p23. extension of previous fusions to the sacro-pelvis vs. primary spino-pelvic fusions in the...
TRANSCRIPT
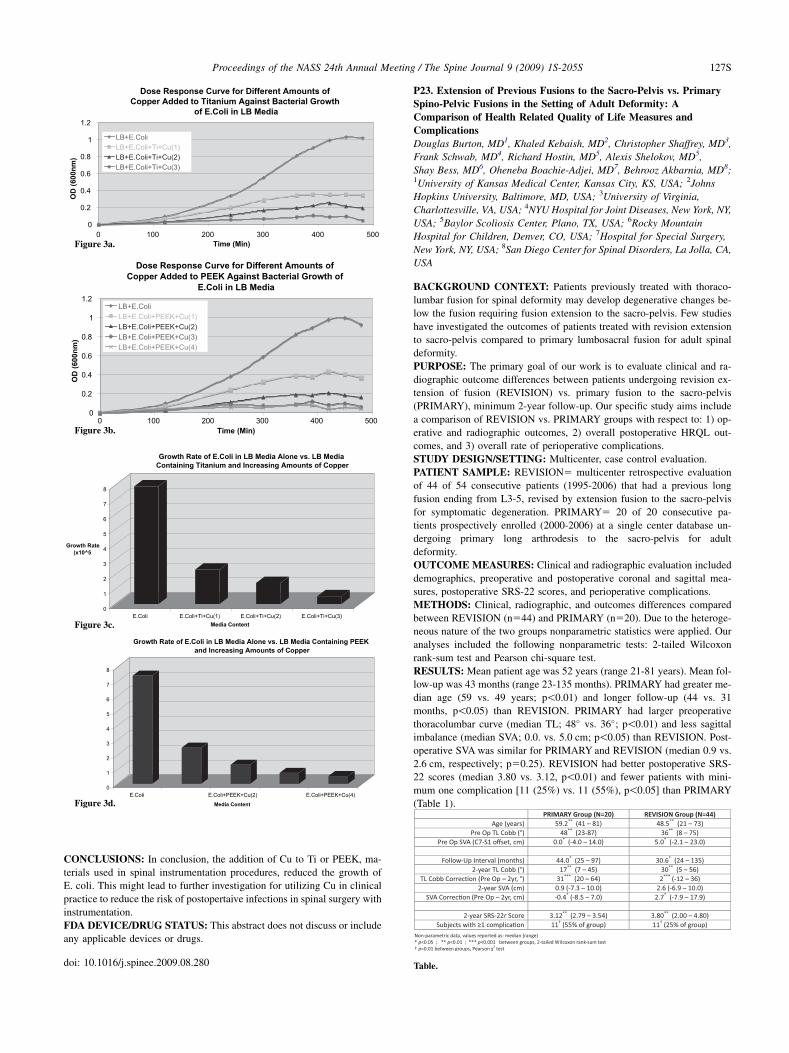
CONCLUSIONS: In conclusion, the addition of Cu to Ti or PEEK, ma-
terials used in spinal instrumentation procedures, reduced the growth of
E. coli. This might lead to further investigation for utilizing Cu in clinical
practice to reduce the risk of postopertaive infections in spinal surgery with
instrumentation.
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include
any applicable devices or drugs.
doi: 10.1016/j.spinee.2009.08.280
P23. Extension of Previous Fusions to the Sacro-Pelvis vs. Primary
Spino-Pelvic Fusions in the Setting of Adult Deformity: A
Comparison of Health Related Quality of Life Measures and
Complications
Douglas Burton, MD1, Khaled Kebaish, MD2, Christopher Shaffrey, MD3,
Frank Schwab, MD4, Richard Hostin, MD5, Alexis Shelokov, MD5,
Shay Bess, MD6, Oheneba Boachie-Adjei, MD7, Behrooz Akbarnia, MD8;1University of Kansas Medical Center, Kansas City, KS, USA; 2Johns
Hopkins University, Baltimore, MD, USA; 3University of Virginia,
Charlottesville, VA, USA; 4NYU Hospital for Joint Diseases, New York, NY,
USA; 5Baylor Scoliosis Center, Plano, TX, USA; 6Rocky Mountain
Hospital for Children, Denver, CO, USA; 7Hospital for Special Surgery,
New York, NY, USA; 8San Diego Center for Spinal Disorders, La Jolla, CA,
USA
BACKGROUND CONTEXT: Patients previously treated with thoraco-
lumbar fusion for spinal deformity may develop degenerative changes be-
low the fusion requiring fusion extension to the sacro-pelvis. Few studies
have investigated the outcomes of patients treated with revision extension
to sacro-pelvis compared to primary lumbosacral fusion for adult spinal
deformity.
PURPOSE: The primary goal of our work is to evaluate clinical and ra-
diographic outcome differences between patients undergoing revision ex-
tension of fusion (REVISION) vs. primary fusion to the sacro-pelvis
(PRIMARY), minimum 2-year follow-up. Our specific study aims include
a comparison of REVISION vs. PRIMARY groups with respect to: 1) op-
erative and radiographic outcomes, 2) overall postoperative HRQL out-
comes, and 3) overall rate of perioperative complications.
STUDY DESIGN/SETTING: Multicenter, case control evaluation.
PATIENT SAMPLE: REVISION5 multicenter retrospective evaluation
of 44 of 54 consecutive patients (1995-2006) that had a previous long
fusion ending from L3-5, revised by extension fusion to the sacro-pelvis
for symptomatic degeneration. PRIMARY5 20 of 20 consecutive pa-
tients prospectively enrolled (2000-2006) at a single center database un-
dergoing primary long arthrodesis to the sacro-pelvis for adult
deformity.
OUTCOME MEASURES: Clinical and radiographic evaluation included
demographics, preoperative and postoperative coronal and sagittal mea-
sures, postoperative SRS-22 scores, and perioperative complications.
METHODS: Clinical, radiographic, and outcomes differences compared
between REVISION (n544) and PRIMARY (n520). Due to the heteroge-
neous nature of the two groups nonparametric statistics were applied. Our
analyses included the following nonparametric tests: 2-tailed Wilcoxon
rank-sum test and Pearson chi-square test.
RESULTS: Mean patient age was 52 years (range 21-81 years). Mean fol-
low-up was 43 months (range 23-135 months). PRIMARY had greater me-
dian age (59 vs. 49 years; p!0.01) and longer follow-up (44 vs. 31
months, p!0.05) than REVISION. PRIMARY had larger preoperative
thoracolumbar curve (median TL; 48� vs. 36�; p!0.01) and less sagittal
imbalance (median SVA; 0.0. vs. 5.0 cm; p!0.05) than REVISION. Post-
operative SVA was similar for PRIMARY and REVISION (median 0.9 vs.
2.6 cm, respectively; p50.25). REVISION had better postoperative SRS-
22 scores (median 3.80 vs. 3.12, p!0.01) and fewer patients with mini-
mum one complication [11 (25%) vs. 11 (55%), p!0.05] than PRIMARY
(Table 1).
Dose Response Curve for Different Amounts of
Copper Added to Titanium Against Bacterial Growth
of E.Coli in LB Media
0
0.2
0.4
0.6
0.8
1
1.2
0 100 200 300 400 500Time (Min)
OD
(600n
m)
LB+E.ColiLB+E.Coli+Ti+Cu(1)LB+E.Coli+Ti+Cu(2)LB+E.Coli+Ti+Cu(3)
Dose Response Curve for Different Amounts of
Copper Added to PEEK Against Bacterial Growth of
E.Coli in LB Media
0
0.2
0.4
0.6
0.8
1
1.2
0 100 200 300 400 500Time (Min)
OD
(60
0n
m)
LB+E.ColiLB+E.Coli+PEEK+Cu(1)LB+E.Coli+PEEK+Cu(2)LB+E.Coli+PEEK+Cu(3)LB+E.Coli+PEEK+Cu(4)
0
1
2
3
4
5
6
7
8
E.Coli E.Coli+PEEK+Cu(2) E.Coli+PEEK+Cu(4)
Media Content
Growth Rate of E.Coli in LB Media Alone vs. LB Media Containing PEEK
and Increasing Amounts of Copper
0
1
2
3
4
5
6
7
8
Growth Rate
(x10^5
E.Coli E.Coli+Ti+Cu(1) E.Coli+Ti+Cu(2) E.Coli+Ti+Cu(3)Media Content
Growth Rate of E.Coli in LB Media Alone vs. LB Media
Containing Titanium and Increasing Amounts of Copper
Figure 3a.
Figure 3b.
Figure 3c.
Figure 3d.
Table.
127SProceedings of the NASS 24th Annual Meeting / The Spine Journal 9 (2009) 1S-205S

CONCLUSIONS: Significant differences were demonstrated between
patients undergoing primary vs. revision extension to the sacro-pelvis.
PRIMARY were older, and had larger TL curves, whereas REVISION
had greater sagittal imbalance. While PRIMARY had more complica-
tions, multiple factors could account for this other than surgery type,
including differences in age or number of levels fused. The retrospec-
tive nature of the study may have also underrepresented minor compli-
cations. Although the groups were heterogeneous, radiographic, SRS-22
and complications analysis indicate clinical outcomes of salvage proce-
dures where a prior spinal fusion procedure is extended to the sacro-
pelvis compare favorably to primary sacro-pelvic fusion for adult
spinal deformity.
FDA DEVICE/DRUG STATUS: This abstract does not discuss or include
any applicable devices or drugs.
doi: 10.1016/j.spinee.2009.08.281
P24. Posterior Dynamic Instrumentation (Isobar TTL) for
Degenerative Disc Disease of Lumbar Spine
Antonio Castellvi, MD, Deborah Clabeaux, RN, William Hudson, MD;
Florida Orthopaedic Institute, Tampa, FL, USA
BACKGROUND CONTEXT: Posterior dynamic stabilization is emerg-
ing as a method to stabilize a pathological spine segment while avoiding
a fusion. The traditional treatments of degenerative disc disease have been
decompression and or fusion. This sets the stage for eventual failure of the
adjacent segment by increasing the loads at the adjacent disc. Stabilization
with a motion preserving pedicle based dynamic rod (Isobar TTL, Scient’x
USA) can control motion at the index segment and share the loads applied
to the entire lumbar spine.
PURPOSE: The Isobar TTL is intended to stabilize the spine, maintain
motion characteristics, and decrease the size of the neutral zone in the af-
fected spinal segments while providing good functional and radiographic
outcomes.
STUDY DESIGN/SETTING: This is an IRB approved, prospective study
of consecutive non-randomized patients. Indications include degenerative
disc disease, spinal stenosis, degenerative grade 1 spondylolisthesis and
post-laminectomy syndrome.
PATIENT SAMPLE: We present a cohort of 35 patients; 16 male, 19 fe-
male with a mean age of 61 years. These patients present with single seg-
ment lumbar degenerative disc disease treated with decompression and
posterior pedicle based dynamic rod instrumentation (Isobar TTL) without
a fusion with a minimum follow up of 2 years to 5 years.
OUTCOME MEASURES: Functional clinical outcomes were measured
with a 100 point Visual Analog Scale (VAS), Oswestry Disability Index
(ODI) and SF-36 questionnaire. Radiographic measurements of disc
height, intervertebral angle, lumbar lordosis and motion were performed
with flexion, extension and neutral x-rays. MRI scans were also performed
at one year. Complications and screw loosening were assessed.
METHODS: Decompression and implantation of the Dynamic TTL Rod
was completed in 35 patients. Patients were scheduled for follow-up at 6
weeks, 3,6,12 months, and annually to 10 years.
RESULTS: Follow-up data ranges from 24 to 60 months. Radiographic
analysis shows all devices to be intact and functioning. No device failure
or screw breakage is identified. Flexion and extension radiographs showed
motion at the index level. No increase in adjacent level ROM or angular
deformity. Disc height was preserved. Radiographic screw loosening pre-
sented at an incidence of 2.8% (1/35); which has not required surgical re-
vision to date. Spontaneous fusion was identified. Functional outcomes
were assessed. Evidence showed significant improvement in VAS of 25
points and ODI of 21 points; SF 36 showed statistically significant im-
provement in physical and mental component at most recent follow up.
Post operative complications include two incidences of adjacent level her-
niated nucleus pulposus (HNP) which required a surgical discectomy. Two
patients developed adjacent segment degenerative disease, one required re-
vision surgery.
CONCLUSIONS: The posterior dynamic instrumentation is a new inno-
vative surgical approach in the treatment of lumbar degenerative disc dis-
ease. Our preliminary results of functional and radiographic outcomes up
to five years are satisfactory and long term follow up will be needed to
fully assess continual functional improvements and decrease in the overall
incidence of adjacent level disc degeneration.
FDA DEVICE/DRUG STATUS: Isobar TTL: Not approved for this
indication.
doi: 10.1016/j.spinee.2009.08.282
P25. The Impact of Reciprocal Regional Alignment Changes Distant
from the Site of Spinal Osteotomies Affects Post-Operative Spinal
Balance
Virginie Lafage, PhD1, Frank Schwab, MD1, Oheneba Boachie-Adjei, MD2,
Jean-Pierre Farcy, MD1, Alexis Shelokov, MD3, Richard Hostin, MD3,
Robert Hart, MD4, Behrooz Akbarnia, MD5, Michael O’Brien, MD6,
Douglas Burton, MD7, Christopher Shaffrey, MD8, Ashish Patel, MD1;1NYU Hospital for Joint Diseases, New York, NY, USA; 2Hospital for
Special Surgery, New York, NY, USA; 3Baylor Scoliosis Center, Plano, TX,
USA; 4Oregon Health Sciences University, Portland, OR, USA; 5San Diego
Center for Spinal Disorders, La Jolla, CA, USA; 6Miami Children’s
Hospital, Miami, FL, USA; 7University of Kansas Medical Center, Kansas
City, KS, USA; 8University of Virginia, Charlottesville, VA, USA
BACKGROUND CONTEXT: Treatment of complex spinal deformity in
adult patients requires an understanding of the effect of regional changes
on global balance. While the regional impact of an osteotomy can be
planned, the impact on distant segments of the spine remains poorly
understood.
PURPOSE: The objective of this study is to analyze reciprocal regional
corrective changes in the unfused segments of the spine away from the site
of osteotomies as it relates to the final radiographic outcome.
STUDY DESIGN/SETTING: A retrospective, multicenter (n58) radio-
graphic review of consecutive patients treated with a pedicle subtraction
osteotomy (PSO) in the thoracolumbar spine.
PATIENT SAMPLE: 134 adult patients (24 M, 110F) with a mean age of
54612 years.
OUTCOME MEASURES: Radiographic pre-post outcome analysis.
METHODS: 29 subjects underwent thoracic resection procedures (’’Tho-
racic group’’), and 105 underwent lumbar resection procedures (’’Lumbar
group’’). Resection levels ranged from T2 to L4 (Table). Radiographic
analysis included pre and postoperative assessment of Thoracic Kyphosis,
Lumbar Lordosis, SVA, Pelvic tilt, Pelvic incidence. Paired independent t-
test analysis (SPSS) was computed to evaluate the changes in radiographic
parameters.
RESULTS: In the ‘‘Thoracic group’’, pre-op thoracic Kyphosis of 58�
was corrected to 38� (p!0.001) and localized correction measured 11�.For the un-fused lumbar segment (12 patients), spontaneous Lordosis
changed from 70� to 62� (p!0.05). Pre-op SVA improved from 2.4 cm
to -1 cm (p50.006) and pelvic tilt improved from 19deg pre-op to
13deg (p!0.001) In the ‘‘Lumbar group’’, the average correction at the
osteotomy was 23�. Lumbar Lordosis increased from 20� to 49�
(p!0.001). For the un-fused thoracic segment (34 patients), Kyphosis in-
creased from 22� to 35 post op (p50.002). Pre op SVA improved from
14 cm to 4 cm post-op (p!0.001) and pelvic tilt improved from 33� to
25� (p!0.001).
CONCLUSIONS: In an attempt to correct spinal imbalance several pa-
rameters play important roles in pre-operative planning. If reciprocal
changes related to regional deformity correction can be anticipated, then
better post-operative alignment can be achieved. Furthermore, limiting re-
section to the site of maximum deformity may address the regional mala-
lignment and result in reciprocal and spontaneous changes in un-fused
segments leading to improved restoration of overall spinal balance. This
may eliminate the need to perform longer fusions of the spine. The data
128S Proceedings of the NASS 24th Annual Meeting / The Spine Journal 9 (2009) 1S-205S