palliative care public - 4-15v2 curtis
TRANSCRIPT

www.uwpalliativecarecenter.com
Palliative Care and Advance Care Planning: What are they and what do you need to know
about them?
J. Randall Curtis, MD, MPHDirector, Cambia Palliative Care Center of
ExcellenceHarborview Medical Center, University of Washington

Disclosures and Funding
• Disclosures– No financial conflict of interest
• Funding
Outline: Four Questions
• What is palliative care?
• What are advance directives and advance care planning?
• How can we improve communication about palliative care?
• What can you do?

Definition of Palliative Care
Specialized care for people with serious illnesses… focused on providing patients with relief from the symptoms, and stress of a serious illness - whatever the diagnosis.
The goal is to improve quality of life for both the patient and family… provided by a team who work with a patient's other doctors to provide an extra layer of support.
Palliative care is appropriate at any age and at any stage in a serious illness, and can be provided together with curative treatment.
Center to Advance Palliative Care 2011

Understanding the Words
• Palliative care: Improving quality of life for patients with serious illness
• End-of-life care: For those who are entering the last phase of life
• Hospice: A model for delivery of end-of-life care
Palliative Care
Hospice Care
End-of-life Care
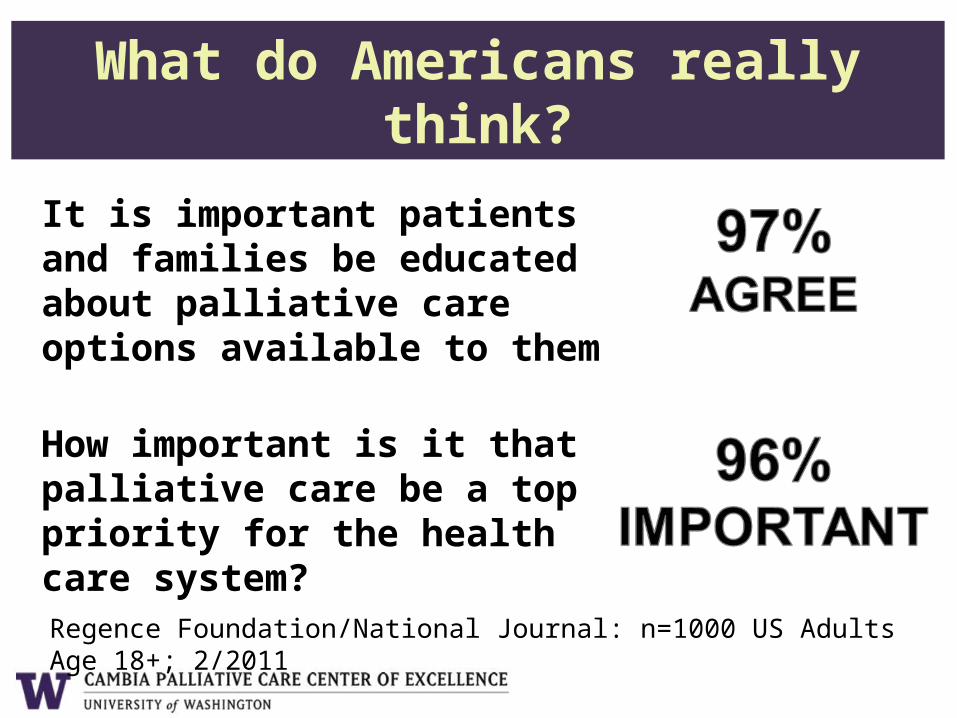
What do Americans really think?
It is important patients and families be educated about palliative care options available to them
How important is it that palliative care be a top priority for the health care system?
Regence Foundation/National Journal: n=1000 US Adults Age 18+; 2/2011

Provision of Palliative Care
• Primary palliative care– Care provided by all clinicians caring
for patients with serious illness
• Specialty palliative care– Care provided by palliative care
specialists

Temel, N Engl J Med, 2010; 363:763

Early PC Improves Quality of Life
38 v 16%. p=0.01
17 v 4%. p=0.04
Temel, NEJM, 2010;
363:763
p=0.04

…Reduces Symptoms
p=0.01
p=0.04
Temel, NEJM, 2010363:763
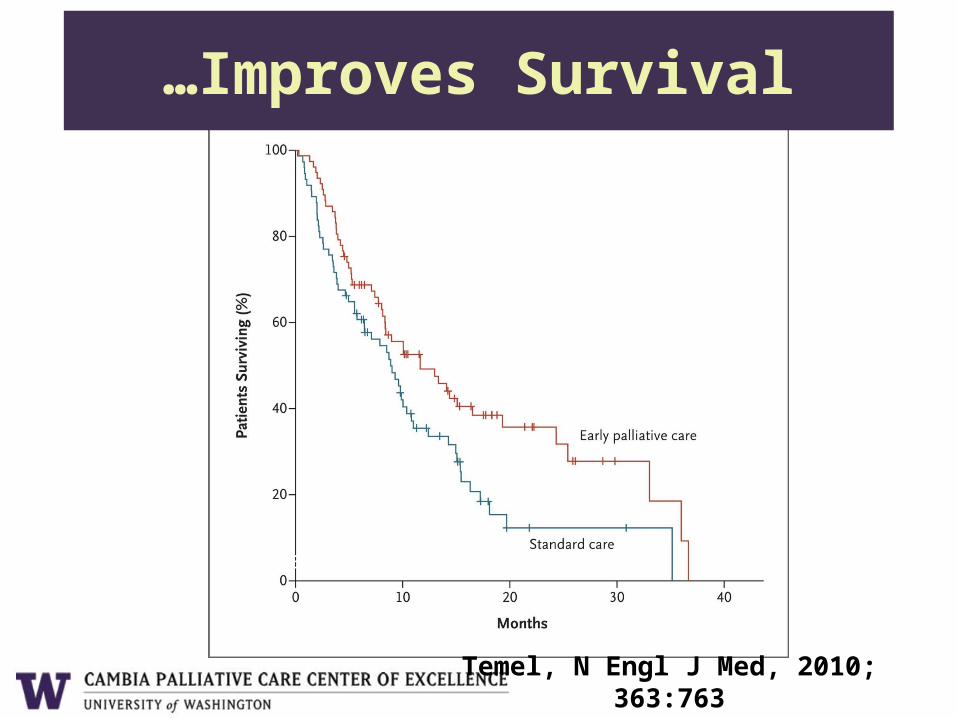
…Improves Survival
Temel, N Engl J Med, 2010; 363:763
Standard care 8.9 months
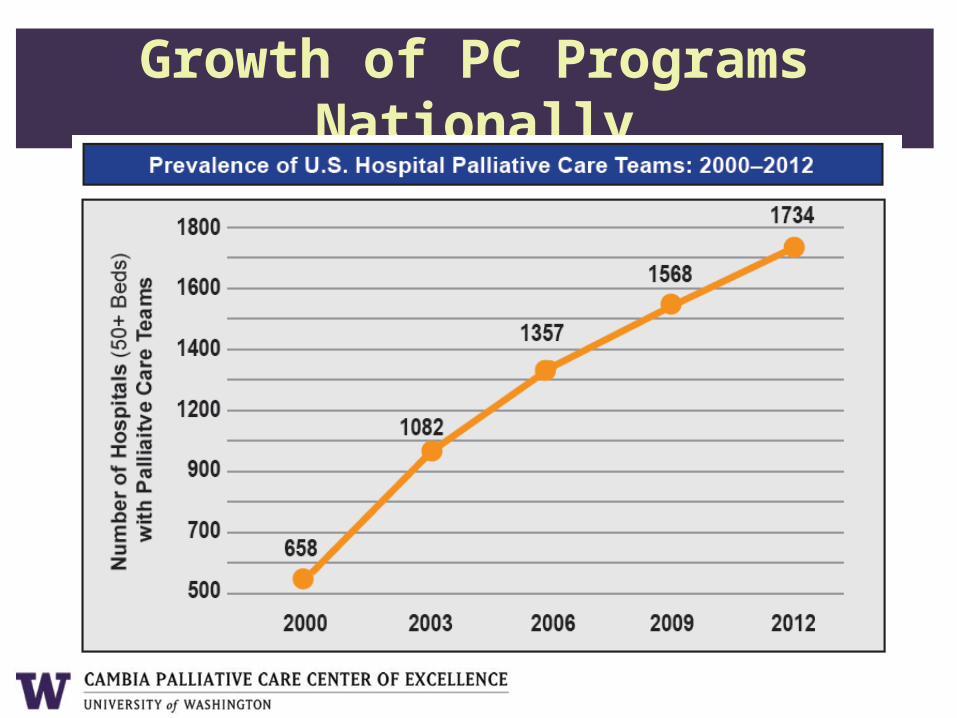
Growth of PC Programs Nationally

Outline: Four Questions
• What is palliative care?
• What are advance directives and advance care planning?
• How can we improve communication about palliative care?
• What can you do?
Who should bring up a discussion about palliative and end-of-life care?
• If you ask patients:
–Doctors should bring it up
• If you ask doctors:
–Patients should bring it up

What can people do to ensure they receive the care they want?
• Advance Directives– Living will
– Durable Power of Attorney for Health Care
– Physician Order for Life-sustaining Treatments (POLST)
• Advance Care Planning– Communication with family and doctors
about goals, values, and preferences

Reasons Advances Directives Might Fail
• Difficulty predicting treatment decisions that will need to be made
• Predicting future preferences limited by– Adaptation to disability– Changes in medical, emotional, social
context
• Patients often want family circumstances and preferences considered

Randomized Trial of Advance Care Planning Among 309 Elderly
• Hospitalized patients age >80 randomized to ACP by trained facilitator vs. usual care
• 81% received ACP; 56% completed AD– Facilitator used “Respecting Patient Choices”– ACP in collaboration with physician– Families present for 72%– Sessions took median 60 minutes
Detering, Br Med J, 2010; 340:c1345

Randomized Trial of Advance Care Planning Among 309 Elderly
Outcome (%) ACP Control p value
Death in ICU 0 14 0.03PTSD in family 0 14 0.03Depression in family 0 30 0.002Anxiety in family 0 19 0.02Satisfied with death 80 68 0.02Satisfied with care 93 65
0.001Detering, Br Med J, 2010; 340:c1345

Why advance directives failed and advance care planning succeeds
• Advance directives focused on document– Static piece of paper difficult to adapt to
real-life situation– Often used without discussing
goals/values• ACP offers discussion of contextual
goals and values – Prepare patient and family to address
actual situation

Outline: Four Questions
• What is palliative care?
• What are advance directives and advance care planning?
• How can we improve communication about palliative care?
• What can you do?

Physician Skill at End-of-life Care
• To identify domains and specific components of physician skill at end-of-life care– Patients with COPD, cancer, or AIDS
(n=79)
– Families who lost a loved one (n=20)
– Physicians, nurses, social workers (n=38)
Curtis, J Gen Intern Med, 2000;16:41

Conceptual Model of the Domains of Physician Skill
Patient-Centered System
•Accessibility & continuity
•Team coordination
Cognitive
•Competence
•Pain and symptom
management
Communication Skills
•Communication with patients
•Patient education
•Inclusion of the family
Affective•Emotional
support•Personalize
care congratulate
Patient-Centered
Values
•Attention to patient values
•Respect & humility
•Support of patient
decision making
Curtis, J Gen Intern Med, 2000; 16:41


Communication With Patients: Competencies
• Listens to patients
• Encourages questions from the patient
• Talks with patients in an honest and straightforward way
• Gives bad news in a sensitive way
• Willing to talk about dying
• Sensitive to when patients are ready to talk about death
Curtis, J Gen Intern Med, 2000;16:41

Back, Arch Intern Med 2007: 167;453
• Before-after study of a 4 day residential workshop for oncology fellows
• 115 fellows from 62 institutions• Evaluated on SP stations and acquired
– 5.4 “delivering bad news” skills
– 4.4 “transition to palliative care” skills
• Used word cancer when giving diagnosis– Before: 16%; After: 54%

Oncotalk Results: Bad News
Back, Arch Intern Med 2007: 167;453
• 5 year RCT funded by NINR• Interdisciplinary: Internal medicine
residents and NP students• Two sites: UW and MUSC• Eight half-day sessions
– Interactive seminar presentations– Communication skills practice
Curtis, JAMA, 2013; 310:2271

Resident and Nurse Practitioner Acquisition of Communication Skills
p<0.003 for all
Percent Completed
Residents: n=128NP: n=17 Bays, J Palliat Med, 2013; epub

Patient and Family Outcomes
Curtis, JAMA, 2013; 310:2271

Post hoc Patient Subgroup Analyses: QOC Score
Outpatient Poor Health Status
Curtis, JAMA, 2013; 310:2271

Conclusions of ICCS
• Intervention improved trainee skills and self-assessment
• No improvement in patient ratings– Untrained or unprompted patients and
families may not be sensitive raters– Care provided by many clinicians
• Slight increase in PHQ symptoms– Increased sense of sadness?– Effect more prominent for R1s
Curtis, JAMA, 2013; 310:2271

Outline: Four Questions
• What is palliative care?
• What are advance directives and advance care planning?
• How can we improve communication about palliative care?
• What can you do?

What documents are available?
• Living will• Durable Power of Attorney for
Healthcare• POLST form
– Physician order for life-sustaining treatment

What are advance directives good for?
• As a tool for raising the discussion
• Good for some specific situations:– If there is a specific treatment you
know you don’t want
– If you don’t want your legal next of kin to be making decisions for you
• Advance directives can ease the burden on your family

www.theconversationproject.org

Why have a Durable Power of Attorney for Health Care?
Who decides if you can’t?1.Court-appointed guardian2.Durable power of attorney for healthcare3.Legal spouse4.Adult children*5.Parents*6.Siblings*
*By consensus
What is a POLST form?
• Physician order for life-sustaining treatments
• Applies in all settings– Home, skilled nursing facility, hospital
• Important if you know you don’t want life-sustaining treatments


Preparing for a Discussion About End-of-life Care with Your Doctor
• Advance preparations– Who should be there?– What do you want to know?– Bring in your documents
• Think about the things you might want– Specific treatments you don’t want– Aspects of health important to you:
independence, ability to communicate– Consider adaptation

Having a Discussion About End-of-life Care with Your Doctor
• If you don’t understand something, ask your doctor to repeat it– Ask for plain language
– Ask the doctor to slow down
• Ask if you can repeat what the doctor has said in your own words
• Feel free to ask your doctor’s opinion and recommendation

What To Discuss?• Your personal goals for healthcare• Your preferences for life support and CPR
– No life support or CPR at all– Life support for short-term reversible situation– Long-term life support without chance of coming
off
• Situations that you would not want life support– Unable to live independently– Unable to communicate with loved ones– Prolonged or indefinite life support in hospital

Focus on Goals before Treatments
• What are the goals of care?– Living independently– Having a good quality of life– Being able to communicate with
loved ones
• Goals more important than specific treatments– ICU treatment– Cardiopulmonary resuscitation

Finishing a Discussion About End-of-life Care
• Take a minute to think if you have any questions
• Summarize discussion in your own words
• Ask if you can meet to discuss this again

Understanding the Discomfort
• Discomfort discussing dying is universal– Patient and family fears– Clinician fears and concerns of
inadequacy
• Recognizing the discomfort can help us work through it– Consider talking about the discomfort
with the doctor

Cambia Palliative Care Center of Excellence at UW
Mission:•Improve palliative care received by patients with serious illness and their families and provide support to clinicians•Develop new knowledge and educational and clinical resources to improve palliative care regionally as well as nationally and globally
http://www.uwpalliativecarecenter.com
http://www.uwpalliativecarecenter.com

How can you get involved?
• Interested in palliative care– Join as a PCCE Member– Help develop and use resources
• Care for patients with serious illness– Education in palliative care– Resources for patients/families
• Community involvement: – Community Advisory Board– Palliative Care Advancement Council
http://www.uwpalliativecarecenter.com

Summary
• Palliative care gaining momentum and communication is a central piece
• Current quality of communication is often poor, but improving
• Interventions for clinicians can clearly improve communication
• Steps you can take– Talk with your doctor and family– Complete advance directives and discuss
• Cambia Palliative Care Center of Excellence
http://www.uwpalliativecarecenter.com