p clinical ntal & light induced damage of
TRANSCRIPT

doi: 10.1111/j.1472-8206.2011.00963.x
O R I G I N A L
A R T I C L E
Novel intraocular and systemic absorptiondrug delivery and efficacy ofN-acetylcarnosine lubricant eye dropsor carcinine biologics in pharmaceuticalusage and therapeutic vision care
Mark A. Babizhayeva,b*, Inna P. Khoroshilova-Maslovab,Anne Kasus-Jacobic
aInnovative Vision Products, Inc., 3511 Silverside Road, Suite 105, County of New Castle, DE 19810, USAbMoscow Helmholtz Research Institute for Eye Diseases, 14/19 Sadovaya-Chernogryazskaya, Moscow 103064, RussiacDepartment of Ophthalmology, University of Oklahoma Health Sciences Center, Dean A. McGee Eye Institute,
608 Stanton L. Young Blvd., Oklahoma City, OK 73104, USA
‘‘There is overwhelming evidence that the higher the level
of self-esteem, the more likely one will be to treat others with
respect, kindness, and generosity.’’
Nathaniel Branden
I N T R O D U C T I O N
Eye diseases that occur more often in elderly patients
increase concomitantly as the population ages. The latest
estimates of the World Health Organization (WHO)
Keywords
carcinine and blindness
prevention,
cataract, age-related macu-
lar degeneration and prolif-
erative vitreoretinopathy,
light induced damage of
photoreceptor cells,
N-acetylcarnosine lubricant
eye drops,
vision care and age-related
ophthalmic diseases
Received 30 December 2010;
revised 4 May 2011;
accepted 13 May 2011
*Correspondence and reprints:
A B S T R A C T
The latest estimates of the World Health Organization indicate that there are
161 million visually impaired individuals worldwide, 37 million of whom are blind,
with a yearly increase of 1–2 million. The scientists developed and patented the
lubricant eye drops formulated as 1% N-acetylcarnosine prodrug of L-carnosine
containing a mucoadhesive cellulose-based compound combined with corneal
absorption promoters in an ocular drug delivery system. Carcinine is suitable for
the systemic administration (per oral) for ophthalmic therapeutic indications. The
HPLC analysis was developed to search the pathways of ocular metabolic activities of
1% N-acetylcarnosine and the bioactivation of this drug molecule promoting
transcorneal uptake of L-carnosine in the aqueous humor. A meta-analysis of phase 2
randomized double-blind placebo-controlled clinical trial data was conducted. The
intraocular absorbed L-carnosine demonstrated a number of pharmacological
mechanisms of prevention and reversal of cataracts. Results of systemic absorption
of L-carnosine provide tuberomammillary activation that regulates neuronal func-
tions such as hypothalamic control promoting sensory input in the primary vision
perceptual pathway. The parabulbar, subconjunctival, and intravitreal injection of
carcinine with most of the vehicle removed is not toxic to intraocular structures,
reduces postoperative intraocular inflammation, is a potentially useful tool in the
treatment of proliferative vitreoretinopathy as well as considered as the antiapoptotic
drug for the protection of photoreceptor cells from oxidative light-induced stress. The
discovery of naturally occurring carnosine derivatives introduces N-acetylcarnosine
and carcinine as effective medical treatment for sight-threatening eye disorders.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology 1
Fund
amen
tal &
Cli
nica
l Pha
rmac
olog
y

indicate that there are 161 million visually impaired
individuals worldwide, 37 million of whom are blind,
with a yearly increase of 1–2 million – this means
approximately 0.85% of the world population. Another
135 million show visual impairment [1].
Prevalence of blindness increases with age, mainly
after 50, being higher in rural areas and among women,
probably because of their socioeconomical vulnerability,
as well as the obstacles they face to access health services
[2]. Notwithstanding the progress in surgical interven-
tion that has been made in many countries over the last
few decades, cataract remains the leading cause of visual
impairment in all regions of the world, except in the most
developed countries. Other major causes of visual
impairment are, in order of importance, glaucoma,
age-related macular degeneration, diabetic retinopathy,
and trachoma [1]. Blindness or low vision affects
approximately 1 in 28 Americans older than 40 years
[3]. Based on demographics from the 2000 US Census,
an estimated 937 000 (0.78%) Americans older than
40 years were blind (US definition). An additional
2.4 million Americans (1.98%) had low vision. The
leading cause of blindness among white persons was age-
related macular degeneration (54.4% of the cases), while
among black persons, cataract and glaucoma accounted
for more than 60% of blindness.
Cataract was the leading cause of low vision
(Figure 1), responsible for approximately 50% of bilateral
vision worse than 6/12 (20/40) among white, black,
and Hispanic persons. The number of blind persons in
the United States is projected to increase by 70% to
1.6 million by 2020, with a similar rise projected for low
vision [3]. Home health care is the fastest growing
expense in the Medicare program because of the aging
population, the increasing prevalence of chronic disease
and increasing hospital costs [4]. Over 375 000 people
can suffer permanent visual impairment every year as a
result of surgical complications [5]. This means that
surgical complications, and cataract complications in
general, represent a significant obstacle to the success of
any blindness prevention program. This article discusses
the use of anticataract new type of medicated
N-acetylcarnosine lubricant eye drop patented by Inno-
vative Vision Products, Inc. (New Castle, DE, USA) (IVP),
which is important to the successful implementation of
VISION 2020 [6–19].
Proliferative vitreoretinopathy (PVR) is a scar tissue
formation within the eye. This condition has been called
by many names, including massive periretinal prolifer-
ation (MPP) and massive vitreous retraction (MVR), and
was finally dubbed PVR by the Retina Society Terminol-
ogy Committee. ‘Proliferative’ is given because cells
proliferate, and ‘vitreoretinopathy’ is given because the
Figure 1 Cataract. Slit lamp photograph of cataract in human eye.
The elderly patient complained of a slowly progressive, painless loss
of vision.
Figure 2 Proliferative vitreoretinopathy (PVR). In PVR, scar tissue
forms in sheets on the retina, which contract. This marked
contraction pulls the retina toward the center of the eye and
detaches and distorts the retina severely. PVR can occur both
posteriorly (as shown) and anteriorly with folding of the retina
both anteriorly and circumferentially.
2 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

problems involve the vitreous and retina. PVR (Figure 2)
can be divided into multiple categories based on the
configuration of the retina and the location of the scar
tissue, and this categorization is used by eye care
specialists to describe to one another the severity and
configuration of the retina in PVR. PVR is the most
common complication of a retinal detachment (RD) and
occurs in approximately 8–10% of patients who develop
an RD.
The retina normally lies on a layer of epithelial cells
that, in turn, rest on a bed of blood vessels. Sometimes
the retina becomes partially or completely detached from
its support tissues, which impairs or completely abol-
ishes vision. Successful retinal reattachment can be
achieved surgically in about 90% of cases. However, in
the remaining 10%, the surgery results in contractile
scarring on the surfaces of the retina, preventing
reattachment. This condition is known as PVR, and
blindness or extremely limited vision is an inevitable
consequence. At the time of a retinal detachment and
the formation of a retinal tear, Retinal pigment epithelial
(RPE) cells that are normally under the retina come
through the retinal tear and enter the vitreous cavity.
After the retinal detachment is repaired or not repaired
(if the patient does not seek help), these cells proliferate
on the surface of the retina (and sometimes under the
retina) in sheets, which contract and pull the retina back
off. These sheets can occur in the posterior portion of the
retina, or in any other location of the retina, including in
the far anterior periphery of the retina, causing
redetachment.
The surgery to repair an eye detached from PVR
includes pars plana vitrectomy, membrane peeling where
ophthalmic surgeons use small instruments to peel the
membranes from the surface of the retina, and scleral
buckling. These techniques are combined with fluids
placed in the eye to flatten the retina and reattach it to the
outer wall of the retina followed by laser photocoagula-
tion to connect the retina to the outer layers perma-
nently. Although PVR is a catastrophic complication of
retinal detachment surgery and can cause profound
visual loss, it has gone from being unsuccessfully repaired
in the late 1970s to having a very high success rate in
repairing PVR detachments today.
Current medical therapies are limited to the use of
drugs that act to reduce scar formation by inhibiting
proliferation of the cells that form the scars. However,
these drugs are quickly metabolized within the eye
minimizing their long-term effectiveness. High doses of
these drugs may also be toxic to the retina.
Our PVR researchers have discovered that the forma-
tion and subsequent contractile action of retinal scars is
produced by the movement of retinal pigment epithelial
cells that normally remain stationary. They have there-
fore surmised that if one can prevent movement of scar-
forming cells therapeutically, we can also prevent PVR.
Work has been therefore ongoing within the team to
identify chemical signals called chemoattractants that
stimulate these cells to move. Here, we are presenting the
original experimental data.
In many cases, prodrugs may offer a way to overcome
the poor drug-like properties of a very potent lead and
provide the opportunity to convert a nondevelopable
natural molecule subjected to enzymatic hydrolysis into
a potent patented candidate for clinical use. The
histidine-containing dipeptide L-carnosine (b-alanyl-
L-histidine) and its ophthalmic bioactivating prodrug
N-acetylcarnosine (N-acetyl-b-alanyl-L-histidine) are
part of this group of products [14,20,21]. Carnosine
(b-alanyl-L-histidine) and related compounds are natural
constituents of excitable tissues possessing diverse bio-
logic activities [22,23]. The level of carnosine in tissues is
controlled by a number of enzymes transforming carno-
sine into other carnosine-related compounds, such as
carcinine, N-acetylcarnosine, anserine, or ophidine (by
decarboxylation, acetylation, or methylation, respec-
tively) or its cleavage into the amino acids, histidine
and b-alanine. Hydrolysis is mainly as a result of tissue
carnosinase (EC 3.4.13.3), which is widely distributed
among different tissues [24,25] or serum carnosinase
(EC 3.4.13.20), found in brain and blood plasma of
primates and humans [26,27]. Both carnosine and
N-acetylcarnosine compounds are found primarily in
the heart and skeletal muscles and in the brain. We have
found appreciable levels of L-carnosine in transparent
human lenses, which are markedly depleted in mature
cataracts [28]. The concentration of carnosine in trans-
parent crystalline lenses detected was about 25 lM. At
different stages of cataract development, the level of
carnosine fell, reaching about 5 lM [28]. Carnosine has
been proven to scavenge reactive oxygen species (ROS)
as well as alpha-beta unsaturated aldehydes formed from
peroxidation of cell membrane fatty acids during oxida-
tive stress [29–31]. It can oppose glycation [32,33], and
it can chelate divalent metal ions. The important studies
have produced clinical and experimental evidence of
beneficial effects of N-acetylcarnosine in treating cata-
racts of the eyes, and these and other ophthamological
benefits have been proven [6–14]. Research with
N-acetylcarnosine (NAC) demonstrates that it is effective
N-acetylcarnosine lubricant eye drops and carcinine for vision care 3
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

not only in preventing cataracts but also in treating
them. NAC has been shown to improve vision by
partially reversing the development of the cataract, thus
increasing the transmissivity of the lens to light [8].
Carcinine (b-alanyl histamine) is an imidazole dipeptide
first discovered in the crustacean Carcinus maenas [34]
and has subsequently been found in the hearts of several
mammalian species [35,36]. It has been demonstrated
that carcinine is metabolically related to histamine,
histidine, and carnosine (b-alanyl-L-histidine) and could
be synthesized from histamine and b-alanine [37]. In
addition, previous studies have shown that carcinine
contains an imidazole group with flexible ethylene side
chain known to be important for histamine H3 receptor–
ligand interactions [38–41]. From these findings, it
seems that a certain relationship exists between brain
histamine and carcinine and that carcinine might be a
new histamine H3 receptor antagonist. The results of the
recent study provide direct evidence that carcinine, as a
novel histamine H3 receptor antagonist, plays an
important role in histaminergic neurons activation and
might be useful in the treatment of certain diseases, such
as epilepsy, and locomotor or cognitive deficit [42].
However, only few reports have explored this relation-
ship, and little is known about the pharmacological and
physiologic role of carcinine. In two of those reports,
carcinine was shown to act as a natural antioxidant
[21,43] and to play a role in regulating stress and shock
with a 1000-fold less potent hypotensive effect than
histamine [36,44], suggesting that carcinine might have
therapeutic use. Carcinine is officially registered for
cosmetic and cosmeto-pharmaceutical application in
the USA and Europe by Exsymol SAM since 1997.
Overall, these low-molecular-mass antioxidant pepti-
domimetics (Figure 3a–c) add significantly to the defense
provided by the enzymes superoxide dismutase, catalase,
and glutathione peroxidases [21,43].
One of the obscure aspects of the carnosine physiologic
role is the biologic significance of the enzymatic meta-
bolism of carnosine or its derivatives in tissues. We found
that to change the antioxidant status, tissue enzymes
can modify the NAC prodrug molecule and that deacet-
ylation increases in vivo the resistance of lens tissues and
its cells to oxidative stress.
Poor bioavailability (<1%) of drugs from conventional
eye drops is mainly owing to the various precorneal loss
factors, which include rapid tear turnover, systemic drug
absorption through naso-lachrymal duct, transient res-
idence time of the drug solution in the cul-de-sac, and the
relative impermeability of the drugs to corneal epithelial
membrane. 1% N-acetylcarnosine is a universal bioacti-
vating antioxidant for vision in the developed and
patented drug delivery system lubricant eye drop formu-
lations containing mucoadhesive cellulose-based com-
pound combined with corneal absorption promoters. Its
topical administration delivers pure L-carnosine and
allows its increased intraocular absorption into the
aqueous humor surrounding the lens, enabling signifi-
cant improvements in anticataract drug efficacy and the
minimization of side effect from either local or systemic
drug absorption/bioavailability to the eye, and also
creates optimization effects in the number of ocular
degenerative age-dependent disorders [10]. The formu-
lation was also found to be nonirritant and well tolerable.
The developed system can be a viable alternative to
conventional eye drops for the treatment of various
ocular diseases and is suitable for clinical application.
The developed IVP N-acetylcarnosine prodrug and
codrug lubricating eye drop systems (including principal
regulatory registered eye drops design IVP CTM and
Can-CTM lubricating eye drops) have been marketed
under numerous brand labels (Figure 4). N-acetylcarno-
sine prodrug and codrug ophthalmic formulations
applied topically to the eye, and moreover, its controlled
time released ophthalmic ingredient L-carnosine exerts
antiglycation, bioactivating antioxidant properties in the
lens and cornea as a scavenger of lipid peroxides, singlet
oxygen, and OH· radicals and provides the spatial aspects
of intracellular pH regulation [8,11,15]. The marketed
patented famous brand label Can-CTM of N-acetylcarno-
sine eye drops approved by Innovative Vision Products,
Inc. recently achieved the important milestone on over
500 000 bottles sold.
We have recently designed an innovative Halometer
DG tester that overcomes previous deficiencies [7,45–
47]. IVP patented the original Halometer DG concept
and designed the vision diagnostic device for clinical
implementation as predictor of visual functions in
subjects during various daily activities, such as driving
(Figure 5) [7,45–47].
The purpose of this study is to examine the effects of a
most often recommended to patients a short-term 5- to
6-month treatment with 1% N-acetylcarnosine in oph-
thalmic formulation with a lubricant carboxymethylcel-
lulose on improvement in visual impairment and glare
disability in older adult subjects and older patients with
cataract whose realistic occupations frequently involve
driving activities.
We used a randomized design that was ethical since
N-acetylcarnosine is an accepted and proven therapeutic
4 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

modality of vision care available on the market of
antiaging medicine since 2002 [16–19].
M A T E R I A L S A N D M E T H O D S
Peptide-based compounds have been manufactured
according to cGMP and GLP certified techniques.
Carcinine (Decarboxy carnosineÆ2HCl) was synthesized
by Exsymol S.A.M. (Monaco, Principaute de Monaco)
(Table I) L-Carnosine and N-acetylcarnosine were
synthesized by Hamari Chemicals Ltd, Osaka, Japan
(Table II) per GLP specifications proposed by IVP.
Experimental design: N-acetylcarnosine lubricant
eye drops studies
Studies of transcorneal uptake and systemic absorption of
carnosine from N-acetylcarnosine ocular drug delivery
formulation
Formulations were used in fifty five Grey Chinchilla
rabbits (male) aged 3–4 months weighing 2–3 kg.
(a)
(c)
(b)
Figure 3 Structures of N-acetylcarnosine (a), carnosine (b), and carcinine (c) shown as chemical structures and energy-minimized structures
(space-filling models). (a) N-acetylcarnosine chemical and energy-minimized structures (space-filling model). (b) Carnosine chemical and
energy-minimized structures (space-filling model). (c) Carcinine chemical and energy-minimized structures (space-filling model). Formula
(N-ethyl-5-imidazolyl)b-aminopropionamide chlorhydrate.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 5
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology
Animal experiments conformed to the guidelines of the
ARVO Resolution on the Use of Animals in Research.
Thirty minutes prior to the ocular incision, right eyes of
rabbits were instilled with 80 lL of formulation A (Can-
CTM) containing 1% N-acetylcarnosine (NAC), and the
control right eyes of the separate rabbits were similarly
instilled with their vehicles (placebo) solutions
(Figure 6a). Formulation A was presented in the final
ophthalmic tubes (per volume of 2.5 mL) and in the
moiety of the plastic bottles. Placebo solution contained
the same ingredients without NAC.
Surgical procedure
Topical anesthesia of the rabbit eyes was performed after
25 min of instillation of the formula ophthalmic
solutions with instillations of 4% lidocaine hydrochloride
solution eye drops (three times with 1 drop at 1.5- to
2.0-min intervals). The eye drops of 4% lidocaine
Figure 4 Most popular OTC public and officially registered International brands of N-acetylcarnosine lubricant eye drops worldwide patented
by Dr. Mark A. Babizhayev/IVP, clinically developed in cooperation with alliance Corporate Partners and marketed worldwide through the
number of International Distributors contractual with obligations to IVP. The IVP CTM brand of N-acetylcarnosine eye drops is officially
registered (CE Marked) in all countries of EC, and the appropriate Free Sales Certificate has been granted by the Italian Ministry of Health.
Under the IVP. Global Vision policy, the IVP C. TMBrand of N-acetylcarnosine lubricant eye drops now became officially registered in U.A.E.
(Dubai), Malaysia, and Indonesia. Indonesia comprises 17 508 islands, and with an estimated population of around 237 million people,
it is the world’s fourth most populous country and has the largest Muslim population in the world. Cataract prevalence in adults aged
21 years and older in rural Indonesia is among the highest reported in Southeast Asia. Despite this, there are inadequate resources
available to manage this treatable disease. Allocation of resources to tackle the present burden of cataract with developed and patented to
Babizhayev N-acetylcarnosine lubricant eye drops would likely have large personal, social, and economic benefits.
6 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

hydrochloride contain benzaltonium chloride preserva-
tive. When ocular anesthesia was achieved, the lids were
extended and fixed with the lid holder, and the ocular
bulb was fixed by tweezers in the area of the inferior
rectus muscle. A stab incision was performed transcorn-
eally 1.0–2.0 mm from the limbus in the temporal
superior quadrant. Aqueous humor (0.1–0.2 mL) was
aspirated from the anterior chamber of a rabbit eye with
25-gauge needle connected to an insulin syringe and
immediately introduced into an Eppendorf tube with the
addition of ethanol (0.2 mL), keeping the sample on ice
before extraction.
Extraction of imidazoles from aqueous humor
Extractions of imidazole-containing compounds from the
aqueous humor aliquots were performed according to
Babizhayev et al., [14]. The published data showed that
all the desired imidazole-containing compounds in the
aqueous humor thus obtained could be of good purity and
recovery [14]. Portions of aqueous humor were added to
ethanol as afore mentioned and thoroughly mixed
(20 �C, 15min). Extracts were centrifuged (2000 g,
15 min), and the supernatants were removed. Samples
were frozen in the gradient of temperatures to )70 �C and
lyophilized using the apparatus JOAN (France). The
lyophilized residue was dissolved in 1 mL of 0.1 M Na2
HPO4 (pH 2.1 adjusted with 85% phosphoric acid) and
filtrated through the membrane filter with the dimensions
of pores 0.22 lm directly prior the analysis.
Analytical HPLC for the detection of L-carnosine and
N-acetylcarnosine
Reverse-phase analytical HPLC was performed using a
Breeze chromatography system (Waters corporation,
Milford, MA, USA), detector Waters 2487 Dual kAbsorbance Detector, column (250 · 4.6 mm) Symme-
try 300 C18 5 lm (Waters), loop 20 lL (Figure 6b). The
column was eluted isocratically at 30 �C with the cited
phosphate buffer 0.1 M Na2 HPO4 (pH 2.1) over 25 min
at a flow rate of 1.0 mL/min. Eluates were monitored
for absorbance at 210 nm. The standards of L-carnosine
and N-acetylcarnosine were prepared by weighing of
the dry material using the analytical balance Mettler
Toledo (accuracy 0.00004) and were further dissolved
in the phosphate buffer 0.1 M Na2 HPO4 (pH 2.1)
(Figure 6b). The quantitative determination of L-carno-
sine and N-acetylcarnosine in the samples was under-
taken using the technique of external standard
according to the area of the peak and linear extra-
polation. The standards of eye drops were prepared by
dissolution of initial solutions of eye drops by 100-fold
using the phosphate buffer 0.1 M Na2 HPO4 (pH 2.1).
Statistical significance was evaluated by the unpaired
Student’s t-test, and P = 0.05 was taken as the upper
limit of significance.
Clinical design: N-acetylcarnosine lubricant eye
drops studies
The examined subjects consisted of 75 older adults with
age-related uncomplicated cataracts in one or both eyes
and 74 adult subjects who did not have cataract in either
eye. Patients in these subsamples suffered from different
degrees of glare problems. Those with cataract ranged in
Figure 5 Principle of the glare test for adults, based on the
measurement of the glare radius (r, mm) a new metric for glare
sensitivity. I0 = Indicatrix of light scatter; u = angle. The technique
utilizes a self-illuminating red or green optotype target and tangen-
tial 2 mm ‘point light source’ seen from a distance of 30 cm. The
patient’s task is to move the optotype closer to the glare source until
it disappears because of the veiling glare from the glare source. A
halometer score is determined as follows. The target is approached
from the source so that the patient becomes unable to distinguish the
target from the source, and then, the target is slowly taken away
until the exact moment when the patient distinguishes the target; at
this time, the incident light angle u between the source and the
target is measured. The target is always fixated with the foveal
vision. The target and the ‘point light source’ are viewed in the
same vertical plane, tangential to the plane of emitted light. In this
case, to measure the angle u of the incident light between the
source and the target, it is necessary only to measure its projection
on this vertical plane, which means to measure the distance
between the source and the target. The measured glare radius is
defined as a target image projection for the vector of light scatter
(indicatrix of light scatter I = I0cos2 u) when the glare source is
activated and the patient is asked to recognize the target during
illumination of the eye with a glare source.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 7
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

age from 54 to 85 years (mean ± SD, 70 ± 8 years),
with 49% female, 100% white and of non-Hispanic
origin. The no-cataract subjects ranged in age from 54 to
80 years (mean ± SD, 68 ± 8 years); 51% were female,
with 100% being white. Subjects who were cataract-free
had to meet the same inclusion criteria as the subjects
with cataract described previously [15–19,45]. All
subjects with cataract were required to meet the follow-
ing inclusion criteria: (i) cataract in one or both eyes
with best-corrected visual acuity of 20/40 or worse in
one or both eyes as indicated by the medical record;
(ii) no previous cataract surgery in either eye; (iii) a
primary diagnosis of cataract in the medical record; (iv)
living independently in the community; specific items
were needed to be addressed if appropriate: (v) the
driving skills: legally licensed to drive and drove during
the 5 years prior to enrollment. Among participants,
bilateral cataracts were present in 91% of subjects
according to the medical record from the most recent
eye examination (within 1 month of enrollment). In the
right eye, 41% had nuclear sclerotic cataract, 9% had
cortical cataract, 11% had posterior subcapsular cata-
ract, and 39% had a combination of at least two types.
The breakdown was similar in the left eye, with 45%
nuclear sclerotic, 10% cortical, 8% posterior subcapsu-
lar, and 37% combination. Seventy-three percent of
subjects with cataract had no additional ocular
conditions other than refractive error; 7% had early
nonexudative age-related maculopathy, 6% had primary
open-angle glaucoma (POAG) associated with cataract,
5% had diabetic retinopathy, 2% had a combination of
two of these problems, and 7% had another ocular
condition. Subjects who were cataract-free had to meet
the same inclusion criteria as the subjects with cataract,
except that they were required to be free of cataract and
to have a best-corrected visual acuity of 20/25 in each
eye, according to medical record review. No cataract-free
subjects had secondary eye conditions other than
refractive error.
Patients with known or presumed hypersensitivity to
any component of the ophthalmic preparations (active
substances or excipients), and those treated with drugs
that could interfere with this trial, were also excluded
from the study. The subjects were recruited and
examined by ophthalmology practices of Innovative
Vision Products Inc (County of New Castle, DE, USA).
The study protocol was approved by the Corporative
Review Board for Human Use. After the purpose of the
study had been explained, each subject was asked
to sign a document of informed consent before
Table I Characteristics and specification of carcinine (Decarboxy
carnosineÆ2HCl) synthesized by Exsymol S.A.M. (Monaco,
Principaute de Monaco).
Composition of the substance: pure substance
cGMP/GLP characteristics
Purity as a percentage: >99%
Hydrosolubility: soluble in water
Liposolubility: insoluble in mineral and vegetal oils
Fusion point: FP = 195 �CQuantification of heavy metals: <20 ppm
Quantification of chlorides: 25.0–30.5%
Infrared characterization: positive
Physical state at 20 �C under 101.3 kPa: solid
Physical characteristics: white crystalline powder, odorless
Microbiology
Mesophilic aerobic bacteria: <1000/g
Yeasts, molds: <100/g
Escherichia coli (per g): none
Table II Characteristics and specification of (a) L-carnosine and
(b) N-acetylcarnosine synthesized by Hamari Chemicals Ltd.
Test item Requirement
Specification of L-carnosine
Appearance White crystal or crystalline
powder
Odor Odorless
Identification Positive
Optical rotation: ½a� 20D +19.8 to +22.2�
Transmittance NLT 95.0%
Heavy metals NMT 10 ppm
Arsenic NMT 2 ppm
Other amino acids Not detectable
Loss on drying NMT 1.0%
Residue on ignition NMT 0.20%
Assay 98.0 to 101.0%
Test name Specification
Specification of N-acetyl-L-carnosine
Appearance White powder
Identification Positive
Optical rotation ½a� 20D +25.2 to +27.5�
pH 4.5–5.5
Heavy metals NMT 10 ppm
Related substances L-Carnosine: NMT 0.3%
Others: NMT 0.2%
Residual solvent 2-propanol: NMT 500 ppm
Water NMT 5.0%
Residue on ignition NMT 0.10%
Assay NLT 99.5% (HPLC area)
NMT, not more than; NLT, not less than.
8 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

enrolling. Demographic data and driving status dur-
ing the prior 5 years were confirmed by interview
(Table IV).
Procedures
After enrollment, subjects were computer-randomized
into two groups assigned according to the double-blind
method: to receive treatment with N-acetylcarnosine 1%
eye drops (Can-CTM) or to a control group who received
placebo eye drops. The blinded testing was carried out by
an independent medical worker who handed out the NAC
vs. placebo eye drops (control group) to the randomized
subject members of the clinical groups. The enrolled
subjects underwent follow-up examinations at baseline
and after 5–6 months of enrollment. Test examiners were
masked to the driving histories of all subjects. Two types
of visual functions were assessed: visual acuity and glare
sensitivity (disability glare). All acuity measurements
were taken while subjects wore the lens correction they
typically used during the performance of everyday
distance activities, including driving. Each eye was
assessed separately. Distance acuity was measured as
described before using the letter chart and its standard
protocol and was expressed as log minimum angle
resolvable [15–19,45,48,49]. For each eye, visual acuity
measurements were grouped into four categories: 20/25
or better, 20/25–20/30, 20/35–20/50, and worse than
20/50. These cut points were chosen because they were
the approximate quartiles of the acuity distribution and
included the practically significant cut point for driving
licensure in many countries (20/40–20/50).
Slit lamp biomicroscopic examination or exampled
photographic registration was performed after pupil
dilation to a minimum of 6 mm with tropicamide.
Disability glare was defined with an optical instrument
and method for measuring susceptibility to glare of a
human vision system as described [15–19,45–47]
and schematically presented in Figure 5. A constant
(a)
(b)
Figure 6 (a) Typical rabbit’s eye used in an ocular pharmacokinetic
study. (b) Configuration of techniques for HPLC analysis of peptides
extracted from the aqueous humor. The BreezeTM HPLC System
delivers technology and performance in an affordable, compact, and
user-friendly system platform. Complete with software, pump,
detector, and injector, the Breeze comes preconfigured for different
levels of HPLC operational needs with peptide moieties. Symmetry
column(s) (image below) continues to set the standard for HPLC drug
assays, giving a confidence in the long-term compliance of HPLC
methods. No need to compromise on peak shape, selectivity, column-
to-column and batch-to-batch reproducibility, or other critical
performance characteristics. For laboratory balances weighing to the
nearest 0.0000001 g, for the provided fine measurements of the
mass of extracted peptide residues from the aqueous humor, it can be
sure to use a Mettler Toledo balance that matches the specific
weighing needs during precise works with peptides.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 9
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

‘point’-like bright glare source is used to create the glare
condition (Figure 5). The examining room was dark (<20
foot-candles) as typical when working with the glare
testers to assure maximum contrast of the projected
target. Tests were performed with the best correction in
place. The indicator of optotypes on the front or back
panels of the instrument indicated the tested optotype to
the patient or clinician, respectively. The diagnostic block
of a device contained source light window (glare source)
and the moving indicator of the optotypes illuminated
with red or green light (Figure 5). The back panel of the
Halometer device facing the clinician was equipped with a
chart/scale and with a moving indicator of the optotype
transition. According to a special embodiment of the
invention, [15–19,45–47] for the clinical testing of glare
sensitivity of a patient, we used an illuminated target with
red or green color, which enables the assessment of the
effect of wavelength on the scattered light.
Treatments with N-acetylcarnosine 1% lubricant eye drops
N-Acetylcarnosine (NAC) eye drops (Can-CTM)
contained a 1% solution of NAC (Babizhayev MA,
Bozzo Costa E. Composizioni farmaceutiche contenenti
N-acetilcarnosina per il trattamento della cataratta.
Italian Patent A61K gruppo 37/00 20122 MI, Priority
Oct. 15, 1993.; Babizhayev MA, Bozzo Costa E. Phar-
maceutical compositions containing N-acetylcarnosine
for the treatment of cataract. Patent PCT/EP 94/03340
SCB 238 PCT, Oct. 10, 1994.; Babizhayev MA. Method
for topical treatment of eye disease and composition and
device for said treatment. PCT Patent Application.
International Publication Number WO 2004/028536
A1. International Publication Date: 8 April 2004) with
a lubricant 0.3% carboxymethylcellulose in the isotonic
ophthalmic formulation in borate buffer with preserva-
tive benzyl alcohol (corneal absorption promoter) and
showed the increased intraocular absorption of the
active principle (L-carnosine) in the aqueous humor
compared with topical administration of a pure 1% NAC
solution:
Deionized water 970 g
Glycerin, 1.0% 13 g
N-acetylcarnosine, 1.0% 10 g
Carboxymethylcellulose, 0.3% 3 g
Benzyl alcohol, 0.3% 3 g
Potassium borate 7.91 ga
Potassium bicarbonate 3.47 ga
aOr what is necessary to bring the solution up to a pH of approximately 6.3–
6.8.
The ophthalmic formulation thus creates a facility to
examine the efficacy of treatment for improvements in
vision during the short-term periods of administration of
N-acetylcarnosine 1% eye drops (5–6 months in this
study). The administration schedule was two drops
instilled twice daily, for patients assigned to NAC and
those assigned to placebo (the same formulation without
N-acetylcarnosine, 1%) alone for 5–6 months. The use of
other topical or nutritional antioxidants was not mea-
sured or evaluated between the two groups. The control
groups and the treated group did not take any prescribed
antioxidant vitamins that might have added to the
antioxidant level. Neither the investigators nor the
patients knew who was receiving NAC.
Carcinine ophthalmic research
Experimental modeling of proliferative vitreoretinopathy
(PVR)
Experimental model of PVR is very important in inves-
tigation of pathogenesis and prophylaxis of this ocular
pathology. Grey Chinchilla male rabbits aged 3–
4 months, each weighing between 2 and 3.0 kg, were
used. All animals were sedated by intramuscular injec-
tions of ketamine-xylazine (10 mg/kg body weight). The
eyes were dilated with one drop of 1% cyclopentolate and
2.5% phenylephrine.
We used the ‘cytokine’-induced model of PVR devel-
oped at Moscow Helmholtz Research Institute for Eye
Diseases [50]. In the in vivo model, rabbit eyes were
injected intravitreously with cytokine complex alone to
induce tractional retinal detachment.
The cytokine complex (each single dose of 600 lg)
included retinal pigment cells (9.1–9.6 · 102 cells in
0.2 mL of medium), endogeneous immunopeptides, and
glycoprotein fibronectin. Formulated in advance hetero-
logic cytokine complex including endogeneous immuno-
peptides with activity of Il-1, TNF-a, MIF, and TGF-b(0.1 mL) was administered with the single intravitreous
injection into both matched rabbit eyes [50]. Separate
control group of rabbits was used for modeling of PVR
with cytokine challenge, placebo (vehicle) administra-
tion [the matched control eyes were injected into the
vitreous with phosphate-buffered saline (PBS)] and the
pure eyes morphological control.
Carcinine (b-alanylhistamine) at a concentration of
10 mM dissolved in PBS was used as a prophylaxis
remedy. This drug was injected into the experimental
eyes using the multiple parabulbar (repeated single daily
injections within consequent 5 days) or single-time
intravitreous administration ways. The therapeutic
10 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

injections were provided to the left eyes after the
experimental intravitreous injection of cytokine complex
was completed. The right eyes served as a control. At the
end of the month, the animals were killed, and their eyes
were enucleated.
Parabulbar injections (5) were applied during 5 days
to the left eye started just after the intravitreous injection
of the cytokine complex. In this group (nine rabbits
studied), the rabbit eyes obtained the parabulbar injec-
tions of carcinine after the intravitreal injection of
cytokine. In a separate group of rabbits (six rabbits),
subconjunctival injections were applied instead of para-
bulbar injections according to the described design. In
the separate group (five rabbits), we have applied single-
dot intravitreous injection of carcinine (10 mM, 0.1 mL
in balanced physiologic saline) simultaneously with
cytokine complex to the left eye. The separate group of
rabbit eyes (four rabbits) received postponed parabulbar
injections of carcinine started 3–4 days after the intra-
vitreal challenge with cytokine complex. These post-
poned parabulbar injections of carcinine prolonged
within 5-day follow-up period. The right eyes served as
a control after the intravitreal injection of cytokine in all
cases.
Morphological (light and electron microscopic) inves-
tigation was carried out. Histopathologic examination of
the globes of rabbits was used to evaluate the morpho-
logical change after intravitreous injection of cytokine
complex and carcinine. On day 30 after treatment, all
animals in the experiment were killed by intravenous
injection of an excessive dose of pentothal. Globes were
enucleated immediately and fixed with phosphate-
buffered 10% formaldehyde. The specimens were then
dehydrated with increasing concentrations of ethanol,
cleared with xylene, and embedded in paraffin. Ten-
micron sections were cut and stained with hematoxylin
and eosin. Tissue sections were observed and photo-
graphed by light microscopy. In the control eyes, clinical
and morphological picture of PVR was observed. In the
treated eyes, there was a noticeable inhibition of
inflammation and proliferation in the retina. The mech-
anism of PVR inhibition under the influence of carcinine
was studied.
Carcinine effects against light-induced damage and
photoreceptor cell death in Balb/C mice
Balb/C mice were raised in a 12-h dim light (10 lux)-
dark cycle (Figure 7a). Two-month-old mice were deeply
anesthetized with a single intraperitoneal injection of
xylazine (20 mg/g) and ketamine (40 mg/g). One
microliter of carcinine or PBS (vehicle control) was
injected intravitreally into the eye using a 36-gauge
needle (World Precision Instruments, Sarasota, FL,
USA) through the temporal limbus of the eye. In each
animal, the left eye was injected with carcinine and the
right eye with PBS. Thus, each animal served as its
own control. Mice were returned in dim cyclic light for
48 h before exposure to bright light (4000 lux) for 5 h
to induce oxidative stress in photoreceptor cells, as
described previously [51]. After light damage, mice
were returned in dim cyclic light for 7 days to allow the
retina to clear all dead cells and return to a well-
organized morphology. Mice were killed by CO2 inha-
lation before tissue collection. This method is approved
by the Panel of Euthanasia of the American Veterinary
Medical Association. All procedures were performed
according to the National Institutes of Health Guide
for the Care and Use of Laboratory Animals and
the University of Oklahoma Health Sciences Center
(OUHSC) Guidelines for Animals in Research. Whole
eyes were enucleated after orientation of the superior
half with a permanent dye. Oriented eyes were embed-
ded in paraffin, and sections were cut along the vertical
meridian, through the optic nerve head (ONH). To
quantify the number of remaining photoreceptors,
hematoxylin- and eosin-stained paraffin sections were
prepared from each eye, and the thickness of the outer
nuclear layer (ONL) was measured at 0.24-mm inter-
vals from the ONH to the inferior and superior ora
serrata as described previously [51].
Figure 7 Balb/C mice were raised in a 12-h dim light (10 lux)-dark
cycle.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 11
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

Study of acute toxicity of carcinine by oral administration
in mice
This experimental series has been conducted to verify
the innocuousness of the carcinine product being tested
in the event of accidental ingestion. Male Swiss mice,
weighing 20 g from the IFFA CREDO (Lyon, France)
Breeding Center, were used in the study. The animals
have been chosen at random, and the batches were
prepared before the beginning of the oral treatment
with carcinine. The mice were kept in cages equipped
with a sterilized sawdust floor. Feeding consisted of
‘SOURIS Entretien’(SA. U.A.R.) food. Water was given
as desired.
Administration of compound being studied (carcinine)
was undertaken under the following conditions. Mice
were deprived of water within 15–20 h. The testing
compound (carcinine) was then administered by gastric
intubation (with an oesophagian probe), one time, to a
group of 10 animals (five males and five females). The
treated animals absorbed 2 g of the tested compound per
kg of body weight (20 mL/kg of a 10% solution), i.e., the
maximal quantity permitted for gnawing animals (JO.CE:
L 383 A/111). In the event of death, the compound to be
studied was administered to another group of 10 mice
(five males and five females). They absorbed 1 g/kg of
body weight (10 mL/kg of a 10% solution). If the LD 0
value was <1 g/kg, the LD 50 was calculated. If the LD 0
was more than 1 g/kg, the compound was said to be
nontoxic.
Statistical analyses
Statistical analysis was performed by Student’s t test;
P = 0.05 was taken as the upper limit of significance. To
assess associations, correlation and linear regression
analyses were used.
R E S U L T S
Intraocular transcorneal and systemic absorption
of L-carnosine from N-acetylcarnosine ocular drug
delivery system (lubricant eye drops Can-CTM):
suitable molecular therapeutic interventions and
visual sensory signaling responses
Histidyl compounds of aqueous humor have been
examined by reverse-phase analytical HPLC (see Exper-
imental design: N-acetylcarnosine lubricant eye drops
studies) as used in separation of imidazole-containing
amino acids and dipeptides described earlier [52]. Amino
acids can be detected by the absorbance of carboxylate
(approximately 200 nm) and peptides by the absorbance
of carboxylate and the peptide bond (200–220 nm).
Chromatograms of solutions of L-carnosine and its
putative N-acetyl derivative (Figure 8a) show that these
compounds are well separated. The elution order of the
compounds was compared with a predicted order based
on their relative hydrophobicities as outlined by Rekker
[53]. The chromatographic system is suitable to monitor
the behavior of other histidine-containing derivatives of
carnosine [14]. The calibrating chromatograms show
the predicted elution order and the average elution times
for each standard of L-carnosine and NAC in mixtures
(Figure 8a) and the presence of majority of NAC in the
lubricant eye drops Can-CTM employed in pharmaco-
kinetic experiments (Figure 8b). Peaks were unequivo-
cally identified by comparison of their retention times to
those of the authentic standard compounds or of
Figure 8 (a) HPLC of a mixture of L-carnosine and N-acetylcarnosine (NAC). Peak fractions were examined for specific chemical reactivity.
The integrated calibrating concentrations for the standard peaks were (a) 140 lg/mL, 3.216 min for carnosine; 82.5 lg/mL, 6.017 min for
NAC. The retention times of compounds in mixtures did not vary significantly from those run singly. Peak at 3.00 min is the solvent front.
(b) HPLC analysis of the imidazole moieties in the eye drops formulation. Can-CTM after appropriate dissolution of initial solutions of eye drops
by at least 100-fold for HPLC chromatography analysis purposes (see, Experimental design: N-acetylcarnosine lubricant eye drops studies
section). The high peak of N-acetylcarnosine (NAC) is detectable with a retention time of 6.078 min. The presence of L-carnosine in the
mixture with retention time of 3.232 min is negligible. The small peak at 3.00 min is the solvent front. (c) HPLC of extract of aqueous humor
aspirated 30 min after the instillation of ophthalmic formulation with 1% NAC and lubricants into the rabbit eye. The integrated
concentration of the carnosine-related product (3.392 lg/mL, 3.225 min) is attributed to accumulation of carnosine in the ophthalmic
formulation-treated eye. Chromatograms of solutions of L-carnosine and its putative N-acetyl derivative show that these compounds are well
separated. The elution order of the compounds was compared with a predicted order based up their relative hydrophobicities, and the
chromatographic system was shown to be suitable to monitor the behavior of other histidine-containing derivatives of L-carnosine.
The calibrating chromatograms showed the predicted elution order and the average elution times for each standard of L-carnosine and
N-acetylcarnosine in mixtures. Peaks were unequivocally identified by comparison of their retention times to those of the authentic standard
compounds or of putative acetylated compound run singly. Tests for specific chemical reactivity provided additional evidence for the
identification of L-carnosine and N-acetylcarnosine [14].
12 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

putative acetylated compound run singly (Figure 8a).
Tests for specific chemical reactivity [54] provided
additional evidence for the identification of L-carnosine
and N-acetylcarnosine.
As a result of its relative hydrophobicity compared with
L-carnosine, NAC might cross the cornea of the treated eye
gradually and maintain longer the concentration of the
active principle (L-carnosine) reaching the aqueous
(c)
(a) (b)
N-acetylcarnosine lubricant eye drops and carcinine for vision care 13
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

humor. In the present section of the study, we considered
whether NAC acts in the ophthalmic formulation with
lubricants and preservatives when topically administered
to the eye as a time release carrier (prodrug) of L-carnosine.
The HPLC pattern of an extract of the aqueous humor
obtained 30 min after instillation to the rabbit eye of
ophthalmic formulation containing 1% NAC, lubricants
carboxymethylcellulose, glycerin, and preservative benzyl
alcohol in the borate buffer confirms that the peak
characteristic of L-carnosine has a concentration and a
retention time (3.225 min) clearly distinct from N-acet-
ylcarnosine (6.0 min) and basically different from the
dead time of the column (3.0 min) (Figure 8c). This
identified peak of L-carnosine quantified and integrated
by the data processor showed that virtually all N-acetyl-
carnosine after the overall extraction efficiency is con-
verted into the L-carnosine compound with a retention
time of 3.225 min (Figure 8c). The data on the L-carno-
sine-related product were blanked with the control
placebo data applied to the paired eyes of the animals.
The mean ratio of L-carnosine (C)/(NAC) relevant to the
L-carnosine release in the aqueous humor 30 min after
instillation of formulation A (Can-CTM) with 1%
N-acetylcarnosine into the rabbit eye corresponded to
C/NAC = 6.64 ± 0.06 (n = 8, where n = number of the
examined treated rabbit eyes; only right eyes were
treated). In the control placebo formulation-treated eyes,
the same indices could not be quantified at statistically
significant rate. Concentrations of imidazole products in
the aqueous humor corresponded to those of intact rabbit
eyes and refer to baseline values of L-carnosine
0.19 ± 0.10 lg/mL related products variously detected
in extracts from normal animals.
Our data demonstrate that topical administration of
pure L-carnosine (1% solution) to the rabbit eye (instil-
lation and subconjunctival injection) does not lead to
accumulation of this natural compound in the aqueous
humor over 30 min in concentration exceeding that in
the placebo-treated matched eyes, and its effective
concentration is exhausted more rapidly [52,55]. In
another aspect, the data presented in Results sections
demonstrate the prospects of applications of an ophthal-
mic composition comprising NAC or its pharmacologi-
cally acceptable salt in combination with a cellulose
compound or its pharmaceutically acceptable salt, which
are effective to treat the eye complex of symptoms. This
complex of symptoms may have an oxidative component
in their genesis, such as senile cataract, glaucoma,
inflammation, or diabetic ocular complications. The
topical administration of N-acetylcarnosine in the devel-
oped and patented lubricant eye drop formulation
delivers pure L-carnosine and allows its increased
intraocular absorption into the aqueous humor
surrounding the lens, thus enabling significant improve-
ments in anticataract efficacy [10]. This formulation also
optimizes beneficial effects in a number of ocular
degenerative age-dependent disorders [15–19].
The important pharmacokinetic observation activities
of the tested ophthalmic formulation Can-CTM including
1% N-acetylcarnosine and lubricant carboxymethyl-
cellulose relate to the accumulation of L-carnosine in the
aqueous humor of the contralateral rabbit eyes after
30 min of instillation of the medication to the tested rabbit
eyes. The detected measure of L-carnosine in the aqueous
humor of the contralateral untreated eyes corresponded to
1.45 ± 0.08 lg/mL (n = 9). The data indicate that
intraocular route for the administered medication in-
cludes (at least partially) a systemic drug absorption in the
preferred intraocular site of L-carnosine released from 1%
N-acetylcarnosine ophthalmic prodrug enhanced with the
addition into the ophthalmic formulation of a cellulose
derivative, i.e., carboxymethylcellulose (bioadhesive and
absorption enhancer) that is also used as a mucoadhesive
carrier for the patented ocular drug, owing to its ability to
coat the cornea and remain on the eye for a longer time.
This route of systemic absorption of biologically active
compound avoids the first-pass effect normally observed
after oral presentation of a compound, and the pharma-
cological sequelae resemble those seen after an intrave-
nous administration. This pharmacokinetic phenomenon
has been given in clinical situations with topical admin-
istration of antiglaucoma medicines to the eye, because
the systemic effects of drugs such as timolol can be quite
pronounced [56].
The systemically absorbed L-carnosine released from
the 1% N-acetylcarnosine ophthalmic prodrug Can-CTM
as lubricant eye drops, which is topically administered to
the eyes, not only acts as a radical scavenger but also
represents a possible neurotransmitter-like molecule that
regulates neuronal functions such as hypothalamic
control of the autonomic nervous system. CN2 (CNDP2)
is a cytosolic enzyme that can hydrolyze carnosine to
yield L-histidine and beta-alanine. CN2-immunoreactivity
was highly concentrated in neuronal cells in the dorsal
part of the tuberomammillary nucleus of the posterior
hypothalamus [57]. As the tuberomammillary nucleus is
the exclusive origin of histaminergic neurons, further
investigations were focused to find whether CN2 is
present in the histaminergic neurons. It was found that
CN2-immunoreactivity was colocalized with that of
14 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

histidine decarboxylase, which is the key enzyme for
histamine biosynthesis specifically expressed in the
histaminergic neurons of the tuberomammillary nucleus
[57]. These results clearly indicate that CN2 is highly
expressed in the histaminergic neurons in the tubero-
mammillary nucleus, implying that systemically
absorbed L-carnosine released from the Can-CTM ophthal-
mic formulation topically administered to the eyes serves
as a metabolic source to supply histidine and activates
histaminergic neurons for histamine synthesis (Figure 9).
Axons of the tuberomammillary nucleus project primar-
ily to the cerebral cortex, thalamus, basal ganglia, basal
forebrain, and hypothalamus. Tuberomammillary acti-
vation usually results in a rapid and significant increase
in the amplitude of baseline activity and visual responses
in lateral geniculate nucleus (LGN) neurons [58].
Tuberomammillary activation causes a small phase lag
in the visual response that is similar at all spatial frequen-
cies, consistent with the induced shift from burst to tonic
firing mode. These results indicate a significant histamin-
ergic effect of L-carnosine on LGN thalamocortical cells,
with no clear effect on thalamic inhibitory neurons.
The histaminergic system appears to strengthen
central transmission of afferent information, intensifying
but not transforming the retinally derived signals. The
increase in visual response developed rapidly within the
first visual stimulus cycle and persisted for the duration
of tuberomammillary activation. Promoting sensory
input in addition to the direct anticataract activities of
N-acetylcarnosine prodrug supported through the num-
ber biochemical mechanisms [19,58] may be one way in
which the histaminergic system plays a role in enhance-
ment of visual functions and responses in elderly patients
with cataracts and no-cataract adult subjects who
usually note the brightness, relaxation, decrease in
disability glare, and clarification of vision in their treated
eyes already after the short-term administration of 1%
N-acetylcarnosine lubricant eye drops (1 week – 5- to
6-month periods of treatment) (this study) and during
the more prolong evaluation period and follow-up
(9 months) described previously [15–19]. Tubero-
mammillary histaminergic neuron activity could be
inhibited by a GABAergic pathway, originating in the
ventrolateral preoptic area, which was activated during
sleep [59].
Inhibition of experimental proliferative
vitreoretinopathy by carcinine in a rabbit model
Proliferative vitreoretinopathy was modeled that was a
complicated ocular pathologic process. Morphologically,
there is an extensive intraretinal proliferation accompa-
nied with the formation of epiretinal membrane in
pathogenesis of PVR.
Contractile properties of epiretinal membrane lead to
the retractive retinal detachment. Initially, we used the
cytokine-induced model in 24 rabbits. During modeling,
the natural complex of cytokines (NCC) that included
endogeneous immunopeptides with activity of IL-1,
TNF-a, MIF, and TQF was injected into the vitreous
body of both contralateral eyes of the animals in a
standard amount of 0.1 mL (single dose of 600 lg). The
main evaluation of the pathologic process was carried
out with clinico-morphological study. The results below
are presented after 1 month of follow-up. Natural
imidazole-containing pseudodipeptide carcinine is ubiq-
uitous in mammalian tissues and presents rather stabil-
ity in the area of inflammation to the action of
proteolysis with specific and nonspecific peptidases
[43,60].
Figure 9 Neurons of tuberomammillary nucleus of hypothalamus
as a target of a systemically absorbed L-carnosine (see, formula) in
the activation (arousal) of vision responses. Possible mechanism of
brightness, relaxation, and clarification effects on vision of adults
and elderly patients after topical administration of carnosine to the
eyes in the form of 1% N-acetylcarnosine ophthalmic prodrug
(lubricant eye drops including carboxymethylcellulose bioadhesive
and absorption enhancer).
N-acetylcarnosine lubricant eye drops and carcinine for vision care 15
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

In this experimental series, carcinine is indicated for
administration as a medicine for ophthalmic treatment
in the injection formulation (subconjunctival, ocular
parabulbar, and intravitreous injections). Recent study
demonstrated the reactivity of carcinine with ROS and
aldehyde products [43]. Carcinine noticeably limits
4-hydroxynonenal (4-HNE)-induced cross-linking of col-
lagen. Carcinine is utilized for ophthalmic protection
based on its antioxidant including hydroxyl-radical-
scavenging and lipid peroxidase activities patented by
Babizhayev et Exsymol [43,47]. Carcinine is working as
a water-soluble universal antioxidant both in the lipid
phase of cellular and biologic membranes and in an
aqueous environment [43,47].
Peculiarities and staging of PVR morphogenesis in the
cytokine-induced model
Proliferative processes occurred in 100% of the control
eyes challenged with cytokine complex. Epiretinal and
subretinal localization of PVR was detected among the
cytokine-challenged control eyes. The spreading of the
process varied (Figure 10). The most frequent was the
paraneural localization of the PVR. Proliferative changes
were characterized by two types of changes.
The first one is the formation of the limited prolifer-
ative hearth in which the fiber elements are combined
with proliferating fibroblast-like cells. Originating from
proliferation, the shaft-braces are protracted inside the
vitreous body. The second mode of changes is the
creation of flat limited formations of the fiber structure
like epiretinal membrane, which are spreaded above
limitans interna of the retina with the single fibroblast
cells as well as with glyal elements. The same structures
form the veil-like thickenings of the internal boundary
retinal membrane. Such formations have rather ex-
tended character. The formed areas of epiretinal and
subretinal proliferation led to the folds of the retina and
its detachment. Among proliferations that contained the
spindle-shaped cells, the accumulations of macrophages
and lymphocytes did occur. In several cases, the massive
fibrotic protractions appeared extended from the funnel
of the nervus opticus toward the lens. The mode of
proliferative processes exhibited hearth-like character
near the accumulations of macrophages at the internal
boundary membrane intermitted with the zones of the
intact retina. The cases of more extended epiretinal
membrane occurred from ora serrata to the disk of the
nervus opticus.
Such extension is regarded with multiple strains of the
internal boundary membrane in which glyal and fibro-
blastic elements are actively proliferated with formation
of the fiber structures of the epiretinal membrane. Often,
combination of epiretinal proliferation with the subreti-
nal proliferation in the control group of animal eyes took
place in such modeling.
Clinical and Morphological data provided with the
cytokine-induced modeling of PVR revealed:
• The role of macrophages as the trigger cells reaction
involved in the pathogenesis of PVR, especially initial
stage of PVR.
• Inhibitory action of carcinine on the PVR progres-
sion, its especial role at the initial stage of PVR, based on
the property of carcinine to block the functional activity
of macrophages in disease.
Morphological stages in the development of PVR:
initial, advanced, and terminal
At the initial stage of PVR, three morphological compo-
nents were noticed.
• Accumulation of macrophages: There was an
accumulation of macrophages attracted from blood
vessels by cytokines into the vitreous of the eye
(Figure 10). Macrophages represent the cells, acting as
regulators and a polyfunctional complex. Macrophages
synthesize different enzymes, peroxide compounds, bio-
logic active substances, and growth factors, promoting to
proliferation of fibroblasts and fibril material. Macrophag-
es are capable for adhesion depending on function
forming conglomerates.
• The damage of the inner limiting membrane: The
conglomerates of active macrophages showed cytotoxic
effect to the environment, especially to the retina. The
result of such process was the damage of the inner
limiting membrane (ILM) and reactive proliferation of
glyal cells (see, Figure 10c).
• Formation of epiretinal membrane: Active prolifera-
tion of glyal and fibroblastic cells around the place of ILM
damage formed an epiretinal membrane. It was possible
to distinguish not only cells but also the collagenous
fibrils and accumulation of the extracellular matrix
fibronectin–like protein component (see, Figure 10d).
Morphology of the advanced PVR stage is character-
ized by the following features: Spread of the epiretinal
membranes with contractile properties leads to the
appearance of the retinal folds (Figure 10e).
Morphology of the terminal stage of PVR is charac-
terized by spreading of the epiretinal and vitreoretinal
proliferation with retractive retinal detachment
(Figure 10f). In the group of rabbit eyes treated with
postponed parabulbar injections started 3–4 days after
16 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology
the intravitreal ocular challenge with cytokine complex
of the rabbit eyes within 5-day follow-up period, less
pronounced inhibitory effect was observed to PVR
morphogenesis than in the case of parabulbar or
subconjunctival injections started immediately after the
intravitreal injection of cytokine (1 parabulbar injection
per day prolonged for 5 days).
In all control cytokine-challenged rabbit eyes, the
inflammatory reaction was noted, which was charac-
terized by the small lymphocyte infiltration inside the
ciliary body and the appearance of inflammatory cells
inside the vitreous cavity, sedimented preferably onto
the collagen fibers of the carcass elements and on the
internal boundary membrane of the retina. Among the
(a) (b)
(c) (d)
(e) (f)
(g) (h)
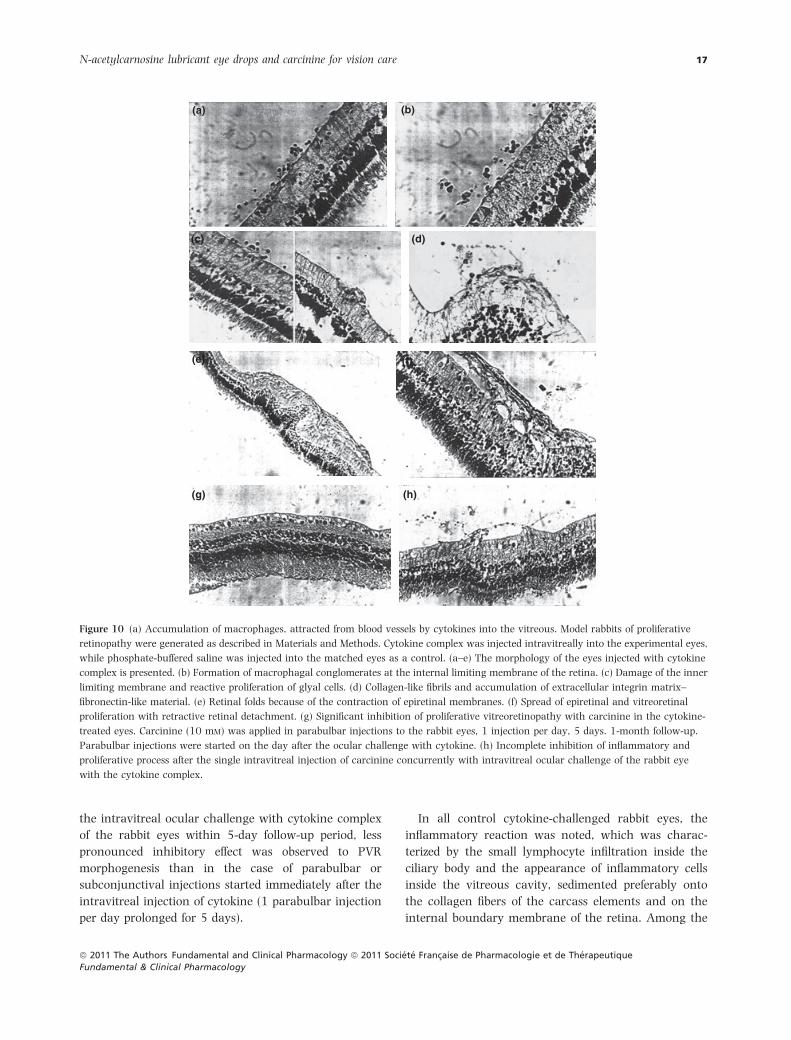
Figure 10 (a) Accumulation of macrophages, attracted from blood vessels by cytokines into the vitreous. Model rabbits of proliferative
retinopathy were generated as described in Materials and Methods. Cytokine complex was injected intravitreally into the experimental eyes,
while phosphate-buffered saline was injected into the matched eyes as a control. (a–e) The morphology of the eyes injected with cytokine
complex is presented. (b) Formation of macrophagal conglomerates at the internal limiting membrane of the retina. (c) Damage of the inner
limiting membrane and reactive proliferation of glyal cells. (d) Collagen-like fibrils and accumulation of extracellular integrin matrix–
fibronectin-like material. (e) Retinal folds because of the contraction of epiretinal membranes. (f) Spread of epiretinal and vitreoretinal
proliferation with retractive retinal detachment. (g) Significant inhibition of proliferative vitreoretinopathy with carcinine in the cytokine-
treated eyes. Carcinine (10 mM) was applied in parabulbar injections to the rabbit eyes, 1 injection per day, 5 days. 1-month follow-up.
Parabulbar injections were started on the day after the ocular challenge with cytokine. (h) Incomplete inhibition of inflammatory and
proliferative process after the single intravitreal injection of carcinine concurrently with intravitreal ocular challenge of the rabbit eye
with the cytokine complex.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 17
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

cells of inflammatory infiltration, lymphocytes and
macrophages have been presented. The latter formed
conglomerates. In the cytoplasm of macrophages, the
grainy inclusions were detected during the accumula-
tion of these cells near the hemorrhage areas. The
significant inflammatory reaction occurred in the area
of the nervus opticus cup around its central vessels. A
combination of atrophic and proliferative processes was
also detected in the control cytokine complex-chal-
lenged eyes. Atrophic changes in the retina were noted
in the majority of cases and were significantly expressed
and localized predominantly in one half of the ocular
fundus.
In the atrophic areas, the retina was significantly
thinned because of the complete reduction in granular
layers. External and internal granular layers were fused
into one, the thickness of which was reached 1–2 rows of
nuclei. Topographically, such changes were localized
predominantly near the nervus optical disk or were
located at the peripheral retina. In the area of the retinal
atrophic changes, the sites of the retinal glyal substitu-
tion occurred.
PVR treatment with carcinine
Morphological investigations have shown the significant
inhibition of PVR in the group of eyes where carcinine
was applied in parabulbar injections (eight rabbit eyes)
started just after the intravitreal ocular challenge of the
rabbit eyes with the cytokine complex, and the parabul-
bar injections with carcinine were continued for 5 days
(five injections during 5 days and one injection daily).
The experimental clinical and morphological investiga-
tions revealed that the retina remained unchanged in all
such carcinine-treated cytokine-challenged animal eyes
compared with the cytokine-treated control. Inflamma-
tory effect was absent too. Carcinine showed the
remarkable preventive action and inhibition of PVR in
this treated group of eyes (see, Figure 10g).
Subconjunctival injections of carcinine were similarly
effective; however, more anti-inflammatory effect of
carcinine appeared after parabulbar injections than after
the single intravitreal administration of carcinine
compound. In the separate group of five rabbit eyes
treated with the single carcinine injection directly into the
vitreous cavity, the retina was conserved; however, there
was possible to find small zones of epiretinal membrane
formation. The inhibition of inflammatory and prolifera-
tive processes was incomplete in such cases (Figure 10h).
Thus, under the treatment with parabulbar injections
and intravitreal injection of carcinine, the distinct
inhibition of PVR was observed in the eyes challenged
with cytokine complex. The inhibitory effect of carcinine
on the PVR overall was more pronounced when it was
administrated at the early stages of pathologic process,
when the link with the inflammatory reaction mediated
by macrophages was a leading cell reaction component
of PVR. In general, upon the treatment with carcinine,
inflammatory processes were less exhibited and charac-
terized only by single lymphocytes, monocyte–macro-
phages adhered onto the internal boundary retinal
membrane (membrana limitans interna), sometimes in
the form of conglomerates. Atrophic changes were
absent at the big extension of the retina and occurred
in the single eyes (one eye) in the form of the single
hearth. The rest of the animals treated with carcinine
showed the intact retina with the intact internal
boundary membrane. Proliferative processes in the form
of epi- and subretinal membrane were completely absent
in the carcinine-treated group. The formation of very
thin one or two rows of the cell elements from epiretinal
membrane has occurred in one eye. In the contralateral
cytokine-challenged eye without treatment with carci-
nine, the massive cellular epiretinal membrane was
formed with 3-fold higher thickness than in the eyes
treated with carcinine. The experiments demonstrate the
clinico-morphological evidence for the inhibitory action
of the universal bioactivated antioxidant carcinine to
proliferative disorders. Based on the established biologic
activities of carcinine, the therapeutic effects on PVR
were because of the block of peroxide compounds and
reactions induced by macrophages in the vitreous cavity.
Apparently, macrophages lost their activity including
chemotaxis-induced cellular signaling and mitogenic
activities in most cases accompanied with proinflamma-
tory oxygen free radical species–mediated pathways and
a potent nitric oxide response [61].
Carcinine protection of photoreceptor cells from
light-induced damage
In photoreceptor cells, oxidative stress is induced by
exposure to bright light causing photoreceptor cell
damage and apoptosis [62]. Current thinking suggests
that ROS formed during oxidative stress can directly
attack polyunsaturated fatty acids (PUFAs) and initiate a
chain reaction that amplifies lipid peroxidation (LPO) in
cellular membranes. This causes a nonenzymatic PUFA
degradation into a variety of oxidized products, including
short- and medium-chain (hydroxy) aldehydes. 4-HNE,
one of the most abundant and the most toxic products of
LPO, is a mediator of the apoptotic response induced by
18 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

oxidative stress [63–66]. 4-HNE reacts with histidine,
cysteine, or lysine residues of proteins forming Michael
adducts [67]. This reaction leads to a variety of cyto-
pathologic effects, such as inhibition of enzyme activity;
inhibition of protein function; inhibition of protein, RNA,
and DNA synthesis; cell cycle arrest; and apoptosis
[66,68,69].
To test the protective effect of carcinine against light-
induced damage in photoreceptors, we performed intra-
vitreal injections of carcinine in wild type Balb/C mice,
followed by exposure to bright light, and quantified the
remaining photoreceptor cells (Figure 11). The ONL
thickness of mice raised in dim cyclic light is 50 lm as
previously published [70]. As shown in Figure 11, our
conditions of light exposure–induced apoptosis of 50–
60% of photoreceptor cells in the PBS-injected eye.
Carcinine significantly protected the other eye from light-
induced photoreceptor apoptosis, presumably through its
universal antioxidant and scavenging effect on 4-HNE
and other LPO products.
Oral administration and acute toxicity test of
carcinine in mice
The behavior, physiologic state, and death of the animals
were studied every day for 14 days following the
treatment of mice (females-5, males-5) with carcinine
chlorohydrate (posology 2 g/kg body mass) (Table III). It
was shown by the data that carcinine represents a
nontoxic product upon oral administration (LD0 > 2
g/kg).
Phase 2 randomized, double-masked, placebo-
controlled clinical trial of N-acetylcarnosine
lubricant eye drops
Sample characteristics
Table IV lists the demographic and ergonomic occupa-
tional characteristics of the cataract (n = 75) and no-
cataract groups (n = 74). Those with cataract were
similarly older on average with the no-cataract group of
subjects.
Both groups were split evenly between males and
females and had similar racial composition, with the
totality white population.
Table V lists the visual function for both groups
enrolled in the study and the distribution of visual
acuity and disability glare scores for subjects with
cataract and those without. As would be expected by
the case definition for cataract group membership, those
in the cataract group had impairments in visual function
as compared with the no-cataract group. This was true
for both the ‘worse’ and ‘better’ eyes. In addition, visual
acuity in the range of 20/35–20/50 and disability glare
readings in the range of glare radius more than 12 mm
was associated with driving difficulties (such as crash
involvement) (Table IV). Although not statistically sig-
nificant, there was also a possible relationship between
visual acuity worse than 20/50 and crashing during
driving experience [71]. Disability glare (glare radius
measured in millimeters) was correlated for statistical
significance with visual acuity at red and green targets at
baseline and 5- to 6-month examination interval in the
total samples of older subjects with cataract and no-
cataract older adult subjects (Table VI).
Older subjects enrolled in the study were divided into
two groups: treated with NAC and control group
(Tables VII–IX). Table VII lists the analogous and adjusted
analyses for the worse eye, which generated results in
the eyes with cataract upon treatment with NAC
prodrug ophthalmic formulation qualitatively similar to
those for the better eye. None of the baseline differences
between the different groups was significant. The two
groups were similar in smoking history, sunlight expo-
sure, and alcohol use. There was not any substantial
difference in the use of sunglasses, where the patients
lived or occupational hazard exposure between the two
groups.
Ophthalmic examinations indicated that the method-
ological variances of measurements were approximately
equal. Correlations of glare sensitivity at red vs. green
targets were significant (Table VI). Intraoperator corre-
lation coefficients obtained as repeated measurements for
each combination of operator, eye (right or left), and
glare radius (at red and green targets) were statistically
significant and presented earlier [6,7,45]. Overall,
the reproducibility for the one operator was good.
Tables VI–IX summarize the effects of study treatment
on VA and glare sensitivity over 9 months in older
subjects with cataract and no-cataract. In the control
placebo-treated group, comparison with baseline values
showed some variability of data in gradual worsening of
glare sensitivity at red and green targets and minimal VA
changes over 5–6 months (Table VIII). Glare sensitivity
indicated mostly changes in lens clarity and confirmed
the tiny changes in the optical media of the eye at the
short-term follow-up examinations when slit lamp–
associated image analysis, data, and densitometric
readings did not differ significantly with baseline
[6,7,12,13,45].
In the NAC-treated group, 5- to 6-month follow-up
generally showed an improvement in VA (according to
N-acetylcarnosine lubricant eye drops and carcinine for vision care 19
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

the distribution score of distance acuities in worse and
better eyes), and a significant improvement in glare
sensitivity at red and green targets was documented in
worse and better eyes using a critical cut point halometer
score (Tables VII and IX). VA was mostly improved in
older subjects with cataract in worse and better eyes, and
an improvement in glare sensitivity was found in both
older subjects with cataract and no-cataract older adult
subjects in worth and better eyes after 5–6 months of
treatment with NAC. The exampled images of cataract
reversal in older subjects are presented on the slit lamp
images just for note (see, Figure 12a–c).
The NAC-treated eyes had statistically significant
difference in VA and glare sensitivity compared with
the control group (P < 0.001) at 5- to 6-month time
point of treatment, as supported by the overall t-test
results of the ratio of the follow-up data to the baseline
values (Table IX). The previously published data illustrate
examinations over 24 months of the eyes treated with
NAC to show that the effect of treatment is sustainable
over more prolonged periods [6,7]. In the eyes of older
subjects with different localization and grade of cataract
and in no-cataract older adult subjects, short-term and
prolonged treatment with NAC did not seem to result in
(a)
(b)
OS
Dim cyclic light
Dim cyclic light
Inferior Superior60
50
40
30
ON
L th
ickn
ess
(µm
)
20
10
02.0 1.0 0 1.0 2.0
Bright light/carcinine
Bright light/carcinine
Bright light/PBS
Bright light/PBS
Distance from ONH (mm)
ISONL
OPL
INL
IPLGCL
Figure 11 Carcinine protects against light-induced oxidative stress and photoreceptor cell death in Balb/C mice. Mice were raised in dim
cyclic light for 8 weeks. Each mouse was injected in one eye with 1 lL phosphate-buffered saline (PBS) and in the other eye with 1 lL of 2 M
carcinine diluted in PBS. Mice were returned in dim cyclic light for 48 h before light damage was initiated. Light damage was then induced in
mice by 5 h exposure to 4000 lux of diffuse, cool, white fluorescent light. After light exposure, mice are returned in dim cyclic light for 7 days
to allow the retina to clear all dead cells and return to a well-organized morphology. (a) Representative histologic sections through the
inferior retina near the optic nerve head (ONH) are shown. The outer nuclear layer (ONL) thickness is indicated by arrows. (b) The thickness
of the ONL was measured at 0.24-mm intervals from the ONH to the inferior and superior ora serrata. Graph shows results from six mice, and
error bars indicate SEM. OS, photoreceptor outer segment; IS, photoreceptor inner segment; OPL, outer plexiform layer; INL, inner nuclear
layer; IPL, inner plexiform layer; GCL, ganglion cell layer.
20 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

a worsening of the visual outcome in this study and
elsewhere [15–19]. Topical short- or long-term admin-
istration of 1% NAC to the eye was well tolerated, with
no ocular or systemic adverse effects, no hyperemia of
conjunctival vessels, and no signs of allergy or other
toxic manifestations being reported. No clinically signif-
icant changes from baseline and no statistically signif-
icant differences between the treatment and control
groups were observed regarding ocular comfort and
ocular signs and symptoms (lack of burning and
stinging, blurred vision, ocular dryness, superficial
punctate keratitis, foreign body sensation, itching,
ocular discharge, ocular pain, tearing, ocular inflam-
mation, and photophobia). All patients completed the
study without any problems related to their allocated
treatment.
Table III Recapitulative table. Study of mortality and behavior
during the time following the intubation (D0) of carcinine within
14 days (D1–D14).
Days
Mortality
BehaviorMales Females
D0 0 0 N
D1 0 0 N
D2 0 0 N
D3 0 0 N
D4 0 0 N
D5 0 0 N
D6 0 0 N
D7 0 0 N
D8 0 0 N
D9 0 0 N
D10 0 0 N
D11 0 0 N
D12 0 0 N
D13 0 0 N
D14 0 0 N
Groups 0 0 N
N, normal.
Table IV Demographic and ergonomic occupational characteristics
of cataract and no cataract adult subjects enrolled in the study.
Cataract No Cataract
n % n %
Total 75 74
Age groups
54–59 years 16 21 24 32
60–69 years 25 34 37 50
70–85 years 34 45 13 18
Sex
Female 37 49 38 51
Male 38 51 36 49
Race White 75 100 White 74 100
Driving exposurea
Total 42 56 44 60
<150 km/week 25 59 19 43
‡150 km/week 17 41 25 57
Data are presented as numbers and percentages.aDriving subjects were classified into two categories according to whether
they drove more or less than the median number of km (150 km) driven per
week based on the distribution of all subjects. Although this was a self-report
measure, prior studies indicate that older adults can provide valid estimates
of driving exposure [12].
Table V Distribution of visual acuity and disability glare in the
cataract and no-cataract groups of the adult subjects enrolled in the
study at baseline examination.
Adult subjects
Cataract group
No cataract
group
n % n %
Total 75 74
Worse eye
Visual acuity
20/25 or better 7 9 53 71
20/25 to 20/30 16 21 12 16
20/35 to 20/50 47 63 5 7
Worse than 20/50 5 7 4 6
Disability glare readings (glare radius)
At red target
<12 mm 12 16 32 43
‡12 mm 63 84 42 57
At green target
<12 mm 10 13 34 46
‡12 mm 65 87 40 54
Better eye
Visual acuity
20/25 or better 14 19 56 76
20/25 to 20/30 33 44 11 15
20/35 to 20/50 23 31 4 5
Worse than 20/50 5 6 3 4
Disability glare readings (glare radius)
At red target
<12 mm 31 41 42 57
‡12 mm 44 59 32 43
At green target
<12 mm 21 28 35 47
‡12 mm 54 72 39 53
Normal measures of glare sensitivity of young subjects (20–30 years) with
best correction without cataracts are 3 ± 2 mm (mean ± SD) of at least four
measurements at red and green targets in the daytime [47].
N-acetylcarnosine lubricant eye drops and carcinine for vision care 21
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

We find that repurchase announcements during 5
recent years of follow give the credible figure in excess of
52 000 patients compliant using their Can-CTM eye
drops for published therapeutic indications (including
treatment of cataracts) and excellent safety on the daily
basis. We examine the factors influencing repurchase
behavior and find that repurchases in the latest quarters
are associated with a number of variables, including the
efficacy of the product and its persistent safety to control
the signs of glare sensitivity, cataract amelioration, and
quality of vision during the daily life activities.
The patented N-acetylcarnosine lubricant all-in-one
eye drops formula Can-CTM can provide beneficial results
for cataracts and recommendations for Rational Pre-
scribing with the following ophthalmic disorders and
visual disturbances in patients:
• Presbyopia [10].
• Open-angle primary glaucoma (in combination with
beta-blockers or prostaglandin derivatives, for example,
lumigan is instilled over night and Can-CTM is instilled as
adjunct therapy twice daily by 10 AM and 2 PM).
• Corneal disorders.
• Computer vision syndrome.
• Driving and night vision disability glare. Perceived
driving disability at night.
• Eyestrain.
• Ocular inflammation.
• Blurred vision.
• Dry eye syndrome.
• Retinal diseases.
• Vitreous opacities and lesions.
• Ocular complications of diabetes mellitus and other
systemic diseases.
• Contact lens difficulties, particularly with soft contact
lenses. (Not only do the lubricants in the Can-CTM
N-acetylcarnosine eye drop help to make wearing
contact lenses more comfortable, but N-acetylcarnosine
is also believed to reduce the build up of lactic acid in the
eye cornea, thus enabling the soft contact lens to be left
safely in the eye for longer).
Of the more than 51 408 patients who were enrolled
in the postmarket evaluation, the several classic various
types of cataracts under following classification (Table X)
are prescribed and delivered for the medical treatment of
eye diseases with the Can-CTM N-acetylcarnosine eye
drop therapeutic platform. The persons with best-
corrected vision of no <20/70 or better in the worse
eye are recommended for eye drop correction.
Nuclear cataracts included the following clinical
symptoms/history:
• Age.
• Occupation hazards.
• Cigarette smoking increases the risk of nuclear sclerosis.
Symptoms/history
• Gradual progressive loss of vision.
• Second sight – development of myopia owing to
increased lenticular refractive index.
• Monocular diplopia.
• Decreased color discrimination especially blue.
Clinical features
• Central yellow to brown discoloration of the lens.
• Myopic shift.
• Bilateral.
• Decreased penetration of cobalt blue slit beam through
lens.
Posterior subcapsular cataracts were characterized
with the following clinical features:
Epidemiology/risk factors
• Younger patients than with nuclear or cortical cata-
racts.
• Diabetes mellitus.
• Primary open-angle glaucoma.
• Radiation.
• Corticosteroids.
• Uveitis and retinitis pigmentosa.
• Smoking.
Symptoms/history
• Progressive loss of vision, sometimes rapid.
• Disability glare, halos.
• Monocular diplopia.
Table VI Linear correlation coefficients (R) between the character-
istics of older subjects with cataract and no-cataract older adult
subjects measured by visual acuities (VA) and glare radius (GR at
red and green targets) at baseline and at 5- to 6-month follow-up
ophthalmic examinations.
Parameter
Baseline study 5–6 months
VA
GR red
target
GR green
target VA
GR red
target
GR green
target
Older subjects with cataracta
VA X )0.61* )0.64* X )0.41 )0.58
GR red target X +0.81* X +0.84*
GR green target X X
Older adult no-cataract subjectsb
VA X )0.63* )0.68* X )0.44 )0.45
GR red target X +0.83* X +0.80*
GR green target X X
*P < 0.01.aNumber of eyes examined 75.bNumber of eyes examined 74.
22 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology
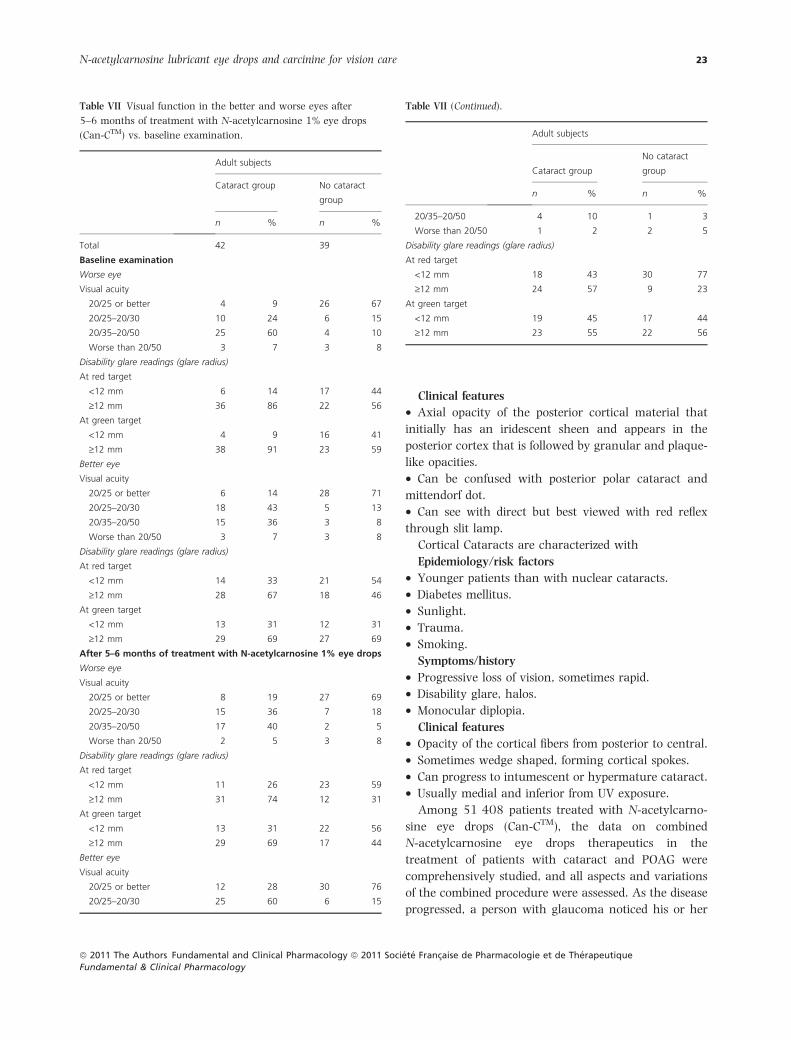
Clinical features
• Axial opacity of the posterior cortical material that
initially has an iridescent sheen and appears in the
posterior cortex that is followed by granular and plaque-
like opacities.
• Can be confused with posterior polar cataract and
mittendorf dot.
• Can see with direct but best viewed with red reflex
through slit lamp.
Cortical Cataracts are characterized with
Epidemiology/risk factors
• Younger patients than with nuclear cataracts.
• Diabetes mellitus.
• Sunlight.
• Trauma.
• Smoking.
Symptoms/history
• Progressive loss of vision, sometimes rapid.
• Disability glare, halos.
• Monocular diplopia.
Clinical features
• Opacity of the cortical fibers from posterior to central.
• Sometimes wedge shaped, forming cortical spokes.
• Can progress to intumescent or hypermature cataract.
• Usually medial and inferior from UV exposure.
Among 51 408 patients treated with N-acetylcarno-
sine eye drops (Can-CTM), the data on combined
N-acetylcarnosine eye drops therapeutics in the
treatment of patients with cataract and POAG were
comprehensively studied, and all aspects and variations
of the combined procedure were assessed. As the disease
progressed, a person with glaucoma noticed his or her
Table VII Visual function in the better and worse eyes after
5–6 months of treatment with N-acetylcarnosine 1% eye drops
(Can-CTM) vs. baseline examination.
Adult subjects
Cataract group No cataract
group
n % n %
Total
Baseline examination
42 39
Worse eye
Visual acuity
20/25 or better 4 9 26 67
20/25–20/30 10 24 6 15
20/35–20/50 25 60 4 10
Worse than 20/50 3 7 3 8
Disability glare readings (glare radius)
At red target
<12 mm 6 14 17 44
‡12 mm 36 86 22 56
At green target
<12 mm 4 9 16 41
‡12 mm 38 91 23 59
Better eye
Visual acuity
20/25 or better 6 14 28 71
20/25–20/30 18 43 5 13
20/35–20/50 15 36 3 8
Worse than 20/50 3 7 3 8
Disability glare readings (glare radius)
At red target
<12 mm 14 33 21 54
‡12 mm 28 67 18 46
At green target
<12 mm 13 31 12 31
‡12 mm 29 69 27 69
After 5–6 months of treatment with N-acetylcarnosine 1% eye drops
Worse eye
Visual acuity
20/25 or better 8 19 27 69
20/25–20/30 15 36 7 18
20/35–20/50 17 40 2 5
Worse than 20/50 2 5 3 8
Disability glare readings (glare radius)
At red target
<12 mm 11 26 23 59
‡12 mm 31 74 12 31
At green target
<12 mm 13 31 22 56
‡12 mm 29 69 17 44
Better eye
Visual acuity
20/25 or better 12 28 30 76
20/25–20/30 25 60 6 15
Table VII (Continued).
Adult subjects
Cataract group
No cataract
group
n % n %
20/35–20/50 4 10 1 3
Worse than 20/50 1 2 2 5
Disability glare readings (glare radius)
At red target
<12 mm 18 43 30 77
‡12 mm 24 57 9 23
At green target
<12 mm 19 45 17 44
‡12 mm 23 55 22 56
N-acetylcarnosine lubricant eye drops and carcinine for vision care 23
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

side vision gradually failing. That is, objects in front may
still be seen clearly, but objects to the side could be
missed. As glaucoma remains untreated, individuals
missed objects to the side and out of the corner of their
eye. Without treatment, individuals with glaucoma
slowly lost their peripheral (side) vision. Over time,
straight-ahead vision may decrease until no vision
remains. Applied N-acetylcarnosine eye drops therapy
has improved the success rate and reduced the compli-
cation rate previously associated with extracapsular
cataract extraction combined with trabeculectomy. A
Table VIII Visual function in the better and worse eyes after 5–
6 months of treatment with placebo (control group) vs. baseline
examination.
Adult subjects
Cataract group
No cataract
group
n % n %
Total
Baseline examination
33 35
Worse eye
Visual acuity
20/25 or better 3 9 27 77
20/25–20/30 6 18 6 17
20/35–20/50 22 67 1 3
Worse than 20/50 2 6 1 3
Disability glare readings (glare radius)
At red target
<12 mm 6 18 15 43
‡12 mm 27 82 20 57
At green target
<12 mm 6 18 18 51
‡12 mm 27 82 17 49
Better eye
Visual acuity
20/25 or better 8 24 28 80
20/25–20/30 15 46 6 17
20/35–20/50 8 24 1 3
Worse than 20/50 2 6 0 0
Disability glare readings (glare radius)
At red target
<12 mm 17 52 21 60
‡12 mm 16 48 14 40
At green target
<12 mm 8 24 23 66
‡12 mm 25 76 12 34
After 5–6 months of treatment with placebo
Worse eye
Visual acuity
20/25 or better 2 6 22 63
20/25–20/30 4 12 11 31
20/35–20/50 24 73 1 3
Worse than 20/50 3 9 1 3
Disability glare readings (glare radius)
At red target
<12 mm 4 12 13 37
‡12 mm 29 88 22 63
At green target
<12 mm 4 12 15 43
‡12 mm 29 88 20 57
Better eye
Visual acuity
20/25 or better 6 18 25 71
20/25–20/30 17 52 7 20
Table VIII (Continued).
Adult subjects
Cataract group
No cataract
group
n % n %
20/35–20/50 8 24 3 9
Worse than 20/50 2 6 0 0
Disability glare readings (glare radius)
At red target
<12 mm 15 45 18 51
‡12 mm 18 55 17 49
At green target
<12 mm 6 18 19 54
‡12 mm 27 82 16 46
Table IX Mean ± SD of changes (improvement) in visual functions.
Treatment group Visual acuity Glare radius
5- to 6-month follow-up of older subjects with cataract
Control group 0.79 ± 0.03 (n = 33) 1.58 ± 0.06 (n = 33)
NAC-treated group 1.65 ± 0.05*,** (n = 42) 0.38 ± 0.05* (n = 42)
5- to 6-month follow-up of older adult no-cataract subjects
Control group 0.91 ± 0.03 (n = 35) 1.37 ± 0.05 (n = 35)
NAC-treated group 1.21 ± 0.05* (n = 39) 0.49 ± 0.05* (n = 39)
The measure of visual acuity readings after 5–6 months of treatment was
divided by the clinical baseline measure of visual acuity for each eye
individually to get ratios, and then, the average of those ratios through each
clinical group of eyes was calculated. Similarly with glare, the calculation of
the ratio of glare sensitivity at red and green target after 5–6 months of
treatment to the baseline reading of glare sensitivity for each eye was made,
and then, the ratios were averaged through the whole groups of eyes.
NAC, N-acetylcarnosine (Can-CTM).
*P < 0.001 compared with control group who received placebo eye drops.
**P < 0.001, where an improvement in visual acuity is statistically signif-
icantly better in the group of older subjects with cataract than an
improvement in visual acuity in the group of older adult no-cataract subjects.
24 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

mean reduction in intraocular pressure (IOP) of 3–
7 mmHg was achieved. Can-CTM was recommended to
combine with another antiglaucoma medication, such as
beta-blocker treatment. Progressive loss of optic nerve
axons and retinal ganglion cells (RGCs) results in
characteristic optic nerve atrophy and visual field defects
in glaucoma patients. In many patients with glaucoma,
IOP is higher than the statistically normal limits; our
extensive evidence supports that elevated IOP-initiated
factors are important for the initiation and progression of
neuronal damage in these patients. Current therapeutic
management of glaucoma therefore aims to halt disease
progression by reducing elevated IOP. However,
although IOP lowering treatment can provide neuropro-
tection and retard the disease progression in many
glaucoma patients, it is not always sufficient to fully
prevent disease progression. This is a reason that our
recent efforts have been focused on the rational pre-
scription of alternative N-acetylcarnosine eye drops
treatment strategies for neuroprotection. In addition,
IOP is not elevated in all of the observed eyes exhibiting
characteristics of glaucomatous neurodegeneration.
(c)
(b)
(a)
1 2
Figure 12 (a) The pictures show the treatment of human cataract in the older subject with the patented by Innovative Vision Products, Inc
formula of 1% N-acetylcarnosine lubricant eye drops for the period of 5 months. The left image shows the appearance of cataract of a
76-years-old woman with opacified cortical layers, and the right image shows that this opacity has partially disappeared after the cited
period after treatment with N-acetylcarnosine is completed. The lens has become clearer. (b) Treatment of posterior subcapsular cataract
in the older subject for the period of 9 months with 1% N-acetylcarnosine lubricant eye drops. Left image – before treatment; right image –
after 9 months interval of treatment. The opalescence lens opacities areas are reversed, and the lens becomes clearer (look like dark greenish
zones) at the right image. (c) Treatment of cortical cataract in the upper segment of the pupil image of the older woman for the period
of 9 months. Upper image: the lens before treatment. Lower image- after 9 months of treatment with the 1% N-acetylcarnosine lubricant
eye drops. The appearance of rose reflex at the lower image demonstrates that the lens becomes clearer.
Table X Types of cataract treated with 1% N-acetylcarnosine
lubricant eye drops (Can-CTM) in population in excess of 51 408
patients.
Type Age of onset
Main clinical
symptoms (complaints)
Nuclear 60–72 Myopic shift
Blurred vision
Loss of blue/yellow
color perception
Posterior
subcapsular
40–63 Disability glare
Diminished reading
Monocular diplopia
Cortical 40–65 Disability glare
Monocular diplopia
N-acetylcarnosine lubricant eye drops and carcinine for vision care 25
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

Additional supportive evidence for oxidative stress dur-
ing glaucomatous neurodegeneration came from our
studies in glaucoma patients aided with N-acetylcarno-
sine eye drops (Can-CTM).
The N-acetylcarnosine lubricant eye drops have been
successfully used for medically oriented home health
care usually helping seniors recover or exercise with aid
in recovery from visual impairment or illness including
cataracts (Figure 13). At IVP, we are focused on provid-
ing patients with the selection and recommendation of
specialty home eye health care products and services for
vision and tailored to meet the specific needs for eye
health recovery and maintenance.
D I S C U S S I O N
The overarching aim of eye-care and vision-related
rehabilitation programs is to improve the quality of life
of visually impaired individuals, but resources for these
programs are limited [72]. Vision impairment has a
significant impact on length and quality of life [73,74].
Difficulty with daily activities as a result of impaired
vision is commonly reported by older adults and often
does not correlate well with clinical measures of vision or
ability to perform specific tasks [75–77]. Previous
research has shown that vision impairment is associated
with an increased risk of falls, hip fractures, depression,
social isolation, greater need for community services,
and greater risk of admission to nursing homes [73,78].
The age- and sex-standardized 7-year cumulative mor-
tality rate was 26% among persons with any visual
impairment and 16% in persons without visual impair-
ment. After adjusting for factors found significantly
associated with mortality, including age, male sex, low
self-rated health, low socioeconomic status, systemic
medical conditions, and negative health risk behaviors,
the presence at baseline of any visual impairment was
independently associated with increased mortality risk
[risk ratio (RR), 1.7; 95% confidence interval, 1.2–2.3].
The presence of age-related cataract, either nuclear (RR,
1.5), cortical (RR, 1.3), or posterior subcapsular cataract
(RR, 1.5), was also significantly associated with
increased mortality risk. These associations remained
statistically significant when visual impairment and each
type of cataract were included simultaneously in the
multivariate Cox model [79].
Nursing homes have changed dramatically over the
past several decades. These changes have been driven by
government regulations and consumer pressures.
Today’s nursing homes are highly regulated, high-
quality institutions for the care and treatment of older
adults who have severe physical health and/or mental
disabilities. Almost half of all individuals who live in
nursing homes are 85 years or older. Relatively few
residents are younger than 65 years. Most are women
(72%), many of whom are without a spouse (60%
widowed) and with only a small group of family
members and friends for support. Some type of disability
or impairment with activities of daily living (ADLs) is the
most common reason that older individuals live in
nursing homes. In the absence of any preventive
measures that can be applied in a public health setting,
the only recourse is surgery. This work intends to
demonstrate that it is possible in a developing country
setting to establish self-sustaining, high-quality home
eye care that is affordable and accessible to poor people
for the community global vision strategy.
The cost-effectiveness and safety of the NAC lubricant
eye drops developed and applied for medical cataract
therapy has been demonstrated [17,18]. In addition to
the restoration of sight, there is an enhancement of the
quality of life in the developing world using available
N-acetylcarnosine ophthalmic therapeutic technology
[16–19].
Use of NAC to treat cataract and aging lens can lead to
diminishing of light scattering units in the lens which
raise glare effect, probably by prevention of the oxidative
modification of crystallins and utilization of lipid perox-
ides [8,9]. After 5–6 months, the worse and better eyes
of older adult subjects and older subjects with cataract
treated with 1% NAC generally showed an improvement
Figure 13 The Innovative Vision Products, Inc. patented Vision
products’ initiatives honor and recognize the exceptional efforts of
homecare, hospice, and private duty providers across the globe
actively engaged in strategic initiatives to improve quality of vision
care and organizational performance.
26 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

in visual functions as compared with baseline. The
results of glare testing show a reduction in light
scattering in the worse and better eyes of older drivers.
Glare sensitivity improvement was accompanied by
improvement in VA more pronounced in the eyes with
cataract during treatment with NAC. The data of visual
functions (VA and glare sensitivity) in older adult
subjects and older subjects with cataract treated with
1% NAC showed significant improvement as compared,
in contrast to the control group that showed generally
no improvement in visual functions, with no difference
from baseline in VA and glare sensitivity readings. In
most of the patients treated, study treatment was well
tolerated, and no ocular or systemic adverse events were
reported.
NAC releases carnosine for intraocular uptake and
systemic absorption, which acts as a vision sensory input
signaling molecule and locally in the lens as universal
antioxidant both in the lipid phase of the cellular lens
membranes and in their aqueous environment and
protects the crystalline lens from oxidative stress-induced
damage [8,9,17]. The treatment with NAC is improving
eyesight in older adult cataract-free patients as
L-carnosine promotes vision sensory input through the
activation of the histamine-containing neurons in the
tuberomammillary nucleus of the hypothalamus.
Besides, the intraocular released carnosine promoted
by specific ophthalmic formulation including muco-
adhesive compound carboxymethylcellulose and corneal
absorption promoters reacts with oxygen radicals, LPO
products, and carbohydrate oxidation products accumu-
lated in the crystalline human lens with aging [8,9].
When cataract was accompanied with POAG, 1% NAC
prodrug was prescribed 15 min prior the topical appli-
cation of beta-blocker, specifically used to decrease the
IOP.
The entire body of supporting research on N-acetyl-
carnosine and its bioactivated principle carnosine reveals
its promise as a water-soluble universal antioxidant that
works at several levels to defend against the oxidative
stresses to the lens, glycosylation problems, and protect
the lens proteins and the membrane lipids from oxidative
damages thus preventing and reversing age-related
cataracts in human eyes. The presented results can be
explained in part by the adduction of the various LPO
products directly by carnosine following de-acetylation of
N-acetylcarnosine. The ability of L-carnosine to inhibit
LPO reactions as well as to diminish the content of LPO
products makes N-acetylcarnosine applied with lubricant
carboxymethylcellulose a prominent tool in the therapy
especially, of the posterior subcapsular and cortical
cataracts, whose mechanism can be related with the
toxic effects of LPO products [80].
The most prevalent age-related ocular diseases are
macular degeneration, open-angle glaucoma, cataract,
and diabetic retinopathy [81,82]. There are several
clinical types of PVR: proliferative diabetic retinopathy,
PVR following rhegmatogenous retinal detachment,
and posttraumatic PVR. PVR occurs after rhegmato-
genous retinal detachment, perforating injury to the
posterior segment of the eye, and retinal detachment
surgery [83]. It is the leading cause of failure in retinal
detachment surgery and is characterized by the
formation of proliferating fibrocellular membrane on
both sides of retinal surfaces and in the vitreous
cavity. Further contraction of the fibrocellular mem-
brane causes tractional retinal detachment (TRD). RPE
cells, fibroblasts, glial cells, macrophages, and myo-
fibroblast-like cells are found in the proliferating
membrane [84].
They are surrounded by various amounts of extracel-
lular matrix (ECM), including collagen, fibronectin,
vitronectin, and laminin [85,86]. PVR is the leading
cause of failure after retinal detachment surgery.
With the advancement of vitreoretinal surgery, the
prognosis of PVR has been improved. Long-term success,
however, often is prevented by the recurrence of
proliferative contractile membranes [87]. Repeated sur-
gery often exacerbates the inflammatory reaction within
the vitreous cavity. Pharmacologically, various drugs,
including antimetabolites, colchicine, and steroids, have
been tested as potential therapeutic agents for the
treatment of PVR [88]. However, many of the cited
inhibitors of cellular proliferation have side effects that
are toxic to the eye. Thus, further understanding the
pathogenesis of PVR and searching for more appropriate
and effective therapeutic agents are critical.
This pilot study suggests that parabulbar, subconjunc-
tival, or intravitreal injection of carcinine with most of
the vehicle removed is not toxic to intraocular struc-
tures, reduces postoperative intraocular inflammation,
and may be a potentially useful additional tool in the
treatment of PVR as well as can be considered as the
antiapoptotic drug for the protection of photoreceptor
cells from oxidative light-induced stress.
Preliminary publications about photoprotector and
antioxidant activities of carcinine have been issued
[16,21,43,89–92]. Carcinine is resistant to hydrolysis
with natural enzymatic systems. Our study shows the
reactivity of carcinine with ROS and aldehyde products
N-acetylcarnosine lubricant eye drops and carcinine for vision care 27
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

[43,89,91]. Carcinine noticeably limits 4-HNE-induced
cross-linking of collagen. For comparison, vitamin E
(lypophilic antioxidant) is not active against this type of
toxic agent. Aminoguanidine is also not efficient in
protection from the aldehyde-induced cross-linking of
collagen. Carcinine is acting as the universal antioxidant
and transition metal and heavy metal ions chelating
agent. It exerts the revival of the enzymatic superoxide
dismutase (SOD) activity in tissues following the expo-
sure with UV or glycation reactions [43,89,91]. Carci-
nine acts as an efficient water-soluble scavenger of
oxygen-derived free radicals and is also able to inhibit
metal-catalyzed free radical oxidation of lipids
[16,21,43,89–92].
The critical role of mitochondria in programmed cell
death leads to the design of mitochondriotropic agents as
a strategy in regulating apoptosis. Recently, phospho-
lipid peroxidation products gained a reputation as key
regulatory molecules and participants in oxidative
signaling pathways. Oxidation of two anionic phospho-
lipids – cardiolipin (CL) in mitochondria and phospha-
tidylserine (PS) in extramitochondrial compartments – is
important signaling event, particularly during the exe-
cution of programmed cell death and clearance of
apoptotic cells. Quantitative analysis of CL and PS
oxidation products is central to understanding their
molecular mechanisms of action [93,94]. Furthermore,
specific characteristics of CL in mitochondria – –its
asymmetric transmembrane distribution and mecha-
nisms of collapse, the regulation of its synthesis, remod-
eling, and fatty acid composition – are given significant
consideration [94,95]. Cytochrome c (cyt c) acts as a CL-
specific peroxidase very early in apoptosis. At this stage,
the hostile events are still secluded within the mitochon-
dria and do not reach the cytosolic targets. CL oxidation
process is required for the release of proapoptotic factors
into the cytosol. Manipulation of cyt c interactions with
CL, inhibition of peroxidase activity, and prevention of
CL peroxidation are prime targets for the discovery of
antiapoptotic drugs acting before the ‘point-of-no-return’
in the fulfillment of the cell death program.
During apoptosis, a mitochondria-specific phospho-
lipid, CL, interacts with cytochrome c (cyt c) to form a
peroxidase complex that catalyzes CL oxidation; this
process plays a pivotal role in the mitochondrial stage of
the execution of the cell death program. Several works
were focused on redox mechanisms and essential struc-
tural features of cyt c’s conversion into a CL-specific
peroxidase that represent an interesting and may be still
unique example of a functionally significant ligand
change in hemoproteins [93,94]. Recently, it was
demonstrated that peroxidase cyt c/CL complexes can
utilize free fatty acid hydroperoxides (FFA-OOH) at
exceptionally high rates that are approximately three
orders of magnitude higher than for H2O2 [93].
Accordingly, the new concepts in drug discovery based
on the design of mitochondria-targeted inhibitors of cyt
c/CL peroxidase and CL peroxidation with antiapoptotic
effects have appeared. Therefore, mitochondria-targeted
disruptors and inhibitors of cyt c/CL peroxidase com-
plexes and suppression of CL peroxidation represent new
strategies in antiapoptotic drug discovery [96].
We have originally discovered that both carnosine and
carcinine (10–25 mM) are capable of inhibiting the
catalysis of linoleic acid and phosphatidylcholine
liposomal peroxidation by the O2)•-dependent iron-
ascorbate- and lipid-peroxyl-radical-generating linoleic
acid 13-monohydroperoxide (LOOH)-activated hemo-
globin systems, as measured by thiobarbituric-acid-
reactive substance. Carcinine and carnosine are good
scavengers of OH· radicals, as detected by iron-depen-
dent radical damage to the sugar deoxyribose. This
suggests that carnosine and carcinine are able to
scavenge free radicals or donate hydrogen ions. The
iodometric, conjugated diene and t.l.c. assessments of
lipid hydroperoxides (13-monohydroperoxide linoleic
acid and phosphatidylcholine hydroperoxide) showed
their efficient reduction and deactivation by carnosine
and carcinine (10–25 mM) in the liberated and bound-
to-artificial-bilayer states. This suggests that the perox-
idase activity exceeded that susceptible to direct reduc-
tion with glutathione peroxidase. Imidazole, solutions of
beta-alanine, or their mixtures with peptide moieties did
not show antioxidant potential [21]. Because of the
combination of weak metal chelating (abolished by
EDTA), OH• and lipid-peroxyl-radicals-scavenging, and
reducing activities to liberated fatty acid and phospho-
lipid hydroperoxides, carnosine and carcinine appear to
be physiologic antioxidants able to efficiently protect the
lipid phase of biologic membranes and aqueous environ-
ments and act as the antiapoptotic natural drug com-
pounds.
The unwanted proliferation of intraocular tissue, such
as vascular retinal cells in eyes with ischemic retino-
pathies, subretinal neovascular tissue in eyes with
exudative age-related macular degeneration, and retinal
pigment epithelium cells in the case of PVR, is one of the
important problems still mostly unsolved in clinical
ophthalmology. Based on clinically oriented experimen-
tal observations and pathogenic considerations provided
28 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

in this study, we have originally suggested that a single
intravitreal injection or several parabulbar injections of
carcinine can locally suppress intraocular inflammation
and proliferation of cells, especially during the modeling
of PVR. Further provided clinical studies (data not
shown) have correspondingly revealed that a single
intraocular injection of carcinine may be a therapeutic
option as adjunctive treatment of exudative age-related
macular degeneration, diabetic cystoid macular edema,
and proliferative diabetic retinopathy.
Although the retina has a remarkable capacity for
morphological and biochemical adaptation to different
environmental luminances, prolonged light exposure
can cause photoreceptor cell damage by nonthermal
mechanisms. It is now clear that light damage involves a
complex series of events that depend on light intensity
[96–98], duration [99,100], and wavelength [101] and
on the distribution of absorbing chromophores in the
retina [102,103]. As it was suggested that light induces
oxidative reactions that result in damage to the photo-
receptor cells, [104] evidence that LPO occurs in the
retina in response to light has gradually accumulated.
An increase in the level of peroxides in rod outer segment
(ROS) extracts [105] and specific loss of docosahexaenoic
acid (22 : 6) from ROS membranes [106] have been
measured after exposure to an intense light. The
hypothesis that oxygen free radicals mediate LPO [107]
has been confirmed in vivo by several investigators
[106,108–110].
Oxygen radicals are generated through a series of
reactions (including the Haber-Weiss and Fenton reac-
tions) [111] that produce the hydroxyl radical (•OH),
which then initiates LPO. The vertebrate retina is very
vulnerable to free radical assault because it contains
high levels of polyunsaturated fatty acids, which are
choice substrates for peroxidation [112]; it consumes
much oxygen compared with other tissues [113], and it
acts as a light processor, which initiates the formation of
free radicals [114].
In this study, the authors have determined through
histologic measurements that carcinine is also effective
in reducing retinal light damage in mice. Unfortunately,
these studies provide no insight on the functional
survival of photoreceptor cells, and the question arises
whether the anatomic rescue of photoreceptors is
accompanied by preservation of the retinal function. In
this study, we have made use of the model of retinal
photodegeneration we had developed. The further clin-
ical analysis of the protective effects of oral carcinine
against retinal degeneration revealed that the observed
carcinine protection of photoreceptor cells from oxidative
stress is morphometric and functional.
Carcinine is indicated for administration as a phar-
maceutical drug in the injection formulation (subcon-
junctival, ocular parabulbar, and intravitreous
injections).
Carcinine is suitable for the systemic administration
(per oss) for ophthalmic and CNS pharmaceutical indi-
cations. This is supported by the fact that carcinine is
only slightly affected by the enzymatic hydrolysis with
natural peptidases [89–91]. The lack of the oral acute
toxicity of carcinine introduces the experimental proof
for this regular oral therapeutic application modality.
The oral therapeutic administration of carcinine and its
bioavailability in patented by IVP oral formulations
thereof have been supported in the matched studies
[115].
In the previous studies, the authors have determined
through histologic measurements that carcinine, a
decarboxylated carnosine natural derivative, is also
effective in reducing retinal light damage in mice
[10,89–91,116]. The further clinical analysis of the
protective effects of lubricant carcinine eye drops against
retinal degeneration revealed that the observed carcinine
protection of photoreceptor cells from oxidative stress is
morphometric and functional. This is supported by the
fact that carcinine is only slightly affected by the
enzymatic hydrolysis with natural peptidases [10,89–
91,115,116]. The lack of the acute toxicity of carcinine
introduces the experimental proof for this regular ocular
topical therapeutic application modality. The therapeutic
administration of carcinine with lubricant eye drops and
its bioavailability in patented by IVP eye drop lubricant
formulations thereof have been supported in the
matched studies [10,89–91,116]. In the previous stud-
ies, we have also presented a growing evidence that
demonstrates the ability of N-acetylcarnosine (lubricant
eye drops) or natural pseudodipeptide carcinine
(b-alanylhistamine) to act as pharmacological chaper-
ones [117–119]; these beta-alanine-containing chaper-
ones can decrease oxidative stress and ameliorate
oxidative and excessive glycation stress-related eye
disease phenotypes, suggesting that the field of chaper-
one therapy might clinically benefit novel treatments for
age-related cataracts, age-related macular degeneration
(AMD), and ocular complications of diabetes (OCD).
Molecular chaperones induced by L-carnosine or carci-
nine antiapoptotic ophthalmic therapeutics facilitate and
regulate protein conformational change within cells.
This encompasses many fundamental cellular processes:
N-acetylcarnosine lubricant eye drops and carcinine for vision care 29
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

including the correct folding of nascent chains; protein
transport and translocation; and signal transduction and
protein quality control. Imidazole-containing peptidom-
imetics acting as pharmacological chaperones are
important in several forms of human disease, including
age-related cataracts and neurodegeneration. Within the
retina, the highly specialized photoreceptor cell presents
a fascinating paradigm to investigate the specialization of
molecular chaperone function and reveals unique chap-
erone requirements including the transglycating activity
of carcinine essential to photoreceptor function [117–
119]. Exploiting natural peptide diversity: imidazole-
containing pharmacological chaperone molecules was a
one driving factor that led IVP pharmacologists in
cooperation with alliance groups to develop scientifically
proven grooming ophthalmic drug products for oral,
intravitreal administration, or topical lubricant eye drops
drug formulations with active ingredients characterized
by interaction to other proteins and mediating their
folding, transport, and interaction with other molecules,
LPO products and membranes. Our research group has
revealed that toxic aldehydes, such as 4-HNE, are
produced in photoreceptor cells by LPO, induced during
exposure to bright light. If not detoxified, they disrupt
photoreceptor functions and induce apoptosis. The
naturally occurring dipeptide-based compounds either
L-carnosine or carcinine have been shown to quench
4-HNE, forming specific adducts [16]. Specifically, we
investigated whether carcinine, a decarboxylated
derivative of L-carnosine offering the advantage of being
more resistant to enzymatic hydrolysis with endogenous
peptidases, had the same ability to quench 4-HNE,
therefore protecting against its toxic effects. Our exper-
iments were conducted in cultured cells and in mice. The
photoreceptor cell line 661W was preincubated with 0,
2, and 20 mM carcinine for 2, 4, 6, and 24 h. After
removing and washing extracellular carcinine, cells were
treated with increasing concentrations of 4-HNE over-
night, and cell death was quantified using an LDH assay.
Balb/C mice were injected intravitreally with carcinine in
one eye and PBS in the other eye. Two days after
injection, mice were exposed to bright light (4000 lux for
5 h) to induce oxidative stress and endogenous produc-
tion of 4-HNE. Protection of photoreceptors by carcinine
was quantified by histology. We found that carcinine
protects 661W cells against 4-HNE-induced apoptosis in
a time- and dose-dependent manner. This suggests that
carcinine can be transported inside the cells and quench
4-HNE [16]. The earlier established by our group lipid
peroxidase and transglycating free-radical-scavenging
activities of carcinine propose the capacity of carcinine
to act as the antiapoptotic drug and mitochondria-
targeted disruptor and inhibitor of cyt c/CL peroxidase
complexes and suppressor of CL peroxidation [16,117–
119]. Carcinine does not protect when preincubated
<6 h, suggesting an additional mechanism of induction
of protective genes, or chaperone proteins, an effect
reported recently with another Zn carnosine derivative.
Carcinine significantly protected photoreceptors against
light-induced apoptosis, suggesting that this compound
is sufficiently resistant to degradation and can be used in
vivo representing new strategies in antiapoptotic
ophthalmic drug discovery. The biologic properties of
carcinine offer a potential treatment strategy for a wide
range of eye diseases linked to oxidative damage. For
example, we have shown that the photoreceptor-specific
enzyme RDH12 offers endogenous protection against
4-HNE. In absence of a functional RDH12 gene, an early
onset congenital vision loss develops. We will further
explore possibilities of replacing the disrupted activity of
RDH12 with a similar functioning molecule such as
carcinine [16,117–119].
C O N C L U S I O N
There is a growing trend worldwide to evaluate cataract
disease and disability prevention on the basis of costs
incurred and benefits accrued. Public health interven-
tions to prevent blindness are particularly revealing in
this respect, as cost savings and return on investment
accrue, because of the avoided rehabilitative costs, on
the one hand, and the gains in productivity, on the
other. Accurate data on the total economic and social
costs of blindness and severe visual impairment are not
available. Moreover, the cost estimates vary widely from
country to country, based on the prevalence and causes
of blindness, the age of those affected, the employment
situation in the country concerned, the wage structure,
and the existence and coverage of social, rehabilitative,
and educational services. However, in every country,
such costs have been shown to be a considerable strain
on the national economy. In 1990, the aggregated cost
of blindness to the federal budget in the United States
was estimated to be approximately US$4.1 billion. A
minimal federal budgetary cost of a person-year of
blindness (vision <6/60 in the better eye) for a working-
age adult was estimated to be US$11 896.
More importantly, it has been estimated that in the
United States, if all the avoidable blindness in persons
under 20 and working-age adults were prevented, a
30 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

potential saving of US$1.0 billion per year would accrue
to the federal budget. In a study from India in 1989, a
conservative estimate of the aggregated costs of blind-
ness to the national economy, including a minimal
subsistence allowance for the blind, amounted to
approximately US$4.6 billion per year. The economic
burden of blindness and visual impairment is only part of
the story. The person who is blind and his/her family
face important social constraints. Both directly and
indirectly, visual impairment interferes with various
activities of daily living. Blind children have to face
developmental challenges. In adult life, employment
opportunities for the visually disabled are extremely
limited, and their participation in a host of leisure
activities is seriously hampered. In addition, in many
societies, visual impairment results in a loss of status and
self-esteem. These physical and, especially, the psycho-
social implications of visual impairment and blindness
cannot be accurately quantified in monetary terms.
However, they do erode the quality of life of both the
affected individuals and their families. Our study in the
UK indicated that visually disabled individuals were
poorer on average and had lower educational levels,
lower employment, and less social life than sighted
individuals.
These findings probably hold true in all societies. Also,
in African settings, it has been reported that blind persons
die earlier compared with the sighted population. The
Nepal blindness survey showed that life expectancy of
blind individuals was 3 years. Cataracts are the most
common cause of avoidable blindness. Worldwide, there
are an estimated 16 million persons who are blind as a
result of cataracts. The majority of these individuals live in
the rural areas of economically developing countries. The
burden on the country is significant.
In this study, we present the evidence that N-acetyl-
carnosine lubricant eye drops globally patented by IVP
have now reached clinical trials and showed encourag-
ing results as anticataract drug or medical device (CE-
marked product) that warrant further investigation. The
discovery of naturally occurring carnosine derivatives:
N-acetylcarnosine and carcinine as effective medical
treatment for sight-threatening eye disorders, such as
cataract, PVR, macular degenerations, POAG, and
ocular complications of diabetes is likely to make global
impact on eye health. The current aims of this paper are
to introduce the updated data on the drug therapy of
cataract with N-acetylcarnosine lubricant eye drops, on
the carcinine treatment of experimental PVR, to cover
the carcinine protection of photoreceptor cells from the
light-induced damages, and to provide updates of the
latest development.
A C K N O W L E D G E M E N T S
This work was planned, organized, and supported by
IVP. Innovative Vision Products, Inc. is a holder of the
worldwide patent (including PCT International Publica-
tion Number WO 2004/028536 A1) for the application
of N-acetylcarnosine for the Treatment of ophthalmic
disorders, including cataracts as well as (PCT Interna-
tional Publication Number WO 2004/064866 PCT/
JP2004/000351) protecting the described in the article
therapeutic applications. The biologically significant
applications of carnosine mimetics including those in
ophthalmology were patented by Dr. Babizhayev and
the alliance Groups (WO 2004/028536 A1; WO 94/
19325; WO 95/12581; WO 2004/064866 A1). Inno-
vative Vision Products Inc. is a Pharmaceutical and
Nanotechnology Development Company with a focus on
innovative chemical entities, drug delivery systems, and
unique medical devices to target specific biomedical
applications. Over the last decade, IVP has developed a
track record in developing these technologies to effec-
tively address the unmet needs of specific diseased
populations.
C O N F L I C T O F I N T E R E S T
Declaration of interest: The authors report the interest in
the Intellectual Property of the described modalities
protected with the patents. The authors bear primary
responsibility for accuracy of made statements and
employment of the described products and for the
content and writing of the paper.
R E F E R E N C E S
1 Resnikoff S., Pascolini D., Etya’ale D. et al. Global data on
visual impairment in the year 2002. Bull. World Health
Organ. (2004) 82 844–851. Epub 2004 Dec 14.
2 Dandona R., Dandona L. Socioeconomic status and blindness.
Br. J. Ophthalmol. (2001) 85 1484–1488.
3 Congdon N., O’Colmain B., Klaver C.C. et al. Causes and
prevalence of visual impairment among adults in the United
States. Arch. Ophthalmol. (2004) 122 477–485.
4 Marrelli T.M.. Handbook of home health standards and
documentation guidelines for reimbursement, 2nd edn.
Mosby, St Louis, 1994.
5 Yorston D. Cataract complications. Commun. Eye Res. J.
(2008) 65 1–3.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 31
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

6 Babizhayev M.A., Deyev A.I., Yermakova V.N. et al. N-acetyl-
carnosine, a natural histidine-containing dipeptide, as a potent
ophthalmic drug in treatment of human cataracts. Peptides
(2001) 22 979–994.
7 Babizhayev M.A., Deyev A.I., Yermakova V.N. et al. Efficacy of
N-acetylcarnosine in the treatment of cataracts. Drugs R. D.
(2002) 3 87–103.
8 Babizhayev M.A., Deyev A.I., Yermakova V.N., Remenschikov
V.V., Bours J. Revival of the lens transparency with
N-acetylcarnosine. Curr. Drug Ther. (2006) 1 91–116.
9 Babizhayev M.A., Deyev A.I., Yermakova V.N., Brikman I.V.,
Bours J. Lipid peroxidation and cataracts: N-acetylcarnosine
as a therapeutic tool to manage age-related cataracts in
human and in canine eyes. Drugs R. D. (2004) 5 125–139.
10 Babizhayev M.A. (2004) Method for topical treatment of eye
disease and composition and device for said treatment. PCT
Patent Application. International Publication Number WO
2004/028536 A1. International Publication Date: 8 April
2004.
11 Babizhayev M.A. Ophthalmic pharmacology of N-acety-
lcarnosine lubricant eye drops. J. Pharmacol. Toxicol. (2006)
1 201–233.
12 Babizhayev M.A.. Rejuvenation of visual functions in older
adult drivers and drivers with cataract during a short-term
administration of N-acetylcarnosine lubricant eye drops.
Rejuvenation Res. (2004) 7 186–198.
13 Babizhayev M.A., Yermakova V.N., Deyev A.I., Seguin M.-C.
Imidazole-containing peptidomimetic NACA as a potent drug
for the medicinal treatment of age-related cataract in humans.
J. Anti-Aging Med. (2000) 3 43–62.
14 Babizhayev M.A., Yermakova V.N., Sakina N.L., Evstigneeva
R.P., Rozhkova E.A., Zheltukhina G.A. Na-Acetylcarnosine is
a prodrug of L-carnosine in ophthalmic application as
antioxidant. Clin. Chim. Acta (1996) 254 1–21.
15 Babizhayev M.A., Guiotto A., Kasus-Jacobi A. N-Acetylcarno-
sine and histidyl-hydrazide are potent agents for multitargeted
ophthalmic therapy of senile cataracts and diabetic ocular
complications. J. Drug Target. (2009) 17 36–63.
16 Babizhayev M.A., Kasus-Jacobi A. State of the art clinical
efficacy and safety evaluation of N-acetylcarnosine dipeptide
ophthalmic prodrug. Principles for the delivery, self-bioacti-
vation, molecular targets and interaction with a highly
evolved histidyl-hydrazide structure in the treatment and
therapeutic management of a group of sight-threatening eye
diseases. Curr. Clin. Pharmacol. (2009) 4 4–37.
17 Babizhayev M.A., Micans P., Guiotto A., Kasus-Jacobi A.
N-acetylcarnosine lubricant eyedrops possess all-in-one uni-
versal antioxidant protective effects of L-carnosine in aqueous
and lipid membrane environments, aldehyde scavenging, and
transglycation activities inherent to cataracts: a clinical study
of the new vision-saving drug N-acetylcarnosine eyedrop
therapy in a database population of over 50,500 patients. Am.
J. Ther. (2009) 16 517–533.
18 Babizhayev M.A., Burke L., Micans P., Richer S.P. N-Acetyl-
carnosine sustained drug delivery eye drops to control the
signs of ageless vision: glare sensitivity, cataract amelioration
and quality of vision currently available treatment for the
challenging 50,000-patient population. Clin. Interv. Aging.
(2009) 4 31–50. Epub 2009 May 14.
19 Babizhayev M.A. Current ocular drug delivery challenges for
N-acetylcarnosine: novel patented routes and modes of deliv-
ery, design for enhancement of therapeutic activity and drug
delivery relationships. Recent Pat. Drug Deliv. Formul. (2009)
3 229–265.
20 Gulewitsch W., Amiradzibi S. Uber das carnosin, eine neue
organische Base des Fleischextraktes. Ber. Deutch. Chem. Ges.
(1900) 33 1902–1903.
21 Babizhayev M.A., Seguin M.-C., Gueyne J., Evstigneeva R.P.,
Ageyeva E.A., Zheltukhina G.A. L-Carnosine (b-alanyl-L-
histidine) and carcinine (b -alanylhistamine) act as natural
antioxidants with hydroxyl-radical-scavenging and lipid per-
oxidase activities. Biochem. J. (1994) 304 509–516.
22 Severin S.E. Problems concerned with the biological activity of
naturally occurring imidazole compounds. Proceedings of
Plen. Sess. Seventh International Biochemical Congress 1964,
NY, pp. 45–61.
23 Boldyrev A.A., Severin S.E. The histidine-containing dipep-
tides, carnosine and anserine: distribution, properties and
biological significance. Adv. Enzyme Regul. (1990) 30 175–
194.
24 Lenney J.F. Specificity and distribution of mammalian carno-
sinase. Biochim. Biophys. Acta (1976) 429 214–219.
25 Jackson M.C., Kucera C.M., Lenney J.F. Purification and
properties of human serum carnosinase. Clin. Chim. Acta
(1991) 196 193–205.
26 Lenney J.F. Separation and characterization of two carnosine-
splitting cytosolic dipeptidases from hog kidney (carnosinase
and non-specific dipeptidase). Biol. Chem. Hoppe Seyler (1990)
371 433–440.
27 Kunze N., Kleinkauf H., Bauer K. Characterization of two
carnosine-degrading enzymes from rat brain. Partial
purification and characterization of a carnosinase and a
beta-alanyl-arginine hydrolase. Eur. J. Biochem. (1986) 160
605–613.
28 Boldyrev A.A., Dupin A.M., Bunin A.Ya., Babizhayev M.A.,
Severin S.E. The antioxidative properties of carnosine, a
natural histidine containing dipeptide. Biochem. Int. (1987)
15 1105–1113.
29 Aldini G., Facino R.M., Beretta G., Carini M. Carnosine and
related dipeptides as quenchers of reactive carbonyl species:
from structural studies to therapeutic perspectives. Biofactors
(2005) 24 77–87.
30 Aldini G., Orioli M., Carini M., Maffei Facino R. Profiling
histidine-containing dipeptides in rat tissues by liquid chro-
matography/electrospray ionization tandem mass spectrome-
try. J. Mass Spectrom. (2004) 39 1417–1428.
31 Orioli M., Aldini G., Beretta G., Facino R.M., Carini M. LC-ESI-
MS/MS determination of 4-hydroxy-trans-2-nonenal Michael
adducts with cysteine and histidine-containing peptides as
early markers of oxidative stress in excitable tissues. J.
Chromatogr. B Analyt. Technol. Biomed. Life Sci. (2005) 827
109–118.
32 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

32 Reddy V.P., Garrett M.R., Perry G., Smith M.A. Carnosine:
a versatile antioxidant and antiglycating agent. Sci. Aging
Knowledge Environ. (2005) 2005 pe 12.
33 Rashid I., van Reyk D.M., Davies M.J. Carnosine and its
constituents inhibit glycation of low-density lipoproteins that
promotes foam cell formation in vitro. FEBS Lett. (2007) 581
1067–1070.
34 Arnould J.M., Frentz R. Presence, isolation and chemical
structure of a substance characteristic of cardiac tissue in
Carcinus maenas (L.): beta-alanylhistamine. Comp. Biochem.
Physiol. C. (1975) 50 59–66.
35 Brotman D.N., Flancbaum L., Fitzpatrick J.C., Fisher H.
Presence of carcinine (b-alanylhistamine) in mammalian
tissues. FASEB J. (1989) 3 1028.
36 Brotman D.N., Flancbaum L., Kang Y.H., Merrill G.F., Fisher H.
Positive inotropic effects of carcinine in the isolated, perfused
guinea pig heart. Crit. Care Med. (1990) 18 317–321.
37 Flancbaum L., Brotman D.N., Fitzpatrick J.C., Van Es T.,
Kasziba E., Fisher H. Existence of carcinine, a histamine-
related compound, in mammalian tissues. Life Sci. (1990) 47
1587–1593.
38 Ali S.M., Tedford C.E., Gregory R. et al. Design, synthesis,
and structure–activity relationships of acetylene-based
histamine H3 receptor antagonists. J. Med. Chem. (1999) 42
903–909.
39 Tedford C.E., Phillips J.G., Gregory R. et al. Development of
trans-2-[1H-imidazol-4-yl] cyclopropane derivatives as new
high-affinity histamine H3 receptor ligands. J. Pharmacol.
Exp. Ther. (1999) 289 1160–1168.
40 Yates S.L., Phillips J.G., Gregory R. et al. Identification and
pharmacological characterization of a series of new 1H-4-
substituted-imidazoyl histamine H3 receptor ligands. J. Phar-
macol. Exp. Ther. (1999) 289 1151–1159.
41 Tozer M.J., Kalindjian S.B. Histamine H3 receptor antagonists.
Expert Opin. Ther. Patents (2000) 10 1045–1055.
42 Chen Z., Sakurai E., Hu W. et al. Pharmacological effects of
carcinine on histaminergic neurons in the brain. Br. J.
Pharmacol. (2004) 143 573–580. Epub 2004 Oct 4.
43 Babizhayev M.A. Biological activities of the natural imidazole-
containing peptidomimetics n-acetylcarnosine, carcinine and
L-carnosine in ophthalmic and skin care products. Life Sci.
(2006) 78 2343–2357. Epub 2006 Jan 4.
44 Arnould J.M., Frentz R. Carcinine (b-alanyl-histamine): rapid
synthesis and action on vertebrate blood pressure. Arch. Int.
Physiol. Biochim. (1977) 85 339–350.
45 Babizhayev M.A., Deyev A.I., Yermakova V.N. et al. Image
analysis and glare sensitivity in human age-related cataracts.
Clin. Exp. Optom. (2003) 86 157–172.
46 Babizhayev M.A. Glare disability and driving safety. Ophthal-
mic Res. (2003) 35 19–25.
47 Babizhayev M.A., Seguin M.-C. Process of assessment of ocular
dysfunctions and implementation devices of this process. US
Patent No. 6,007,203. Date of patent: December 28, 1999.
48 Ferris F.L., Kassoff A., Bresnick G.H. et al. New visual acuity
charts for clinical research. Am. J. Ophthalmol. (1982) 94 91–
96.
49 Ferris F.L., Sperduto R.D. Standardized illumination for visual
acuity testing in clinical research. Am. J. Ophthalmol. (1982)
94 97–98.
50 Khoroshilova-Maslova I.P., Babizhayev M.A., Ilatovskaya L.V.,
Kiseleva O.A., Gankovskaya L.V.. Method of prophylaxis of
proliferative vitreoretinopathy. Moscow Helmholtz Institute for
Eye Diseases. Russian Patent No 2175223. Patent issued on
27 October 2001. Priority of 29.07.1999.
51 Kanan Y., Wicker L.D., Al-Ubaidi M.R., Mandal N.A., Kasus-
Jacobi A. Retinol dehydrogenases RDH11 and RDH12 in the
mouse retina: expression levels during development and
regulation by oxidative stress. Invest. Ophthalmol. Vis. Sci.
(2008) 49 1071–1078.
52 Babizhayev M.A. Ocular drug metabolism of the bioactivating
antioxidant N-acetylcarnosine for vision in ophthalmic pro-
drug and codrug design and delivery. Drug Dev. Ind. Pharm.
(2008) 34 1071–1089.
53 Rekker R.F.. The hydrophobic fragmental constant. Elsevier,
Amsterdam, 1977.
54 O’Dowd J.J., Robins D.J., Miller D.J. Detection, characterisation,
and quantification of carnosine and other histidyl derivatives
in cardiac and skeletal muscle. Biochim. Biophys. Acta (1988)
967 241–249.
55 Babizhayev M.A., Yermakova V.N., Semiletov Y.A., Deyev A.I.
The natural histidine-containing dipeptide N-acetylcarnosine
as an antioxidant for ophthalmic use. Biochemistry (Mosc)
(2000) 65 588–598.
56 Hepsen I.F., Yildirim Z., Yilmaz H., Kotuk M. Preventive effect
of lacrimal occlusion on topical timolol-induced bronchocon-
striction in asthmatics. Clin. Experiment. Ophthalmol. (2004)
32 597–602.
57 Otani H., Okumura A., Nagai K., Okumura N. Colocalization of
a carnosine-splitting enzyme, tissue carnosinase (CN2)/cyto-
solic non-specific dipeptidase 2 (CNDP2), with histidine
decarboxylase in the tuberomammillary nucleus of the hypo-
thalamus. Neurosci. Lett. (2008) 445 166–169. Epub 2008
Sep 7.
58 Uhlrich D.J., Manning K.A., Xue J.-T. Effects of activation of
the histaminergic tuberomammillary nucleus on visual
responses of neurons in the dorsal lateral geniculate nucleus. J.
Neurosci. (2002) 22 1098–1107.
59 Panula P., Pirvola U., Auvinen S., Airaksinen M.S. Histamine-
immunoreactive nerve fibers in the rat brain. Neuroscience
(1989) 28 585–610.
60 Pegova A., Abe H., Boldyrev A. Hydrolysis of carnosine and
related compounds by mammalian carnosinases. Comp.
Biochem. Physiol. B Biochem. Mol. Biol. (2000) 127 443–
446.
61 Haddad G., Belosevic M. Transferrin-derived synthetic peptide
induces highly conserved pro-inflammatory responses of
macrophages. Mol. Immunol. (2009) 46 576–586. Epub
2008 Oct 25.
62 Wenzel A., Grimm C., Samardzija M., Remae C.E. Molecular
mechanisms of light-induced photoreceptor apoptosis and
neuroprotection for retinal degeneration. Prog. Retin. Eye Res.
(2005) 24 275–306.
N-acetylcarnosine lubricant eye drops and carcinine for vision care 33
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

63 Awasthi Y.C., Sharma R., Cheng J.Z. et al. Role of 4-
hydroxynonenal in stress-mediated apoptosis signaling. Mol.
Aspects Med. (2003) 24 219–230.
64 Yang Y., Sharma R., Sharma A., Awasthi S., Awasthi Y.C.
Lipid peroxidation and cell cycle signaling: 4-hydroxynonenal,
a key molecule in stress mediated signaling. Acta Biochim. Pol.
(2003) 50 319–336.
65 Tanito M., Elliott M.H., Kotake Y., Anderson R.E. Protein
modifications by 4-hydroxynonenal and 4-hydroxyhexenal in
light-exposed rat retina. Invest. Ophthalmol. Vis. Sci. (2005)
46 3859–3868.
66 Uchida K. 4-Hydroxy-2-nonenal: a product and mediator of
oxidative stress. Prog. Lipid Res. (2003) 42 318–343.
67 Uchida K., Stadtman E R. Modification of histidine residues in
proteins by reaction with 4-hydroxynonenal. Proc. Natl Acad.
Sci. USA (1992) 89 4544–4548.
68 Esterbauer H., Schaur R.J., Zollner H. Chemistry and bio-
chemistry of 4-hydroxynonenal, malonaldehyde and related
aldehydes. Free Radic. Biol. Med. (1991) 11 81–128.
69 Esterbauer H. Cytotoxicity and genotoxicity of lipid-oxidation
products. Am. J. Clin. Nutr. (1993) 57 779S–785S. discussion
785S–786S.
70 Kasus-Jacobi A., Ou J., Birch D.G. et al. Functional charac-
terization of mouse RDH11 as a retinol dehydrogenase
involved in dark adaptation in vivo. J. Biol. Chem. (2005) 280
20413–20420.
71 Owsley C., Stalvey B.T., Wells J., Sloane M.E., McGwin G. Jr.
Visual risk factors for crash involvement in older drivers with
cataract. Arch. Ophthalmol. (2001) 119 881–887.
72 Eye Research Australia, Access Economics (2004) Clear
insight: the economic impact and cost of vision loss in
Australia. Access Economics, Melbourne.
73 Taylor H.R., McCarty C.A., Nanjan M.B. Vision impairment
predicts five-year mortality. Trans. Am. Ophthalmol. Soc.
(2000) 98 91–96.
74 Weih L.M., Hassell J.B., Keeffe J. Assessment of the impact of
vision impairment. Invest. Ophthalmol. Vis. Sci. (2002) 43
927–935.
75 Klein B.E., Klein R., Jensen S.C. A short questionnaire on
visual function in older adults to supplement ophthalmic
examination. Am. J. Ophthalmol. (2000) 130 350–352.
76 Haymes S.A., Johnston A.W., Heyes A.S. The development of
the Melbourne Low Vision ADL Index: a measure of vision
disability. Invest. Ophthalmol. Vis. Sci. (2001) 42 1215–1225.
77 Friedman S.M., Munoz B., Rubin G.S., West S.K., Bandeen-
Roche K., Fried L.P. Characteristics of discrepancies between
self-reported visual function and measured reading speed.
Invest. Ophthalmol. Vis. Sci. (1999) 40 858–864.
78 McCarty C.A., Fu C.L., Taylor H.R. Predictors of falls in the
Melbourne visual impairment project. Aust. N. Z. J. Public
Health (2002) 26 11611–11619.
79 Wang J.J., Mitchell P., Simpson J.M., Cumming R.G., Smith W.
Visual impairment, age-related cataract, and mortality. Arch.
Ophthalmol. (2001) 119 1186–1190.
80 Babizhayev M.A., Deyev A.I. Lens opacity induced by lipid
peroxidation products as a model of cataract associated
with retinal disease. Biochim. Biophys. Acta (1989) 1004
124–133.
81 Fishman G.A., Baca W., Alexander K.R., Derlacki D.J., Glenn
A.M., Viana M. Visual acuity in patients with best vitelliform
macular dystrophy. Ophthalmology (1993) 100 1665–1670.
82 Wu D.Z., Wu L., Chang F.X., Jin C., Padula W. Visual
rehabilitation in low vision patients with aging macular
degeneration. J. Am. Optom. Assoc. (1995) 66 39–41.
83 The Retinal Society Terminology Committee. The classification
of retinal detachment with proliferative vitreoretinopathy.
Ophthalmology (1983) 90 121–125.
84 Kampik A., Kenyon K.R., Michels R.G., Green W.R., de la Cruz
Z.C. Epiretinal and vitreous membranes: comparative study of
56 cases. Arch. Ophthalmol. (1981) 99 1445–1454.
85 Jerdan J.A., Pepose J.S., Michels R.G. et al. Proliferative
vitreoretinopathy membranes. An immunohistochemical
study. Ophthalmology (1989) 96 801–810.
86 Morino P., Hiscott P., McKechnie N., Grierson I. Variation in
epiretinal membrane components with clinical duration of the
proliferative tissue. Br. J. Ophthalmol. (1990) 74 393–399.
87 Rachal W.F., Burton T.C. Changing concepts of failures after
retinal detachment surgery. Arch. Ophthalmol. (1979) 97
480–483.
88 Peyman G.A., Schulman J. Proliferative vitreoretinopathy and
chemotherapeutic agents. Surv. Ophthalmol. (1985) 29 434–
442.
89 Babizhayev M.A., Seguin M.-C. Pseudodipeptide product hav-
ing an imidazole grouping and applications. Patent PCT/
FR94/01272. Filed 3 Nov. 1994. WO 95/12581.
90 Babizhayev M.A., Seguin M.-C. Coupling product obtained
from histamine and an amino acid. Patent PCT/FR94/00189.
Filed 21 February 1994. WO 94/19325.
91 Babizhayev M.A., Courbebaisse Y., Nicolay J.-F., Semiletov
Y.A. Design and biological activity of imidazole-containing
peptidomimetics with a broad-spectrum antioxidant activity.
Lett. Pept. Sci. (1998) 5 163–169.
92 Babizhayev M.A., Lozovskaya E.L., Makareyeva E.N., Lul’kin
Y.A., Sapezhinskii I.I. Photoprotector and antioxidant prop-
erties of histamine-containing peptidomimetics in the photo-
oxidation of glycyltryptophan. Biochemistry (Mosc) (1998) 63
523–528.
93 Belikova N.A., Tyurina Y.Y., Borisenko G. et al. Heterolytic
reduction of fatty acid hydroperoxides by cytochrome
c/cardiolipin complexes: antioxidant function in mitochondria.
J. Am. Chem. Soc. (2009) 131 11288–11289.
94 Kagan V.E., Bayir H.A., Belikova N.A. et al. Cytochrome
c/cardiolipin relations in mitochondria: a kiss of death. Free
Radic. Biol. Med. (2009) 46 1439–1453. Epub 2009 Mar 12.
95 Tyurin V.A., Tyurina Y.Y., Jung M.Y. et al. Mass-spectromet-
ric analysis of hydroperoxy- and hydroxy-derivatives of
cardiolipin and phosphatidylserine in cells and tissues induced
by pro-apoptotic and pro-inflammatory stimuli. J. Chromatogr.
B Analyt. Technol. Biomed. Life Sci. (2009) 877 2863–2872.
Epub 2009 Mar 13.
96 Kagan V.E., Bayir A., Bayir H. et al. Mitochondria-targeted
disruptors and inhibitors of cytochrome c/cardiolipin peroxi-
34 M.A. Babizhayev et al.
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology

dase complexes: a new strategy in anti-apoptotic drug
discovery. Mol. Nutr. Food Res. (2009) 53 104–114.
97 McKechnie N.M., Fould W.S. Qualitative observations on the
variations of light induced damage to the rabbit retina.
Graefes. Arch. Clin. Exp. Ophthalmol. (1981) 215 305–325.
98 Duncan T.E., O’Steen W.K. The diurnal susceptibility of rat
retinal photoreceptors to light induced damage. Exp. Eye Res.
(1985) 4l 497–507.
99 Kremers J.J.M., Norren D.V. Retinal damage in macaque after
white light exposures lasting ten minutes to twelve hours.
Invest. Ophthalmol. Vis. Sci. (1989) 30 1032–1040.
100 Lee F.L., Yu D.Y., Tso M.O.M. Effect of continuous versus
multiple intermittent light exposures on rat retina. Curr. Eye
Res. (1990) 9 11–21.
101 Rapp L.M., Tolman B.L., Dhindsa H.S. Separate mechanisms
for retinal damage by ultraviolet-A and mid-visible light.
Invest. Ophthalmol. Vis. Sci. (1990) 31 1186–1190.
102 Penn J.S., Howard A.G., Williams T.P.. Light damage as a
function of ‘‘light history’’ in albino rat, in: La Vail M.M.,
Hollyfield J.G., Anderson R.G.. (Eds). Retinal degeneration:
experimental and clinical studies. Alan R. Liss, New York,
1985, pp. 439–447.
103 White M.P., Fisher L.J. Degree of light damage to the retina
varies with time of day of bright light exposure. Physiol.
Behav. (1987) 39 607–613.
104 Noell W.K. Retinal damage by light in rats. Invest. Ophthal-
mol. Vis. Sci. (1966) 5 450–473.
105 Wiegand R.D., Guisto N.M., Rapp L.M., Anderson R.E.
Evidence for rod outer segment lipid peroxidation following
constant illumination of the rat retina. Invest. Ophthalmol.
Vis. Sci. (1983) 24 l433–l435.
106 Organisciak D.T., Wang H.M., Li Z.Y., Tso M.O.M. The
protective effect of ascorbate in retinal light damage of rats.
Invest. Ophthalmol. Vis. Sci. (1985) 26 1580–1588.
107 Feeney L., Berman E.R. Oxygen toxicity: membrane damage by
free radicals. Invest. Ophthalmol. Vis. Sci. (1976) 15 789–
792.
108 Li Z.Y., Tso M.O.M., Wang H.M., Organisciak D.T. Ameliora-
tion of photic injury in rat retina by ascorbic acid. Invest.
Ophthalmol. Vis. Sci. (1985) 26 1589–1598.
109 Organisciak D.T., Bicknell I.R., Darrow R.M. The effect of L
and D ascorbic acid administration on retinal tissue levels
and light damage in rats. Curr. Eye Res. (1992) 11 231–
241.
110 Ham W.T., Muller H.A., Ruffolo J.J. et al. Basic mechanisms
underlying the production of photochemical lesions in
the mammalian retina. Curr. Eye Res. (1984) 3
165–174.
111 Aust S.D., Morehouse L.A., Thomas C.E. Role of metals in
oxygen radical reactions. Free Radic. Biol. Med. (1985) 1
3–25.
112 Fliesler S.J., Anderson R.E. Chemistry and metabolism of
lipids in the vertebrate retina. Prog. Lipid Res. (1983) 22
79–131.
113 Rodieck R.W.. The vertebrate retina: principles of structure
and function. WH Freeman, San Francisco, 1973.
114 Girotti A. Photodynamic lipid peroxidation in biological
systems. Photochem. Photobiol. (1990) 51 497–509.
115 Babizhayev M.A., Meguro K. (2004) Combined use of carn-
osinase inhibitor with l-carnosines and composition. WO
2004/064866 PCT/JP2004/000351. Filed 20 January 2003
(20.01.2003).
116 Babizhayev M.A. Method for topical treatment of eye
disease and composition and device for said treatment. United
States Patent No. US 7,795,203 B2, Date of Patent Sep.
14,2010, PCT filed: Sep. 29, 2003 PCT No. PCT/IB03/
04259.
117 Babizhayev M.A., Yegorov Y.E. Advanced drug delivery of
N-acetylcarnosine (N-acetyl-beta-alanyl-L-histidine), carcinine
(beta-alanylhistamine) and L-carnosine (beta-alanyl-L-histi-
dine) in targeting peptide compounds as pharmacological
chaperones for use in tissue engineering, human disease
management and therapy: from in vitro to the clinic. Recent
Pat. Drug Deliv. Formul. (2010) 4 198–230.
118 Babizhayev M.A., Yegorov Y.E. Therapeutic uses of drug-
carrier systems for imidazole-containing dipeptide compounds
that act as pharmacological chaperones and have significant
impact on the treatment of chronic diseases associated with
increased oxidative stress and the formation of advanced
glycation end products. Crit. Rev. Ther. Drug Carrier Syst.
(2010) 27 85–154.
119 Babizhayev M.A. Designation of imidazole-containing dipep-
tides as pharmacological chaperones. Hum. Exp. Toxicol.
(2010) [Epub ahead of print].
N-acetylcarnosine lubricant eye drops and carcinine for vision care 35
ª 2011 The Authors Fundamental and Clinical Pharmacology ª 2011 Societe Francaise de Pharmacologie et de TherapeutiqueFundamental & Clinical Pharmacology