parents' food choices: obesity among minority parents and children
TRANSCRIPT
This article was downloaded by: [Eindhoven Technical University]On: 21 November 2014, At: 15:40Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Community Health NursingPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/hchn20
Parents' Food Choices: Obesity AmongMinority Parents and ChildrenYvette M. Sealy Ph.D. and MPH aa Graduate School of Social Service , Fordham University , New York,New YorkPublished online: 01 Feb 2010.
To cite this article: Yvette M. Sealy Ph.D. and MPH (2010) Parents' Food Choices: ObesityAmong Minority Parents and Children, Journal of Community Health Nursing, 27:1, 1-11, DOI:10.1080/07370010903466072
To link to this article: http://dx.doi.org/10.1080/07370010903466072
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Parents’ Food Choices: Obesity AmongMinority Parents and Children
Yvette M. SealyGraduate School of Social Service, Fordham University, New York, New York
This article examines obesity among minority parents and children in the context of culture, socioeco-nomic status, and the parent–child dyad. Knowing parental attitudes about eating habits, food prepara-tion, and dietary guidelines is crucial to addressing childhood obesity. Parents of African American,Caribbean, and Hispanic descent participated in focus groups to explore their attitudes and practicesregarding the food choices they make for themselves and their 6- to 12-year-old children. Culturalidentification and time constraints were identified as key themes that influence food choice decisions.Several recommendations are made for health care practitioners working with families to reduce theincidence of obesity.
Childhood obesity is taking a considerable physical, psychological, and social toll on minority chil-dren in communities across the United States. Childhood obesity has doubled over the past three de-cades, with the highest prevalence among African American, Hispanic, and Native American chil-dren (Ogden, Carroll, & Flegal, 2008). The increased weight places children at risk for chronicdisease, diminished quality of life, and poor health outcomes. As such, obesity poses a considerablefinancial cost to society. The multiple health problems of obese individuals often lead to physicaldisabilities and an inability to actively participate in academic endeavors and the workforce. Obe-sity-attributablemedicalexpenses in theUnitedStates reached$75billion in2003,withhalfof thesecosts financed by the taxpayer-funded programs Medicaid and Medicare (Finkelstein, Fiebelkorn,& Wang, 2004). The literature on childhood obesity readily documents that prevalence is increasingat faster rates for African American and Hispanic youth than for White children (Kumanyika, 2008;West, Prewitt, Bursac, & Felix, 2008). This study examines the perceptions, attitudes, food choices,and eating habits of African American, Caribbean, and Hispanic parents, and explores the practicesthat influence what they provide for their children to eat.
LITERATURE REVIEW
Childhood Obesity Prevalence and Associated Health Risks
National Health and Nutrition Examination Survey (NHANES) data for the period 2003–2006found that obesity prevalence was 12.4% for children ages 2–5 years, 17.0% for 6- to
Journal of Community Health Nursing, 27:1–11, 2010Copyright © Taylor & Francis Group, LLCISSN: 0737-0016 print/1532-7655 onlineDOI: 10.1080/07370010903466072
Address correspondence to Yvette M. Sealy, Ph.D., MPH, Assistant Professor, Fordham University, Graduate Schoolof Social Service, 113 West 60th St., Rm. 903 B, New York, NY 10023. E-mail: [email protected]
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14
11-year-olds, and 17.6% for adolescents 12–19 years old (Centers for Disease Control and Pre-vention [CDC], 2009a). These rates increased from 5.0%, 6.5%, and 5.0% during 1976–1980 forthe respective age groups.
Childhood obesity among African American adolescent boys increased from 10.7% to 22.9%across the NHANES survey periods 1988–1994 and 2003–2006. This reflects a 12.2% increasefor African American teens. Likewise, data for Hispanic adolescent males showed a 7% increase(from 14.1% to 21.1%) for the same period. A smaller increase (4.4%) was observed for White ad-olescent boys, with prevalence increasing from 11.6% to 16.0%. Results were similar for adoles-cent girls, with African American girls having the highest prevalence of obesity at 27.7%, fol-lowed by Hispanic-Americans at 19.9%, and White Americans at 14.5%. The percentage increaseamong White, Hispanic, and African American girls was 7.1%, 10.7%, and 14.5% respectively.Little is known about the prevalence of obesity among Caribbean or Caribbean American youthbecause the CDC reports statistics in aggregate form and people with Caribbean ancestry are in-cluded with African Americans.
A recent report evaluating the impact of obesity-policy legislation indicated that two-thirds ofAmerican adults are either overweight or obese (Robert Wood Johnson Foundation [RWJF], 2009).The report further revealed that adult obesity rates increased in 23 states, with no decreases in anystate in the country. Meanwhile, the percentage of obese or overweight children is at or above 30% in30 states in the United States (RWJF, 2009). The continued failure to reduce obesity prevalence be-comes apparent with the growing number of children experiencing chronic diseases due to over-weight and obesity. Obese children are more likely to experience physical conditions such as hyper-tension, hyperlipidemia, type-2 diabetes, asthma, sleep apnea, joint pain, and other orthopedicproblems than children with a normal weight (Cali & Caprio, 2008; CDC, 2009b). Diabetes, highblood pressure, and high cholesterol during childhood each place children at greater risk for athero-sclerosis, heart attacks, and strokes during adulthood (Baker, Olsen, & Sorensen, 2007; Blacksher,2008; Freedman, Dietz, Srinivasan, & Berenson, 2009). These conditions are even more severe inadulthood if they first appear in childhood. Prolonged exposure to a compromised health status islikely to impose limitations on obese adults’ ability to sustain employment or participate in recre-ational or social activities, and places adults at greater risk for premature death (Haas et al., 2003;Must et al., 1999). Low self-esteem, depression, anxiety, and decreased educational attainment areother critical consequences of childhood obesity (CDC, 2009b; Karnehed, Rasmussen,Hemmingsson, & Tynelius, 2006; Zametkin, Zoon, Klein, & Munson, 2004).
Convergence of Culture, Socioeconomic Status, and Childhood Obesity
Today, the meal experience, and food itself, has become more than a coming together of family andcommunity (Airhihenbuwa et al., 1996); it has become a form of recreation, and a tool to alleviateboredom, stress, and fatigue. In addition, the predominant approach to food preparation amongmany African Americans and Hispanics often involves cooking with large quantities of sodium,sugar, fats, andfrying inoils insteadofhealthiermethods (e.g.,baking,boiling,orbroiling), thus fur-ther promoting obesity and other adverse health consequences (Hudson, 2008; Walker-Sterling,2005). For many, the combination of food choice and method of preparation is in direct opposition tothe dietary guidelines recommended by the US Department of Agriculture and the Department ofHealth and Human Services (2005). The difficulty lies in attempting to change eating habits that areingrained and inherently woven into the tradition and fabric of the individual’s culture(Airhihenbuwa et al., 1996; Singh, Kogan, Van Dyck, & Siahpush, 2008; West et al., 2008).
2 SEALY
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

An inverse socioeconomic gradient for childhood obesity, health, and overall well-being alsoexists (Ard et al., 2008; Blacksher, 2008; Goodman, Slap, & Huang, 2003; Singh et al., 2008).Poor physical health during childhood sets children on a downward trajectory and leads to chronicdisease and degenerative conditions during adulthood. Low- and middle-income parents mustmanage modest household budgets that may not consistently allow for essential resources letalone seemingly expendable items like fruits and vegetables. During the current economic crisis,parents are concerned about their employment status, losing health care benefits, and are workinglonger hours to earn moderate wages. The national unemployment rate increased from 4.9% inJanuary 2008 to 10% in November 2009 and is higher among minority groups (US Bureau of La-bor Statistics, 2009). In addition, the cost of food has sharply increased thus making it harder forparents to afford quality foods (RWJF, 2009; US Department of Agriculture, 2009).
Fewer studies are conducted with obese minority populations to explore contributing factorsand the uniqueness of their experiences. As a result, it is essential to know what the influences arebefore interventions can be designed to meet the different experiences people have in the variousenvironments in which they live.
METHODS
Design
The study used focus groups to determine what factors influenced the eating habits, food choices,and food preparation practices of African American, Caribbean, and Hispanic parents. Five ques-tions guided the focus groups: (a) When you were growing up what were your favorite foods?, (b)Was there anything special that your mother or family cooked?, (c) In your opinion, what types offoods are children today eating?, (d) How many meals a week do you prepare at home or orderfrom take-out?, and (e) How do you decide to cook at home or get take-out?
Sample
Three focus groups were conducted at a large, not-for-profit organization in New York City pro-viding primarily African American and Hispanic youth between the ages of 6–18 years with recre-ation, education enhancement, guidance, and leadership development services. Parents had tospeak English and have at least one 6- to 12-year-old child enrolled in the program to be includedin the study. Weight status was not measured thus it was not a criteria for inclusion in the study.Parents (n = 34) within each of the focus groups were similar with respect to marital and employ-ment status, and higher education but differed in ethnicity and income (Table 1). The demographiccharacteristics of parents in the study were representative of their neighborhoods and the popula-tions at large within the areas studied (US Census Bureau, 2008).
Setting
The convenience sample of parents was recruited from three different agency sites including theMorrisania section of the Bronx, the Fort Greene section of Brooklyn, and the Flatbush section ofBrooklyn. Flyers were posted at the sites inviting parents to speak with the program director ifthey were interested in participating in a focus group on health and nutrition. Directors at each site
PARENTS’ FOOD CHOICES 3
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14
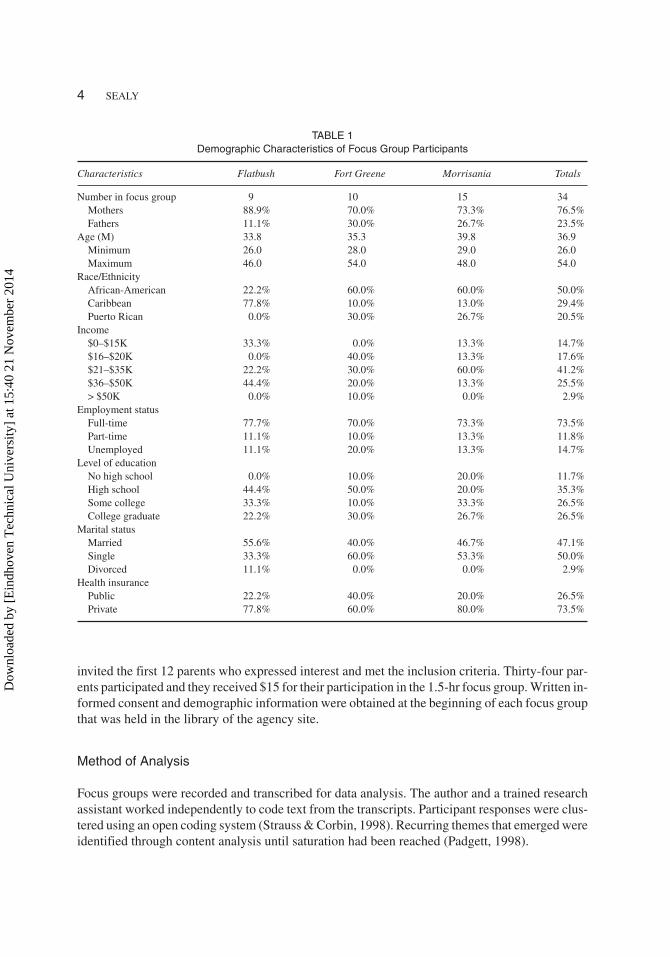
invited the first 12 parents who expressed interest and met the inclusion criteria. Thirty-four par-ents participated and they received $15 for their participation in the 1.5-hr focus group. Written in-formed consent and demographic information were obtained at the beginning of each focus groupthat was held in the library of the agency site.
Method of Analysis
Focus groups were recorded and transcribed for data analysis. The author and a trained researchassistant worked independently to code text from the transcripts. Participant responses were clus-tered using an open coding system (Strauss & Corbin, 1998). Recurring themes that emerged wereidentified through content analysis until saturation had been reached (Padgett, 1998).
4 SEALY
TABLE 1Demographic Characteristics of Focus Group Participants
Characteristics Flatbush Fort Greene Morrisania Totals
Number in focus group 9 10 15 34Mothers 88.9% 70.0% 73.3% 76.5%Fathers 11.1% 30.0% 26.7% 23.5%
Age (M) 33.8 35.3 39.8 36.9Minimum 26.0 28.0 29.0 26.0Maximum 46.0 54.0 48.0 54.0
Race/EthnicityAfrican-American 22.2% 60.0% 60.0% 50.0%Caribbean 77.8% 10.0% 13.0% 29.4%Puerto Rican 0.0% 30.0% 26.7% 20.5%
Income$0–$15K 33.3% 0.0% 13.3% 14.7%$16–$20K 0.0% 40.0% 13.3% 17.6%$21–$35K 22.2% 30.0% 60.0% 41.2%$36–$50K 44.4% 20.0% 13.3% 25.5%> $50K 0.0% 10.0% 0.0% 2.9%
Employment statusFull-time 77.7% 70.0% 73.3% 73.5%Part-time 11.1% 10.0% 13.3% 11.8%Unemployed 11.1% 20.0% 13.3% 14.7%
Level of educationNo high school 0.0% 10.0% 20.0% 11.7%High school 44.4% 50.0% 20.0% 35.3%Some college 33.3% 10.0% 33.3% 26.5%College graduate 22.2% 30.0% 26.7% 26.5%
Marital statusMarried 55.6% 40.0% 46.7% 47.1%Single 33.3% 60.0% 53.3% 50.0%Divorced 11.1% 0.0% 0.0% 2.9%
Health insurancePublic 22.2% 40.0% 20.0% 26.5%Private 77.8% 60.0% 80.0% 73.5%
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

RESULTS
Parents spoke about the challenges they faced in planning meals for their families. Across thegroups, the parents shared accounts of their successes and challenges in trying to meet recom-mended dietary guidelines versus maintaining traditional and culturally based meals. In addition,parents discussed their decision-making process for determining what foods to provide for theirchildren. Two recurring themes emerged from the content analysis: ethnicity and culture and timeconstraints. Parents’ perceptions and practices are presented using their own words to illustratethese themes.
Ethnicity and Culture
The findings show that the parents’ ethnicity and culture have a strong influence on the foods theyselect. Parents uniformly reported that their childhood eating habits were very much associatedwith their ethnic and cultural identity. Many of the African American parents referred to their fa-milial roots in the southern United States; Puerto Rican parents reported the influence of the cul-ture in Puerto Rico; and Caribbean parents either grew up in or had parents from countries includ-ing Barbados, Haiti, Jamaica, and Trinidad.
The parents unanimously agreed there were distinct differences between what they ate as chil-dren and the eating patterns they and their children have today. African American parents reared inthe South spoke of routinely eating an assortment of fresh vegetables grown on land owned byfamily or friends when they were children. If their parents, alone, were raised in the South, thenthe practice of eating vegetables was passed down to them. This practice was maintained, withoutchange, in some cases and revised in others. The following excerpts from the focus group partici-pants reflect how ethnic or cultural practices and associated patterns of behavior have added totheir decision-making regarding food choices.
A mother in the Flatbush group compared the naturalness of foods when she was child with thecontemporary American food environment. She said,
I’m from Jamaica, so all these things they have up here, we don’t have it down there. I see McDon-ald’s, and we didn’t have those things, nothing about that fast food. We have to cook every day. Every-thing is there for you to cook.
Another mother in the Flatbush group, who was born in the United States but whose familycame from Antigua, commented on what’s missing from her child’s diet.
I think that it’s [vegetables] missing in my son’s diet. To be honest, I don’t like vegetables; that’s justmy preference. He usually gets vegetables at school or at my mother’s house. [laughter] You know, I’llhave broccoli, but it has to be from the Chinese restaurant.
An African American mother in the Morrisania group commented on her childhood foodchoices and how they changed when she grew up. First, she said, reflecting on her early childhood,“My mother had me at 40; she didn’t have canned food then. Everything was fresh or frozen …and apple juice and orange juice too.” Then, she compared that to her teenage years:
But by the time I grew up and went to the store, that’s when I realized they had vegetables in a can orfruit in a can. You really didn’t know that vegetable was in the can. To this day my mother still cooks
PARENTS’ FOOD CHOICES 5
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

fresh vegetables. Fridays was like a treat. We would go to a restaurant. You know, McDonald’s was atreat.
Another mother continued to speak, echoing the sentiments of several respondents. “Well, I’mused to the South,” she said.
“I’m used to Southern cooking, I like the baked macaroni and cheese the homemade way, not the box;and I take those recipes from what my mother used like the butter, bread crumbs, egg mixture and allthat. That’s the best way.”
An African American father from Morrisania said, referring to his childhood food choices,
I’m from the South—Florida. Back then parents were different than parents they got today. You usu-ally went straight home and you fixed you a frank and got a glass of milk, and you watched Lost inSpace [laughter]. You did your homework. And if there’s someone to cook rice and neck bones, youhad leftovers for the next day. [laughter in agreement]
Speaking about children today and comparing them to his youth, he added:
So your kids now, when they get out of school, they tell you they want a hero. We didn’t get no heroback then [laughter]. Wasn’t no McDonald’s. You went and got those franks and got that big Carnationmilk [condensed milk, high in fat]�one can would last you a whole month if you add water. Mymother had no problems with us kids.
The main difference among parents in the three groups was the manner in which they preparedfood. African American and Hispanic parents tended to add large quantities of sodium, sugar, andfat-based products to foods during preparation. They were also more likely to fry foods in satu-rated fat. Caribbean parents, in contrast, typically utilized healthier means of food preparation thatincluded herbs, spices, grilling, and baking. Caribbean parents also spoke of eating more fresh fishthan the African American or Puerto Rican parents, whose diets contained more red meat andpork.
A majority of Puerto Rican parents in the focus groups said they did not regularly consumevegetables during childhood, and they still struggle to incorporate vegetables into their family’sdiet. A Puerto Rican mother from Fort Greene, with a reportedly overweight 6-year-old son, put itthis way:
We’re Hispanic and we were raised in a Hispanic home. I envy the people that were born down South,because they had vegetables, like they grew. My mother raised me here and I didn’t realize that beanswere not a vegetable. You know, we always had rice and beans and this, and rice and beans and that.Two starches and no vegetable, you know; so my kids … I had to introduce them to vegetables becauseI was not introduced to vegetables. And it wasn’t that my mother didn’t love me; my mother didn’tknow.
A Puerto Rican mother from the Morrisania group said,
I mean, I learned how to eat collard greens and all these other vegetables when I moved here. ‘Cause ofmy [African-American] neighbors, you know, and trust me, I love it. My people didn’t know how tocook anything else besides rice and beans. You know, that’s how we grew up, and that’s what I’mteaching my kids now, because that’s what I do. Even though I cook rice some days, and beans, I gottaget off of that, you know. I try to do little, different things. So they got different types of food, but it’shard.
6 SEALY
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14
Another Puerto Rican mother, from the Fort Greene group, said,
But let me also ask something else. It’s very hard, also, but I notice that my son, he eats vegetables, car-rots, I mean things that is coming from the school. And he loves it, and he says, “Mom, why do you al-ways cook Spanish food? [laughter]. Don’t you know how to cook something else?” And I say, “Thisis how I was raised, basically. I don’t eat other stuff. I guess it’s just me.” But I’m proud to see thatother kids eats that, you know, especially my son. He’s Hispanic. As a parent, the only thing I cook is… well I do cook Italian. He likes that, but my basic meal is Spanish food, and that’s the only thing Icould cook.
Time Constraints
The second theme to emerge from the discussion on food choices was the impact time constraintshave on what parents and their children consume for meals. The problem of limited time to shopand prepare meals at home over getting take-out is a big issue for families.
One mother in the Fort Greene group said,
I’m so tired, I don’t feel like cooking; and I feel bad, because when I was growing up I had good mealsand I should do that for my daughter. Instead, I go to McDonald’s, I go to Burger King, not every day,but I’m being honest. You know, I do give a damn. I know it’s not right.
A father from Morrisania said of his childhood,
I never went to a fast-food place when I was young. I think the reason why, back then, we were able toeat hot, cooked meals was because my father was the one that worked and my mother stood home.
A mother from Morrisania said,
Today there are a lot of parents, especially mothers, women that are working. Back then they did notwork. They used to stay home and they had the time to cook. Look at me now. I’m here [at the focusgroup, 7:30 p.m.], what’s my kid gonna eat for dinner? I’m gonna put popcorn chicken, the frozenkind, in the microwave. I don’t have time right now to start making a meal.
A mother from the Flatbush group, said,
Sunday I make sure I make a big dinner to last 2 or 3 days. Or during the week, when I come out [fromwork] early, ‘cause you know, I work every day. If I come out early, then I’ll go and I’ll cook a dinner,but on my later days, I can’t. And it’s sad but it’s true, I can’t.
A father from the Fort Greene group said,
Well, me and my sons, we eat out. Like once the food in the house gets low, and I don’t feel like goingshopping yet, we just go outside and we eat out when food is low in the house.
His sentiment was echoed and elaborated on by a mother in the Fort Greene group who said,
You have to make sure the kids have their homework done or go to bed at a certain time, so all that stuffis factored into making a meal. I know for me it’s all factored in. Sometimes I get lackadaisical, and soI may not make the healthiest plates because of the time. I mean, the way things are today, everythingneeds to be fast.
PARENTS’ FOOD CHOICES 7
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

“I feel bad for my kids, you know, like by the time we get home, I pick them up [from the program] at7, then you go home it’s 8, and we go over homework while I’m trying to cook … it’s late, said onemother.
A mother in the Morrisania group said,
You pick that one spot after you pick them up [from the program] to go get something, or go some-where at 8, 9 o’clock, when you get home. When I was younger, I felt like I had all day after I got homefrom school … ran outside and played, did the homework. Still had TV time and time to go tosleep�but not today.
Another mother stated,
I try to do those 30-minute meals. And when I go food shopping, I usually buy all my meat, ‘causethat’s the way my mother taught me. Season everything … you put it in zip-lock bags, put the little tagson them, take them out the freezer the night before. Then when you come home, everything is readyand you’re done.
DISCUSSION
The findings elucidate how food choices for parents and children are closely connected with (a)culturally determined eating habits, (b) foods that can be easily accessed, and (c) foods that re-quire minimal time for preparation. The influence of ethnic and cultural identity and tradition wasclearly present when parents discussed their food choices. This was evident as ethnicity and cul-ture appeared to be the template through which food choices are made (e.g., “I’m from the WestIndies and we …,” “In Puerto Rico we …,” and “Down South …”). It also demonstrates how per-ceptions of a healthy diet, eating habits, and food preparation differ among minority subgroupsand across generations. There was a clear difference between what parents felt they ate as childrencompared with their current food choices for themselves and their children. In particular, the studyshows how Caribbean participants differ from both African American and Puerto Rican partici-pants in their attitudes and practices regarding food. In general, African American parents—par-ticularly from the South—and Caribbean parents reported having more of a reliance on fresh andfrozen food during their youth. Although Caribbean parents reported maintaining that practice,more African Americans and Hispanics incorporated processed foods and canned goods into theirdiet during adulthood.
With either an affinity for Southern-style cooking (high in fat), or the staple of rice and beans(high starch), African American and Hispanic parents reported being big consumers of beef andpork, but Caribbean parents incorporated more fish into their diets. In addition, some children’sdiets were influenced by the fact that their parents disliked a particular food group, and thus chosenot to prepare that food (i.e., vegetables) for meals. Parents relied on school meal programs to pro-vide the food groups missing from the at-home diet. Parents also reported that they ate less fastfood as children than their children currently consume. Occasions when they ate fast food duringchildhood were described as a treat for good behavior, or a reward for an achievement. Today, con-suming fast food has become an expected and normalized component of the weekly diet. More Af-rican American and Hispanic parents spoke of being aware of the need for improving their fami-lies’ diet even though they felt ill-equipped to make such changes.
8 SEALY
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

Time constraints presented another considerable challenge for parents. In each group, par-ents compared themselves to their stay-at-home mothers or grandmothers, whose primary taskwas caring for the family. With parents working long hours at one or more jobs, having multiplechild-care responsibilities (e.g., homework help, recreation, doctor visits, supervision), manag-ing a household, caring for aging parents, and trying to meet their own personal needs, parentsreport being stressed and feeling overwhelmed at times. These and other related strains haverendered parents’ food choices subject to not only ethnic and cultural familiarity, availability,and affordability, but also to timing required to prepare meals. The strain of multiple roles in-cited feelings of dread for parents when needing to prepare meals and appears to have parentsunwittingly relying more on energy-dense foods with lower nutritional values. The sociodemo-graphic characteristics of study participants—such as low income and level of education—arealso reflective of the strains found to be correlated with obesity (Haas et al., 2003; Kumanyika& Grier, 2006).
Several practice implications can be made to address the consumption of unhealthy cultur-ally-bound foods and the inevitable time constraints experienced by parents. Although ethnicityand culture were guides for food choices, parents were moderately cognizant of when the food tra-ditions of their culture posed a threat to their health. Parents and children can be assisted by healthcare practitioners in a variety of settings to make small and practical health improving changesthereby reducing their risk for obesity. Practitioners should readily interview parents and childrenabout their eating habits and provide information on the close relationship between diet and dis-ease. This can be done while educating them about the influence of dietary intake (food choicesand portion sizes) on the incidence of obesity related health conditions. The goal should be to ac-knowledge the ethnic and cultural connections to particular food groups while working with par-ents to introduce sustainable healthy substitutions into the family’s diet. Annual physical exami-nations are also insufficient when parents or children have been identified as overweight or obese.The obesity prevention plan for the family system must include regular visits with a health careteam for ongoing monitoring and support. Culturally relevant health communication tools likecooking videos and interactive nutritionally focused computer software designed specifically forparents and children can be disseminated to further encourage families to improve their eatinghabits.
The environmental context in which many low-income families live must be restructured tosupport the culturally determined attitudinal and behavioral changes necessary for maintainingoptimal weight and overall good health. Obesity-policy legislation (e.g., ban on the use oftrans-fats by restaurants, and large fast-food chains being required to post calorie-count informa-tion directly on menus) notwithstanding, families are in need of more immediate guidance aboutfood choice. Practitioners need to ensure that parents and children have an opportunity to practiceand reinforce new behavior patterns. Enrollment in youth service programs—such as the onewhere this study was conducted—provide social support in the fight against childhood obesity, yetsuch programs do not exist in all communities. Places of worship, community centers, publichousing developments, and other sites where families from similar cultural backgrounds gatherare prime networks for lectures, shopping, and cooking demonstrations on nutrition and diet.Once such changes in eating patterns become culturally sanctioned within and across support sys-tems, families will be more willing to consume healthier foods and utilize better food preparationtechniques.
PARENTS’ FOOD CHOICES 9
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

LIMITATIONS
This exploratory study was limited by its small sample size. Although these numbers are commonin focus group research and often suit the needs of exploratory, information-gathering studies, alarger sample size is recommended for future studies. Because the parents had differing percep-tions, exposure to, and experiences with food, there is a need for additional research to assess theplace of culture and community in accounting for food choices and a healthy lifestyle among addi-tional ethnic and cultural groups. Although weight status was not an inclusion criteria for partici-pation in the study, having that information would have provided some basic information aboutthe actual health status of the parents. In addition, the study does not explore parent and child in-volvement in any regular forms of physical activity or other methods of maintaining good health.
CONCLUSIONS
Findings of the study reveal that cultural identity and limited time to prepare healthy meals are keyfactors in determining what foods parents provide for their children. Parents were found to con-tinue the eating habits and food traditions associated with their African American, Caribbean, orHispanic heritage. These practices were perpetuated despite awareness of their association withobesity and increased health risk. Educational interventions that demonstrate recognition of cul-turally-bound eating practices are needed to attract parents and engage them in utilizing practicalalternatives to improve the overall family diet. In addition, parents and children would benefitfrom ongoing opportunities to practice meal planning and preparation within the context of busylifestyle demands. Furthermore, one uniform intervention will not be successful in addressing thefulfillment of dietary needs across cultural groups. Future research must incorporate what isknown about cultural and time influences on diet and examine the impact of regional influencesthat support or hinder the development of a healthy lifestyle inclusive of diet and physical activity.
REFERENCES
Airhihenbuwa, C., Kumanyika, S., Agurs, T., Lowe, A., Saunders, D., & Morssink, C. (1996). Cultural aspects of Afri-can-American eating patterns. Ethnicity & Health, 1, 245–260.
Ard, J., Kumanyika, S., Stevens, V., Vollmer, W., Samuel-Hodge, C., Kennedy, B. et al. (2008). Effect of group racial com-position on weight loss in African-Americans. Obesity, 16, 306–310.
Baker, J., Olsen, L., & Sorensen, T. (2007). Childhood body-mass index and the risk of coronary heart disease in adult-hood. The New England Journal of Medicine, 357, 2329–2337.
Blacksher, E. (2008). Children’s health inequalities: Ethical and political challenges to seeking social justice. HastingsCenter Report, 38(4), 28–35.
Cali, A., & Caprio, S. (2008). Obesity in children and adolescents. Journal of Clinical Endocrinology & Metabolism,93(11), 31–36.
Centers for Disease Control and Prevention. (2009a). NHANES data on the prevalence of overweight among children andadolescents: United States, 2003–2006. CDC National Center for Health Statistics, Health E-Stat. Retrieved May 20,2009, from http://www.cdc.gov/nchs/products/pubs/pubd/hestats/overweight/overwghtchild_03.htm.
Centers for Disease Control and Prevention. (2009b). Overweight and obesity. Retrieved May 20, 2009, from http://www.cdc.gov/nccdphp/dnpa/obesity/childhood/consequences.htm.
Finkelstein, E., Fiebelkorn, I., & Wang, G. (2004). State-level estimates of annual medical expenditures attributable toobesity. Obesity Research, 12, 18–24.
10 SEALY
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14

Freedman, D., Dietz, W., Srinivasan, S., & Berenson, G. (2009). Risk factors and adult body mass index among overweightchildren: The bogalusa heart study. Pediatrics, 123, 750–757.
Goodman, E., Slap, G., & Huang, B. (2003). The public health impact of socioeconomic status on adolescent depressionand obesity. American Journal of Public Health, 93, 1844–1850.
Haas, J., Lee, L., Kaplan, C., Sonneborn, D., Phillips, K., & Liang, S. (2003). The association of race, socioeconomic sta-tus, and health insurance status with the prevalence of overweight among children and adolescents. American Journal ofPublic Health, 93, 2105–2110.
Hudson, C. (2008). Being overweight and obese: Black children ages 2–5 years. Association of Black Nursing Faculty inHigher Education, 19(3), 89–91.
Karnehed, N., Rasmussen, F., Hemmingsson, T., & Tynelius, P. (2006). Obesity and attained education: Cohort study ofmore than 700,000 Swedish men. Obesity, 14, 1421–1428.
Kumanyika, S. (2008). Cultural differences as influences on approaches to obesity treatment, In G. Bray & C. Bouchard(Eds.), Handbook of obesity: Clinical applications (3rd ed., pp. 55–80). London: Taylor & Francis.
Kumanyika, S., & Grier, S. (2006). Targeting interventions for ethnic minority and low income populations. Future ofChildren, 16, 187–207.
Must, A., Spadano, J., Coakley, E., Field, A., Colditz, G., & Dietz, W. (1999). The disease burden associated with over-weight and obesity. Journal of the American Medical Association, 282, 1523–1529.
Ogden, C., Carroll, M., & Flegal, K. (2008). High body mass index for age among U.S. children and adolescents,2003–2006. Journal of the American Medical Association, 299, 2401–2405.
Padgett, D. K. (1998). Qualitative methods in social work research. Thousand Oaks, CA: Sage.Robert Wood Johnson Foundation. (2009). Childhood obesity: New report finds obesity epidemic increases, Mississippi
weighs in as heaviest state. Retrieved July 2, 2009, from http://www.rwjf.org/childhoodobesity/product.jsp?id=45348.Singh, G., Kogan, M., Van Dyck, P., & Siahpush, M. (2008). Racial/ethnic, socioeconomic, and behavioral determinants of
childhood and adolescent obesity in the United States: Analyzing independent and joint associations. Annals of Epide-miology, 18, 682–695.
Strauss, A., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for developing grounded the-ory (2nd ed.). Thousand Oaks, CA: Sage.
U.S. Bureau of Labor Statistics. (2009). The employment situation—September 2009. Retrieved October 22, 2009, fromhttp://www.bls.gov/news.release/pdf/empsit.pdf.
U.S. Census Bureau. (2008). Household income rises, poverty rate unchanged, number of uninsured down. Retrieved July8, 2009, from http://www.census.gov/ Press-Release/www/releases/archives/incomewealth /012528.html.
U.S. Department of Agriculture. (2009). Food CPI, prices, and expenditures. Retrieved July 2, 2009, from http://www.ers.usda.gov/Briefing/CPIFoodAnd Expenditures.
U.S. Department of Agriculture, & U.S. Department of Health & Human Service. (2005). Dietary guidelines for Ameri-cans (6th ed.). Washington, DC: US Government Printing Office.
Walker-Sterling, A. (2005). African-Americans and obesity: Implications for clinical nurse specialist practice. ClinicalNurse Specialist, 19, 193–198.
West, D., Prewitt, T., Bursac, Z., & Felix, H. (2008). Weight loss of black, white, and Hispanic men and women in the dia-betes prevention program. Obesity, 16, 1413–1420.
Zametkin, A., Zoon, C., Klein, H., & Munson, S. (2004). Psychiatric aspects of child and adolescent obesity: A review ofthe past 10 years. Focus, 2, 625–641.
PARENTS’ FOOD CHOICES 11
Dow
nloa
ded
by [
Ein
dhov
en T
echn
ical
Uni
vers
ity]
at 1
5:40
21
Nov
embe
r 20
14