palliative medicine and hospice – when comfort is the goal michelle schultz, md director of...
TRANSCRIPT

Palliative Medicine and Hospice – When Comfort is the Goal
Michelle Schultz, MDDirector of Palliative MedicineSSM St. Mary’s Health [email protected]

Objectives
•Summarize the benefits of palliative care and hospice care for patients with advanced illness
•Describe basic principles of medical management of chronic pain
•Apply pain management strategies for elderly patients seeking comfort in advanced or terminal illness
What is Palliative Care?
Medical care for people with serious illnesses Focused on providing relief from pain, symptoms
and stress Improving QOL for patient and family Provided by a team of doctors, nurses and other
specialists who work with a patient’s other doctors to provide extra layer of support
Appropriate at any age or stage of a serious illness Can be provided together with curative treatment
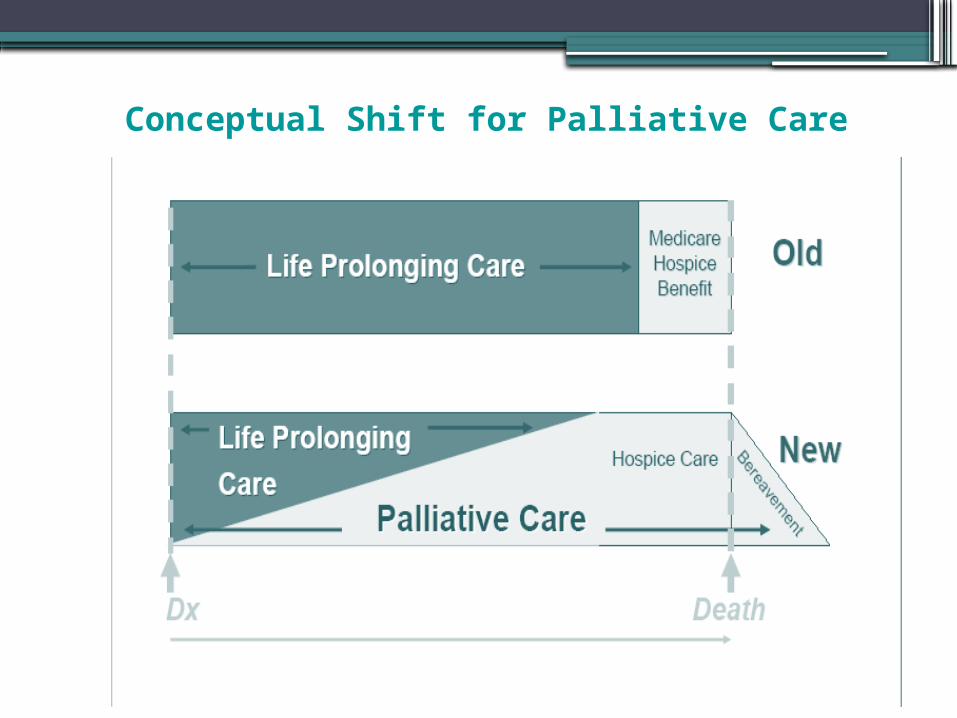
Conceptual Shift for Palliative Care

Palliative Care Improves Care in 3 Domains
1. Relieves physical and emotional suffering
2. Improves patient-professional communication and decision-making
3. Coordinates continuity of care across settings

The Palliative Medicine Team
•Physicians•Nurses•Social Workers•Chaplains
Working together to improve quality of life and decrease family stress

What Does the Palliative Medicine Team Do?
•Helps to relieve pain and other symptoms• Provides support throughout all phases of
chronic illness • Facilitates discussions about goals of care•Helps make decisions with respect to
healthcare wishes • Enhances communication with the healthcare
team•Discusses options for care in the hospital and
beyond• Provides community resources

Goals of Care
• Cure of disease• Prolongation of life• Maintenance or improvement in Quality of life• Relief of suffering• Maintaining control• Staying at home• Minimizing burden on family• A good death

Identifying Goals to Hope For
•False hope may deflect from other important issues▫Unfinished business▫Foregoing aggressive unpleasant measures▫Accepting hospice care
•Redirect from unrealistic to realistic goals
Honest Communication about Prognosis and Treatment Options
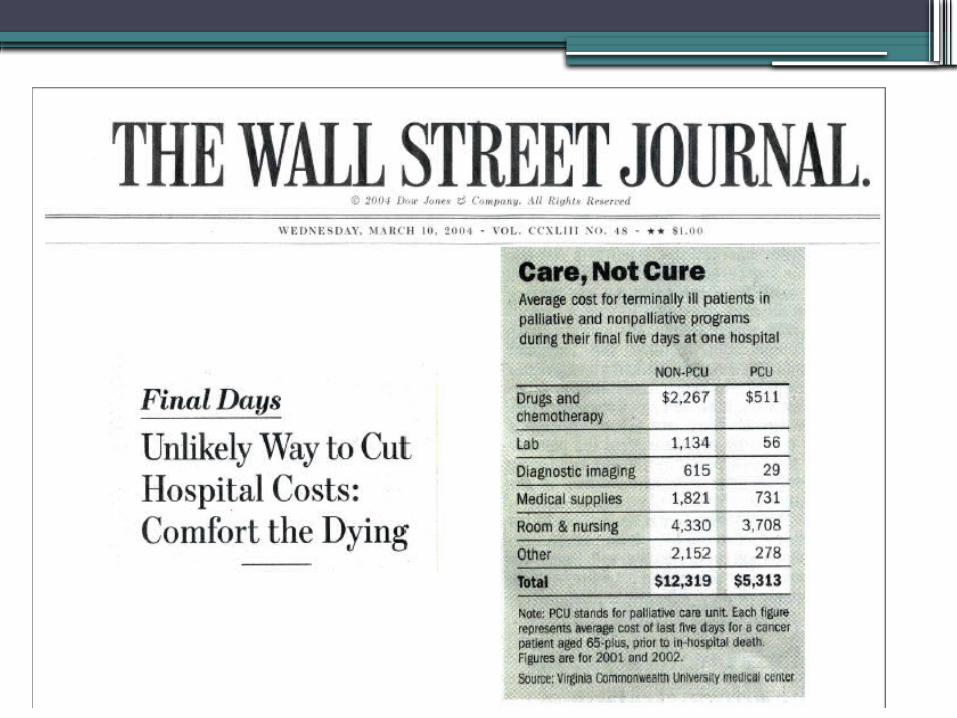
Palliative Care Reduces Hospital Costs
How? –Talking with patients and families and
treating physicians about what is happening and their realistic options leads to more conservative choices.
–Allows provision of higher quality care in appropriate, often less costly, settings.
Demand for Palliative Care
•What Patients and Families want…▫Pain and symptom control▫Avoid inappropriate prolongation of the
dying process▫Achieve a sense of control▫Relieve burdens on family▫Strengthen relationships with loved ones
▫ Singer et al, JAMA 1999;281:163-168▫ Steinhauser et al, Ann Int Med 2000;132:825-32

…And What They Get
• Half of patients had moderate-severe pain >50% of last 3 days of life
• 38% of those who died spent >10 days in ICU, in coma or on a ventilator (Unable to say goodbye)
National Data on the Experience of Advanced Illness in 5 Teaching Hospitals (9000 pts/median survival 6 mo.)

Is Palliative Care the Same Thing as Hospice?

How Does Palliative Care Differ from Hospice?
• Hospice care provides palliative care for those in the last weeks to months of life under a Federal Medicare Benefit. Complex treatments like chemotherapy, dialysis and hospitalizations are usually excluded.
•Non-hospice palliative care is appropriate at any point in a serious illness. It can be provided at the same time as life-prolonging treatment and is not dependent on prognosis.
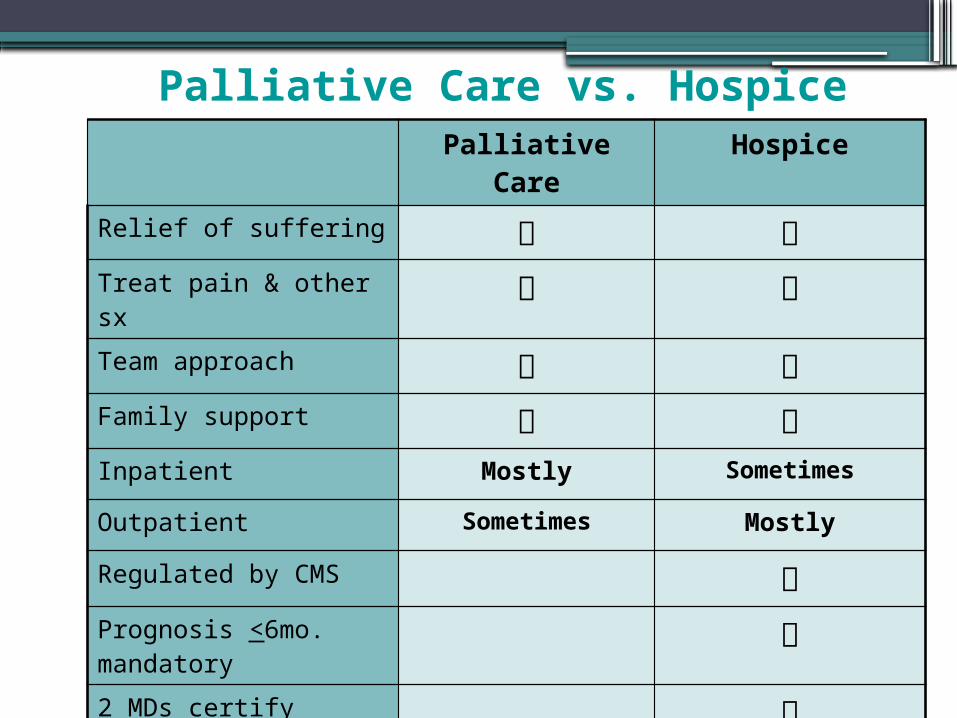
Palliative Care vs. HospicePalliative Care Hospice
Relief of suffering Treat pain & other sx Team approach Family support Inpatient Mostly Sometimes
Outpatient Sometimes Mostly
Regulated by CMS Prognosis <6mo. mandatory
2 MDs certify terminal

Pain among hospitalized patients with serious illness
% of 5176 pts reporting moderate to severe pain between days 8-12 of hospitalization
▫ Colon cancer 60%▫ Liver failure 60%▫ Lung cancer 57%▫ MOSF + cancer 52%▫ MOSF + sepsis 52%▫ COPD 44%▫ CHF 43%
▫ Desbiens JAGS 2000;48:S183-186

WHO 3-step Ladder
1 mild1 mild
2 moderate2 moderate
3 severe3 severe
Morphine
Hydromorphone
Methadone
Levorphanol
Fentanyl
Oxycodone
± Adjuvants
Morphine
Hydromorphone
Methadone
Levorphanol
Fentanyl
Oxycodone
± Adjuvants
A/Codeine
A/Hydrocodone
A/Oxycodone
Tramadol
± Adjuvants
A/Codeine
A/Hydrocodone
A/Oxycodone
Tramadol
± AdjuvantsASA
Acetaminophen
NSAIDs
± Adjuvants
ASA
Acetaminophen
NSAIDs
± Adjuvants

Opioid Pharmacology
•Duration of effect of “immediate-release” formulations (except methadone)▫3–5 hours po ▫shorter with parenteral bolus
•Steady state after 4–5 half-lives▫(24 hours)

THERAPEUTIC RANGE
PRN Dosing
TIME
Conc.
Overmedicated
PAIN

Routine dosingImmediate-release preparations
•Codeine, hydrocodone, morphine, hydromorphone, oxycodone, tramadol▫dose q 4 h for oral agents, q 3 h for IV▫Adjust dose daily
• mild / moderate pain 25%–50%• severe pain 50%–100%
• Adjust more quickly for severe uncontrolled pain
Extended-release preparations
• Improve compliance•Better pain relief▫Sleep through the night
•MS Contin, Oxycontin – dose every 12 hours▫Adjust dose q 2–3 days (once steady state
reached)•Fentanyl Patch - dose every 72 hours▫Steady state in ~24 hrs▫Advantages: Compliance, swallowing
problems•Methadone – dose BID▫See below

The Sea of Pain

Breakthrough dosing
•Use immediate-release opioids▫10% - 15% of 24-hr dose prn▫May dose q 1-2 hours in extreme
cases•Do NOT use extended-release opioids
prn
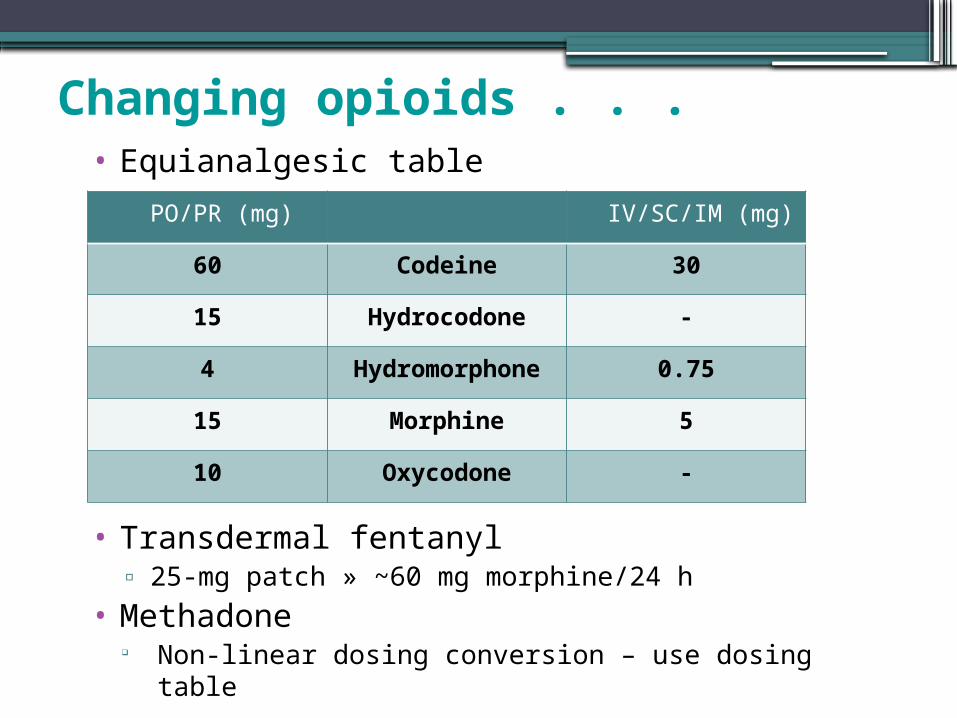
Changing opioids . . .• Equianalgesic table
• Transdermal fentanyl▫ 25-mg patch » ~60 mg morphine/24 h
• Methadone Non-linear dosing conversion – use dosing table
PO/PR (mg) IV/SC/IM (mg)
60 Codeine 30
15 Hydrocodone -
4 Hydromorphone 0.75
15 Morphine 5
10 Oxycodone -
. . . Changing opioids
•Cross-tolerance▫Start with 50%–75% of published
equianalgesic dose more if pain less if adverse effects

Converting to MS Contin
• Calculate total daily dose of each opioid• Convert to oral morphine equivalent ▫MEDD
• Divide by 2• Add 10% - 15% of 24o morphine dose as
immediate release q 3o prn

Methadone
•Synthetic opioid•Used to treat addiction and chronic pain•Schedule II▫Addiction: Prescribers must register with
DEA for that purpose▫Pain: Any prescriber with Schedule II
privileges •Safety concerns▫<5% of opioid prescriptions but ~33% of
opioid-related deaths
Methadone Advantages
▫Low cost▫High oral bioavailability▫Naturally long acting - may dose QDay or
BID▫Steady analgesic effect▫Blocks NMDA receptors – efficacious in
neuropathic pain▫Lack of active metabolites▫No dose adjustments in renal impairment
Methadone Disadvantages
•Stigmatization•Complex pharmacology
Dose conversion ratios are complex and vary based on current opioid dosage
Long variable half life (6 – 190 hours) can lead to drug accumulation, sedation,
confusion, and respiratory depression, especially in the elderly or with rapid dose adjustment
• Prolongs QT interval – may lead to fatal arrhythmias (torsades de pointe)
•Not recommended for breakthrough pain

Methadone Caveats
• Elimination half life longer than its duration of action• Precise opioid dose ratio for methadone is unknown• Equianalgesic dosing in not linear:▫Dose varies inversely with the previous oral morphine
equivalent dose• Drug interactions at CYP 450(3A4, 2D6):▫ Inhibitors ↑ methadone level = toxicity▫ Inducers ↑clearance = pain

CYP Inhibitors and Inducers
Inhibitors Inducers
Macrolides (erythromycin, azithromycin)
Anticonvulsants (phenobarbital, phenytoin)
Imidazoles (ketoconazole) Rifampin
SSRIs (paroxetine, fluoxetine) Corticosteroids
Antiviral drugs (ritonavir)
Benzodiazepines (lorazepam)
Quinolones (ciprofloxacin)
Acute alcohol ingestion Chronic alcoholism
Dosing Methadone: Overview
1. Determine the oral morphine equivalent daily dose (MEDD)
2. Select the initial methadone dose based on the oral MEDD
3. Stop the previous opioid and start methadone4. Utilize immediate-release opioid for
breakthrough pain▫ Switch to an opioid different than the one
used previously if toxicity experienced▫ Do not use methadone for breakthrough pain
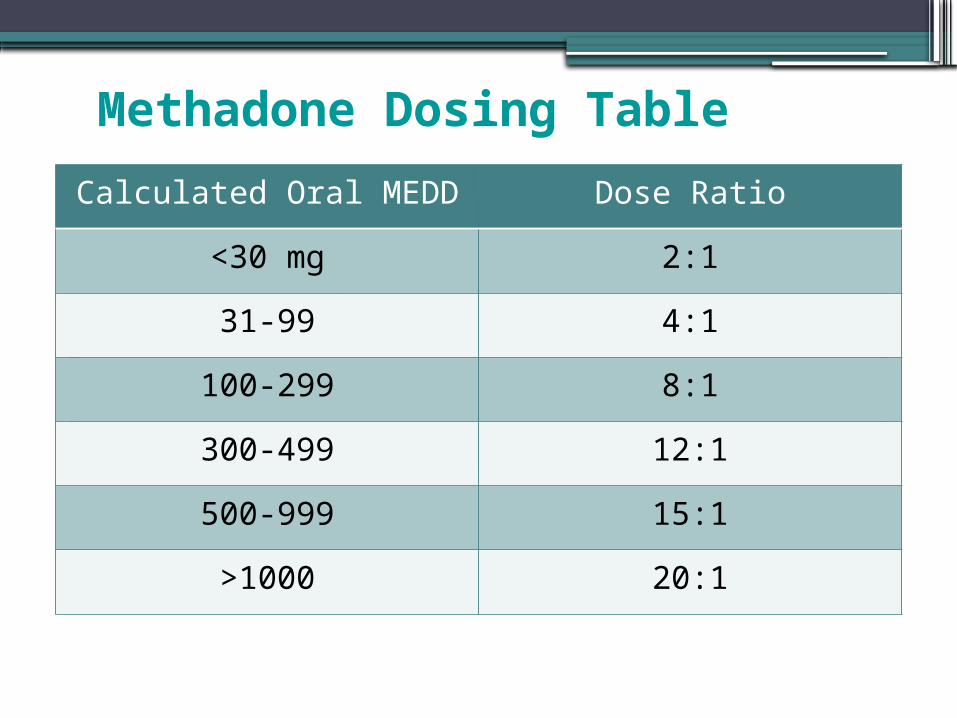
Methadone Dosing Table
Dose Ratio*
31-99mg 4
100-180mg 6
181-240mg 8
241-300mg 10
Calculated Oral MEDD Dose Ratio
<30 mg 2:1
31-99 4:1
100-299 8:1
300-499 12:1
500-999 15:1
>1000 20:1
American Pain Society – Methadone Guidelines• Careful patient selection▫ Baseline EKG - Assess QTc▫ Drug interactions – avoid if other QT-prolonging
medications
• Patient Education about risks• Low starting dose• Opioid naïve patients▫ 2.5 mg q 8 h starting dose
• Slow titration - no more than every 5 days• Buprenorphine as alternative for patients with
opioid addiction and prolonged QTc
“Follow Directions: How to Use Methadone Safely”
•FDA educational materials•Designed to educate both consumers and
healthcare professionals •Brochures, fact sheets, and posters are
available for download or order at the SAMHSA website
• http://www.dpt.samhsa.gov/methadonesafety/print_materials.aspx
Pain poorly responsive to opioids
• If dose escalation adverse effects▫Use alternative route of administration (intrathecal) opioid (“opioid rotation”)
▫Add adjuvant▫Try a non-pharmacologic approach

Adjuvant analgesics
•Medications that supplement primary analgesics▫May themselves be primary analgesics Acetaminophen, NSAIDs
▫May have different primary indication Anticonvulsants, antidepressants
▫Use at any step of WHO ladder
Burning, tingling, neuropathic pain• Anticonvulsants▫Gabapentin, Pregabalin▫Carbamazepine, Phenytoin
• Tricyclic antidepressants (TCAs)▫Amitriptyline, desipramine
• SNRI▫Duloxetine
• Corticosteroids• Lidoderm Patch• Capsaicin Cream

Cannabinoids
•Work synergistically to allow lowered opioid dosing
•Marginal benefit for central pain and spasticity associated with multiple sclerosis
•May reverse opioid-associated hyperalgesia
•Prevention and treatment of chemotherapy-induced neuropathy
Strouse TB: J Pall Med 2015;18:7-10

Importance of Pain Management in Elderly• Rapidly growing segment of the population• Prevalence of pain increases with age• May go unreported due to belief that it is a
normal part of aging• Consequences▫ Impairment in ADLs, ambulation, stamina▫Requirement for higher level of caregiving

Prevalence of pain in Elderly
• Pain in elderly cancer patients
• 66% of geriatric Nursing home patients have chronic pain
• 34% of these unrecognized by their physician
Age Untreated Pain
65-74 21%
75-84 26%
>84 30%

Pain Assessment
• Location (1°, referral pattern)
• Quality• Timing• Severity• Radiation
• Modifying factors• Impact on function• Effect of prior
treatments• Patient perspectives
The patient’s self report is the single most reliable indicator of pain!


Supplemental Pain Assessmentin Elderly• Cognitive function• Depression Screen• Functional Status• Gait/Balance• Loss of sensory/visual/auditory acuity
American Geriatric Society’s Indicators of Pain
• Facial expressions• Verbalizations/vocalizations▫ Crying/Moaning/Groaning
• Touching/rubbing area• Change in gait or posture• Changes in interpersonal interactions• Changes in activity patterns or routines• Mental status changes• Change in functional status• Withdrawal• Agitated behavior
• Seek reports from caregivers and family
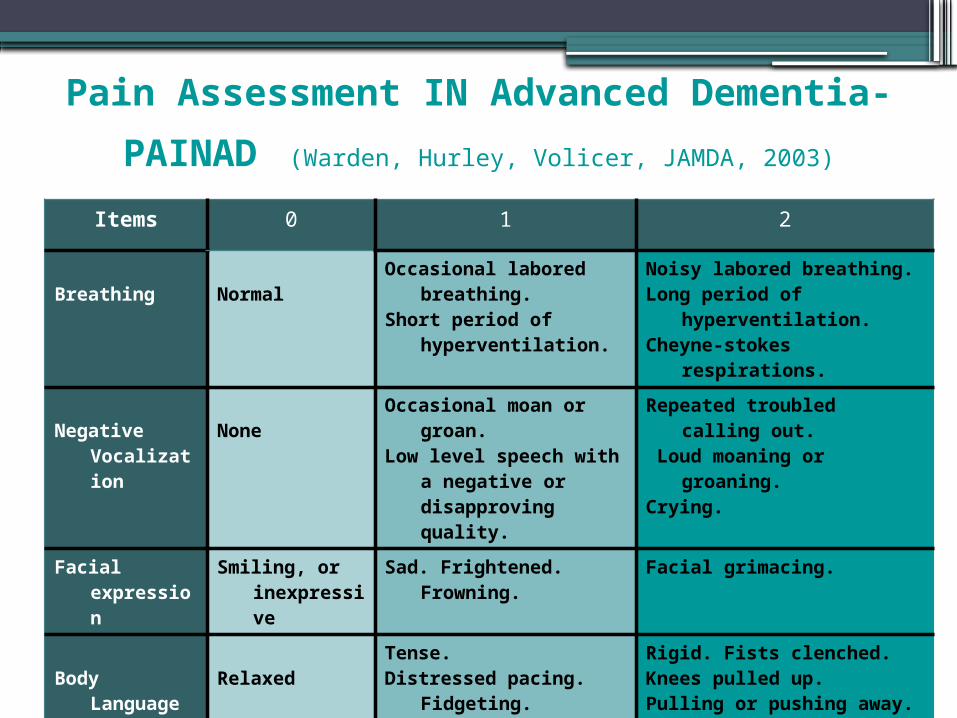
Items 0 1 2
Breathing NormalOccasional labored
breathing.Short period of
hyperventilation.
Noisy labored breathing.Long period of
hyperventilation. Cheyne-stokes
respirations.
Negative Vocalization
NoneOccasional moan or
groan. Low level speech with
a negative or disapproving quality.
Repeated troubled calling out.
Loud moaning or groaning.
Crying.
Facial expression
Smiling, or inexpressive
Sad. Frightened. Frowning.
Facial grimacing.
Body Language
RelaxedTense. Distressed pacing.
Fidgeting.
Rigid. Fists clenched. Knees pulled up. Pulling or pushing away.
Striking out.
ConsolabilityNo need to
consoleDistracted or
reassured by voice or touch.
Unable to console, distract or reassure.
Pain Assessment IN Advanced
Dementia- PAINAD (Warden, Hurley, Volicer, JAMDA, 2003)

Multidisciplinary Approach to Treatment•Pharmacotherapy•Physiotherapy•Psychosocial support• Interventional procedures

Factors Leading to Poor Compliance in Elderly
•Compromises in ▫Communication skills▫Cognitive function
•Cost•Polypharmacy
• KISS: Keep it Simple Stupid
Pharmacokinetic Changes
• Altered drug distribution▫ Increased body fat and decreased muscle mass
Lipophilic drugs (e.g. fentanyl, lidocaine) will have increased duration of action
▫Decreased body water (diuretics, dehydration) Hydrophilic drugs will have higher plasma concentrations
resulting in increased side effects▫Poor nutrition/decreased albumin effects protein-
bound drugs (increased free drug) NSAIDS, antiepileptics
▫Drug half life increased for benzodiazepines and tricyclics
• Declines in renal and hepatic function affect clearance

American Geriatrics Society Pharmacotherapy
Recommendations - 2009•Acetaminophen should be considered as initial
and ongoing therapy because of good safety and efficacy profiles
•NSAIDS should rarely be considered in highly selected patients with extreme caution▫Risks of renal, GI and cardiovascular toxicity▫Use with PPI▫Patients on ASA for CVD should not use
ibuprofen

American Geriatrics Society Pharmacotherapy
Recommendations - 2009•Opioids should be used for patients with
continuous or frequent pain with poor QOL▫Regularly assess for and anticipate adverse
effects and adjust accordingly▫Use around the clock scheduled dosing to
achieve steady state▫Provide breakthrough doses for those on long-
acting opioids▫Cautious use of methadone
American Geriatrics Society Pharmacotherapy Recommendations - 2009
•Adjuvants for neuropathic pain▫Use lowest dose and titrate slowly▫Provide adequate therapeutic trial before
changing▫Avoid tricyclic antidepressants (TCAs) due to
high frequency of adverse anticholinergic and cognitive effects
▫Consider topical agents for localized pain Lidocaine for neuropathic pain Topical NSAIDS, Capsaicin, menthol for non-
neuropathic pain
Case 1 – DeborahInpatient Palliative Care Consult
• 52 yo lady with metastatic cervical cancer to retroperitoneal and para-aortic lymph nodes failing chemotherapy and radiation
• Hospitalized March 23, 2014 with 10/10 pain in the right flank, right lower quadrant, right groin radiating down right leg with burning quality
• Also complained of n/v, anorexia, wt loss and constipation (no BM x 7 days)
• Right hydronephrosis and elevated creatinine

Case 1 (Cont.)
• Rx Ketoralac 15 mg IV q 6 hrs and Hydromorphone 2 mg IV q 3 h prn pain (total 9 mg) with good relief within 24 hours
• Changed to Hydromorphone 2 mg PO q 3 h prn without relief

Doing the Math
• IV Hydromorphone: PO Morphine 20:1• Hydromorphone 9 mg iv = Morphine 180 mg PO
• Morphine 60 mg PO: Fentanyl patch 25 mcg/h q 72 h
• Fentanyl 75 mcg/h q 72h
• Breakthrough dose (1/6 of 24 h dose)• 30 mg PO morphine = 8 mg PO hydromorphone

Deborah’s regimen
• Fentanyl patch 75 mcg/h q 72 h• Hydromorphone 8 mg PO q 2 h prn• Lidoderm patch to right flank and right leg• Gabapentin 300 mg q 8 h• Dexamethasone 4 mg PO Qday• Prochlorperazine 10 mg ac and qhs• Senna-s 2 tabs bid• Dulcolax tab prn constipation

Hospice course
• Excellent response initially – gained weight, went camping
• June 14 – Increased Fentanyl patch to 100 mcg/h and Hydromorphone 1-2 tabs q 2 h prn
• Nov. 1 – Increased Fentanyl patch to 125 mcg/h q 72 h
• Dec. 1 – Increased Fentanyl patch to 175 mcg/h q 72 h and Hydromorphone 10 mg/ml 10-20 mg SL q 2 h prn pain
• Died 12/7/14

Case 2 - Michael
•68 yo man with lung cancer and paraspinal mass invading ribs and spine
•Progressive disease despite chemotherapy and radiation therapy
•Elected hospice care from home•Pain 8/10, continuous, throbbing

Case 2 - Michael• Previous pain regimen▫MS Contin 60 mg q 12 h▫MSIR 15 mg q 3 h prn breakthrough pain▫Taking 8 doses of per day with little relief
• Having myoclonic jerks and visual hallucinations

Conversion to Methadone• Oral MEDD▫ MS Contin = 240 mg/day (120mg x 2)▫ MSIR = 120mg/day (15mg x 8)▫ Total oral MEDD = 360 mg/day (240mg + 120mg)
• Initial methadone dose▫ Dose ratio from table (300 – 499 mg MEDD) = 12▫ Initial methadone dose = 30 mg/day (360÷12)▫ Methadone 15 mg every 12 hours
• Breakthrough medication▫ 10-15% of 24 h morphine dose ≈40-60 mg▫ Morphine 20 mg/ml 2-3 ml q 2 h prn pain

Adjuvants
• Dexamethasone 4 mg Q day• Lidoderm Patch to site of pain
• TENS unit• Massage therapy

One week later
•Averaging 4-5 breakthrough doses/day•~180 mg MEDD•Same dosing ratio (12) ~15 mg
methadone• Increased Methadone to 20 mg q 12 h
•Pain level currently 3/10