pancreatic cancer: highlights from the 42 nd annual meeting of the american society of clinical...
Post on 22-Dec-2015
215 views
TRANSCRIPT

Pancreatic Cancer: Highlights from the 42nd Annual Meeting of the American Society of Clinical
Oncology, 2006
Muhammad Wasif Saif, M.D.Associate Professor
Yale University School of MedicineNew Haven, CT, USA

AbstractDespite advances in our understanding of the molecular and genetic basis of pancreatic cancer, the disease remains a clinical challenge. Gemcitabine, the standard chemotherapy for pancreatic cancer, offers modest improvement of tumor-related symptoms and marginal advantage of survival. New approaches, alone and in combination with gemcitabine, are being developed to combat this cancer. Combination chemotherapy trials incorporating gemcitabine, cisplatin, 5-fluorouracil, oxaliplatin, or irinotecan generally show improved outcomes in objective response rates but with little or no improvement in survival in phase III trials. In this article, the author describes the key studies presented at the Annual Meeting of ASCO, held in Atlanta, GA from June 2nd to 6th. The studies discussed here include the following: RTOG 9704 (#4007), FFCD-SFRO study (#4008), meta-analysis of gemcitabine plus cisplatin and gemcitabine plus oxaliplatin vs. gemcitabine alone (GERCOR #4003), and ECOG 6201 (Late Breaking Abstract #4004). Based on the results presented at the annual meeting, it comes to us that patients with locally advanced vs. metastatic pancreatic cancer should be studied separately, better understanding of the biology of pancreatic cancer is mandatory and evaluation of novel agents is crucial. We as oncologist have to change our attitudes towards clinical trials and need to think beyond a trial design such as gemcitabine vs. drug of our choice. Environment within which research is being conducted also has to be changed and last but not the least, access to trials for patients with pancreatic cancer is the key step in the fight against pancreatic cancer.

What did we know already?
What we learn?
What we miss?
What we do next?
Lessons from ASCO 2006

Lessons from ASCO 2006
What did we know already?
What we learn?
What we miss?
What we do next?

Median Survival of Patients with Pancreatic Cancer
(Staley’s Classification, 1996) [1]
Localized/Resectable 15-19 months 10%
Locally Advanced6-10 months 30%
Metastatic/Advanced 3-6 months 60%
[1] Staley CA, et al. Pancreas 1996; 12:373-80.

Adjuvant Chemo and Chemo-XRT
No clear consensus on adjuvant therapy for pancreas cancerGITSG [2]:
43 pts randomized into two groups:XRT/bolus 5-FU weekly 5-FU x 2 years vs. Observation
Median survival 20 and 11 months, respectively favoring Chemo-XRT arm
ESPAC – 1 [3]: No benefit for Chemo-XRT (P=0.24)Significant overall benefit for Chemotherapy
(P<0.001)CONKO-001 [4]:
Randomize to: Gemcitabinevs.ObservationDisease free survival:14.2 mvs. 7.5 m
(P<0.001)
GITSG: Cancer 1987 ESPAC-1: Lancet 2003
[2] Cancer 1987; 59:2006-10. [3] Neoptolemos JP, et al. Lancet 2001; 358:1576-85.[4] Neuhaus P, et al. J Clin Oncol 2005, 23(16S):4013.

Locally Advanced Disease
Chemo-XRT may improve survival compared to XRT alone
Chemotherapy is equivalent to the combination of Chemo-XRTin randomized trials
No randomized trials comparing gemcitabine to Chemo-XRTwas available till FFCD-SFRO study presented at ASCO 2006
GITSG [5] # Pts
Median
survival
Localfailure
rate
1-year
1.5-yearXRT (60 Gy/10 weeks) only
25 5.3 monts
24% 10% 5%
XRT (40 Gy/6 weeks) + 5-FU
83 8.4 monts
26% 35% 20%
XRT (60 Gy/10 weeks) + 5-FU
86 11.4 monts
27% 46% 20%
Survival
[5] Moertel CG, et al. Cancer 1981; 48:1705-10.

Gemcitabine Pivotal Studies: Results
[6] Rothenberg ML, et al. Ann Oncol 1996; 7:347-53.[7] Burris HA 3rd, et al. J Clin Oncol 1997; 15:2403-13.
Rothenberg [6] Burris [7] Burris [7]Gemcitabine 5-FU
Partial response6 (9.5%) 3 (5.4%) 0Stable disease17 (27%) 22 (39.3%) 11 (19.3%)Progressive disease 20 (31.7%) 19 (33.9%)
34 (59.6%)
Survival: median3.9 months5.7 months 4.4 months6-month 31% 46% 31%9-month 15% 24% 6%12-month 4% 18% 2%
Time to progression 2.5 months 2.1 months0.9 months
Clinical benefitResponse 17 (27%) 15 (23.8%) 3 (4.8%)
(P=0.0025)
(P=0.0002)
(P=0.0022)

Developmental Strategies of Gemcitabine-Based Therapies in Pancreas Cancer: 4 Approaches
In doublets/Triplets of cytotoxics
With radiation
By fixed dose rateinfusion
With targeted therapies
GemcitabGemcitabineine
II
I
III
IV

Fixed Dose-Rate Gemcitabine
Gemcitabine is a pro-drug that must be phosphorylated to its active metabolites, gemcitabine diphosphate and triphosphate
Conversion of gemcitabine to the active triphosphate form is saturable with standard rates of infusion
Gemcitabine infused at a fixed dose rate of10 mg/m2/min optimizes triphosphate accumulation

Gemcitabine MetabolismGemcitabine
(dFdC) Cell membrane
dFdC-DNA
dFdCDeoxycytidine
deaminase
Deoxycytidine kinase
dF-dCMP
dF-dCTP
dFdU
dF-dCDP

What Did We Know Before?Advanced Pancreatic Cancer
Gemcitabine used Media
n1-year
Author
30-min infusion 5.7 month
s
18% Burris [7]
Fixed dose rate (FDR)
7.8 month
s
24% Tempero [8]
GemOx 9.2 month
s
36% Louvet [9]
[7] Burris HA 3rd, et al. J Clin Oncol 1997; 15:2403-13.[8] Tempero M, et al. J Clin Oncol 2003; 21:3402-8. [9] Louvet C, et al. J Clin Oncol 2005; 23:3509-16.
Survival

Lessons from ASCO 2006
What did we know already?
What we learn?
What we miss?
What we do next?

Pancreatic Cancer UpdateAdjuvant
I. RTOG 9704 (Abstract #4007) [10]
Locally advancedI. FFCD-SFRO study (Abstract #4008)
[11]
MetastaticI. GERCOR: Gem/cisplatin vs. GemOx vs.
Gem alone (Abstract #4003) [12]
II.ECOG 6201: 30-min vs. FDR vs. GemOx (Late Breaking Abstract #4004) [13]
[10] Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007.[11] Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008.[12] Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003.[13] Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004.

Pancreatic adenocarcinoma, status-post resection:T1-4, N0/N1
July 1998 – July 2002538 patients in the trial(pancreatic head carcinoma: 381)
442 patients eligible and analyzable(22 no CA19-9, >8 weeks post op.)
More T3/4 disease in the Gem arm (P=0.013)
Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007. [10]
RTOG 9704: Adjuvant Trial in Pancreatic Ca

Random
5-FU 250 mg/m2/day
for 3 weeks
Gemcitabine1,000 mg/m2 weekly
for 3 weeks
XRT 50.4 Gy + 5-FU (250 mg/m2/day)
5-FU 250 mg/m2/dayfor 12 weeks
Gemcitabine1,000 mg/m2 weekly
for 12 weeks
RTOG 9704: Treatment
AA BB
Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007. [10]

RTOG 9704: Toxicity
Arm A Arm B> Grade 3 Hem 2% 14%*> Grade 3 non-Hem
58% 58%
Ability to complete Chemo
88% 90%
Ability to complete XRT
86% 88%* No difference in febrile neutropenia
Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007. [10]

Regimen Arm A(n=18
7)
Arm B(n=194
)
Median survival(months)
20.6 36.9
P=0.047HR=0.79
(95% CI=0.63-0.99)
3-yearr survival
21% 32%When analysis was inclusive of patients with body/tail tumors (n=442) no significant difference in survival was found (P=0.20).
RTOG 9704: Survival
Pancreatic head Ca (n=381)
Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007. [10]

RTOG 9704: Conclusions
Addition of gemcitabine to 5-FU/XRT improves survival in head pancreatic cancer
Addition of gemcitabine increases hematologic toxicity, but manageable
? New standard to be consideredESPAC-3 [14]:Randomize to Gemcitabine vs.
5-FU vs. ObservationOngoing
[14] National Cancer Research Network Trials Portfolio, 2004. (ISRCTN 37494643)

ESPAC–3: Trial Design
Patients with adenocarcinoma of the pancreashaving ‘curative’ resection
Randomizationstratified by resection margins
Gemcitabine5-FU/FA ObservationFA (20 mg/m2 iv bolus),
5-FU (425 mg/m2 iv bolus)5 days every 28 days,
x6 cycles
1,000 mg/m2 iv infusiononce weekly x3 wks,
1 wk rest,x6 cycles
National Cancer Research Network Trials Portfolio, 2004. (ISRCTN 37494643) [14]

FFCD-SFRO study
Rationale: The GITSG studies have shown a greater
survival after 5 FU-based Chemo-XRT than XRT radiotherapy [5] or polychemotherapy alone [15] in patients with locally advanced non metastatic pancreatic cancer
Gemcitabine is more active than 5-FU in advanced pancreatic cancer [7]
This randomized trial evaluated whether initial Chemo-XRT adds to modern gemcitabine in term of overall survival. Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008. [11]
Phase III trial comparing Chemo-XRT (cisplatin and 5-FU) followed by
gemcitabine vs. gemcitabine alone in patients with locally advanced pancreatic
cancer
[5] Moertel CG, et al. Cancer 1981; 48:1705-10.[7] Burris HA 3rd, et al. J Clin Oncol 1997; 15:2403-13.[15] J Natl Cancer Inst 1988; 80:751-5.

FFCD-SFRO: Study Design
Stratification:• PS (WHO)• Center• Exp surgery or not
Patients with
locally advance
d nonmeta
tstaic pancreat
ic cancer
Ran
dom
izati
on 5-FU
+ cisplatin+ XRT
Gemcitabine
Gemcitabine
InductionMaintenan
ce
Randomized Phase III Study
Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008. [11]
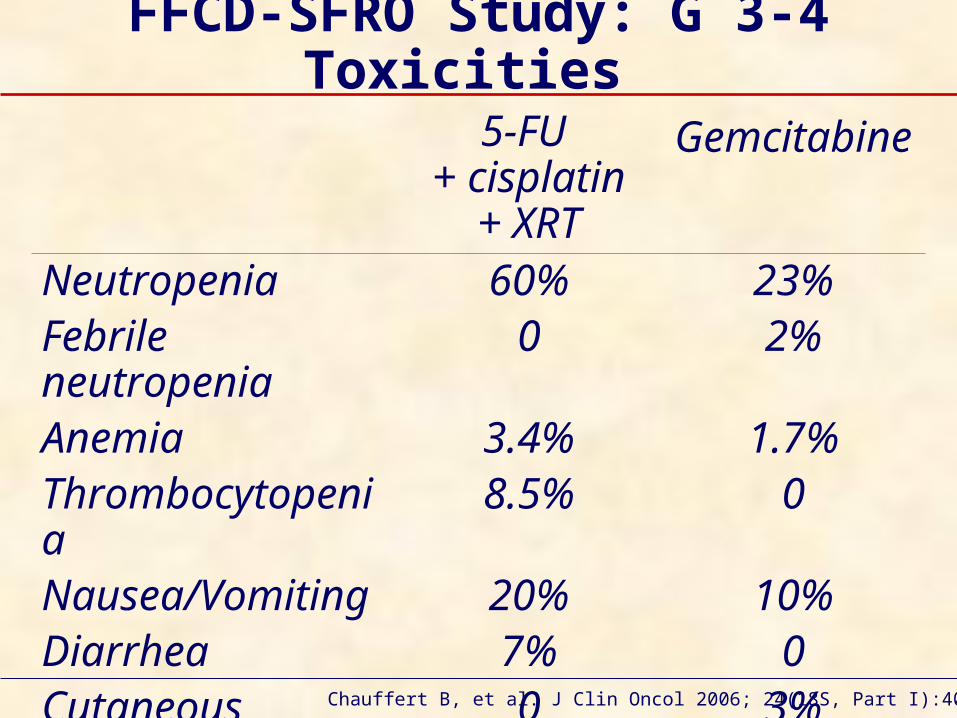
FFCD-SFRO Study: G 3-4 Toxicities
5-FU + cisplatin
+ XRT
Gemcitabine
Neutropenia 60% 23%Febrile neutropenia
0 2%
Anemia 3.4% 1.7%Thrombocytopenia
8.5% 0
Nausea/Vomiting
20% 10%
Diarrhea 7% 0Cutaneous 0 3%
Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008. [11]

FFCD-SFRO Study: Survival
Survival 5-FU +
cisplatin+ XRT
Gemcitabine
Median (months)
8.4 14.3 P=0.014
6 months 78% 82%12 months 24% 51.4%
Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008. [11]

FFCD-SFRO Study: Conclusions
Gemcitabine alone allowed a significant overall survival in locally advanced nonmetatstatic pancreatic cancer
Increased toxicity and decreased maintenance gemcitabine in patients with initial Chemo-XRT may explain this difference
Study was stopped before the planned inclusion due to lower survival with initial Chemo-XRT when compared to Gem alone

Pooled Analysis of 2 Randomized Trials
GERCOR/GISCAD Intergroup Study and a German Multicenter Study
Gem + platinumcompoun
d
Gemalone
Patients (n=503) n=252 n=251ECOG PS = 0 40% 35%Distant metastases
72% 73%
Pathological grading = 3
34% 38%
Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003. [12]

Meta-Analysis: Results GERCOR/GISCAD Intergroup Study and a German
Multicenter Study
Gem + platinu
mcompou
nd
Gemalone
P value; HR
Progression-free survival
5.5months
3.5months
P=0.003
HR: 0.66
Overall survival8.3
months6.7
months
P=0.031
HR: 0.77
Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003. [12]
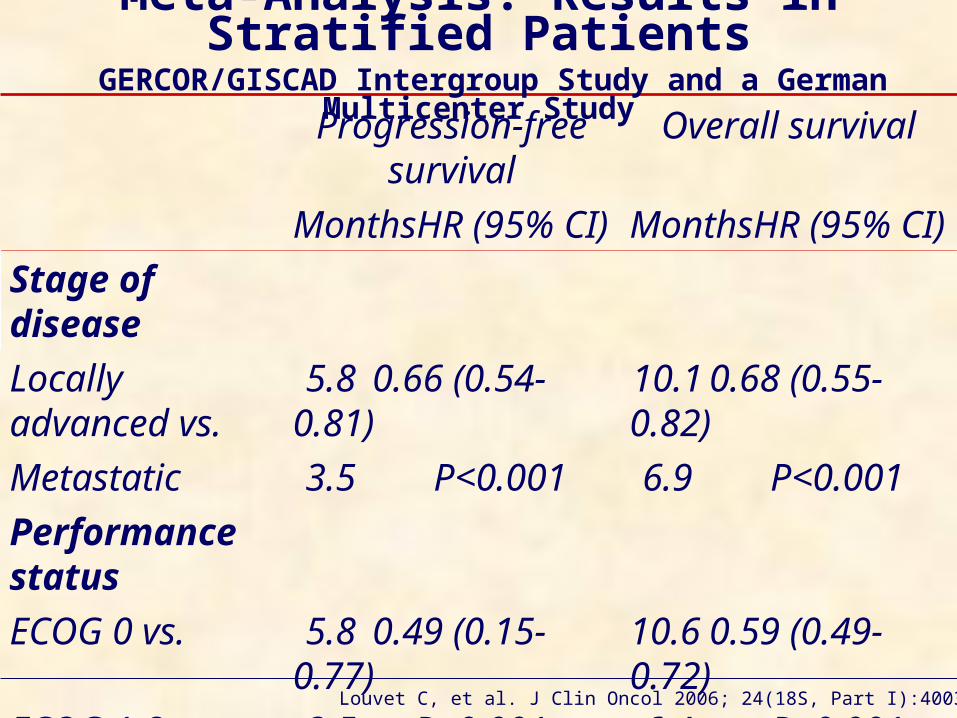
Meta-Analysis: Results in Stratified Patients
GERCOR/GISCAD Intergroup Study and a German Multicenter Study
Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003. [12]
Progression-free survival
Overall survival
MonthsHR (95% CI)
MonthsHR (95% CI)
Stage ofdiseaseLocally advanced vs.
5.80.66 (0.54-0.81)
10.10.68 (0.55-0.82)
Metastatic 3.5 P<0.001 6.9 P<0.001
PerformancestatusECOG 0 vs. 5.80.49 (0.15-
0.77)10.60.59 (0.49-0.72)
ECOG 1-2 3.5 P<0.001 6.4 P<0.001

Meta-Analysis: Conclusions GERCOR/GISCAD Intergroup Study and a German
Multicenter Study PS 0 pts may achieve a greater benefit in
progression-free survival (5.8 vs. 3.5 months; HR 0.49, P<0.001) and overall survival (10.6 vs. 6.4 months; HR 0.59, P<0.001) from treatment with a gemcitabine/platinum doublet
This is similar to data reported by Hermann [16] with gemcitabine + capecitabine
Stage of disease and PS remain important prognostic factors
Careful PS evaluation and stratification is important
Specific studies according to stage: locally advanced vs. advanced should be done
[16] Herrmann R, et al. J Clin Oncol 2005; 23(16S Part I):LBA4010.
Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003. [12]

Meta-Analysis: Comparison to Other Gemcitabine-Based Combinations
Evidence from Randomized Trials
Regimen No. of
cases
Survival
(months)
HR P valu
e
Gem + platinum-analog vs. Gem alone (meta-analysis)
5038.36.7
0.77
0.031
Gem + capecitabine vs.Gem alone [16]
5337.46.0
0.80
0.026
Gem + erlotinib vs.Gem alone [17]
5306.45.9
0.81
0.034
[16] Herrmann R, et al. J Clin Oncol 2005; 23(16S Part I):LBA4010.[17] Moore MJ, et al. J Clin Oncol 2005; 23(16S):1.

Gemcitabine administration: 30-min vs. FDR
Gemcitabine dose intensity across single agent and combined arms
Platinum analogs (oxaliplatin is not cisplatin)
It is not know how many pts received XRT prior
Impact of these differencescannot be implicated
Meta-Analysis: Differences in Groups

Meta-Analysis: Pitfalls
ObviousExtent of diseasePerformance statusIt will take a lot of patients to show a
differenceOxaliplatin is not cisplatin30-min gemcitabine is not FDR
gemcitabine Pharmacologic basis Toxicity Cost (time of infusion)

ECOG 6201: Advanced Pancreatic Cancer
Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]
Random
Gemcitabine 1,000 mg/m2 30 min i.v.weekly x7 on 1 off , then x3 on 1 off
Gemcitabine 1,500 mg/m2
150 min i.v. (10 mg/m2/min FDR) weekly x3 on 1 off
Gem 1,000 mg/m2, FDR, day 1Oxaliplatin 100 mg/m2, day 2every 14 days
AAn=280
BBn=277
CCn=276
March 2003 – March 2005: 833 patientsMedian follow-up: 5.7 months
Males: 53% - PS 0-1: 88% - Metastases: 88%

Primary:To determine whether either FDR gemcitabine or GemOx increases survival compared with standard 30-min infusion
Secondary:Progression-free survivalToxicityQuality of life
ECOG 6201: Objectives
Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]

Adenocarcinoma or poorly differentiated
No > grade 2 peripheral neuropathy
Prior adjuvant Chemo-XRT allowed
No prior gemcitabine or oxaliplatin
ECOG PS > 2
ECOG 6201: Inclusion Criteria
Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]

ECOG 6201: Worst Toxicity
Arm A Arm B Arm CGrade 3 4 3 4 3 4Neutrophils 19%15%29%31%10%14%
Platelets 12% 0 29% 0 10%<1%
Hemoglobin 8% 2% 15% 3% 4% 1%
Nausea 7% 0 8%<1%
14%<1%
Vomiting 5% 0 5% 1% 10% 1%
Infection 2% 1% 5%<1%
1% 0
Peripheral neuropathy
0 0<1%
0 9% 0
Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]

ECOG 6201: Response rate (RECIST)
Response Arm A
Arm B
Arm C
Complete/partial
5% 10% 9%
Stable disease
29% 29% 29%
Progressive disease
26% 24% 24%
Unknown 41% 37% 38%Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]

ECOG 6201: Survival and HR
Survival Arm A Arm B Arm CMedian (months)
5.0 (4.5-5.6)
6.0 (5.4-6.9)
6.5 (6.1-6.8)
1-year 17% 21% 21%HR 95% CI
30 min vs. FDR (A vs. B)
1.21 1.00-1.45
P=0.053
30 min vs. GemOx (A vs. C)
1.22 0.73-1.05
P=0.045Survival by
disease extentLocally advance
d
Advanced
Median (months) 9.1 5.4 P=0.001Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004. [13]

ECOG 6201: Conclusions
Both FDR and GemOx had approximately 1 month longer median overall survival than standard Gem, but not statistically significant
Survival outcome with 30 min gemcitabine is persistent
Median overall survival: slightly less than other trials:
Study design, such as locally advanced and metastatic patients, need to be studied separately
FDR and GemOx with increased toxicity: Hematologic, nausea and vomiting with
FDR Neuropathy with GemOx
ECOG 6201 adds to multiple studies that showed adding another cytotoxic to gemcitabine does not add any benefit to the modest survival by gemcitabine alone
Progression-free survival and quality of life not given at the meeting

Lessons from ASCO 2006
What did we know already?
What we learn?
What we miss?
What we do next?

Promising New Regimens inthe Cooperative Groups
Gemcitabine + bevacizumab [18]Median survival of 8.8 monthsNow in randomized trial vs.
gemcitabine aloneGemcitabine + cetuximab [19]Promise in this regimen was a 1-year
survival rate of 32%Erlotinib data adds encouragement to
this trialNow in randomized trial vs.
gemcitabine aloneIrinotecan + docetaxel [20] Ignored largely, but phase II trial had
a 9-month median survivalBeing tested in a multi-institutional
trial with or without cetuximab to confirm this data
[18] Kindler HL, et al. J Clin Oncol 2005; 23:8033-40.[19] Xiong HQ, et al. J Clin Oncol 2004; 22:2610-6.[20] Kurtz JE, et al. Hepatogastroenterology 2003; 50:567-70.

Lessons from ASCO 2006
What did we know already?
What we learn?
What we miss?
What we do next?

Promise from Non-Clinical Trials
Better understanding of the biology of pancreatic cancer is emerging
New mouse models show promise as potentially more predictive than the old models
Newer imaging techniques may help to gauge disease better
Palliative care is improvingWe can’t underestimate this as
data suggest that improved pain control alone impacts on survival in this disease

GemcitabineAlone
Can Oncologists Change?
RANDOMIZE
Gemcitabine + Your Drug
Here

What Really Needs to Change?
Oncologist attitudes towards clinical trials
Environment within which research is being conducted
Access to trials for patients

What Actions Need to Be Taken to Change?
Study design:Locally advanced and metastatic patients
need to be studied separatelyAppropriate trial size:Gemcitabine + cisplatin may have been
underpoweredGemcitabine + erlotinib may have been
overpoweredAdvocacy input needs to be sought
early:How much benefit is enough to a patient?How much toxicity is too much for a
patient?Regulatory environment: Gemcitabine vs. drugs X + Y wins no
FDA approval and may never be able to happen
Conclusions
30-min Gem vs. FDR? Revisit platinum compounds probably not
FFCD another study negating benefit of platinum compounds
Need to identify surrogates for survival Accelerate testing new drugs, including
targeted agents Move more quickly to adjuvant setting Focus on 2nd Line Rx as most 1st Line regimens
failed in the last decade Standardize our approach: design, analysis,
reporting Move away from “ONE SIZE FITS ALL”
approach to TAILORED patient management

References1. Staley CA, et al. Pancreas 1996; 12:373-80.2. Cancer 1987; 59:2006-10.3. Neoptolemos JP, et al. Lancet 2001; 358:1576-85.4. Neuhaus P, et al. J Clin Oncol 2005, 23(16S):4013.5. Moertel CG, et al. Cancer 1981; 48:1705-10.6. Rothenberg ML, et al. Ann Oncol 1996; 7:347-53.7. Burris HA 3rd, et al. J Clin Oncol 1997; 15:2403-13.8. Tempero M, et al. J Clin Oncol 2003; 21:3402-8. 9. Louvet C, et al. J Clin Oncol 2005; 23:3509-16.10.Regine WF, et al. J Clin Oncol 2006; 24(18S, Part I):4007.11.Chauffert B, et al. J Clin Oncol 2006; 24(18S, Part I):4008.12.Louvet C, et al. J Clin Oncol 2006; 24(18S, Part I):4003.13.Poplin E, et al. J Clin Oncol 2006; 24(18S, Part I):LBA4004.14.National Cancer Research Network Trials Portfolio, 2004.
(ISRCTN 37494643)15.J Natl Cancer Inst 1988; 80:751-5.16.Herrmann R, et al. J Clin Oncol 2005; 23(16S Part
I):LBA4010.17.Moore MJ, et al. J Clin Oncol 2005; 23(16S):1.18.Kindler HL, et al. J Clin Oncol 2005; 23:8033-40.19.Xiong HQ, et al. J Clin Oncol 2004; 22:2610-6.20.Kurtz JE, et al. Hepatogastroenterology 2003; 50:567-70.

Keywords bevacizumab; capecitabine; cetuximab; Cisplatin; Chemotherapy, Adjuvant; gemcitabine; Epidermal Growth Factor; erlotinib; Fluorouracil; oxaliplatin; Pancreatic Neoplasms; Radiation; Radiotherapy, Adjuvant; Receptor, Epidermal Growth Factor; Review; Vascular Endothelial Growth Factor AAbbreviations ASCO: American Society of Clinical Oncology; CONKO: Charité Onkologie - clinical studies in GI cancers; ECOG: Eastern Cooperative Oncology Group; EGFR: epidermal growth factor receptor; ESPAC: European Study Group of Pancreatic Cancer; FA: folinic acid; FDR: fixed dose rate; FFCD-SFRO: Federation Francophone de Cancerologie Digestive and Societe Francaise de Radiotherapie Oncologique; Gem: gemcitabine; GemOx: gemcitabine plus oxaliplatin; GERCOR: Groupe d'Etude et de Recherche en Cancreologie Onco-Radiotherapic; GISCAD: Italian Group for the Study of Gastrointestinal Tract Carcinomas; GITSG: Gastro-Intestinal Study Group; HR: hazard ratio; LBA: late breaking abstract; PS: performance status; RECIST: Response Evaluation Criteria in Solid Tumors; RTOG: Radiation Therapy Oncology Group; XRT: radiation/radiotherapy

The author is grateful to the authors/presentors of the major studies discussed in this review article:Chauffert B. Unite INSERM 517, Faculty of Medicine, 7, Boulevard Jeanne d'Arc, BP 87900, 21079, Dijon, France. [email protected] (FCCD-SFRO).Louvet C. Institut National de la Sante et de la Recherche Medicale (INSERM), Unit 643 and Institut de Transplantation et de Recherche en Transplantation (ITERT), Nantes, France. [email protected] (meta-analysis: GERCOR/GISCAD).Poplin EA. Cancer Center of New Jersey, New Brunswick, New Jersey 08901, USA. [email protected] (ECOG 6201)Regine WF. University of Maryland School of Medicine, Radiation Oncology Clinical, Gudelsky Tower; Room GGK-17E, Baltimore, MD 21201, USA. [email protected] (RTOG 9704)CorrespondenceMuhammad Wasif SaifSection of Medical Oncology - Yale University School of Medicine333 Cedar Street; FMP 116New Haven, CT 06520 - USAPhone: +1-203.737.1569Fax: +1-203.785.3788E-mail: [email protected]
Acknowledgement