to decipher more accurately the
complex acid-base disorders in critically ill patients.• Bicarbonate therapy must be used with caution in view of it’s various
deleterious effects.
References
• Miller’s Anesthesia, 7th Edition• Civetta, Taylor, Kirby; Critical care 4th Edition• Wylie And Churchill Davidson’s A Practice of
Anaesthsia, 5th Edition• Morgan Michael , 4th Edition• Clinical Application of Blood Gases, Shapiro, 5th
Edition • Harrison’s Principles of Internal Medicine, 16th
Edition

THANK YOU ALL!!