outbreaks associated with (1) reusing dialyzers and (2...
TRANSCRIPT

Outbreaks Associated with (1) Reusing Dialyzers and
(2) Compounding Medications: Why We Keep Repeating History
1
Jon Rosenberg MD Healthcare Associated Infections Program
Center for Health Care Quality California Department of Public Health
November 14, 2012
BSIs in ESRD Patients - Background
• Primary bloodstream infections (BSI) in dialysis patients are predominately gram-positive and are usually assumed to be related to vascular access.
• CDHS became aware of outbreaks of bloodstream infections in several chronic dialysis facilities occurring between July and December of 2003.
• Most of these outbreaks involved gram-negative water bacteria (Stenotrophomonas maltophilia, Burkholderia cepacia, B pickettii) and/or Candida parapsilosis, hereafter referred to as “key organisms.”
2

Key Organisms and Reprocessing
• S maltophilia, B cepacia, B pickettii, C parapsilosis properties – Present in water
– Cold resistant
– Form biofilms
• Facilities with outbreaks reused dialyzers, often refrigerating them overnight or as long as 24 hours before reprocessing

BSIs in California ESRD Study
• We implemented a study to determine: 1. The prevalence of BSI infections in California
dialysis centers
2. If dialyzer reprocessing techniques were associated with BSI
3. If specific organisms were more likely than others to occur in temporal clusters.
4

Study Methods • We surveyed all 353 licensed chronic dialysis centers in California by mail
– Number of primary BSIs by month and infectious organism for 2003. – Ownership, size, water supply and distribution, infection control surveillance
practices and policies, multi-dose medication use policies, and dialyzer handling procedures.
• Primary BSI – Signs/symptoms of sepsis/endotoxemia during/within 24 hours after dialysis – Positive blood culture – No other site of infection identified
• Temporal cluster – at least 3 BSIs of the same organism within a 2-month period. T – gram-negative organisms and C. parapsilosis.
• Calculated BSI rates per 100,000 dialysis procedures (DPs) and tested rates for homogeneity using exact Poisson methods.
5

Study results
6
Study: BSI characteristics
• 184 (58.3%) facility respondents reported 1,670 BSIs (35.0 infections per 100,000 DPs) for the study period.
– 1157 (69.4%) gram positive
– 453 (27.2%) gram negative
– 58 (3.5%) fungal or yeast
– 116 (6.9%) key organisms
7

8
Temporal Clusters
• 16 (0.3%) facilities reported BSI clusters due to:
– S. maltophilia (4),
– C. parapsilosis (3),
– Enterobacter cloacae (3),
– B. cepacia (1),
– B. pickettii (1),
– Pseudomonas aeruginosa (1)
– unspecified gram-negative rods (3)
• Clusters of S. maltophilia, B. cepacia, B. pickettii, and C. parapsilosis occurred more often in facilities that reprocessed dialyzers and refrigerated dialyzers prior to reprocessing.
• C. parapsilosis was cultured from 3 of 5 dialyzers used for infected patients in a cluster facility that used refrigeration. 9

10
Stenotrophomonas maltophilia Outbreak in a Dialysis Center, Los Angeles County, 2011
• In August 2011, Dr. X of Hospital Y informed Los Angeles County Department of Public Health of five cases of bacteremia in hemodialysis patients from Dialysis Center A.
• Dialysis Center A licensed facility, separate from Hospital Y, unaware of the outbreak, reuses dialysers
11
Courtesy of Kelsey OYong, MPH,1 L’Tanya English, RN, MPH,1 Patricia Marquez, MPH,1 Dawn Terashita, MD, MPH,1 Eduardo Ramos, BS,2 Hector Rivas, BS,2 Laurene Mascola, MD, MPH1
1County of Los Angeles, Department of Public Health, Acute Communicable Disease Control Program 2County of Los Angeles, Department of Public Health , Public Health Laboratory
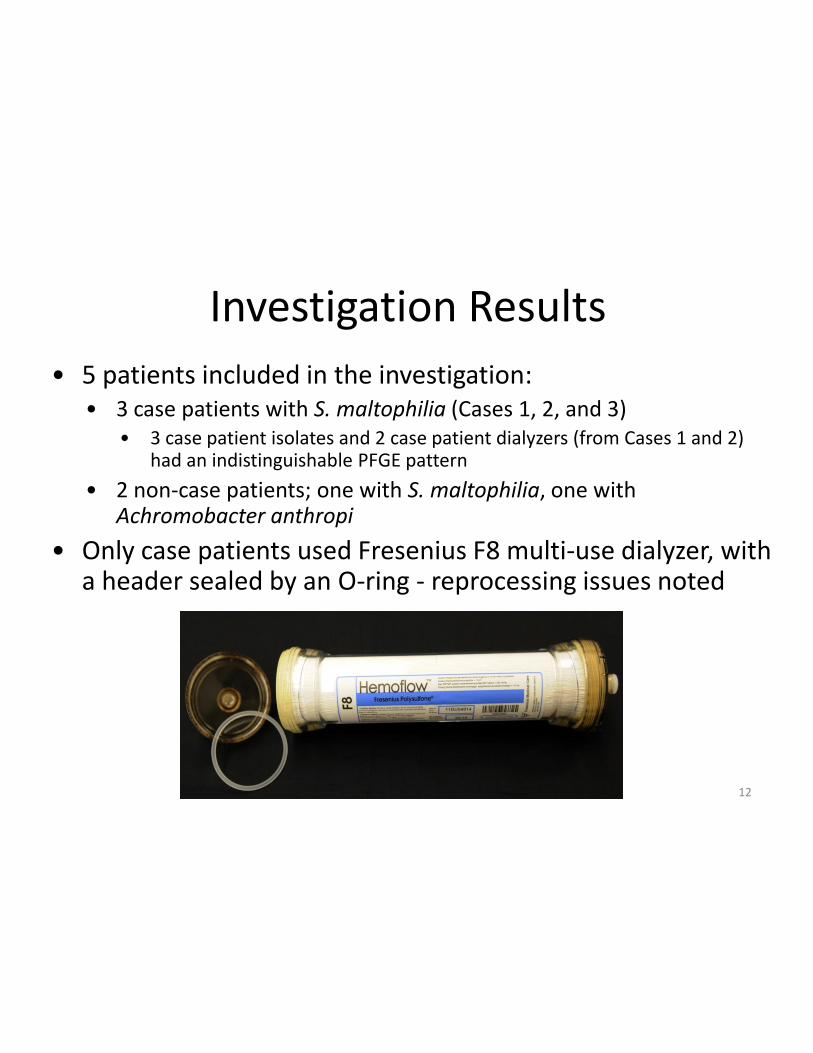
Investigation Results • 5 patients included in the investigation:
• 3 case patients with S. maltophilia (Cases 1, 2, and 3) • 3 case patient isolates and 2 case patient dialyzers (from Cases 1 and 2)
had an indistinguishable PFGE pattern
• 2 non-case patients; one with S. maltophilia, one with Achromobacter anthropi
• Only case patients used Fresenius F8 multi-use dialyzer, with a header sealed by an O-ring - reprocessing issues noted
12

Dear State Epidemiologists We realize that it is late on Friday. However we wanted to make you aware of a potentially serious situation that may require urgent attention over coming days. CDC, in partnership with state health departments and FDA, is investigating a cluster of clinical meningitis cases following spinal injection procedures for pain. We are writing this email to notify you of this investigation, and to encourage active surveillance among potentially exposed persons in your state.
13

We would appreciate your assistance in contacting the affected facilities, included in the attached list, so they can begin outreach to patients. On September 18, 2012, the Tennessee Department of Health was notified of a patient with clinically diagnosed meningitis following an epidural steroid injection at a Tennessee ambulatory surgical center. All initial cultures of cerebrospinal fluid (CSF) and blood were negative; the patient eventually had Aspergillus fumigatus isolated from CSF by fungal culture and had a high CSF galactomannan ratio.
14

Subsequent outreach has demonstrated 9 additional patients, including one at a facility in North Carolina, most with a similar clinical picture:
– One or more spinal injections during July 30 - September 18, 2012.
– Subacute presentation of clinical meningitis, often 7-28 days following spinal procedure
– CSF profile with low glucose, elevated protein and high, neutrophil-predominant, white cell count;
– Negative CSF bacterial cultures and Gram stain
– Many patients had cerebrovascular accident (stroke) in deep brain locations
15
Although the source of these infections is not yet known, three lots of methylprednisolone acetate, recently recalled by the New England Compounding Center (NECC), were among the medications that were used for all of the infected patients.
Given the potential of high morbidity associated with this condition, we recommend that all patients who have received spinal injection at one of the clinics that received product from NECC have active surveillance conducted to determine their clinical status.
16

• Also note that CDC is only aware of infections occurring in patients who received spinal injections and recommends urgent outreach to these patients. Some facilities may have performed injections at other body sites and, because the source of these infections is not yet known, should be encouraged to remain alert for, and promptly report, complications associated with these other types of injections
17

date invoice# name qty city lot number
Invoice 06/13/2012 218775
CYPRESS SURGERY
CENTER DBA 100.00 VISALIA 05212012@68
Invoice 07/11/2012 221848
CYPRESS SURGERY
CENTER DBA 100.00 VISALIA 05212012@68
Invoice 08/01/2012 224284
CYPRESS SURGERY
CENTER DBA 100.00 VISALIA 06292012@26
Invoice 08/22/2012 226630
CYPRESS SURGERY
CENTER DBA 100.00 VISALIA 08102012@51
Invoice 06/26/2012 220237
ENCINO OUTPATIENT
SURGICENTER 300.00 ENCINO 05212012@68
Invoice 09/21/2012 230072
ENCINO OUTPATIENT
SURGICENTER 100.00 ENCINO 08102012@51
Invoice 07/03/2012 220992
UKIAH VALLEY MEDICAL CENTER 50.00 UKIAH 05212012@68
Invoice 07/30/2012 223964
UKIAH VALLEY MEDICAL CENTER 50.00 UKIAH 06292012@26
Invoice 08/24/2012 226952
UKIAH VALLEY MEDICAL CENTER 50.00 UKIAH 08102012@51
Invoice 07/03/2012 220989 UNIVERSAL PAIN MANAGEMENAT 50.00 PALMDALE 05212012@68
Invoice 07/26/2012 223659 UNIVERSAL PAIN MANAGEMENAT 50.00 PALMDALE 05212012@68 18
Response • DCDC duty officer notified each LHD Friday • 3 ASCs closed for weekend, notified Monday • Mendocino hospital notified Saturday • LAC issues HAN Friday night • Mendocino and Tulare EDs near facilities notified
Saturday • Facilities initiate telephone notification Tuesday-
Thursday • Monday 10-8 500/513 voice contact • Monday 10-15 512/513 voice contact (1 died)
19

California Methylprednisolone Update and Injection Type, October 19, 2012
• Exposed: 513 (all directly notified) • 425 spinal/paraspinal
– LA 156 – Ukiah 86 – Visalia 183
• Other injection sites 88 – LA 55 – Ukiah 11 – Visalia 22
20

Cases and Deaths with
Fungal Infections Linked to Steroid
Injections by State
10-29-12
21

22

23

New England Compounding Center (NECC) Preliminary Investigation Findings
THE COMMONWEALTH OF MASSACHUSETTS EXECUTIVE OFFICE OF HEALTH AND HUMAN SERVICES
Massachusetts Department of Public Health October 23, 2012
New England Compounding Center (NECC) Preliminary Investigation Findings
• DPH investigators principally communicated with three NECC staff members during the on-site investigation along with FDA investigators. After September 26, 2012, the majority of NECC employees were no longer on site. As has publicly been documented, NECC terminated many of their staff. The continuing investigation will include interviews of NECC employees.
24

SELECTED PRELIMINARY FINDINGS
• NECC distributed large batches of compounded sterile products directly to facilities apparently for general use rather than requiring a prescription for an individual patient.
• NECC distributed two of the recalled lots of methylprednisolone acetate (PF) 80 MG/ML prior to receiving results of sterility testing – While NECC’s records show the sterility tests found no contamination, the adequacy of NECC’s sterility testing methods are currently under examination
25

• Final sterilization of product did not follow proper
standards for autoclaving (sterilization through high pressure steam) pursuant to United States Pharmacopeia Standard 797 (USP 797) and NECC’s own Standard Operating Procedures: – Examination of NECC records indicated a systemic failure to
keep products in the autoclave for the required minimum 20-minute sterilization period necessary to ensure product sterility.
• NECC did not conduct proper validation of autoclaves pursuant to USP 797: – NECC failed to test their autoclaves to ensure proper function
• Powder hoods, intended to protect pharmacists from inhaling substances during medication preparation, within the sterile compounding area were not thoroughly cleaned pursuant to USP 797. – Residual powder was visually observed within the hood during
inspection. This contamination may subsequently lead to contamination of compounded medications
26
• Condition of “Tacky” mats, which are used to trap dirt, dust, and other potential contaminants from shoes prior to clean room entry, violated the USP 797. – Mats were visibly soiled with assorted debris.
• A leaking boiler adjacent to the requisite clean room created an environment susceptible to contaminant growth: – A pool of water was visually observed around the
boiler and adjacent walls, creating an unsanitary condition; the culture results of this potential contaminant are still pending
27
Outbreak of Serratia marcescens Infections following Injection of Betamethasone Compounded at a Community Pharmacy
• June 2001, Infectious Diseases Branch notified by Contra Costa County Public Health Department of 4 patients with Serratia marcescens meningitis at hospital A
28
Rachel Civen,1 Duc J. Vugia,2 Richard Alexander,4 Wendel Brunner,4 Sirlura Taylor,4 Nancy Parris,5 R. Wasserman,5 Sharon Abbott,3 S. B. Werner,2 and Jon Rosenberg2
1Los Angles County Department of Health Services, Acute Communicable Disease Control Program, Los Angeles, 2Infectious Diseases Branch and 3Microbial Diseases Laboratory, Division of Communicable Disease Control, California Department of Health Services, Richmond, 4Contra Costa County Public Health Department, Martinez, and 5John Muir Hospital, Walnut Creek, California
Clinical Infectious Diseases 2006; 43:831–7

• All 4 patients had received lumbar epidural injections of betamethasone between 29 May and 31 May 2001 at ambulatory surgery center (ASC) A, which is affiliated with hospital A, from 12 to 24 h before onset of their symptoms.
• The betamethasone used in these procedures had been compounded by pharmacy X, a community pharmacy near ASC A.
29
• All physicians who received any compounded injectable product from pharmacy X within the previous 6 months were notified and requested to examine their patients for infectious complications.
• Local hospital infection-control practitioners were asked to report culture-positive S. marcescens CNS and joint infections that had occurred in the previous 6 months.
30
• Initial 4 patients received betamethasone with a label preparation date of 17 May 2001.
• Compounding records at pharmacy X traced betamethasone to actual preparation day of 11 May 2001, when 60 5-mL vials were produced.
• 60 vials traced forward to 2 ASCs and 2 outpatient orthopedic practices
• All 78 patients who received betamethasone were evaluated for infectious complications.
31

32
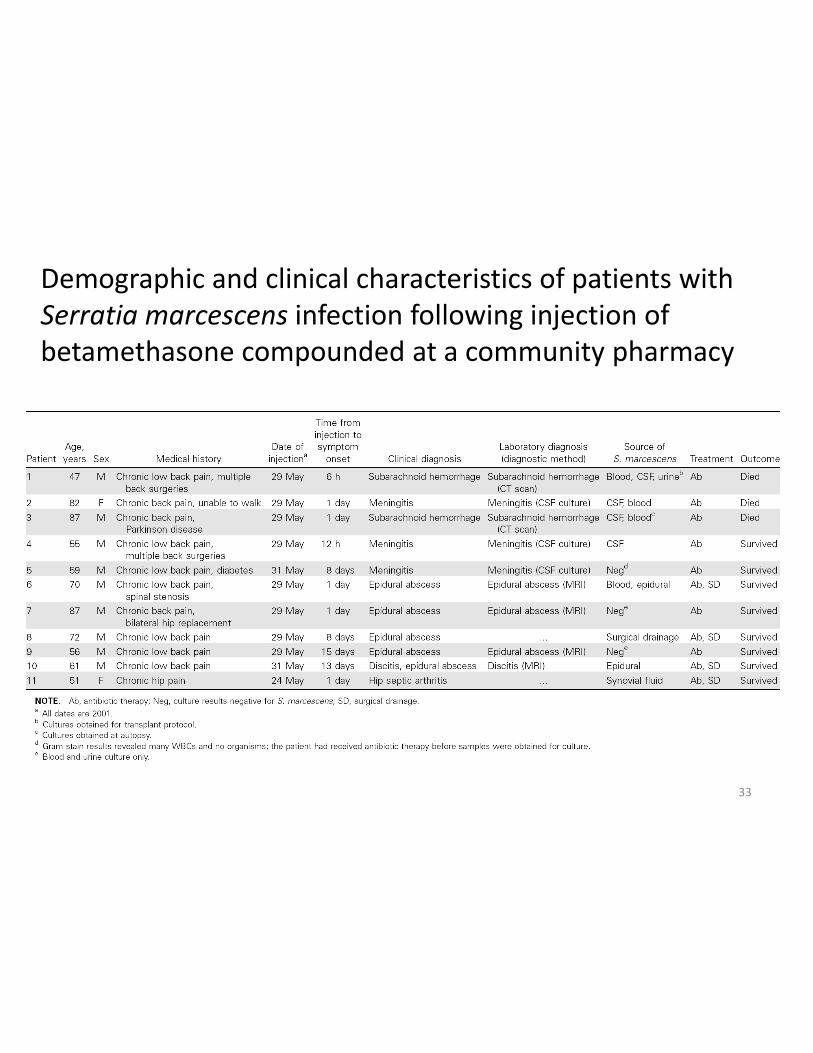
Demographic and clinical characteristics of patients with Serratia marcescens infection following injection of betamethasone compounded at a community pharmacy
33

• Pharmacy X technicians and pharmacists reportedly followed American Society of Health-System Pharmacists guidelines on quality assurance for pharmacy-prepared sterile products – recommended autoclaving both stock solutions
and final products
34

• The California Board of Pharmacy determined that on 11 May 2001 a technician autoclaved three 100-mL stock solutions but not the individual vials of betamethasone, as had previously been the practice. – The technician reported changing the automated
autoclave setting and eliminating terminal sterilization, because autoclaving of previous lots of betamethasone resulted in discoloration
– The 5-mL vials were cleaned with alcohol pads before pipetting the betamethasone
35

• Inadequacies – Sterilization techniques (i.e., inadequate
autoclaving temperatures and lack of final autoclaving step)
– Technical staff training – Labeling practices – Supervision of pharmacy technicians
• 10 individual ingredients used – Sodium carboxymethylcellulose 1% stock solution
grew S. marcescens • Methycellulose pellets (not a sterile product) used to
make the 1% carboxymethylcellulose solution were no longer present at pharmacy X
36

A Multistate Outbreak of Serratia marcescens Bloodstream Infection Associated with Contaminated Intravenous Magnesium Sulfate from a Compounding Pharmacy
• From 5 through 16 January 2005, 6 patients in LA Hospital had S. marcescens BSI – Indistinguishable PFGE – All in the Cardiac Surgery Unit
37
Rebecca H. Sunenshine, Esther T. Tan, Dawn M. Terashita, Bette J. Jensen, Marilyn A. Kacica, Emily E. Sickbert-Bennett, Judith A. Noble-Wang, Michael J. Palmieri, Dianna J. Bopp, Daniel B. Jernigan, Sophia Kazakova, Eddy A. Bresnitz, Christina G. Tan, and L. Clifford McDonald Clinical Infectious Diseases 2007; 45:527–33

No remaining product
38

NJ INVESTIGATION, MARCH 2005
• While deciding how to proceed, CDC received notification of second outbreak in NJ hospital
• + Culture of infusion administered to patient at BSI symptom onset and remaining MgSO4
• + Culture of sample from unopened bag of intravenous MgSO4 in same lot
39

• Compounding pharmacy X operated as outsourcing pharmacy (provides medications to other pharmacies) and prepared compounded products for hospitals in every state, except Ohio
• Compounded MgSO4 in multiple doses and purchased sterile components from pharmaceutical manufacturers
• Each lot of 50-mL of MgSO4 consisted of 240 units, sent to multiple facilities
40

• Did not test and retain samples of each lot for sterility, as do manufacturers
• No definitive source identified
• Manipulation of previously sterilized components by compounders, leading to an increased likelihood of the final product being contaminated
• Recalled and voluntarily ceased production and distribution of product
41

• FDA released guidance for 9 inappropriate activities, not enforceable by law – Pharmacy practiced 2 of 9
• Did not receive prescriptions for individual patients – State Board of Pharmacy issued a warning notice
• Failure to conform with applicable state laws
• Neither hospital pharmacy aware that product was compounded; no specific indication package labeling product was compounded
• Prior to this outbreak, many involved clinicians, pharmacy staff, and public health officials were unaware of the differences between compounded and manufactured sterile products
42

Multistate Outbreak of Postprocedural Fungal Endophthalmitis Associated with Sterile Products
from a Single Compounding Pharmacy, 2012
Christina A. Mikosz, MD MPH CDC Epidemic Intelligence Service Officer Los Angeles County Dept of Public Health
Presented At IDWeek, San Diego October 18, 2012
43
Endophthalmitis
Inflammation of intraocular cavities Usually caused by infection
Endogenous or exogenous
Exogenous infection Extension of keratitis
Complication of intraocular surgery
or procedures
Penetrating trauma

Endophthalmitis
Complicates 0.04% of intravitreal injections or vitrectomy surgeries Mostly bacterial, fungal even rarer
Extremely poor outcomes Repeat surgeries
Vision loss
From www.life-worldwide.org
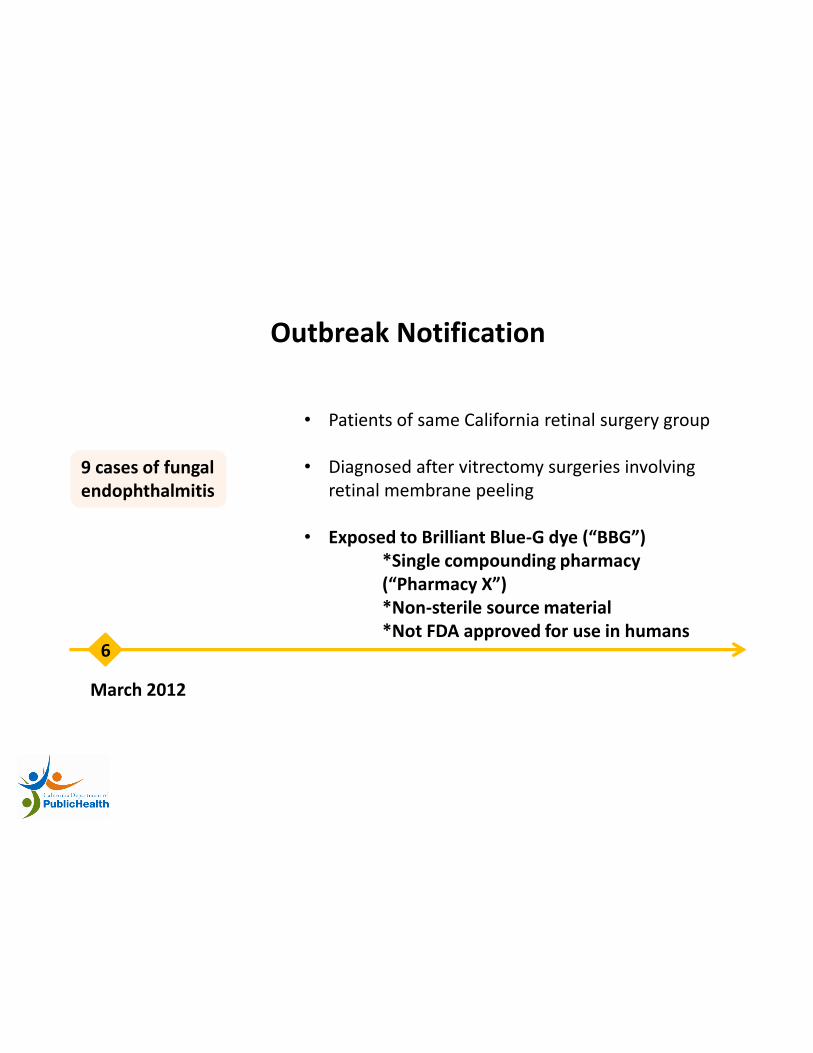
Outbreak Notification
March 2012
6
9 cases of fungal endophthalmitis
• Patients of same California retinal surgery group • Diagnosed after vitrectomy surgeries involving
retinal membrane peeling • Exposed to Brilliant Blue-G dye (“BBG”) *Single compounding pharmacy (“Pharmacy X”) *Non-sterile source material *Not FDA approved for use in humans
BBG from Pharmacy X
California surgery practice Unopened BBG vial Fusarium spp mold
Shipped to 22 ophthalmology practices in 15 states
Investigation initiated
Case Finding Strategies
Epi-X posts
FDA MedWatch alerts
Blast emails to: ClinMicroNet laboratories
American Society of Retinal Specialists
American Academy of Ophthalmologists
Review of available Pharmacy X sales records

Epidemiologic Investigation: BBG
21 fungal endophthalmitis cases 14 probable
7 confirmed
Fusarium incarnatum-equiseti species complex

3
4 1
1 9
3
BBG Case Distribution
50
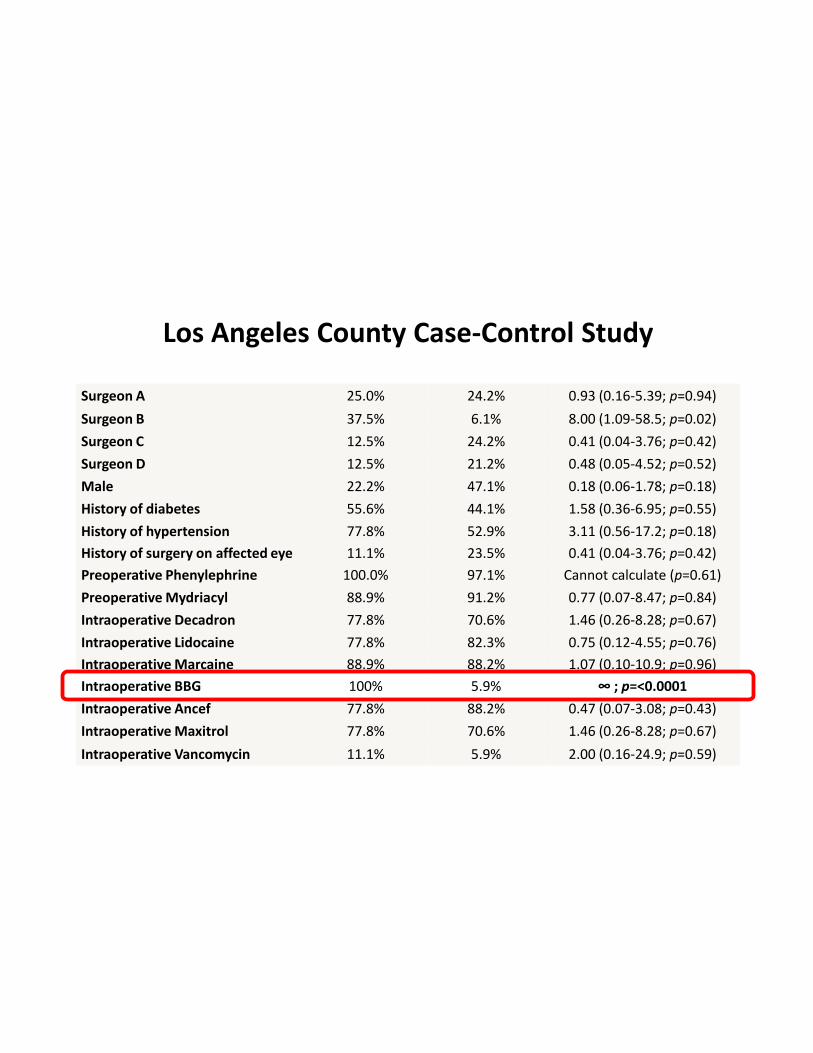
Los Angeles County Case-Control Study Exposure Cases (n=9) Controls (n=33) Odds ratio (95% CI; P-value)
Surgeon A 25.0% 24.2% 0.93 (0.16-5.39; p=0.94)
Surgeon B 37.5% 6.1% 8.00 (1.09-58.5; p=0.02)
Surgeon C 12.5% 24.2% 0.41 (0.04-3.76; p=0.42)
Surgeon D 12.5% 21.2% 0.48 (0.05-4.52; p=0.52)
Male 22.2% 47.1% 0.18 (0.06-1.78; p=0.18)
History of diabetes 55.6% 44.1% 1.58 (0.36-6.95; p=0.55)
History of hypertension 77.8% 52.9% 3.11 (0.56-17.2; p=0.18)
History of surgery on affected eye 11.1% 23.5% 0.41 (0.04-3.76; p=0.42)
Preoperative Phenylephrine 100.0% 97.1% Cannot calculate (p=0.61)
Preoperative Mydriacyl 88.9% 91.2% 0.77 (0.07-8.47; p=0.84)
Intraoperative Decadron 77.8% 70.6% 1.46 (0.26-8.28; p=0.67)
Intraoperative Lidocaine 77.8% 82.3% 0.75 (0.12-4.55; p=0.76)
Intraoperative Marcaine 88.9% 88.2% 1.07 (0.10-10.9; p=0.96)
Intraoperative BBG 100% 5.9% ∞ ; p=<0.0001
Intraoperative Ancef 77.8% 88.2% 0.47 (0.07-3.08; p=0.43)
Intraoperative Maxitrol 77.8% 70.6% 1.46 (0.26-8.28; p=0.67)
Intraoperative Vancomycin 11.1% 5.9% 2.00 (0.16-24.9; p=0.59)

Laboratory Testing: BBG Investigation
Patient Fusarium isolates
Unopened BBG vial Fusarium isolate
Indistinguishable by genetic sequencing

Epidemiologic Investigation
March 2012
26
Cluster of 4 new cases
6
Initial report
• Patients at same NY practice • Received intraocular injections of triamcinolone
• Triamcinolone compounded at Pharmacy X
Epidemiologic Investigation: Triamcinolone
22 fungal endophthalmitis cases linked to triamcinolone (TAC) exposure 9 probable
13 confirmed
Bipolaris hawaiiensis

10
8
2
2
TAC Case Distribution
55

California Case Characteristics (N=15)
BBG (n=9)
TAC (n=6)
Received antifungal treatment (%)
8 (89) 6 (100)
Vision loss (%) 7 (78) 5 (83) Additional surgeries during 6 month post-exposure period (%; range in # of surgeries)
9 (100; 2-3)
6 (100; 1-3)
Unresolved infection at 6 months post-exposure (%)
0 (0) 3 (50)

Public Health/Regulatory Action
March 2012
26 6
BBG report
TAC report
California Board of Pharmacy: cease/desist shipment of
Pharmacy X products
19
April 2012

Public Health/Regulatory Action
March 2012
26 6
BBG report
TAC report
April 2012
FDA: “microorganisms and fungal growth” in clean
room at Pharmacy X
May 2012
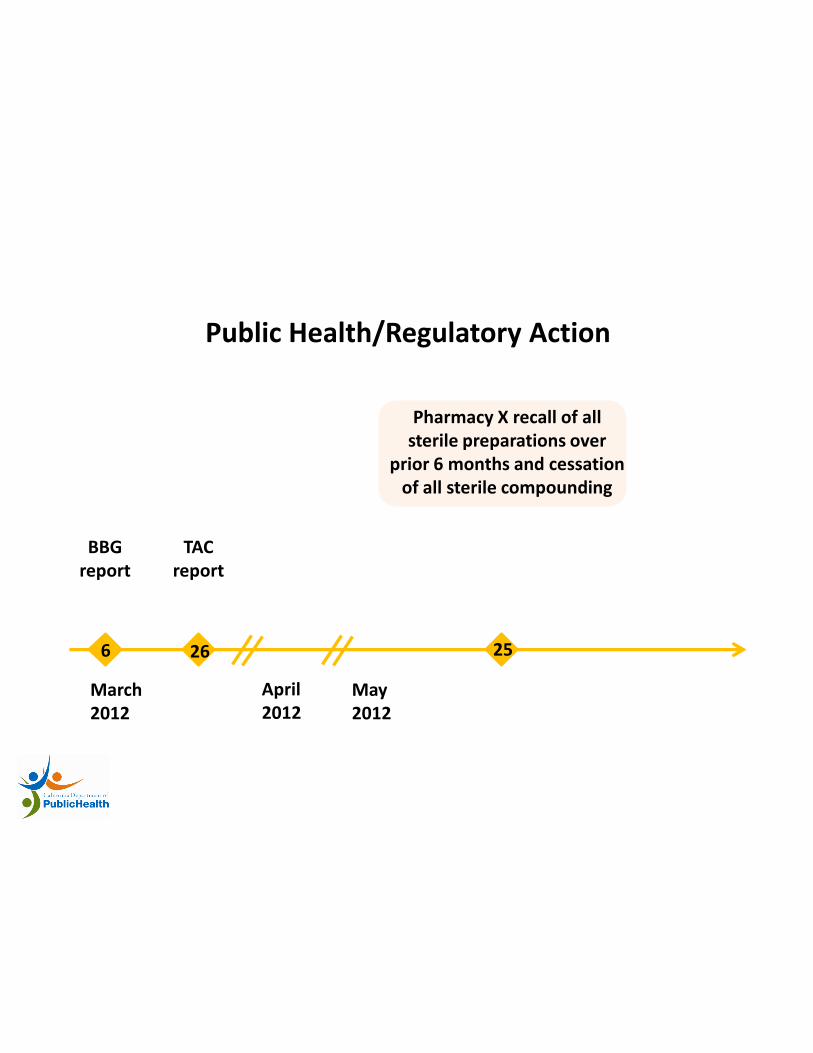
Public Health/Regulatory Action
March 2012
26 6
BBG report
TAC report
April 2012
May 2012
Pharmacy X recall of all sterile preparations over
prior 6 months and cessation of all sterile compounding
25

Public Health/Regulatory Action
March 2012
26 6
BBG report
TAC report
April 2012
May 2012
July 2012
Pharmacy X closed
31

Dear State Epidemiologists We realize that it is late on Friday. However we wanted to make you aware of a potentially serious situation that may require urgent attention over coming days. CDC, in partnership with state health departments and FDA, is investigating a cluster of clinical meningitis cases following spinal injection procedures for pain. We are writing this email to notify you of this investigation, and to encourage active surveillance among potentially exposed persons in your state.
61