pathologies of the trachea department of thoracic, general and oncological surgery medical...
TRANSCRIPT

PATHOLOGIES OF THE TRACHEA
Department of Thoracic, General and Oncological SurgeryMedical University of Lodz
Head of the Department: Prof. Marian Brocki
Author of the lecture: Edyta Santorek-Strumiłło, MD

ETIOLOGY OF TRACHEAL STRICTURES
prolonged endotracheal intubation, prolonged endotracheal intubation, tracheostomy,tracheostomy, direct and indirect tracheal injuries,direct and indirect tracheal injuries, aspiration of a foreign body into the tracheal lumen, aspiration of a foreign body into the tracheal lumen, tracheal burns, tracheal burns, tracheal wall infections, tracheal wall infections, other (sarcoidosis, tuberculosis, histoplasmosis), other (sarcoidosis, tuberculosis, histoplasmosis), primary benign and malignant tracheal tumors, primary benign and malignant tracheal tumors, malignant infiltration of the trachea. malignant infiltration of the trachea.
92 % of strictures
Introduction::
• An increasing number of patients treated due to respiratory failure by prolonged endotracheal intubation, mechanical ventilation and tracheostomy causes the increase of a number of airway obturations.
• According to different authors the rate of complications of tracheostomy ranges from 2 % to 21%.
• There is only a low percentage of tracheal stenoses that are symptomatic and demand surgical treatment.

ENDOTRACHEAL INTUBATION
Endotracheal intubation is a minimally-invasive procedure. A plastic tube is introduced through the month or nostrils into the tracheal lumen usually under a laryngoscope control and is fixed within the trachea by the inflation of a special balloon.
It is a routine medical procedure used, among others, during general anesthesia or resuscitation.

COMPLICATIONS OF ENDOTRACHEAL INTUBATION
injuries of the lips, teeth, tongue, tonsils, throat, larynx, injury of the vocal cords, injury of the trachea laryngeal edema or spasm after intubation tube removal, acute pulmonary distention or tension pneumothorax infection of the airway, errosions of the tracheal wall caused by an endotracheal tube
cuff pressure and chronic ischemia

A Fome-Cuf endotracheal tube

TRACHEOSTOMY
Tracheostomy is one of the most frequent procedure performed in
intensive care units, laryngologic and surgical departments as it
preserves the patency of the airway and enables effective
mechanical ventilation in patients with respiratory failure.
INDICATIONS FOR TRACHEOSTOMY : obstruction of the airway control of the secretions mechanical ventilatory support in respiratory failure decrease of dead respiratory space and the treatment for sleep apnea

TRACHEOSTOMY
in patients that require mechanical ventilation for longer than
14 days tracheostomy should be performed as soon as
possible when their general state is stable enough.
duration of endotracheal intubation shouldn’t be longer than
7 days and if extubation is not possible within next 5-7 days
due to patient’s general state tracheostomy must be done.

Relative anatomyRelative anatomy
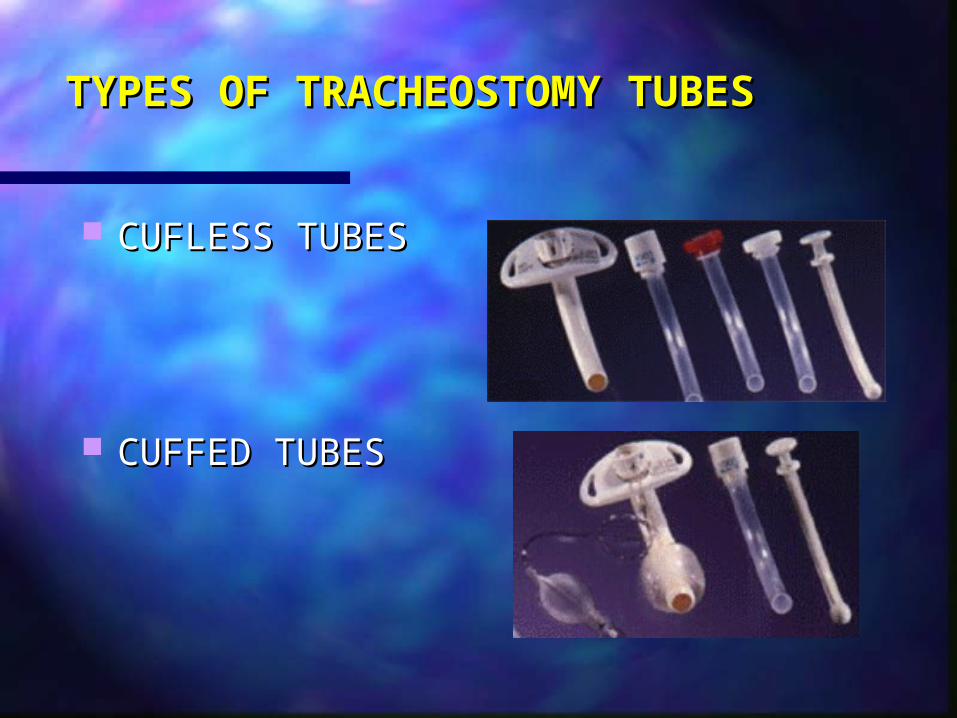
TYPES OF TRACHEOSTOMY TUBESTYPES OF TRACHEOSTOMY TUBES
CUFLESS TUBESCUFLESS TUBES
CUFFED TUBESCUFFED TUBES
TECHNIQUE
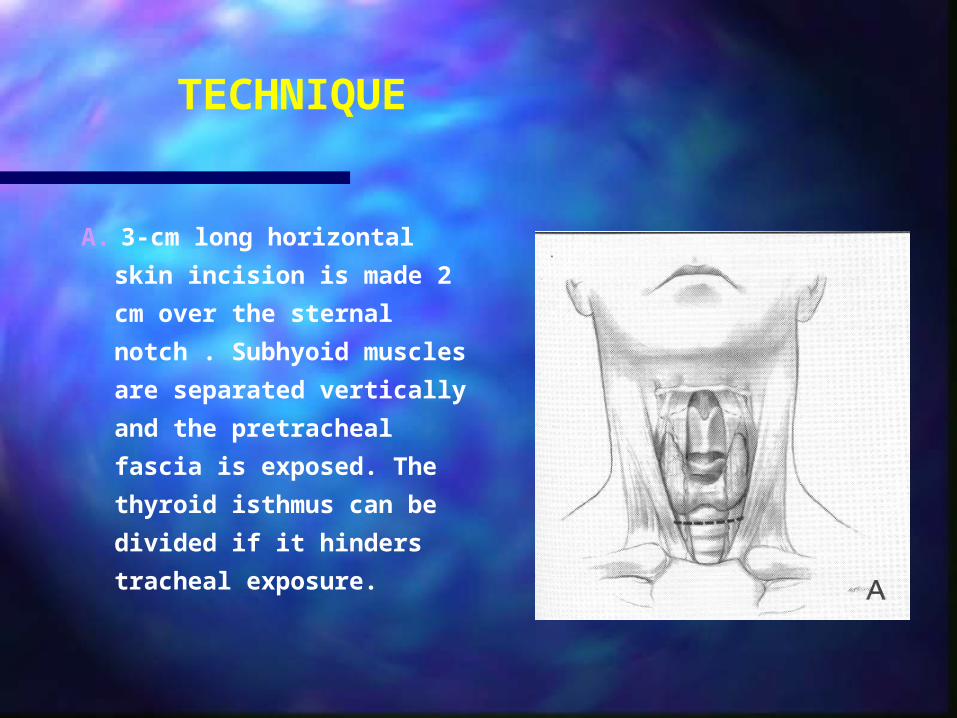
A. 3-cm long horizontal skin
incision is made 2 cm over the
sternal notch . Subhyoid
muscles are separated
vertically and the pretracheal
fascia is exposed. The thyroid
isthmus can be divided if it
hinders tracheal exposure.

TECHNIQUE
B. Tracheostomy is usually
done below the second
tracheal ring. The third
ring is elevated with a
sharp hook and a disk is
excised using a surgical
blade No 11.
TECHNIQUE
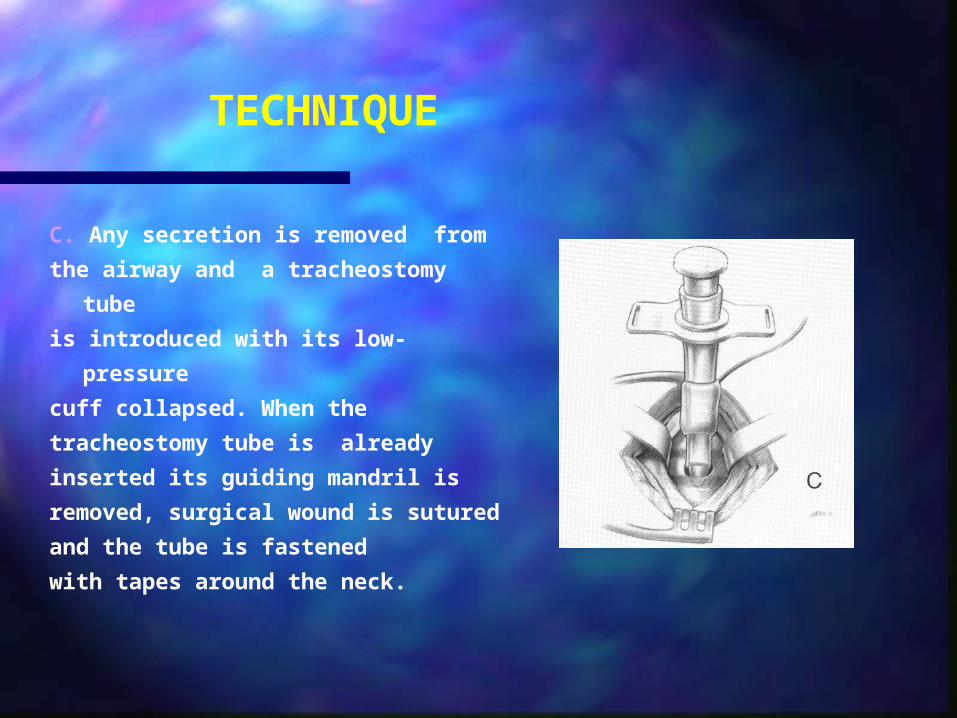
C. Any secretion is removed from
the airway and a tracheostomy tube
is introduced with its low-pressure
cuff collapsed. When the
tracheostomy tube is already
inserted its guiding mandril is
removed, surgical wound is sutured
and the tube is fastened
with tapes around the neck.

TECHNIQUE
D. In the case of initracheostomy
or if tracheostomy is performed
due to emergency conditions it is
done through the cricothyroid
membrane. A small skin incision is
made over the membrane and it
punctured with a mandril of
smaller diameter. The procedure is
carried out under local anesthesia.

TRACHEOSTOMY

COMPLICATIONS OF TRACHEOSTOMY –6%
EARLY COMPLICATIONS :
hemorrhage abscess in tissues
sourrounding a stomy subcutaneous emphysema mediastinal emphysema dislocation of a tracheostomy
tube tracheostomy tube obstruction
LATE COMPLICATIONS :
tracheoarterial fistula tracheoesophageal fistula postintubation tracheal
stricture tracheomalacia persistent tracheocutaneous
fistula

MAIN FACTORS RESPONSIBLE FOR POST-INTUBATION AND POST-TRACHEOSTOMY
TRACHEAL STENOSES :
compression of an endotracheal tube to tracheal mucosa
movements of an endotracheal tube along the tracheal wall
bad surgical technique and improper care of tracheostomy
prolonged intubation pressure within a cuff over 30 mmHg infections patient’s general state (hypotension, hypoxia).

Tracheal stenosis after long-term Tracheal stenosis after long-term endotracheal intubation or tracheostomyendotracheal intubation or tracheostomy
Incidence: ~31%Incidence: ~31% Site: Cuff level or stoma levelSite: Cuff level or stoma level Degree of stenosis: Degree of stenosis: 11~25% in 18% patients, 11~25% in 18% patients,
26~50% in 22% patients, 26~50% in 22% patients,
>50% in 3.7% patients >50% in 3.7% patients
only 3~20% were symptomatic (stenosis>30%)only 3~20% were symptomatic (stenosis>30%)
SSymptomsymptoms: shortness of breath: shortness of breath,, inspiratory stridor inspiratory stridor,, expiratory wheeze expiratory wheeze

Tracheal stenosis after long-term Tracheal stenosis after long-term endotracheal intubation or tracheostomyendotracheal intubation or tracheostomy -
diagnosis- chest an neck roentgenograms chest an neck roentgenograms - rrigidigid/flexible/flexible bronchoscopy bronchoscopy - computed tomographycomputed tomography- spiral computed tomographyspiral computed tomography- magnetic resonance imaging magnetic resonance imaging - spirometry spirometry - laryngoscopy, laryngoscopy, - fluoroscopy, fluoroscopy, - virtual bronchoscopy on the basis of computed picture virtual bronchoscopy on the basis of computed picture
analysisanalysis- EBUS – endobronchial ultrasound. EBUS – endobronchial ultrasound.

CLASSIFICATION OF TRACHEAL STENOSES :
Classical classification : glottic stenosis subglottic stenosis stenosis of the cervical part of the
trachea stenosis of the mediastinal part of
the trachea
McCaffrey’s classificationI – subglottic stenosis shorter than 1 cm II – isolated subglottic stenosis longer than 1 cmIII – subglottic stenosis without glottis inclusion IV – stenosis including the glottis
Cotton’s classification - based on the grade of the tracheal lumen stenosis
I - stenosis < 70% II - 70% < stenosis< 90% III - stenosis > 90% IV - complete obstruction of the trachea

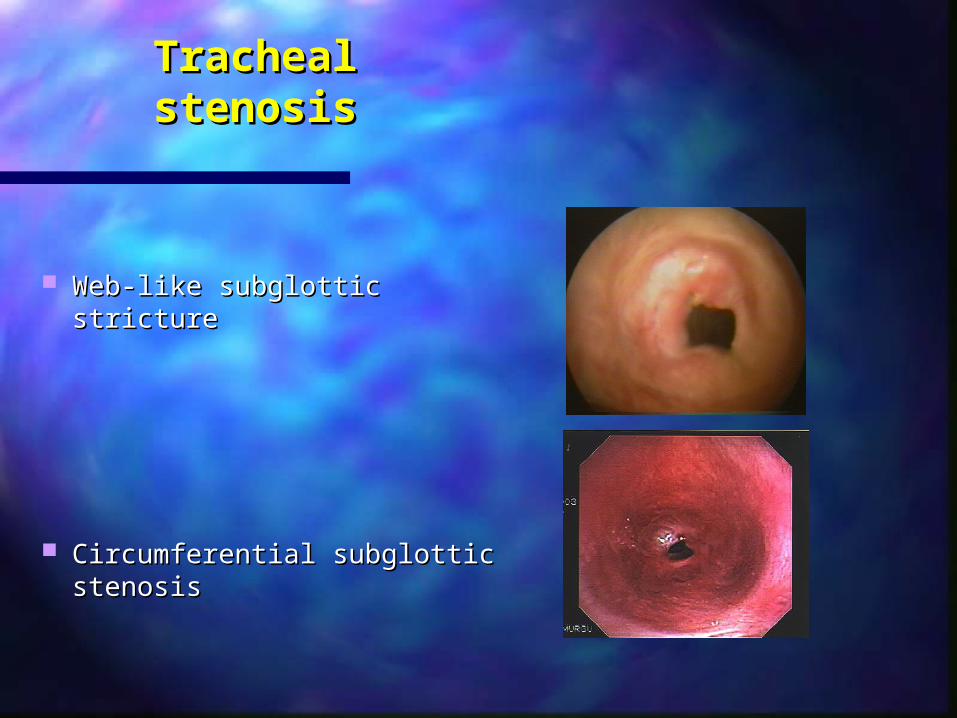
Tracheal stenosisTracheal stenosis
Web-like subglottic strictureWeb-like subglottic stricture
Circumferential subglottic stenosisCircumferential subglottic stenosis

TREATMENT OF TRACHEAL STENOSES
endoscopic dilation of a strictureendoscopic dilation of a stricture (mechanical dilators, balloon (mechanical dilators, balloon dilation) completed by laser therapy or argon plasma coagulation. dilation) completed by laser therapy or argon plasma coagulation.
mechanical ablation of granulation through a rigid bronchscope mechanical ablation of granulation through a rigid bronchscope ( forceps, electroresection)( forceps, electroresection)
endoscopic laser patency restorationendoscopic laser patency restoration (evaporation : CO2 -laser, (evaporation : CO2 -laser, Nd:YAG laser), Nd:YAG laser),
T-tube implantationT-tube implantation, ,
silicone stentssilicone stents
expandable metallic stentsexpandable metallic stents
tracheal resection with end-to-end anastomosis.tracheal resection with end-to-end anastomosis.

Indications for treatment :Indications for treatment :
Endocopic dilation :Endocopic dilation : method of temporary tracheal lumen restorationmethod of temporary tracheal lumen restoration
before final treatment. Used often due to emergency indications. before final treatment. Used often due to emergency indications. Drawbacks : risk of tracheal perforation, hemorrhage, short-term therapeutic
effect.
Laser therapy Laser therapy :: effective ablation of granulation, membranous strictures effective ablation of granulation, membranous strictures
and central stenoses shorter than 4 cm with preserved partial lumen patency. and central stenoses shorter than 4 cm with preserved partial lumen patency.
Enables dilation of the stricture and airway splinting. The method is ineffective Enables dilation of the stricture and airway splinting. The method is ineffective
in a case of complete tracheal obstruction. in a case of complete tracheal obstruction. Drawbacks : risk of tracheal perforation, intensification of stenosis, arrythmia,
air embolism, risk of ignition of a fiberoptic bronchoscope and an intubation tube.

Indications for treatment :Indications for treatment :
Argon plasma coagulation :Argon plasma coagulation : enables relatively safe repeatable enables relatively safe repeatable ablation of granulation during endoscopy (the depth of coagulation is ablation of granulation during endoscopy (the depth of coagulation is 0.5-3 mm) 0.5-3 mm)
In some cases it gives permanent restoration of the tracheal lumen in In some cases it gives permanent restoration of the tracheal lumen in other cases it makes it possible to prepare a patient to a radical other cases it makes it possible to prepare a patient to a radical treatment (resection, stent implantation)treatment (resection, stent implantation)
Drawbacks : method ineffective in complete tracheal obstruction and strictures longer than 1 cm.

Indications for treatment :Indications for treatment :
Stent implantation :Stent implantation : high efficient, simple technique offering instant high efficient, simple technique offering instant improvement of respiratory function. It is usually used in patients in whom improvement of respiratory function. It is usually used in patients in whom surgery is contraindicated or a temporary protection of the tracheal lumen surgery is contraindicated or a temporary protection of the tracheal lumen patency is necessary before surgical treatment. patency is necessary before surgical treatment.
Drawbacks: granulation formation, retention of secretion, hemorrhage, stent migration to the lower part of the trachea, stent rupture, intolerance of stent, stent erosion into adjacent organs.

Tracheal resection
INDICATIONS : INDICATIONS : Tracheal resection is presumed to be the most effective method for the Tracheal resection is presumed to be the most effective method for the treatment of tracheal stenoses as it enables the elimination of the stricture treatment of tracheal stenoses as it enables the elimination of the stricture and restoration of a physiologic airway state. and restoration of a physiologic airway state. The method gives good results in patients with benign isolated tracheal The method gives good results in patients with benign isolated tracheal stenoses not longer than 4 cm- maximally 6 cm and low surgical risk. stenoses not longer than 4 cm- maximally 6 cm and low surgical risk.
CONTRAINDICATIONS :CONTRAINDICATIONS : stenosis > 50% of the tracheal lengthstenosis > 50% of the tracheal length multilevel stenosismultilevel stenosis high stenosis (glottic or subglottic) high stenosis (glottic or subglottic) recurrence of stenosis after tracheal resectionrecurrence of stenosis after tracheal resection bad patient’s general statebad patient’s general state
TRACHEAL RESECTION
Complications :
Early :Early : laryngeal and tracheallaryngeal and tracheal
mmucosa edema ucosa edema pneumothoraxpneumothorax mediastinitismediastinitis disturbances of phonation, disturbances of phonation, dysphagia, dysphagia, hemorrhage,hemorrhage, surgical wound infectionsurgical wound infection
Late :Late : formation of granuloma in formation of granuloma in
the line of anastomosis,the line of anastomosis, recurrence of stenosis, recurrence of stenosis, retension of secretion in retension of secretion in
the bronchial tree, the bronchial tree, tracheoesophageal fistula,tracheoesophageal fistula, tracheoarterial fistula.tracheoarterial fistula.
NEOPLASTIC STENOSES OF THE TRACHEA
Etiology of neoplastic tracheal stenosis : adenomas, adenomas, carcinomas (primary tracheal carcinomas are extremely rarecarcinomas (primary tracheal carcinomas are extremely rare)) papillomas,papillomas, polyps, polyps, lipomas, lipomas, chondromas, chondromas, malignant tumors of adjacent tissues infiltrating the trachea malignant tumors of adjacent tissues infiltrating the trachea
(esophageal tumors, thyroid tumors, mediastinal tumors )
NEOPLASTIC STENOSES OF THE TRACHEA
Symptoms and signs of neoplastic tracheal stenoses are similar tothose observed in postintubation strictures. A basic sign is anincreasing dyspnea. Hemoptysis and retrosternal pains are observed more frequently inneoplastic than in postintubation stenoses.
DIAGNOSIS OF TRACHEAL TUMORS: laryngoscopylaryngoscopy tracheal endoscopy and endoscopic biopsy tracheal endoscopy and endoscopic biopsy x-ray examination x-ray examination computed tomographycomputed tomography magnetic resonance imagingmagnetic resonance imaging

NEOPLASTIC STENOSES OF THE TRACHEA
TREATMENT: endoscopic resection of benign tumors
endoscopic resection of a benign tumor + ablation of residual tumor tissues with argon plasma coagulation
partial tracheal resection for benign and selected malignant tumors (subglottic tumors, tumors invading adjacent tissues and tumors involving more than 4 cm of the tracheal length are unsuitable for resection as oncological margins can’t be achieved)
palliative methods for the restoration of the tracheal lumen in inoperable tumors (laser, argon plasma coagulation, expandable stents, T-tube)
resection of larger than 6 cm of the trachea with the implantation of a prosthesis

RECAPITULATION :
The resection of the cervical part of the trachea for postintubation stenosis is a safe procedure if a patient is qualified properly for this method of treatment. It means that his or her general state, the localization and length of the stenosis meet the conditions for resection.
To perform the procedure successfully, apart from its technical aspects, an experienced anesthesiologist having necessary equipment to provide effective patient ventilation during the operation and good postoperative care is an indispensable condition.