part 5 examination of reflex
TRANSCRIPT


CONTENTS
1. Purpose of examination
2. Upperlimb tendon reflex
3. Lower limb tendon reflex
4. Other reflexes
5. Abnormalities of deep tendon reflex
6. Grading of reflex
7. Superficial reflexes
8. Neonatal Reflexes
9. References

Reflex arc requires a stimulus, a sensory pathway, a link with a motor unit, a motor
neuron and a effector element.
Reflex

PURPOSE OF EXAMINATION:-
o Whether the reflex is present or absent.
o If present whether its normal or showing signs that influences
from higher centres are defective.
o If absent, whether the arc is breached on the motor or sensory
side.
o Whether any abnormalities are unilateral, bilateral, affecting all
reflexes or whether a definite level can be detected in the
nervous system at which abnormalities first appear because
reflex ‘levels’ may be helpful as sensory level.
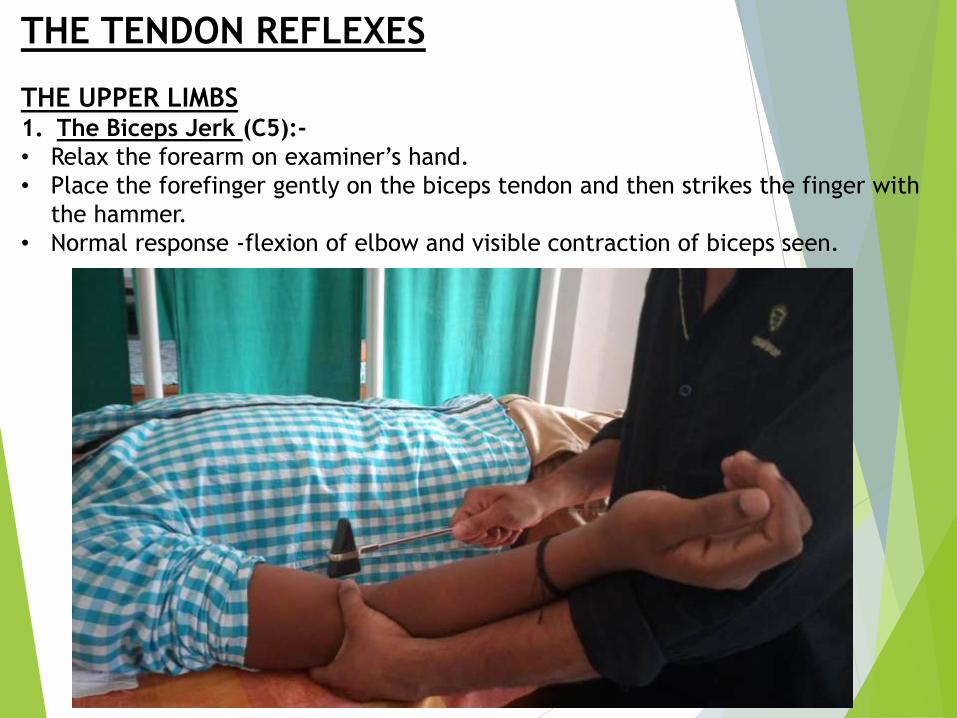
THE TENDON REFLEXES
THE UPPER LIMBS1. The Biceps Jerk (C5):-
• Relax the forearm on examiner’s hand.
• Place the forefinger gently on the biceps tendon and then strikes the finger with
the hammer.
• Normal response -flexion of elbow and visible contraction of biceps seen.
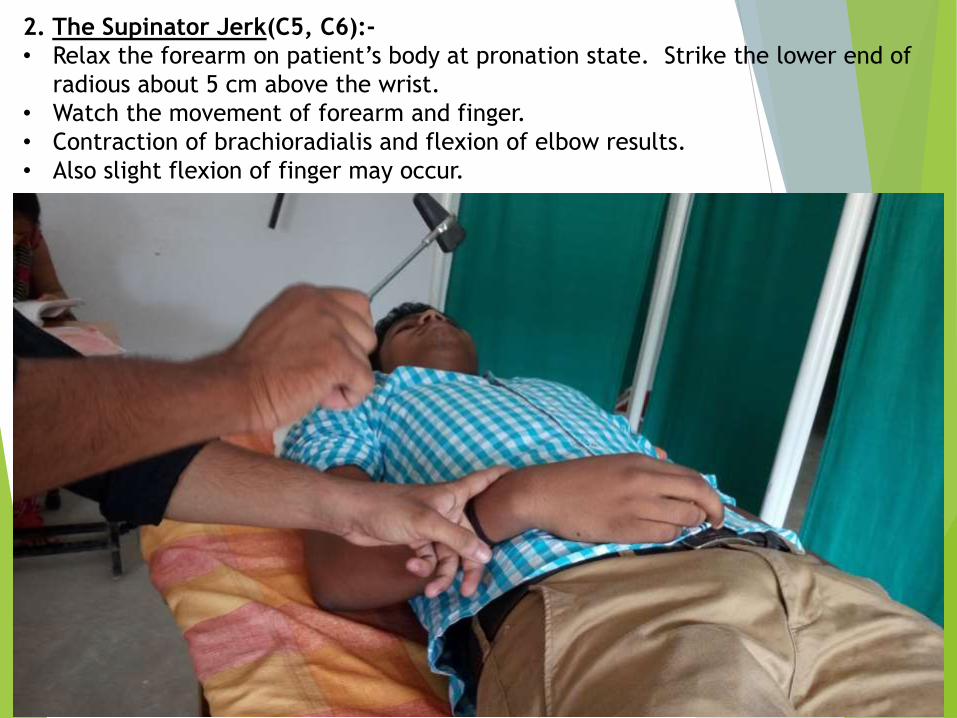
2. The Supinator Jerk(C5, C6):-
• Relax the forearm on patient’s body at pronation state. Strike the lower end of
radious about 5 cm above the wrist.
• Watch the movement of forearm and finger.
• Contraction of brachioradialis and flexion of elbow results.
• Also slight flexion of finger may occur.
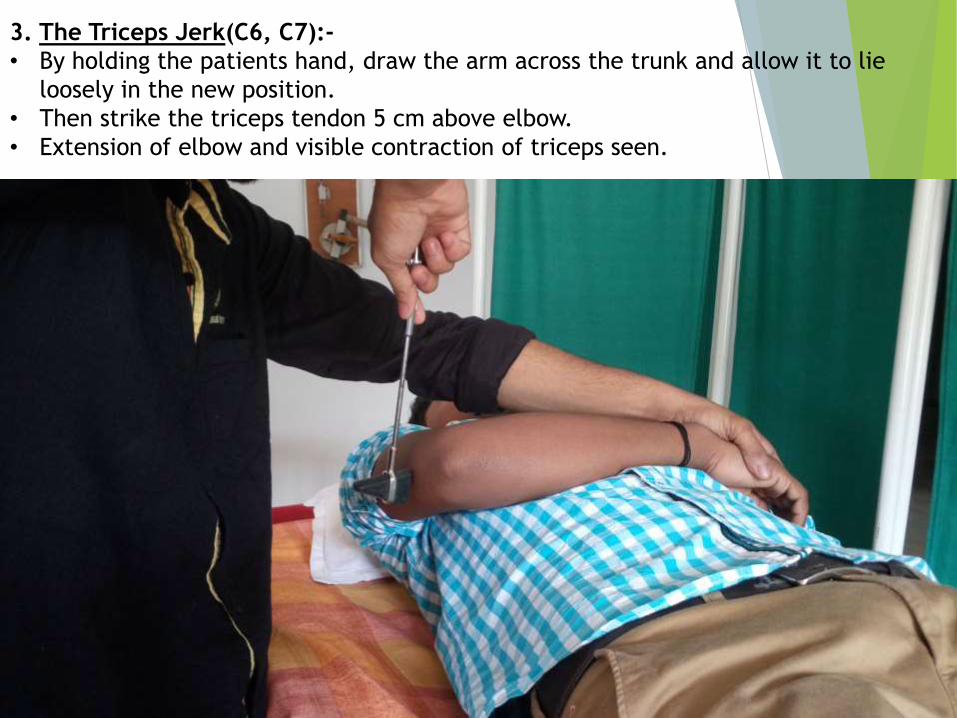
3. The Triceps Jerk(C6, C7):-
• By holding the patients hand, draw the arm across the trunk and allow it to lie
loosely in the new position.
• Then strike the triceps tendon 5 cm above elbow.
• Extension of elbow and visible contraction of triceps seen.

THE LOWER LIMBS1. The Knee Jerk(L3-L4):-
• Patient supine, flex the knee 60ᵒ by placing the forearm under the knee to be
tested.
• Strike the patellar tendon midway between its origin and insertion.
• Extension of knee and visible contraction of quadriceps seen.
• It can also be done with patient in high sitting on bed and leg hanging at edge.


2. The Ankle Jerk(s1):-
• Patient in supine position, hip externally rotated, slightly flex the knee (medial
malleolus facing upward), dorsiflex the ankle by examiner as to stretch the achillis
tendon.
• Strike the tendon on posterior surface.
• The calf contracts and moves ankle.
• The plantarflexion of foot can be felt by the hand of examiner.
• Alternative method:- ask the patient to kneel on the chair so that the ankle are
hanging loose over the edge. Then strikes the achillis tendon.
• Normal response – plantar flexion of the foot and the contraction of gastrocnemius
muscle.

ABNORMALITIES OF DEEP TENDON REFLEX
Pendular movements:-
• Pendular movements are the slow oscillatory movements (instead of
brisk movements) that are developed while eliciting a tendon jerk.
• It occur because of hypotonicity of muscles.
• These are very common while eliciting the knee jerk or patellar
tendon reflex in the patients affected by cerebellar lesion.
• In normal conditions, after the extension, the leg returns back to
resting position immediately.
• In cerebellar lesion, the leg swings forwards and backwards several
times before coming to rest. Normally number of oscillation is 3.
Hung-up reflex-
• The movement is retarded, especially during delayed relaxation, so
that the impression of a slightly sloe motion film is obtained.
• The reflex is appearing to “hang-up” compared with a normal jerk.
• It is mainly seen in hypothyrodism.

Grade Reflexes What it means
0 Absent Lower motor neuron lesion
1+ Present but
depressed
Normal but may indicate
neuropathy
2+ Present/ brisk Normal
3+ Very brisk or
increased
Maybe normal but may indicate
UMN lesion
4+ Clonus UMN lesion
GRADING OF REFLEXES
OTHER REFLEXES-
1. The Hoffman Reflex-• The terminal phalanx of patient middle finger flicked downward
between examiner’s finger and thumb.
• Instead of hyperflexia the tip of other finger flex and the thumb flex
and adduct.
• It is a sign of unilateral pyramidal tract disease.
2. Rossolimo’s reflex –• The patient lies supine with the leg extend and the foot partially
dorsiflex.
• The ball of foot is then struck with the hammer and in hypertonic
state there is a brisk contraction of all toes.
• Normally no response

3. Waternberg SIGN-• The patient supinate his hand slightly flexing the fingers.
• The examiner pronate his hand and links his similarly flexed finger with patient’s.
• Both then flex their finger further against each others resistance.
• Normally the thumb extends, though the terminal phalanx may flex slightly.
• In pyramidal tract lesion, the thumb adduct and flexed strongly.
Normal
Pyramial tract lesion
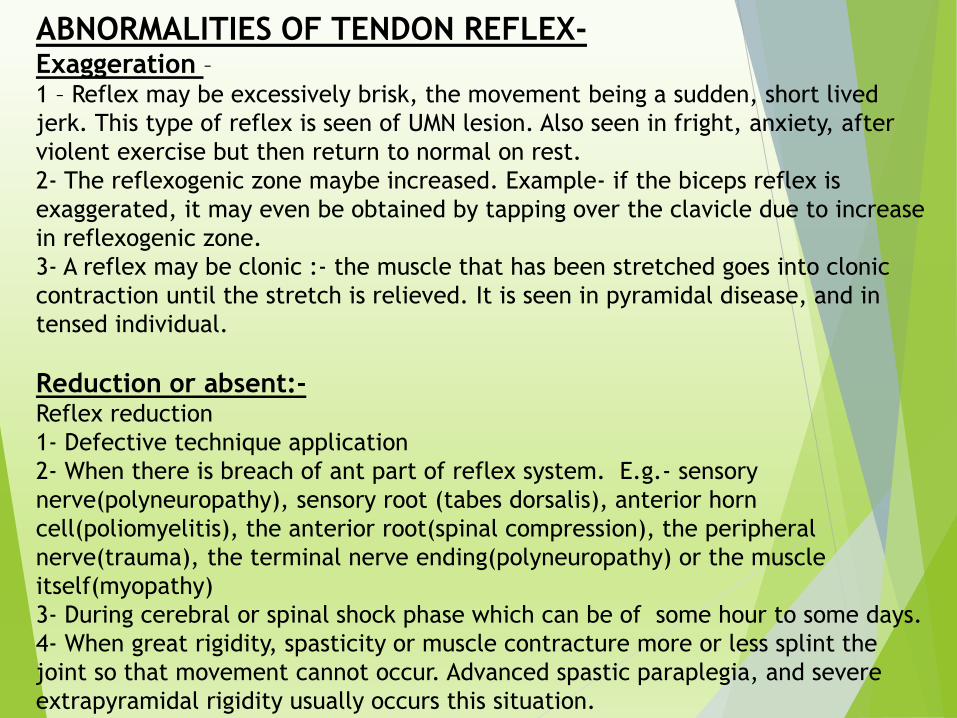
ABNORMALITIES OF TENDON REFLEX-Exaggeration –1 – Reflex may be excessively brisk, the movement being a sudden, short lived
jerk. This type of reflex is seen of UMN lesion. Also seen in fright, anxiety, after
violent exercise but then return to normal on rest.
2- The reflexogenic zone maybe increased. Example- if the biceps reflex is
exaggerated, it may even be obtained by tapping over the clavicle due to increase
in reflexogenic zone.
3- A reflex may be clonic :- the muscle that has been stretched goes into clonic
contraction until the stretch is relieved. It is seen in pyramidal disease, and in
tensed individual.
Reduction or absent:-Reflex reduction
1- Defective technique application
2- When there is breach of ant part of reflex system. E.g.- sensory
nerve(polyneuropathy), sensory root (tabes dorsalis), anterior horn
cell(poliomyelitis), the anterior root(spinal compression), the peripheral
nerve(trauma), the terminal nerve ending(polyneuropathy) or the muscle
itself(myopathy)
3- During cerebral or spinal shock phase which can be of some hour to some days.
4- When great rigidity, spasticity or muscle contracture more or less splint the
joint so that movement cannot occur. Advanced spastic paraplegia, and severe
extrapyramidal rigidity usually occurs this situation.

SUPERFICIAL REFLEXESThe Abdominal Reflexes –• The patient should first lie flat. Palpate gently to asses the degree of relaxation and
the sensitivity of the skin. Explain the patient the procedure.
• Lightly stroke the abdomen with a pencil, key or with the end of the hammer in all
quadrants of abdomen and lower margin of the thoracic case.
• Normal result the muscle contract and umbilicus moves in that direction.
• Segmental innervation- Epigastric-T7-T9, Upper abdominal T9-T11, Lower abdomen
T11-T12
Abnormal response- Exaggerated abdominal reflexes occur in psychoneurosis,
nervousness.
• Absent of reflex- UMN lesion above the level of reflex arc, LMN lesion at
corresponding reflex arc, obesity, rigid abdomen.

The Cremasteric Reflex-• The patient lies supine, with the lower limbs in a slightly abducted
and externally rotated position.
• With the handle of the knee hammer, lightly stroke the upper and
inner aspects of thigh from below upwards.
• The normal response is an immediate contraction of cremaster
muscle that pulls the ipsilateral testis.
The Anal Reflex:-• Lightly scratch the perianal skin which contract the external
sphincter muscle.

The Plantar Reflex• Position the patient so that knee is slightly flexed, and thigh externally rotated.
• The foot is rest on the couch. Ask the patient to let the foot remain closed.
• The outer aspect of sole is then firmly stroked with the blunt point end of knee
hammer.
• Then curve the stimulus towards the middle metatersophalengeal joint.
• Do the stimulation slowly and allow yourself time to see what is happening.
• Normally great toe flex at the metatersophalengeal joint.
• At the same time other toe will flex and close together.
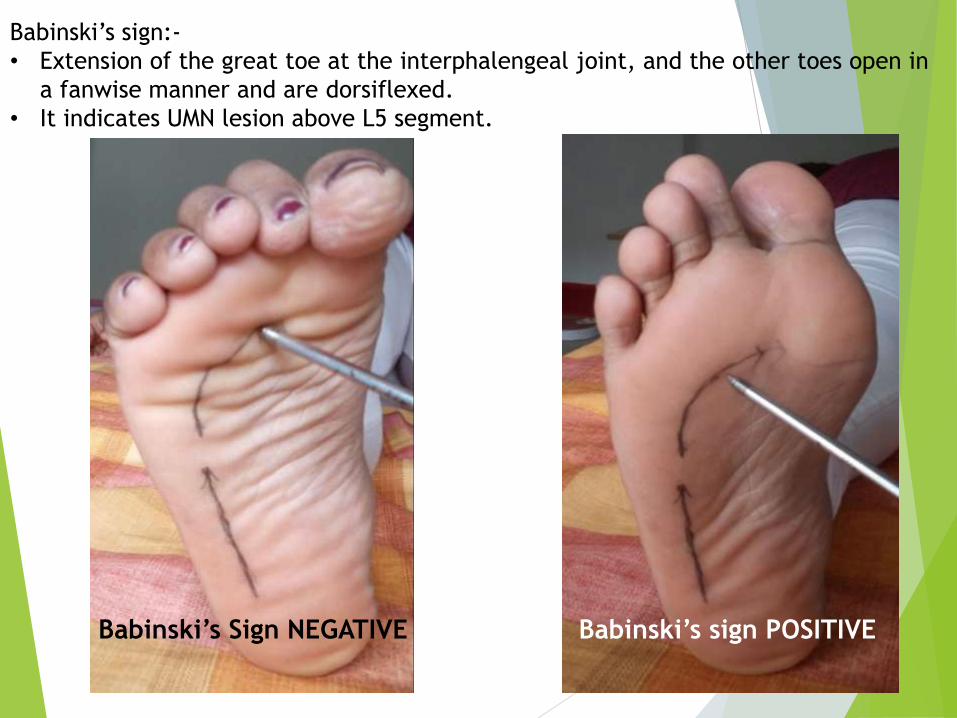
Babinski’s sign:-
• Extension of the great toe at the interphalengeal joint, and the other toes open in
a fanwise manner and are dorsiflexed.
• It indicates UMN lesion above L5 segment.
Babinski’s sign POSITIVEBabinski’s Sign NEGATIVE

Neonatal Reflexes:-
The Grasp Reflex:-• Touch palm with the finger of examiner on the radial border between thumb and
index finger.
• If the grasp reflex is present, the finger will be held tightly by the hand in the first
instance.
• The reflex is normal in babies.
• Also it present in mental deficiency, birth injury, vascular accident in premotor
cortex, lesion in corpus callosum.
• This can occur in normal aging.

Gabellar Tap:-• Tap the gabella (root of nose) repeatedly with one finger brought from
above and behind the patient’s head.
• Normally there is blinking response only to first 2-3 taps. In parkinsonism
the blinking continues as long as the ta given.
The Sucking Reflex:-• Touching the corner of mouth produces a sucking movement of the lips
and deviation of the mouth in the direction of stimulus.
• This is normally present in infants.
• This is also seen in advanced and diffuse cerebral atropic lesion,
traumatic lesion.

References
1. BICKERSTAFF ’s Neurological Examination by KAMESHWAR PRASAD
2. Neurological Assessment by RUBEN D. RESTREPO
3. Neurological Examination by WILLIAM HOWLETT
4. Neurological intervention for Physical Therapy by MARTIN KESSLER
5. A Concise Guide to Neurology by REMA PAI
6. Neurology Illustrated by KENNETH W LINDSAY, IAN BONE

Repetition Of The Same Thought Or Physical Action
Develops Into A Habit,
which Repeated Frequently enough,
Becomes An Automatic Reflex..
THANK YOU !