ovulation induction for pcos roy homburg barzilai medical center, ashkelon, israel barzilai medical...
TRANSCRIPT

Ovulation Induction for PCOSOvulation Induction for PCOS
Roy HomburgRoy Homburg
Barzilai Medical Center, Ashkelon, IsraelBarzilai Medical Center, Ashkelon, Israeland Homerton University Hospital, Londonand Homerton University Hospital, London

Clomiphene QuestionsClomiphene Questions• Spelling – clomiphene or clomifene?Spelling – clomiphene or clomifene?
• Give hCG at mid-cycle?Give hCG at mid-cycle?
• Monitor CC cycles with ultrasound?Monitor CC cycles with ultrasound?
• When to stop?When to stop?
• Is CC still the best first-line treatment?Is CC still the best first-line treatment?

ClomipheneClomiphene
n = 5268n = 5268
Ovulation – 3858 Ovulation – 3858 (73%)(73%)
Pregnancies – 1909 Pregnancies – 1909 (36%)(36%)
Miscarriage – Miscarriage – 20%20%
Multiple pregnancy rate – Multiple pregnancy rate – 10%10%
Single live-birth rate – 25%Single live-birth rate – 25%
Homburg, Hum Reprod, 2005Homburg, Hum Reprod, 2005

Should we give hCG in CC cycles? Should we give hCG in CC cycles? Agarwal & Buyalos, 1995Agarwal & Buyalos, 1995
No improvement in conception ratesNo improvement in conception rates
Deaton et al, 1997Deaton et al, 1997
No differenceNo difference
Viahos et al, 2005Viahos et al, 2005
hCG may be beneficialhCG may be beneficial
Kosmas et al, 2007 Meta-analysisKosmas et al, 2007 Meta-analysis
Favoured hCG but noFavoured hCG but no significant differencesignificant difference
Brown et al, 2009, Cochrane reviewBrown et al, 2009, Cochrane review
No difference No difference
NO
NO
Maybe
Yes
NO

Should we monitor clomiphene Should we monitor clomiphene cycles with ultrasound?cycles with ultrasound?
Konig, Homburg et al, ESHRE, 2009 Konig, Homburg et al, ESHRE, 2009
With U/S + hCGWith U/S + hCGNo U/S or hCGNo U/S or hCG
nn105105150150
Cumulative Cumulative pregnancy ratepregnancy rate
48%48%34.7%34.7%
DeliveriesDeliveries35.6%35.6%26.7%26.7%
Multiple Multiple pregnanciespregnancies
0011

Clomiphene CitrateClomiphene Citrate
StoppingStopping… …
• No ovulation with 150 mg/dayNo ovulation with 150 mg/day
• 6 ovulatory cycles fail to yield a pregnancy 6 ovulatory cycles fail to yield a pregnancy
• Endometrial thickness <7 mm at ovulationEndometrial thickness <7 mm at ovulation

Reasons for Clomiphene FailureReasons for Clomiphene Failure
Ovulation Ovulation
but no conceptionbut no conception
• Anti-estrogen effectsAnti-estrogen effects
- Cervical mucus- Cervical mucus
- Endometrium- Endometrium
• High LHHigh LH
Failure to ovulateFailure to ovulate
• FAIFAI
• BMIBMI
• LHLH
• InsulinInsulin
Failure to ovulateFailure to ovulate
• FAIFAI
• BMIBMI
• LHLH
• InsulinInsulin

Aromatase Inhibitor Treatment:Aromatase Inhibitor Treatment:Day 3-7 of CycleDay 3-7 of Cycle
ERER
ERER
E2E2FSHFSH
AIAI
ERER
ERER
Casper & MitwallyCasper & Mitwally
Aromatase Inhibitors:Aromatase Inhibitors:Theoretical AdvantagesTheoretical Advantages
• Do not block estrogen receptorsDo not block estrogen receptors • No detrimental effect on endometrium No detrimental effect on endometrium or cervical mucusor cervical mucus • Negative feedback mechanism not Negative feedback mechanism not turned off—less chance of multiple turned off—less chance of multiple follicular development follicular development
ERER
ERER
E2E2FSHFSH
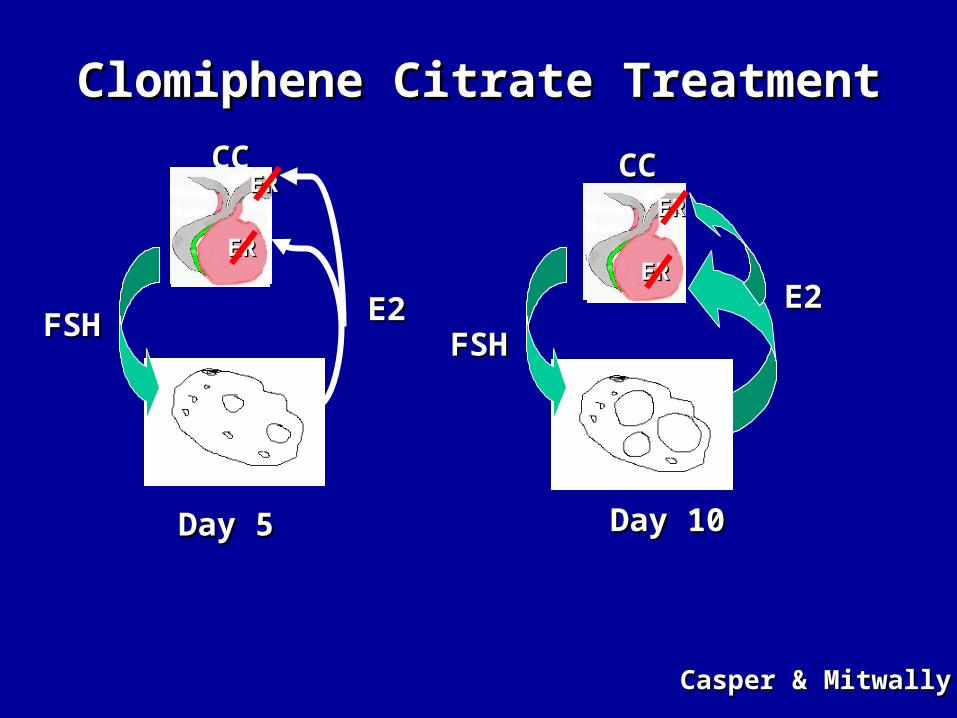
Day 5Day 5
Clomiphene Citrate TreatmentClomiphene Citrate Treatment
ERER
ERER
Day 10Day 10
FSHFSH
E2E2
CCCC CCCC
ERER
ERER
ERER
ERER
Casper & MitwallyCasper & Mitwally

ERER
ERER
E2E2FSHFSH
AIAI
Day 5Day 5
Aromatase Inhibitor TreatmentAromatase Inhibitor Treatment
ERER
ERER
E2E2
FSHFSH
Day 10Day 10
ERER
ERER
ERER
ERER
Casper & MitwallyCasper & Mitwally

Aromatase InhibitorAromatase InhibitorQuestionsQuestions
• Do they work?Do they work?
• Better than CC for first-line treatment?Better than CC for first-line treatment?
• Safety?Safety?

Aromatase Inhibitors vs CCAromatase Inhibitors vs CC
• Meta-analysis, 4 RCTsMeta-analysis, 4 RCTs
• Clear superiority of aromatase inhibitors Clear superiority of aromatase inhibitors in pregnancy rates (OR 2.0) and in pregnancy rates (OR 2.0) and deliveries (OR 2.4)deliveries (OR 2.4)
Polyzos et al, Fertil Steril, 2008Polyzos et al, Fertil Steril, 2008

Letrozole vs CCLetrozole vs CC
• 911 newborns in 5 centers911 newborns in 5 centers
CC LetrozoleCC LetrozolePregnancies 397Pregnancies 397 514514
Congenital Congenital 19 19 (4.8%)(4.8%) 14 14 (2.7%)(2.7%)
malformationsmalformations
Major malformations 12 Major malformations 12 (3%)(3%) 6 6 (1.2%)(1.2%)Total cardiac anomalies Total cardiac anomalies 1.8%1.8% 0.2%0.2%
Tulandi et al, 2006Tulandi et al, 2006

Aromatase InhibitorsAromatase Inhibitors
• Letrozole 2.5-10 mg/day, n=1102Letrozole 2.5-10 mg/day, n=1102
• Pregnancies 368 (33.4%)Pregnancies 368 (33.4%)
– Miscarriages 99 (26.9%)Miscarriages 99 (26.9%)
– Twins 2 (0.5%)Twins 2 (0.5%)
– Fetal anomalies 1 (0.2%)Fetal anomalies 1 (0.2%)
Aghssa et al, 2007 (PCOS, eds Allahbadia, Agrawal)Aghssa et al, 2007 (PCOS, eds Allahbadia, Agrawal)

Gonadotropin Treatment: Gonadotropin Treatment: Why Is PCOS Different?Why Is PCOS Different?Greater sensitivity to gonadotropin Greater sensitivity to gonadotropin
stimulationstimulation
Therefore, multiple Therefore, multiple (“explosive”) follicular development(“explosive”) follicular development

Conventional Regimen With Conventional Regimen With GonadotropinsGonadotropins
55 55 55DaysDays
7575
7575
7575
55

Results of Conventional Therapy:Results of Conventional Therapy:14 Series, 1966-1984, WHO I & II14 Series, 1966-1984, WHO I & II
Hamilton-FairleyHamilton-Fairley & Franks, 1990 & Franks, 1990
Conceived 46%( 16-78)
Multiple preg. 34%( 22-50)
Miscarriages 23%( 12-30)
Severe OHSS 4.6%( 1.3-9.4)

Problems With Conventional Problems With Conventional Gonadotropin Therapy for PCOSGonadotropin Therapy for PCOS
• Multiple follicle developmentMultiple follicle development
- Multiple pregnancies- Multiple pregnancies
- OHSS- OHSS

Low-Dose rFSHLow-Dose rFSH
75-112.5 IU50-75 IU
100-150 IU
14 7 7
Days

Low-Dose Gonadotropins:Low-Dose Gonadotropins:Summary of ResultsSummary of Results
Pregnancies 411 (40%)
Fecundity/ov. cycle 23%
Uniovulation 71%
OHSS 0.14%
Multiple preg. 5.1%
Updated from Homburg & Howles, 1999Updated from Homburg & Howles, 1999
Patients - 1040, Cycles 2472Patients - 1040, Cycles 2472

Incremental Dose RiseIncremental Dose Rise50 IU starting dose; increments of 25 or 50 IU
n=158
11 88 1515 2222 2929 3535
150 150 IIUU daily daily
100 100 IIUU daily daily125 125 IIUU daily daily
75 75 IIUU daily daily7 days
7 days7 days
7 days50 50 IU dailyIU daily
7 days
StartStart day 3 of day 3 of mensesmenses
DDays of treatmentays of treatment11 88 1515 2222 2929 3636
250 250 IIUU daily daily
150 150 IIUU daily daily
7 days
200 200 IIUU daily daily
7 days7 days
100 100 IIUU daily daily
7 days50 50 IU dailyIU daily
7 days
FSH increments:FSH increments: Only allowed when no follicle Only allowed when no follicle 12 mm 12 mm hCG:hCG: 1 follicle 1 follicle 18 mm18 mmCancellation:Cancellation: 3 follicles 3 follicles 15 mm 15 mm Leader et al, 2006Leader et al, 2006
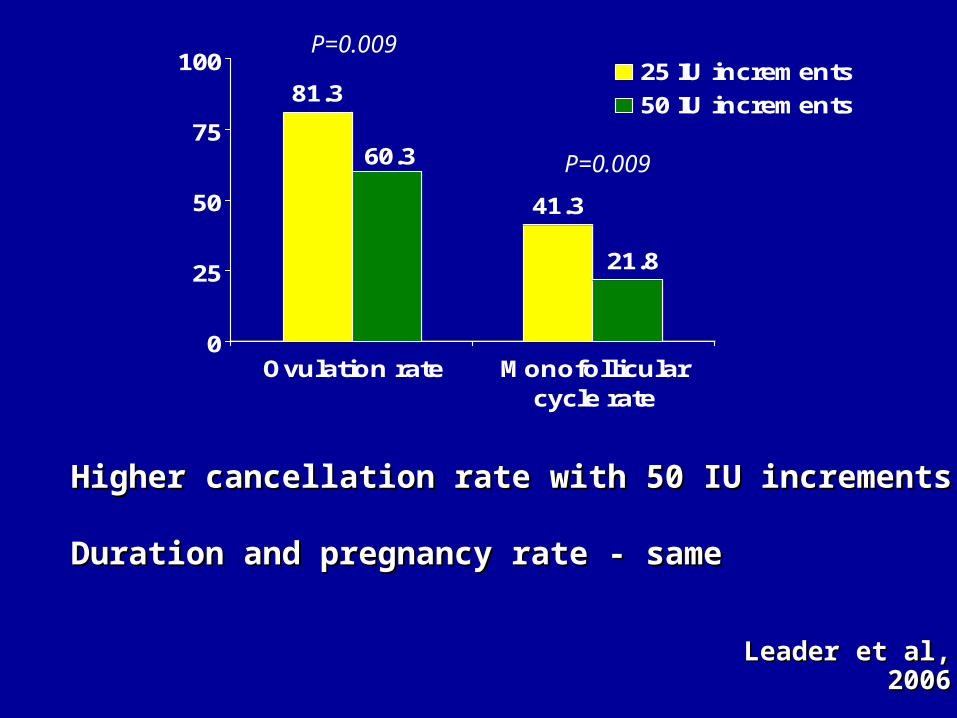
81.3
60.3
41.3
21.8
0
25
50
75
100
Ovulation rate Monofollicularcycle rate
25 IU increments
50 IU increments
P=0.009
P=0.009
Leader et al, 2006Leader et al, 2006
Higher cancellation rate with 50 IU incrementsHigher cancellation rate with 50 IU increments
Duration and pregnancy rate - sameDuration and pregnancy rate - same

• Incremental dose rise of Incremental dose rise of 8.38.3 IU each week IU each week
• N=25, PCOS, CC failures, 69 cyclesN=25, PCOS, CC failures, 69 cycles
50 IU58.3 IU
64.6 IU
7 14 21
Orvieto & Homburg, 2008Orvieto & Homburg, 2008
Days
Only Minimal DoseOnly Minimal Dose Increment Needed Increment Needed
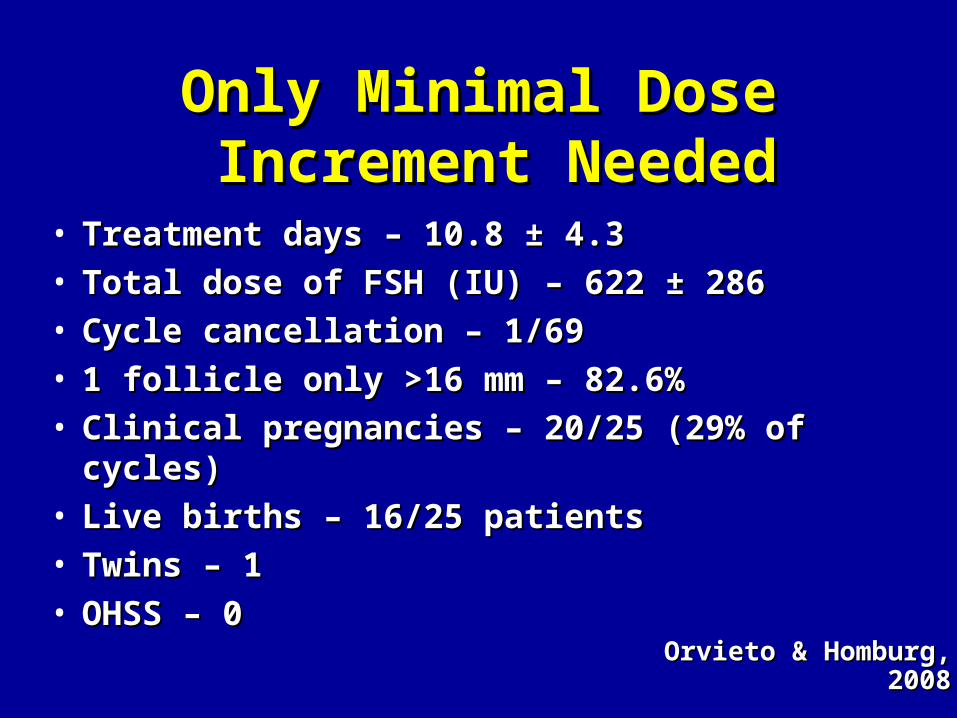
Only Minimal DoseOnly Minimal Dose Increment Needed Increment Needed
• Treatment days – 10.8 Treatment days – 10.8 ±± 4.3 4.3 • Total dose of FSH (IU) – 622 Total dose of FSH (IU) – 622 ±± 286 286 • Cycle cancellation – 1/69 Cycle cancellation – 1/69 • 1 follicle only >16 mm – 82.6%1 follicle only >16 mm – 82.6%• Clinical pregnancies – 20/25 (29% of cycles)Clinical pregnancies – 20/25 (29% of cycles)• Live births – 16/25 patients Live births – 16/25 patients • Twins – 1 Twins – 1 • OHSS – 0OHSS – 0
Orvieto & Homburg, 2008Orvieto & Homburg, 2008

Low-Dose rFSH in Vietnamese Low-Dose rFSH in Vietnamese Women With PCOS Women With PCOS
• N=183, PCOS, CC failure, normal or low BMIN=183, PCOS, CC failure, normal or low BMI
25 IU50 IU
75 IU
14 5 514 5 5 DaysDays
Puregon
Lan et al, RBM Online, 2009Lan et al, RBM Online, 2009
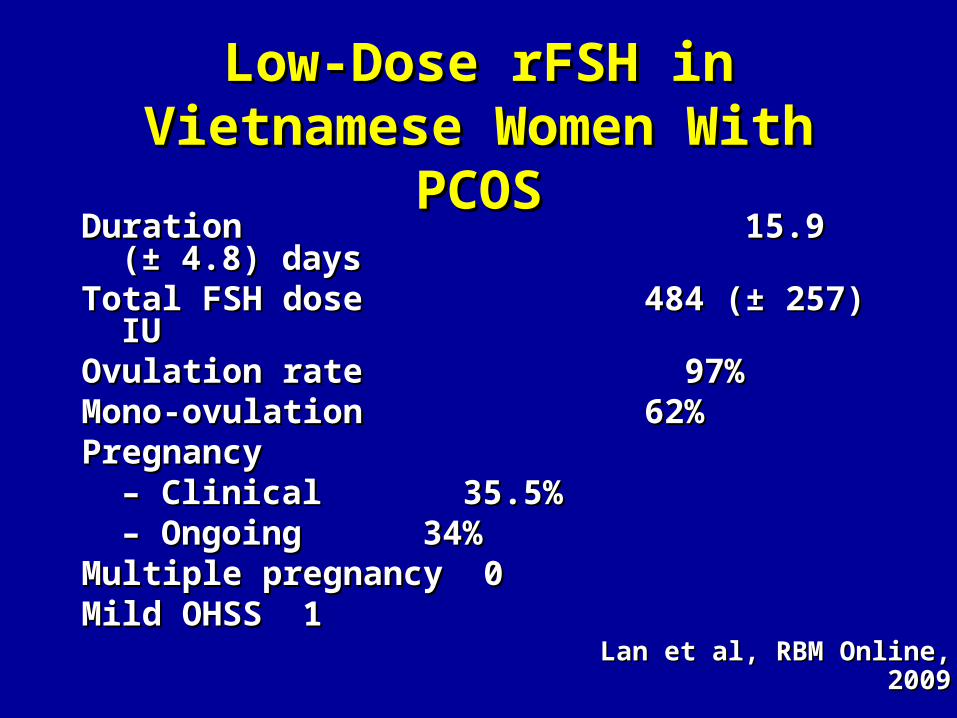
Low-Dose rFSH in Vietnamese Low-Dose rFSH in Vietnamese Women With PCOSWomen With PCOS
Duration 15.9 (Duration 15.9 (±± 4.8) days 4.8) daysTotal FSH dose 484 (Total FSH dose 484 (±± 257) IU 257) IUOvulation rate 97%Ovulation rate 97%Mono-ovulation 62%Mono-ovulation 62%PregnancyPregnancy
– – Clinical 35.5%Clinical 35.5% – – Ongoing 34%Ongoing 34%Multiple pregnancy 0 Multiple pregnancy 0 Mild OHSS 1 Mild OHSS 1
Lan et al, RBM Online, 2009Lan et al, RBM Online, 2009

Duration of Initial Dose: 14 or 7 Days?Duration of Initial Dose: 14 or 7 Days? 14 days 14 days 7 days7 days
FSH required FSH required - Amps - Amps 22 1722 17- Days - Days 17.4 1317.4 13
1 large follicle/cycle 74% 60%1 large follicle/cycle 74% 60%
E2 (pmol/L) 1659 2072E2 (pmol/L) 1659 2072Pregnancies 10 (40%) 14 Pregnancies 10 (40%) 14
(56%)(56%)OHSS 0 0OHSS 0 0Multiple pregnancies 0 Multiple pregnancies 0 2/14 2/14
N=50, 107 cyclesN=50, 107 cycles
Homburg, 1999Homburg, 1999

Multiple pregnanciesMultiple pregnancies
14 days 0/1014 days 0/10
7 days 6/29 7 days 6/29
Homburg, 1999Homburg, 1999
Extended StudyExtended Study

How long does it take?How long does it take?
• With a starting dose of 75 IU FSH, With a starting dose of 75 IU FSH, unchanged for a minimum of 14 days, unchanged for a minimum of 14 days, 90% will get to the criteria for hCG90% will get to the criteria for hCGwithin 14 dayswithin 14 days
Homburg & Howles, 1999Homburg & Howles, 1999

Comparison of Results:Comparison of Results:CC vs FSH – 100 WomenCC vs FSH – 100 Women
BUT…….BUT……. Low-dose FSH has only been given to Low-dose FSH has only been given to clomiphene failures!clomiphene failures!
Homburg, Hum Reprod, 2005; Homburg & Howles, HR Update, 1999Homburg, Hum Reprod, 2005; Homburg & Howles, HR Update, 1999
CCCCFSHFSH
Single live birthsSingle live births25253434
TwinsTwins3322

If we started with FSH…. If we started with FSH….
Starting withStarting withCCCC rFSHrFSH
Singleton live birthsSingleton live births 2525 5050
MultiplesMultiples 33 33
Projection/100 womenProjection/100 women

CC or low-dose FSH for first-line CC or low-dose FSH for first-line treatment?treatment?
Treatment-naive Treatment-naive PCOSPCOS
RandomizationRandomization
CCCC Low-dose FSHLow-dose FSH 3 cycles3 cycles Homburg et al, Hum Reprod, In pressHomburg et al, Hum Reprod, In press

R. Rueda-Saenz
A. Martinez
A. Balen
T. Child
M. Davis
M-L. HendriksT. KonigCB. LambalkP. Hompes
T. D’HoogheM. Welkenhuysen
R. Anderson
M. Rajkhowa
M. Brincat

RandomizedRandomizedN=302N=302
Allocated Allocated N=143N=143
Allocated Allocated N=159N=159
Drop-outsDrop-outsN=20N=20
AnalyzedAnalyzedN=132N=132
AnalyzedAnalyzedN=123N=123
CCCC FSHFSH
Per-protocolPer-protocol
Drop-outsDrop-outsN=27N=27

CC or low-dose FSH for first-line CC or low-dose FSH for first-line treatment?treatment?
• CC CC – 1st cycle, 50 mg/day1st cycle, 50 mg/day– If no ovulation, dose increased by 50 mgIf no ovulation, dose increased by 50 mg
in subsequent cyclesin subsequent cycles • FSH (Puregon)FSH (Puregon)
50 IU
100 IU75 IU
1 7 14 21 1 7 14 21
hCG – when at least 1 follicle >17 mm. hCG – when at least 1 follicle >17 mm.

ResultsResults
CC FSH PCC FSH PPatients per protocol 123 132Patients per protocol 123 132Cycles 310 288Cycles 310 288
Pregnancies 54 (44%) 76 (58%) 0.03Pregnancies 54 (44%) 76 (58%) 0.03Miscarriage rates 5 (9%) 7 (9%)Miscarriage rates 5 (9%) 7 (9%)Multiple pregnancies 0 2 (3%)Multiple pregnancies 0 2 (3%)Pregnancies/cycle 17% 26% 0.008Pregnancies/cycle 17% 26% 0.008Live births 49 (39%) 69 (52%) 0.04Live births 49 (39%) 69 (52%) 0.04
Homburg et al, Hum Reprod, In pressHomburg et al, Hum Reprod, In press
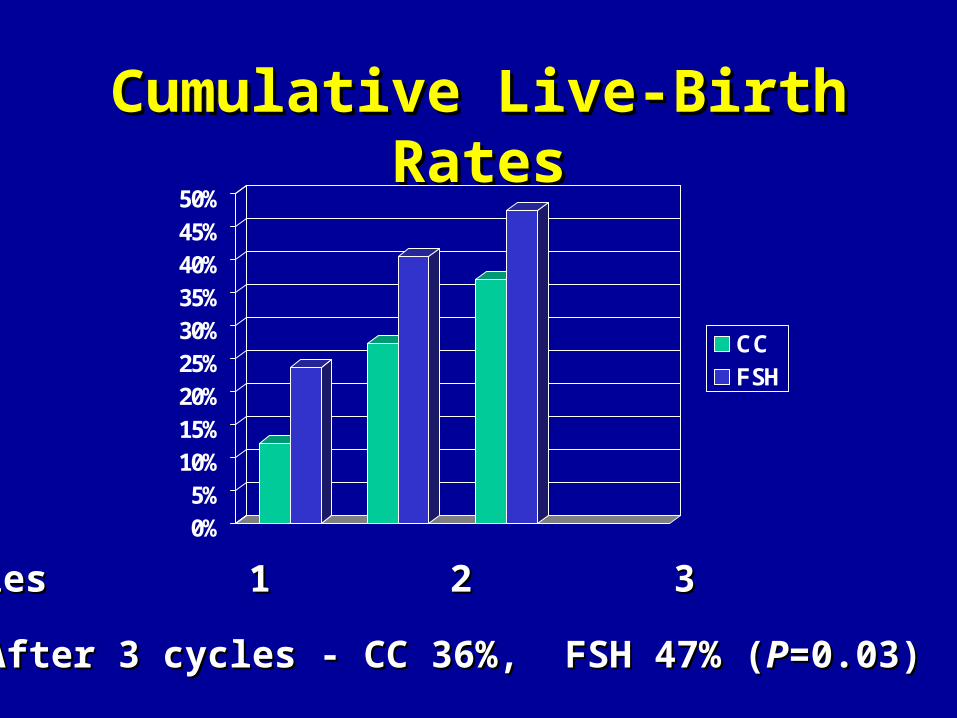
Cumulative Live-Birth RatesCumulative Live-Birth Rates
0%5%
10%15%20%25%30%35%40%45%50%
CCFSH
Cycles 1 2 3Cycles 1 2 3
After 3 cycles - CC 36%, FSH 47% (After 3 cycles - CC 36%, FSH 47% (PP=0.03)=0.03)
SummarySummary• Clear superiority of low-dose FSH over CC forClear superiority of low-dose FSH over CC for
first-line treatment of anovulatory PCOSfirst-line treatment of anovulatory PCOS
• ××2 chance of clinical pregnancy in 1st cycle 2 chance of clinical pregnancy in 1st cycle
– 30% vs 14.6% (30% vs 14.6% (PP=0.003) =0.003)
• After 2nd cycle, 50.7% vs 32.5% (After 2nd cycle, 50.7% vs 32.5% (PP=0.003)=0.003)
• Shorter treatment to pregnancy time Shorter treatment to pregnancy time
Homburg et al, Hum Reprod, In pressHomburg et al, Hum Reprod, In press

Can low-dose FSH Can low-dose FSH replace CC?replace CC?
CC FSHCC FSH
++Ease of administration Ease of administration ++ Cost Cost
== MonitoringMonitoring ==
Treatment - pregnancy timeTreatment - pregnancy time ++
Chances for pregnancyChances for pregnancy ++
Single live birthSingle live birth ++

ConclusionsConclusions
• Differences in cost and convenience may Differences in cost and convenience may limit the choice of low-dose FSH as limit the choice of low-dose FSH as first-line treatmentfirst-line treatment
But….But….
• This study provides “real-life” results to This study provides “real-life” results to enable judgment of this option, according enable judgment of this option, according to individual countries and circumstances to individual countries and circumstances
