pain dr akhavan akbari fellowship of pain ardebil university of medical science
TRANSCRIPT

PAIN
Dr Akhavan akbari
Fellowship of pain
Ardebil university of medical science

AIMS
Detail the development of pain theories
Highlight current thinking
Describe current methods of treatment

Acute PainAssociated with trauma, procedures etc.
Meaningful signal to inhibit more harm
Adrenalin release often co-occurs
Anxiety goes after diagnosis and treatment (tx)
Tx typically medicines, activity, tractions
Recovery time usually short

Chronic PainVarious opinions on time-lag
8 weeks (Jensen, 2004)6 months (Hardin, 2004)
Essentially, sig. > expected recovery time
Often not related to tissue damage
Medical tx unsuccessful
Anxiety does not decrease

Important? LBP most common cause of absenteeism & disability
in Europe (van Tulder et al, 1998)
Lifetime prevalence LBP: 70% (Andersson et al, 1991)
1.7% GDP - Holland (van Tulder et al, 1998)
5-25% children report pain – headaches, abdominal & limb pain (Campo et al, 2002)
~ 25% kids attending for JRA report mid-high levels of pain (Schanberg et al, 1997)

Chronic Pain Syndrome Common, understandable pattern of behaviour seen
in those with on-going pain
Continual seeking of medical help without success
Acute pain treatments seem to worsen matters – eg bed rest leads to muscle atrophy
Despair, hopelessness, dependency, clinical depression, worthlessness, anger, social withdrawal

Early Theories Pain as a sensation
Stimulus-response theory
Von Frey (1895) – specificity theory
Specific receptors for specific sensations
PAIN
Pain
Warmth
Touch

Biomedical View
Reflects approach to sensory systems
Led to similar research to identify:
Receptive organs / cells
Pathways that conduct sensory info.
Part of brain that processed pain info.

Biomedical View - Assumptions
Tissue damage causes pain
Psychological states are outcomes of pain
Pain experience is an automatic response
Pain is either organic or psychogenic

Pain Receptors Attempt to explain variability across skin
Led to id. of polymodal nociceptors / free nerve
endings (in skin surface, around blood vessels etc.) for:
Pain
Touch
Warmth
Relationship between pain & FNE unclear
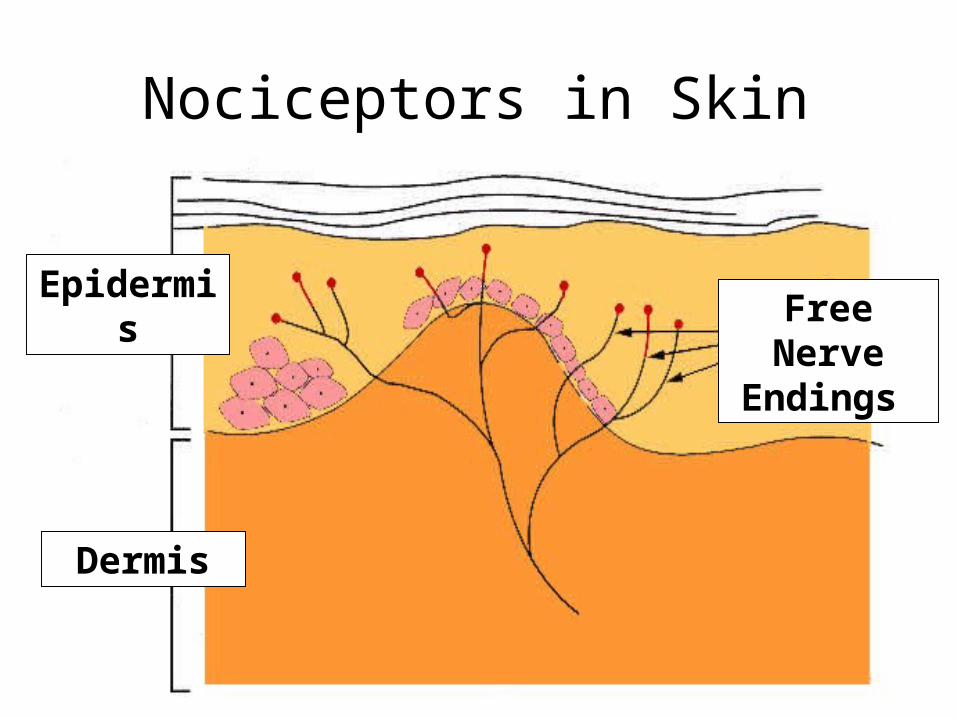
Nociceptors in Skin
Epidermis
Dermis
Free Nerve Endings

Pain PathwaysLots of effort to id neural pathways
Found distinct categories of nerve fibres
A δ : mylinated, carry rapidly sharp pains (20-30 ms-1)
C : unmylinated, carry slowly burning pain (0.5-2 ms-1)
Hence, short sharp, then delayed slow pain

Associated Area of Brain
Fibres pass signals up spinal cord as electrical impulses then onto the thalamus
Thalamus relays messages to cortex
Proved difficult to id. specific area of the cortex that produce pain

Summary
Evidence for:
Pain receptors
Pain pathways
Associated areas of the brain (?)
Consequently, unsurprising that surgery & medications are effective in many cases

Problems for the Biomedical View
Similar tissue damage – dissimilar pain (Beecher, 1956)
Medical tx not always helpful
Disease severity explains only 1 – 10% of
variance (Ilowite, 1992)
Phantom limb pain: up to 60% have pain 7
years post-amputation (Krebs, 1984)
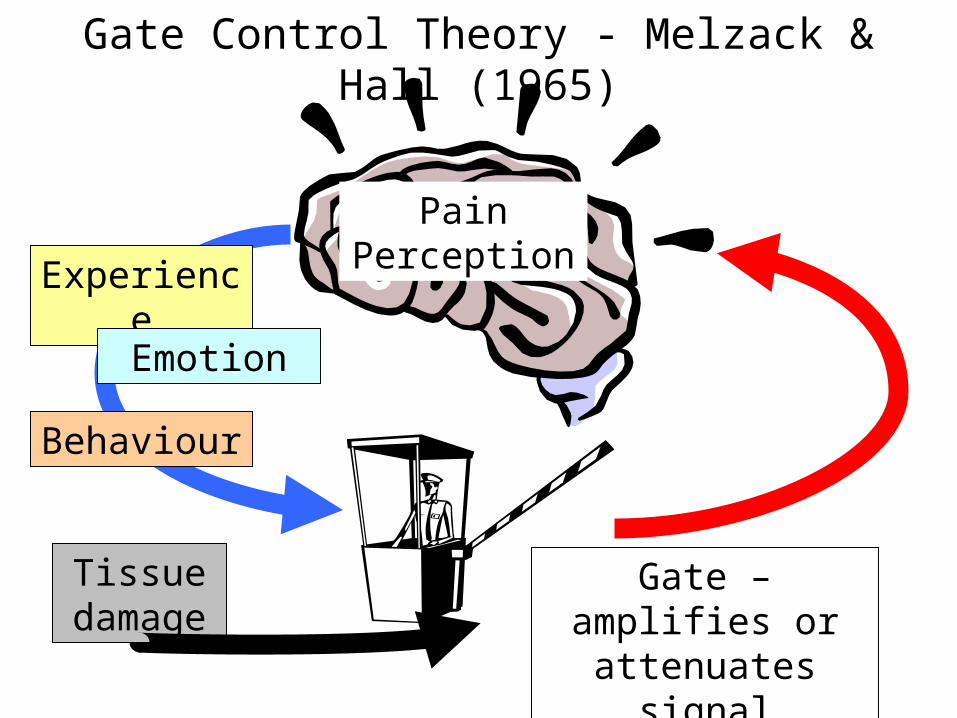
Gate Control Theory - Melzack & Hall (1965)
Experience
Behaviour
Tissue damage
Gate – amplifies or attenuates signal
Pain Perception
Emotion

Opening & Closing the GateFactor Opens Closes
Physical injuryagitation
medication
Emotional anxietystress
frustrationdepression
tension
relaxationoptimismhappiness
Behavioural
(Cognitive)
ruminationboredom
enjoyable activitiescomplex tasks
distractionsocial interaction

Gate Control v Biomedical Theory
Pain as perception not sensation (active)
Multiple factors influence pain perception
Move away from mind-body dualism
Tries integrating biological & psychological views
Variability in people not inherent problem

Problems for Gate Control Theory
Evidence for propsed moderators, but no
physical evidence of gate
Still organic basis for pain (phantom limb?)
Not truly integrative re: psyche & soma
Still improvement on stimulus-response paradigm

Subsequent Pain Theories Reflect trends in general psychology
Fordyce (1976) - pain as behaviour
Reinforcement contingencies
+ve reinforcement (e.g. attention / affection for pain
behaviours)
-ve reinforcement (e.g. avoid unpleasant events
such as work, school)
Recently, growth in cognitive behaviour models
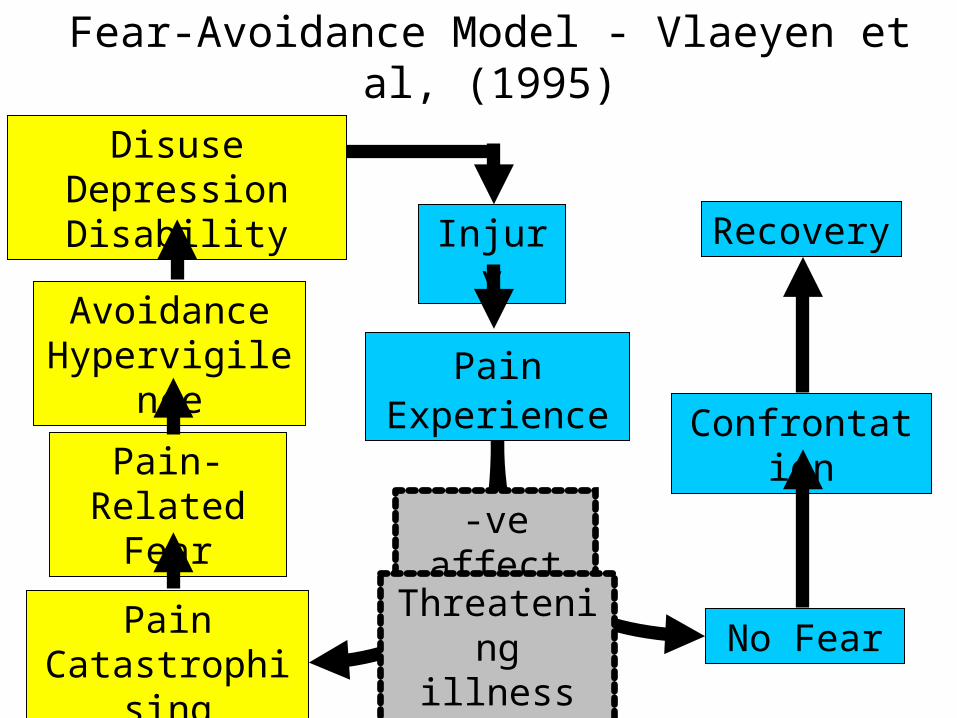
Fear-Avoidance Model - Vlaeyen et al, (1995)
Injury
Pain Experience
Pain Catastrophising
No Fear
Confrontation
Recovery
Pain-Related Fear
Avoidance Hypervigilence
Disuse Depression Disability
-ve affect
Threatening illness info

Fear-Avoidance Theory(-ve) appraisals (catastrophising) → fear of pain
(illness cognitions) & re-injury
Fear of pain → avoidance of potentially painful events (illness behaviour)
Little opportunity to disconfirm beliefs
Avoidance → disuse syndrome & ↑ p (mood problems)
Disuse leads to ↑ p (painful experience)

Treatments Mirror pain theories
Medical (especially acute pain)
Non-anti-inflammatory non-steroid (paracetamol)
Anti-inflammatory non-steroids (eg ibprofen)
Opioids (eg morphine)
Psychological
Behavioural initially
Mostly cognitive behavioural now

CBT for Chronic PainEducation: offering another possible
explanation for individual situation
Meaning: linking illness cognitions & behaviour
Individually designed graded exposure to dangerous situations
Restructruring of illness cognitions & changing illness behaviour

Vlaeyen et al 2001…Compared:
CBT in-vivo graded exposure (Treatment A)
Graded Activity (Treatment B)
Subjects
Chronic pain for > 5 years
Substantial fear of movement / re-injury
Spent most of their time lying down
Total N = 4

TreatmentsCBT (Treatment A)
Pain as common, manageable experience
Explanation of fear-avoidance model
Hierarchy of fearful situations
Practice outside therapy
Graded Activity (Treatment B)
Baseline activity measured
Individual regime designed & implemented
High fear situations excluded

MeasuresPain catastrophising
e.g. When I am in pain I wonder whether something serious might happen
Fear of movement**
e.g. If I exercise I might be in danger of re-injuring myself
Pain disability**
e.g. I only walk short distances because of my back pain
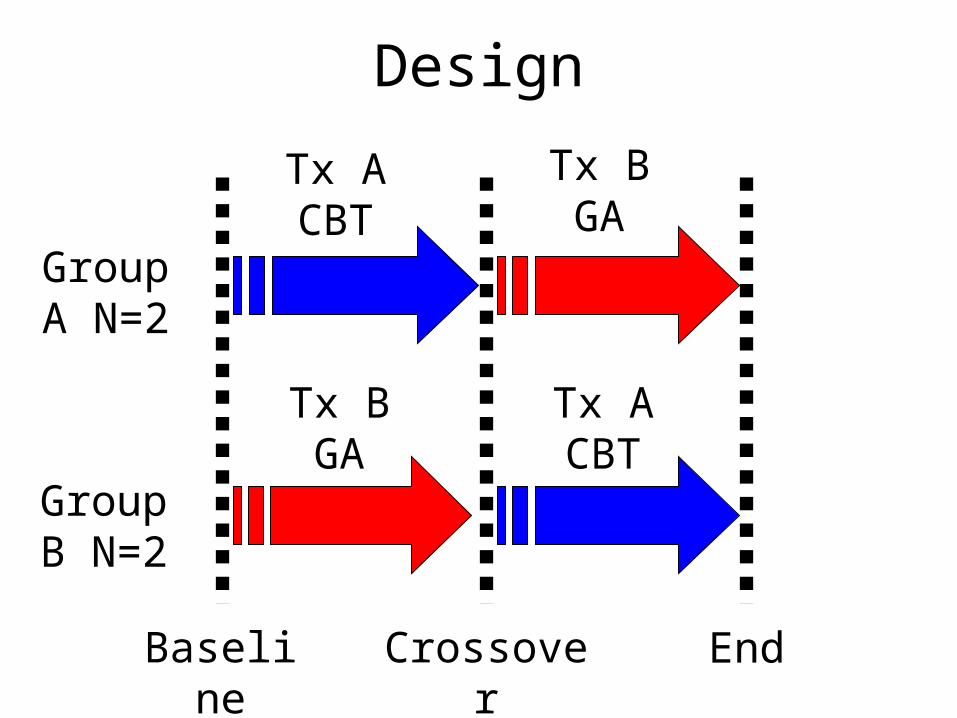
Design
Baseline
Tx B GA
Tx B GA
Tx A CBT
Group B N=2
Group A N=2
Tx A CBT
Crossover End

0
20
40
60
Base Start CBT Start GA End
Subject 1
Subject 4
Figure 1. Fear of movement: CBT then graded activity

0
20
40
60
Base Start GA Start CBT End
Subject 2
Subject 3
Figure 2. Fear of movement: graded activity then CBT

0
5
10
15
20
25
Base StartCBT
StartGA
End
Subject 1
Subject 4
Figure 3. Self-report disability: CBT then graded activity

0
5
10
15
20
25
Base StartGA
StartCBT
End
Subject 2
Subject 3
Figure 4. Self-report disability: graded activity then CBT

Conclusions
Pain-related fear reduced by CBT not GA
Exposure leads to disconfirmation of pain-related cognitions
This leads to less self-report disability
Chronic pain patients should be screened for pain-related fear

Issues
Small number of subjects
Individual variation in effectiveness
High fear activities excluded in graded exposure
No assessment of pain perception

SummaryAcute & chronic pain are different
Chronic pain impacts on society & individuals
Theories of pain have changed over time
Psychological models reflect general trends
Treatment approaches reflect theories
CBT is the current psych treatment of choice

The End