parkinson’s disease clinical research challenges and best practices 2015
TRANSCRIPT
By:
Ajeigbe Isaac Olaolu, B.Sc., M.B.A.
Parkinson’s Disease Clinical Research Challenges and Best Practices
Humber, Toronto, Canada
2015
Clinical Research Project Supervisor in Specific Diseases
Prof. Peivand Pirouzi



Definition
What is Parkinson’s disease?
What causes PD?
Who gets Parkinson’s disease?
How is Parkinson’s disease diagnosed?
What are the symptoms?
What are treatment options available?
Clinical Trials on Parkinson’s disease
Challenges, Progress and Future approaches
Parkinson’s disease is a chronic, progressive
neurological disease that affects nerve cells
(neurons) in an area of the brain called the
substantia nigra.
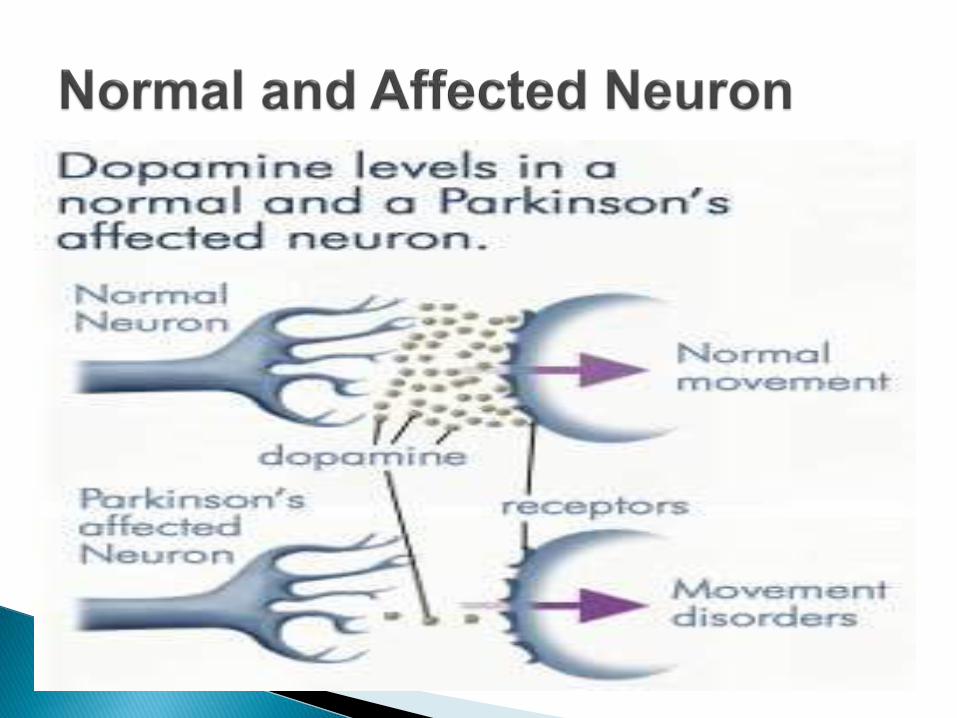
These cells normally produce dopamine, a
chemical (neurotransmitter) that transmits signals
between areas in the brain. These signals, when
working normally, coordinate smooth and
balanced muscle movement.
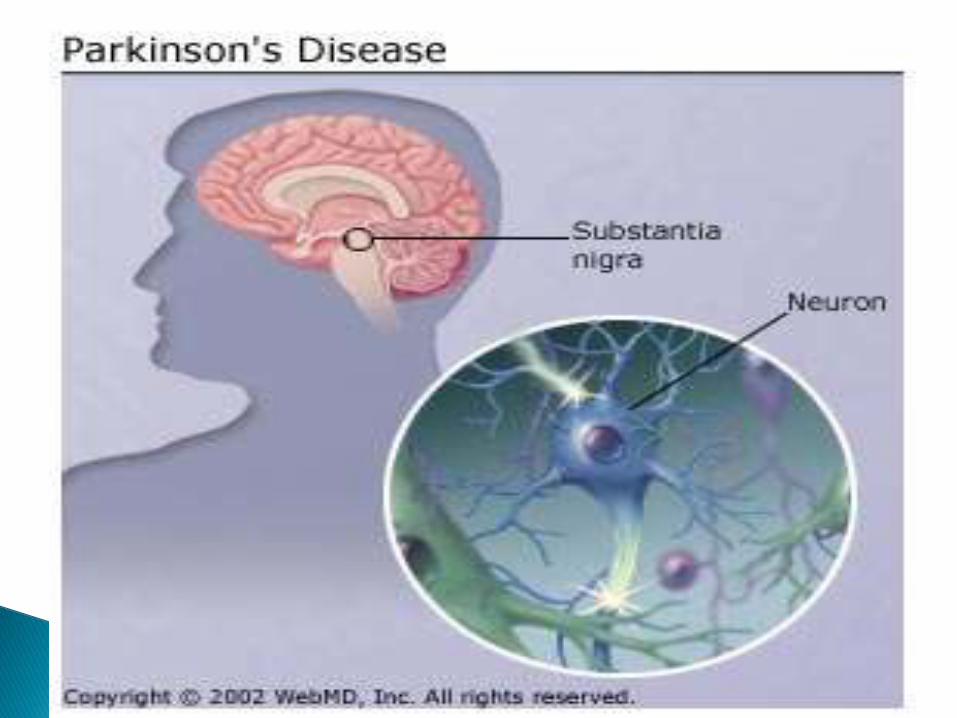

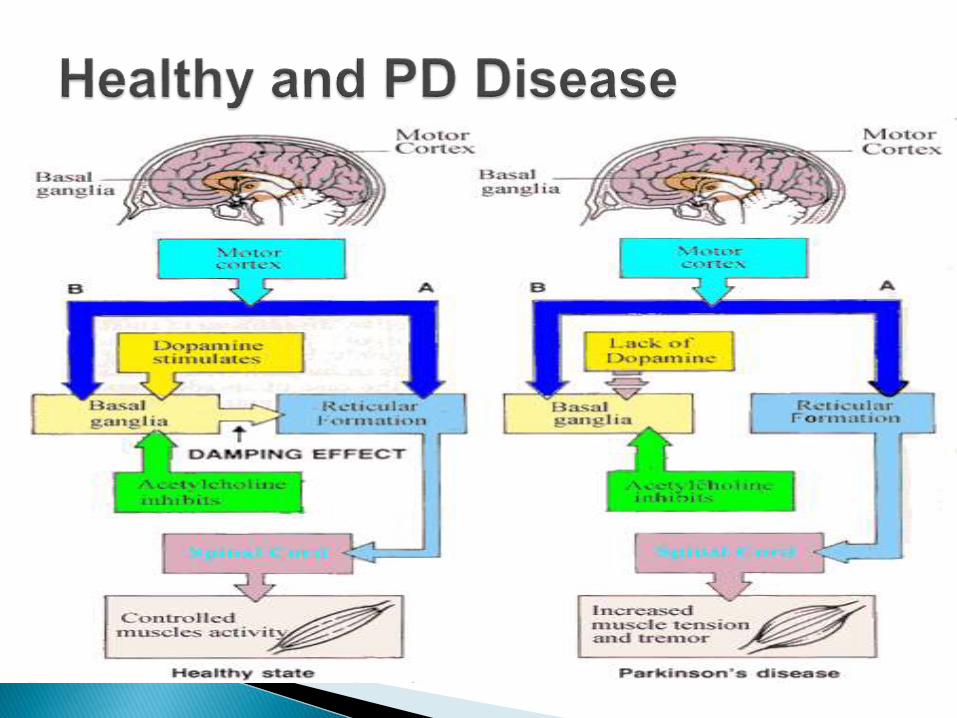
The brain stem called the substantia nigra controls movement.
Parkinson's disease cells in the substantia nigra stop making dopamine
Neurotransmitter helps nerve cells communicate.
As these dopamine-making cells dies due to accumulation of protein alpha-synuclein bound to damaged cell.
The brain does not receive the necessary messages about how and when to move.
The loss of dopamine causes PD symptoms


PD is a progressive disease of the nervous system
marked by tremor, muscular rigidity, and slow, imprecise
movement, chiefly affecting middle-aged and elderly
people.
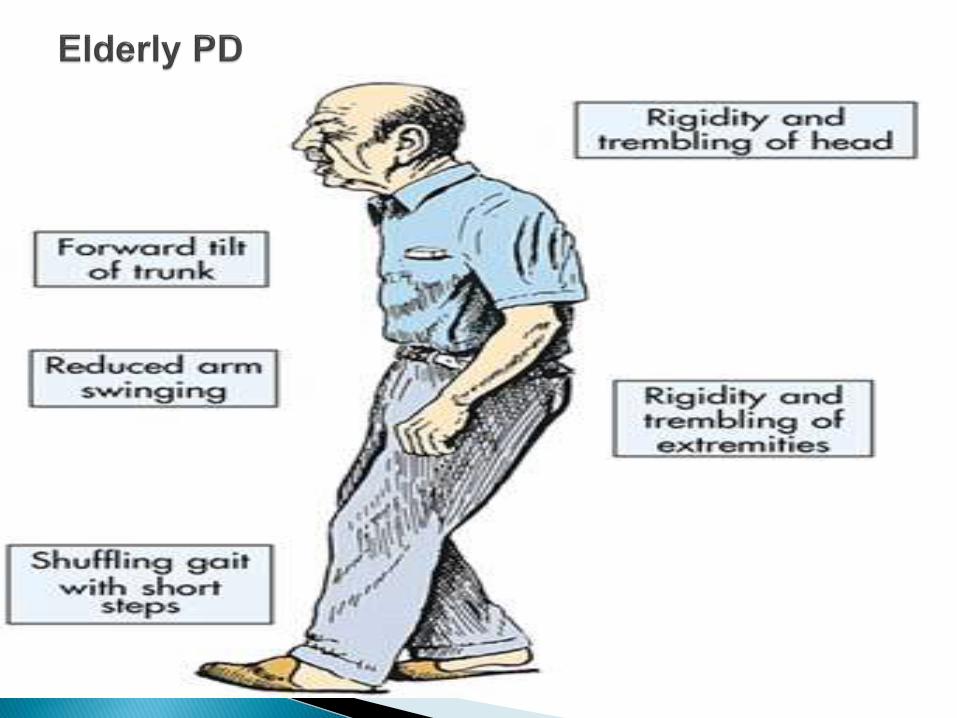
The primary symptoms of PD are tremor, or trembling in
hands, arms, legs, jaw, and face; rigidity, or stiffness of
the limbs and trunk; bradykinesia, or slowness of
movement; and postural instability, or impaired balance
and coordination.

Incidence of PD has reported higher in men than
woman, especially after the age of 60.
The average age at the onset of symptoms is 61.
Reported that about10 percent of patients are
diagnosed before age 40.
PD may be inherited genetically
Environmental factors associated with risk of
having PD
Environmental exposures to toxins contributes to
having PD

Qualified, trained Neurologist diagnoses PD
Currently no sophisticated blood or laboratory tests
available to diagnose the disease.
Some imaging tests, such as CT (computed
tomography) or MRI (magnetic resonance imaging)
scans, may be used to rule out other disorders that
cause similar symptoms.
A detailed medical history needed. This includes
questions about the patient’s symptoms, medications,
and the possible exposure to toxins
Neurological examination
Use of diagnostic criteria especially in the early stages


PD affects movement, producing motor symptoms and non-motor signs.
Common motor symptoms includes tremor (confined to a body part), rigidity of muscles or stiffness of limbs, bradykinesia (slowness of movement) and postural instability.
Less common non-motor symptoms includes neuropsychiatric problems like mood, cognition, behaviour or thought alterations, sensory and sleep difficulties, constipation and skin problems
Others may include speech changes, handwriting changes, pain, apathy, fatigue, impaired color discrimination and restless leg syndrome.
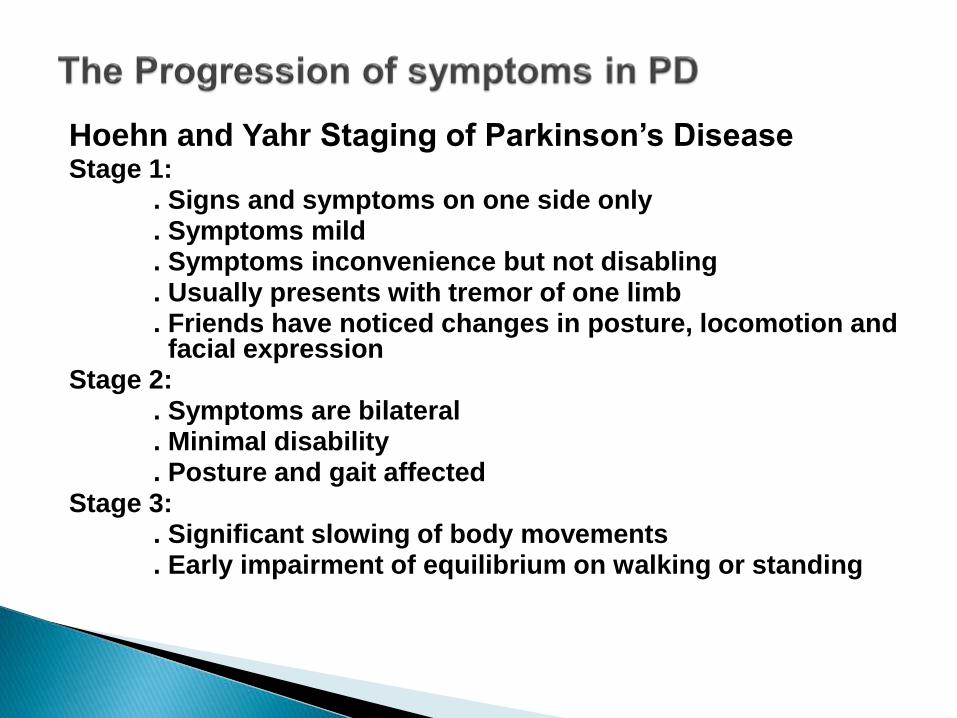
Hoehn and Yahr Staging of Parkinson’s DiseaseStage 1:
. Signs and symptoms on one side only
. Symptoms mild
. Symptoms inconvenience but not disabling
. Usually presents with tremor of one limb
. Friends have noticed changes in posture, locomotion and facial expression
Stage 2:. Symptoms are bilateral. Minimal disability. Posture and gait affected
Stage 3:. Significant slowing of body movements. Early impairment of equilibrium on walking or standing
Stage four:
◦ . Severe symptoms
◦ . Can still work to a limited extent
◦ . Rigidity and bradykinesia
◦ . No longer able to live alone
◦ . Tremor may be less than earlier stages
Stage five:
. Cannot stand or walk
. Invalidism complete
. Cachectic stage
. Requires constant nursing care

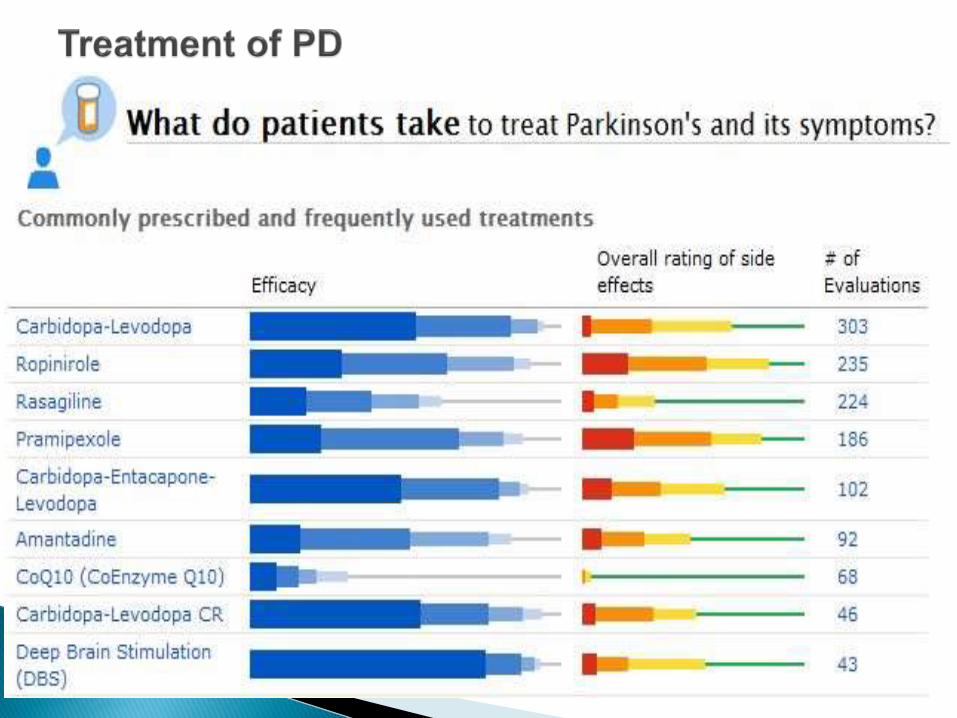
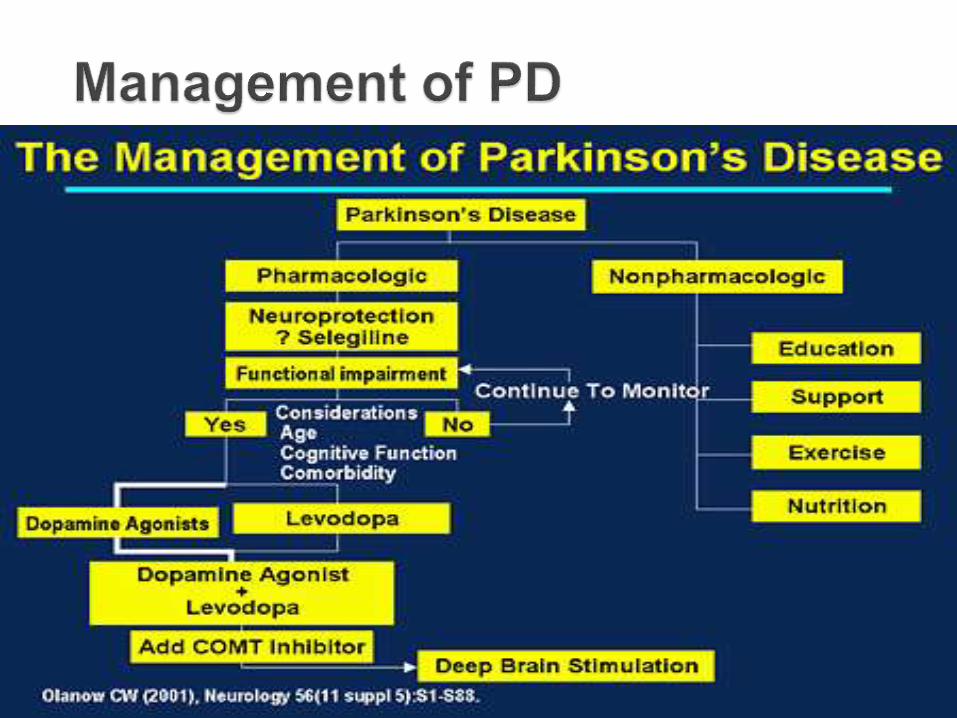
Although there is no cure for PD but medications to relief from symptoms
Two major treatments: Drug treatments and surgery, others are complementary and supportive therapies.
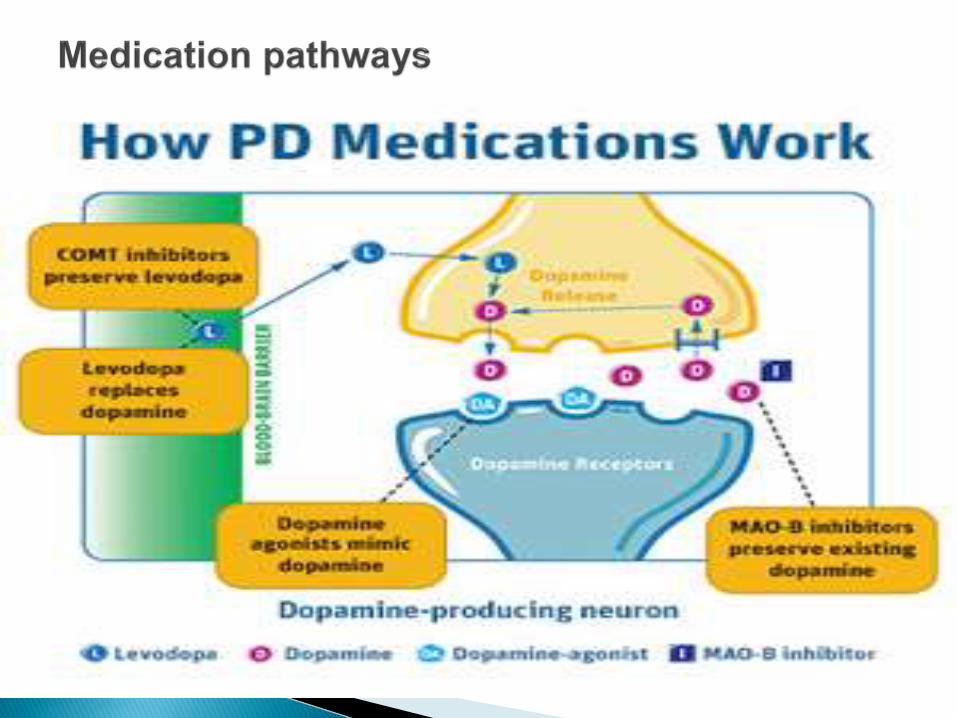
Medication options Levodopa + a dopa decarboxylase inhibitor
(carbidopa) or COMT inhibitor. Dopamine agonist + MAO-B inhibitors (selegiline,
rasagiline) Some COMT inhibitors: tolcapone, entacapone, Some dopamine agonists like ropinirole, pramipexole,
bromocriptine, pergolide, piribedil, cabergoline, apomorphine, lisuride and rotigotine
Others are amantadine and benzotropine


Deep brain stimulation : this involves implantation of medical device called a brain peace maker.
DB Stimulator send electrical impulses to specific part of the brain.
For PD with motor fluctuations and inadequately controlled tremor by medication
Pallidotomy: it involves surgical destruction of the globus pallidus to control dyskinesia
Here lesions are formed to suppress overactivity of specific subcortical areas


. Rehabilitation:
Regular physical exercise help with gait and
voice therapy
. Palliative care:
Specialized medical care for people with
serious illness
. Dietary care:
Balanced diet based on periodic nutritional
assessments
.Caffeine & Nicotine consumption –appears protective

Clinical Trial: NCT00594165
. An Open-Label Extension Trial to Assess the
Safety of Long-Term Treatment of Rotigotine
in Early-Stage Parkinson’s Disease
Clinical Trial: NCT00501969
. An Open-Label Extension Trial to Assess the
Safety of Long-Term Treatment of Rotigotine
in Advanced- Stage Parkinson’s Disease

Purpose:
The objective of this open-label extension is to
assess the safety and tolerability of long-term
treatment of the Rotigotine patch in subjects with
Early Idiopathic Parkinson’s Disease
Study design:
Endpoint classification: Safety/ Efficacy study
Intervention Model: Single group Assignment
Masking: Open Label
Primary purpose: Treatment
Condition: Early-Stage PD

Recruitment Information:
Recruitment status: Completed
Enrollment : 217
Study Start Date : June 2002
Completion Date : November 2008
Eligibility Criteria for Study:
Age Eligible : 31 Years and Above
Gender Eligible : Both
Accept Healthy Volunteers : No
Inclusion Criteria :
Subjects who have completed six months of maintenance treatment in the SP512 double-blind trial
Exclusion Criteria :
Subjects who had an ongoing serious adverse
event from SP512 double-blind trial that was
assessed as related to study medication
Intervention : Drug Rotigotine; Rotigotine trans-
dermal patch 10 cm2 (2 mg/24 hours);
20 cm2 (4 mg/24 hours);
30 cm2 (6 mg/24 hours);
40 cm2 (8 mg/24 hours)
Study Phase : Phase 3

During the first year :
The maximum Rotigotine dose allowed is 6 mg/24
hours.
After the first year : allowed dose increase of
Rotigotine up to a maximum of 16 mg/24 hours.
Primary Outcome Measures :
Number of Subjects With at Least One Adverse
Event During This Open-label Extension Study
[Time Frame: 7 years ]
Secondary Outcome Measures:
Number of Subjects Who Withdrew From the Trial Due to an Adverse Event. [ Time Frame: 7 years ]
Overall Study Results:
Number of Participants analyzed = 216
Number of Subjects with at least one AE =214
Number of subjects who withdrew due to an AE =52
Total Adverse Events in the Study = 206/216 (95.37%)
Total Serious Adverse Events in the study = 102/216 (47.22%)

No cure yet to Parkinson’s disease
Subject withdrawal before the end of trials
Subject unsatisfactory compliance – protocol
violations
Subject enrollment in other trials
Subject moving to other places
Finding the potential cause of PD
Investigating potential new treatments
Finding Global statistical test for diagnosing PD
Environmental factors; Industrialized nations and
exposures to toxins.
Therapeutic Approaches
Drug Therapies
Surgical Therapies
Cell transplants (Stem cells)
Gene therapy
Transcranial Magnetic Stimulation
Deep Brain Stimulation
Genes discoveries
Neuroprotection

Efforts to halting the progression of PD
Restoring lost functions due to PD
Moving towards preventing PD
Improving Rehabilitation and Assertiveness of Technology for PD
Assessing Quality of life of PD patients
On-going studies includes: Studies of Structures and functions of proteins involved in PD;
Studies PD risk factors in people of different gender and ethnicity and Anatomical studies of structures and brain channels involved in PD
https://www.youtube.com/watch?v=aYRCexa5FCk

