ouch, that’s gottahurt! pediatric fractures & injuries · pediatric fractures & injuries...
TRANSCRIPT

© 2011 Children’s Mercy Hospitals and Clinics. All Rights Reserved. • June 2011© 2011 Children’s Mercy Hospitals and Clinics. All Rights Reserved. • June 2011
Ouch, That’s Gotta Hurt! Pediatric Fractures & Injuries
Greg Canty, MDMedical Director, Sports Medicine CenterAttending Physician, Emergency Medicine
Children’s Mercy Kansas City

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/132
Disclosures
• I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this CME activity
• I do not intend to discuss any unapproved/investigative use of a commercial product/device in my presentation

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/133
The Game Plan
• Review the unique features of pediatric bone
• Understand how to best assess suspected fractures in the urgent care
• Implement the latest evidence for acute management of fractures and injuries
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/134
Fractures in Pediatrics ?• 1/3 of patients will have a
fracture before age 17
• 42% boys & 27% girls
• 10‐15% of all childhood injuries involve a fracture
• Most common– Distal forearm
– Clavicle
– Fingers
– Ankle

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/135
The Pediatric Skeleton
• Bone porous and flexible…unique fractures• Periosteum is very thick & active• Ligaments are strong relative to the bone• Presence of the physis ‐ “weak link”• Ligament injuries & dislocations are less common – “kids don’t sprain”
• Fractures heal quickly and have the capacity to remodel

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/136
Anatomy of Pediatric Bone
• Epiphysis
• Physis
• Metaphysis
• Diaphysis
• Apophysis

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/137
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
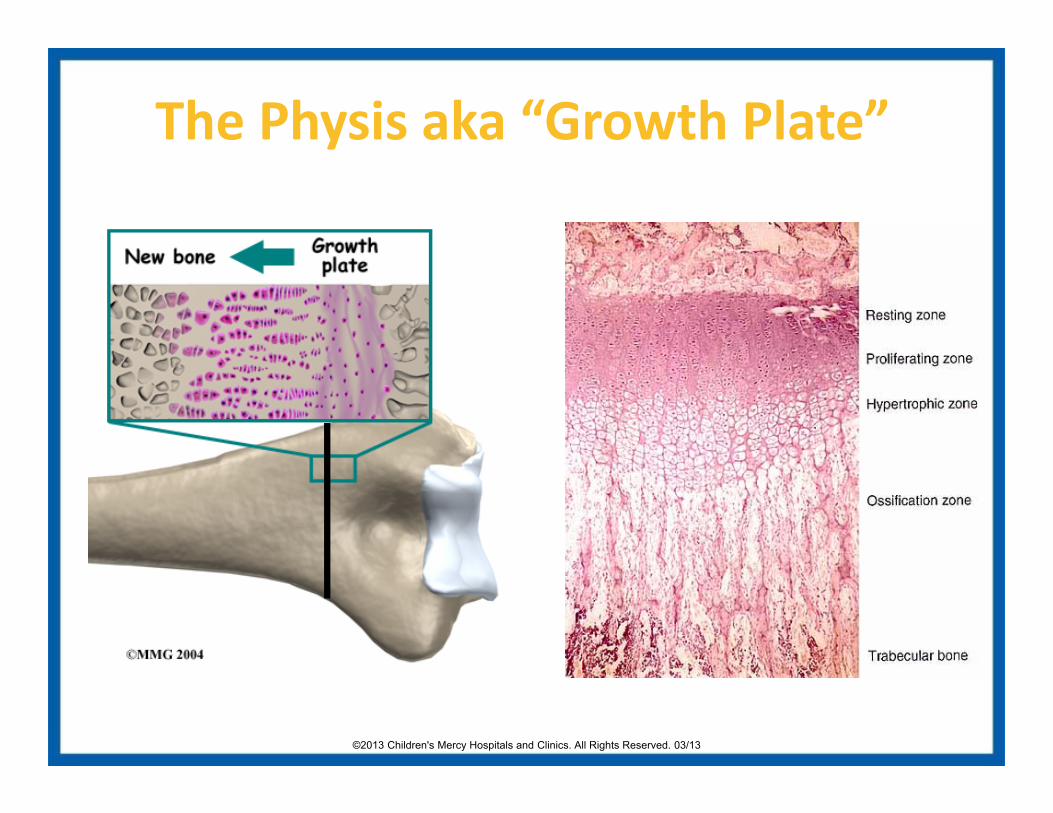
The Physis aka “Growth Plate”

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/139
Pediatric Fracture “Language”
• Buckle/ Torus – compression, stable
• Plastic Deformation – Bowing esp. fibula or ulna
• Greenstick – plastic deformity w/ partial fx on one side of the bone
• Complete ‐ Spiral, Oblique, Transverse
• Physeal – involves growth plate “Salter‐Harris fx”
• Avulsion – involves an apophysis

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1310
Buckle (Torus) Fracture
• Buckled Periosteum
• Metaphyseal/ diaphyseal junction

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1311
Greenstick Fracture
• Cortex Broken on Only One Side
– Incomplete

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1312
Plastic Deformation

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1313
Physeal Fractures - General
• “Weak link” of pediatric bone (cartilage)
• Adults=sprains....kids=fractures!
• Rapid healing (1/2 time of shaft fractures)
• Anatomic alignment critical
• Risk of premature growth arrest leading to limb length discrepancy or angular deformity

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1314
Physeal Fractures: Salter‐Harris

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1315
Salter-Harris 4Salter-Harris 3
Salter-Harris 1

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1316
“The History”
• Kids are not good historians• Mechanism - Any Fall
– Sports/Trampolines/ Monkey Bars/ Skating
• May not be much swelling, bruising or deformity• Non-weight bearing• Limp• Not using the arm• Be suspicious!

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1317
Musculoskeletal Physical Exam
1) Inspection: swelling, bruising, deformity, skin intact?
2) Gentle Palpation: focus on bony structures, crepitus, step‐offs, & growth plates
3) ROM: flexion, extension, abduction, adduction,
4) Neurovascular: motor function, sensation, and strength
5) Special maneuvers: ligaments, tendons, laxity

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1318
X‐Ray’s
• Consider 2‐3 views = AP, Oblique, Lateral
• Focus XR beam: try to pinpoint pain
• Minimize radiation when possible
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1319
Splinting: General Principals
• Inspect for any open wound, swelling, or deformity• Check distal pulse and neuro status• In general, immobilize the joint above and below the fracture
• Pad all rigid splints (minimum 2 layers, with 3 around bony prominences)
• When in doubt, splint! A sugar‐tong is safe choice.

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1320
Case #1
• 8 yo skateboarder fell yesterday onto his wrist
• Mild swelling but persistent pain
• Parents waited a few days because it didn’t look too bad

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1321
The FOOSH
• Fall On the Out Stretched Hand
• Common mechanism – Forearm fx’s #1
• Distal radius fractures = ¼ of all pediatric fx’s
• Excellent remodeling capability
• Growth disturbance is unusual
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
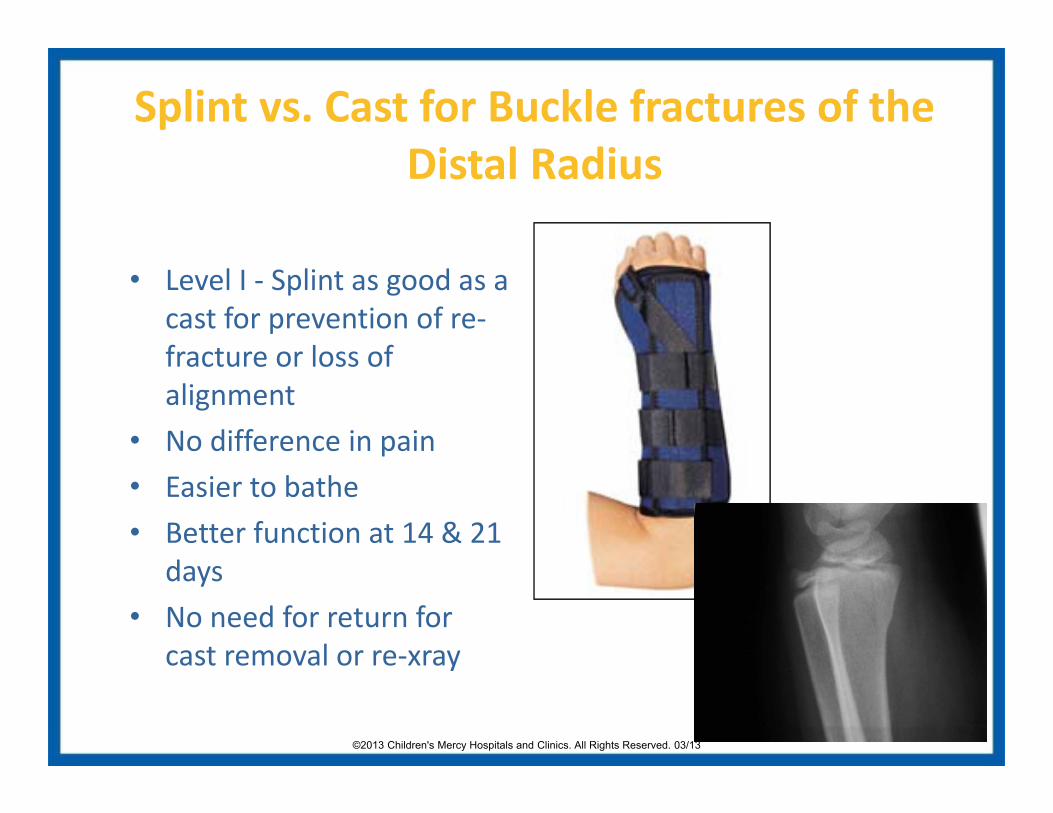
Splint vs. Cast for Buckle fractures of the Distal Radius
• Level I ‐ Splint as good as a cast for prevention of re‐fracture or loss of alignment
• No difference in pain• Easier to bathe• Better function at 14 & 21
days• No need for return for
cast removal or re‐xray

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1323
Case #2• 16 y/o basketball player lands on outstretched hand after getting undercut while getting rebound (FOOSH)
• Now c/o Right Wrist Pain
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1324
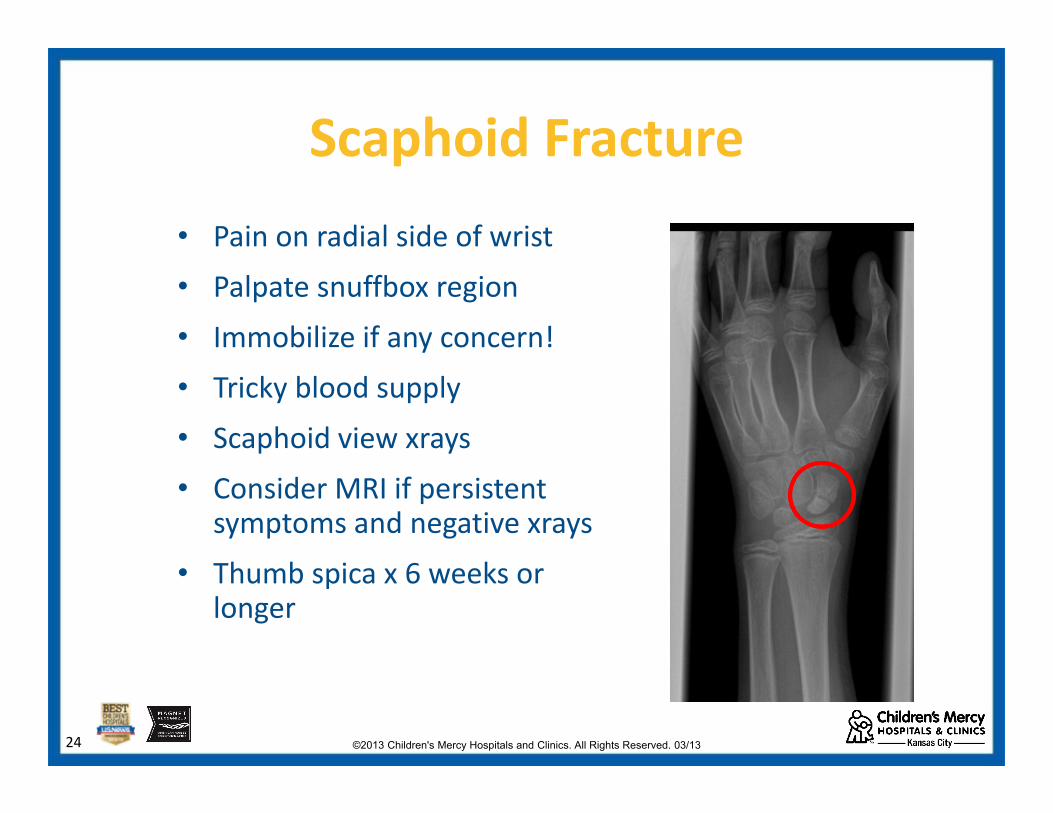
Scaphoid Fracture• Pain on radial side of wrist
• Palpate snuffbox region
• Immobilize if any concern!
• Tricky blood supply
• Scaphoid view xrays
• Consider MRI if persistent symptoms and negative xrays
• Thumb spica x 6 weeks or longer

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1325
Case #3
• 15 y/o QB is tackled hard and crashes into the ground landing on his right shoulder
• He has severe shoulder pain and refuses to raise his Right arm

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1326
Differential to Consider
• Acromioclavicular sprain– Shoulder separation
• Fracture
• Sternoclavicular dislocation
• Glenohumeral dislocation

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
CLAVICLE FRACTURE
An Example of Pediatric Healing Potential
8 weeks

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1328
Be Careful !
Palpate both ends of the clavicle!

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1329
Treatment
• Sling for pain/protection
– vs. Figure of 8 brace
• Pain Control
• Progressive ROM/Strengthening
• RTP ?? – Clavicle fx: Contact sports ~ 8 weeks

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1330
Case #4• 9 yo fell off monkey bars
earlier today
• C/o elbow pain and swelling
• Refuses to fully extend elbow due to pain and swelling
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1331
Elbow Fractures• Multiple physes
• Look for swelling
• Effusion
– Loss of flexion/ extension
– No loss of supination/ pronation
• Typically supracondylar in the very young and radial head in the older child

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1332
Ossification Centers of the Elbow (CRITOE):
• C = Capitellum
• R = Radial Head
• I = Internal (Medial)
• T = Trochlea
• O = Olecranon
• E = External (Lateral)
• 2 Years
• 4 Years
• 6 Years
• 8 Years
• 10 Years
• 12 Years

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
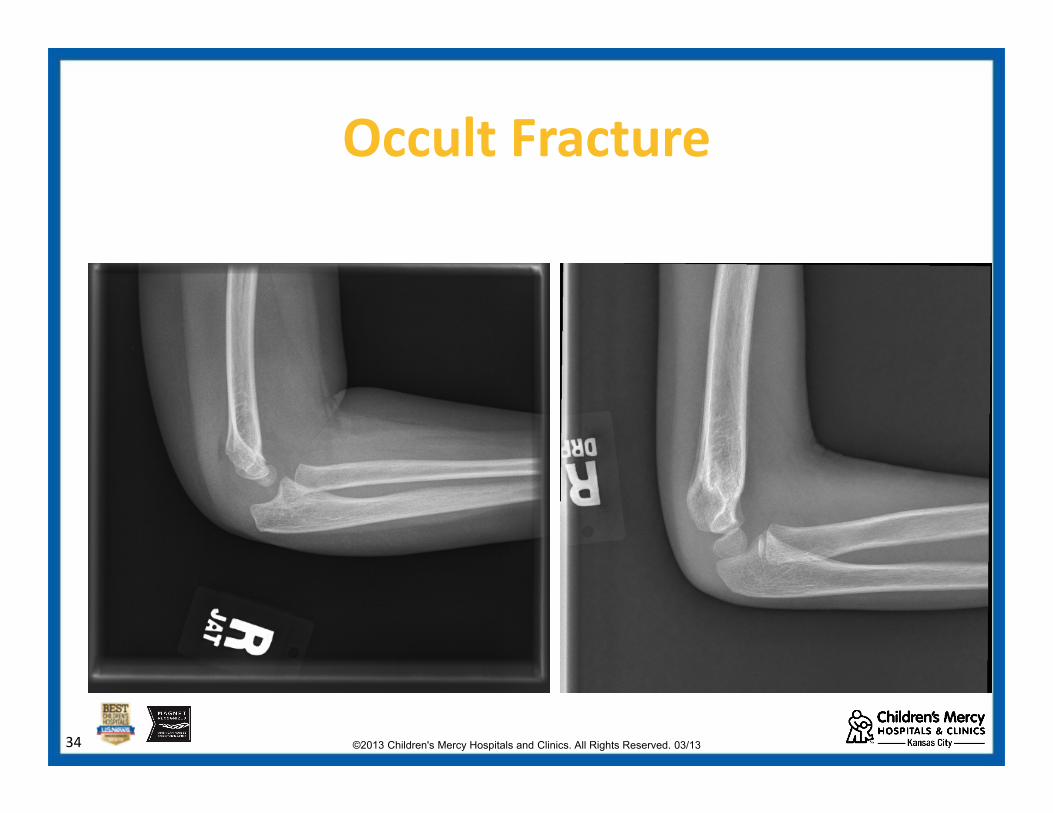
Elbow Fat Pads
• Anterior – normal if lying flat against the humerus, abnormal if elevated – “sail sign”
• Posterior – always pathologic!
• Indicates hemarthrosis
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1334
Occult Fracture

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1335
Case #5
16 yo male football player injured left 4th
finger while tackling an opposing player…

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1336
Jersey Finger • Mechanism‐ forced extension of
a flexed distal phalange• Flexor digitorum profundus
tendon avulsed (+/‐ bony fragment)
• Inability to flex the DIP when the PIP joint is stabilized
• Splint in comfortable position• MUST RECOGNIZE EARLY!!
Requires repair within 7‐10 days

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1337
Case #6
15 yo female basketball player injured her index finger while catching a pass

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1338
Mallet Finger
• Mechanism is direct blow onto an extended distal phalanx; “Jammed finger”
• Occurs when catching ball• Extensor digitorum
ruptures & DIP assumes flexed position (? pain)
• Xray for avulsion fracture

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1339
Mallet Finger
Treatment ‐• Constant splinting of the DIP in full extension/hyperextension x 6‐8 weeks
• May RTP with proper splint when pain controlled
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
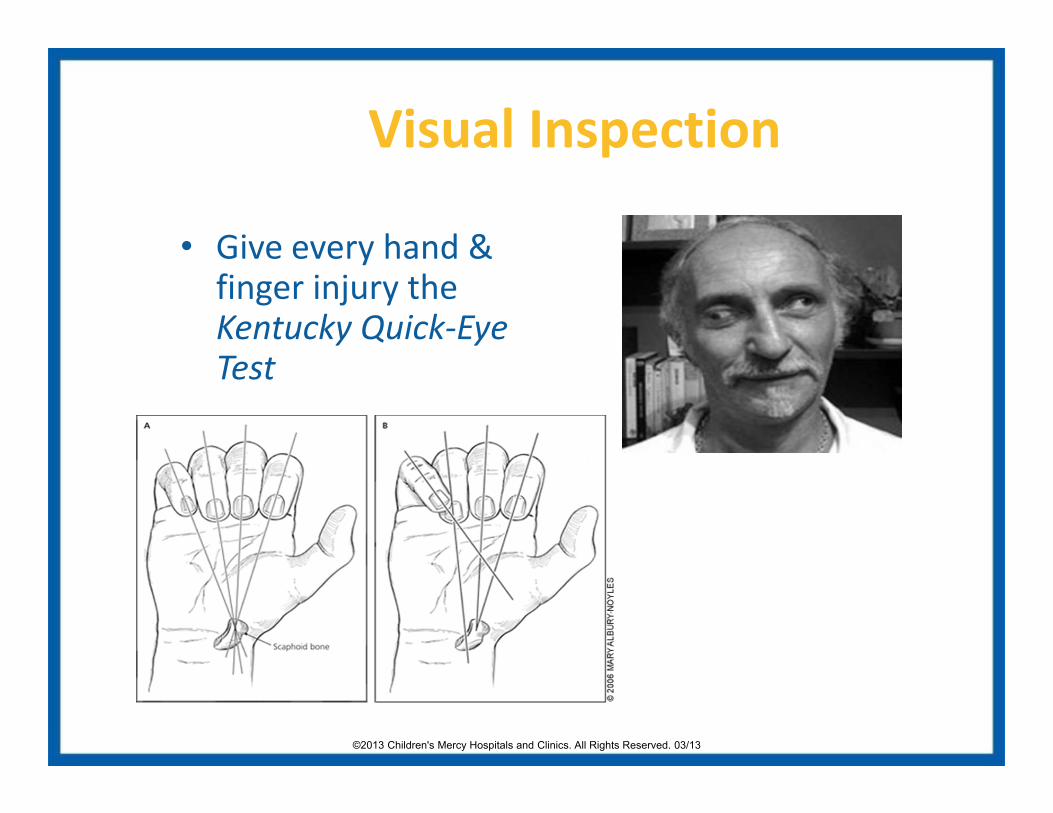
Visual Inspection
• Give every hand & finger injury the Kentucky Quick‐Eye Test
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
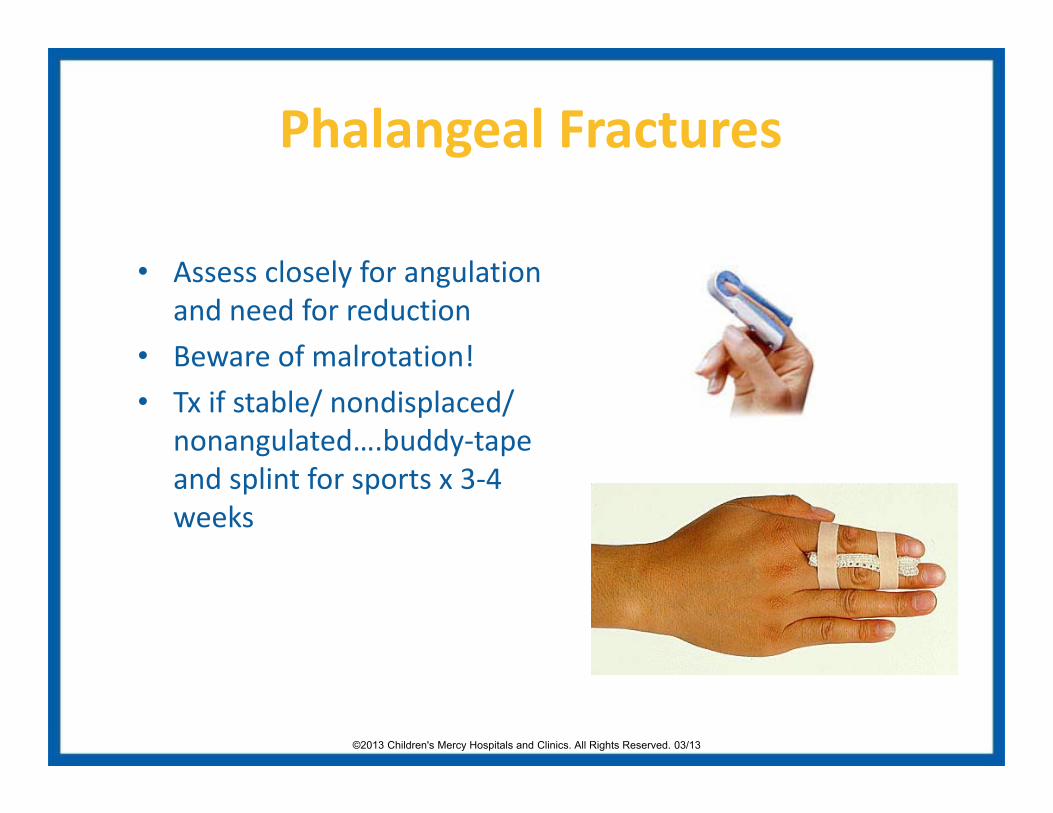
Phalangeal Fractures
• Assess closely for angulation and need for reduction
• Beware of malrotation!• Tx if stable/ nondisplaced/
nonangulated….buddy‐tape and splint for sports x 3‐4 weeks

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1342
Case #8
• 15 yo football player presents on Sat morning
• He recalls an inversion ankle injury when he stepped on another player’s foot
• He was able to limp afterwards but unable to run

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/13
Ottawa Ankle Rules• Ankle x-rays if ankle pain with: 1) bony tenderness
along the posterior edge/tip of lateral or medial malleolus or 2) inability to bear weight for 4 steps
• Foot x-rays if foot pain with: 1) bony tenderness at the base of the 5th metatarsal or 2) bony tenderness of the navicular bone or 3) inability to bear weight for 4 steps
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1344

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1345
The Pediatric “Ankle Sprain”Distal Fibula Fractures
• Common in youth and pre-adolescent athletes
• Always palpate the physis!
• Salter Harris I fractures are a clinical diagnosis
• Excellent Prognosis

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1346
Removable Ankle Braces• Isolated distal fibula
fractures are very common
• Most are very low-risk
• Casting vs. splinting
• Quicker return to baseline activities
• 57% casted group would have preferred brace!

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1347
“Ankle Injuries” with Foot Pain5th Metatarsal Avulsions• Caused by pulling of the
peroneus brevis• Always feel the bump!• CAM walker boot

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1348
Toddler’s fracture
• Any toddler with a mechanism and refuses to bear weight
• Regardless of exam or xray
• Wee Walker

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1349
Case #8
• A 13 y/o gymnast presents with right hip pain and the inability to bear weight. She felt a “pop” in her hip while doing the splits.

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1350
Her most likely diagnosis is…
a) Femur fracture
b) Hamstring strain
c) Pelvic avulsion fracture
d) Slipped capital femoral epiphysis(SCFE)

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1351
Ischium Avulsion
• On exam she had limited ROM with hip flexion, hip IROM, knee extension.
• She was tender to palpation over the ischium.

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1352
Pelvic Avulsion Fractures
• Occur with aggressive, athletic motions
• AIIS ‐ soccer/rugby
• ASIS ‐ sprinters/soccer
• Ischium ‐gymnasts/hurdlers
• Crutches, NWB, pain control

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1353
Case #9
• 16 yo runner (XC and track) presents with L‐hip pain x month
• Worse w/ running
• Does not recall injury

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1354
Femoral Neck Stress Fracture
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1355
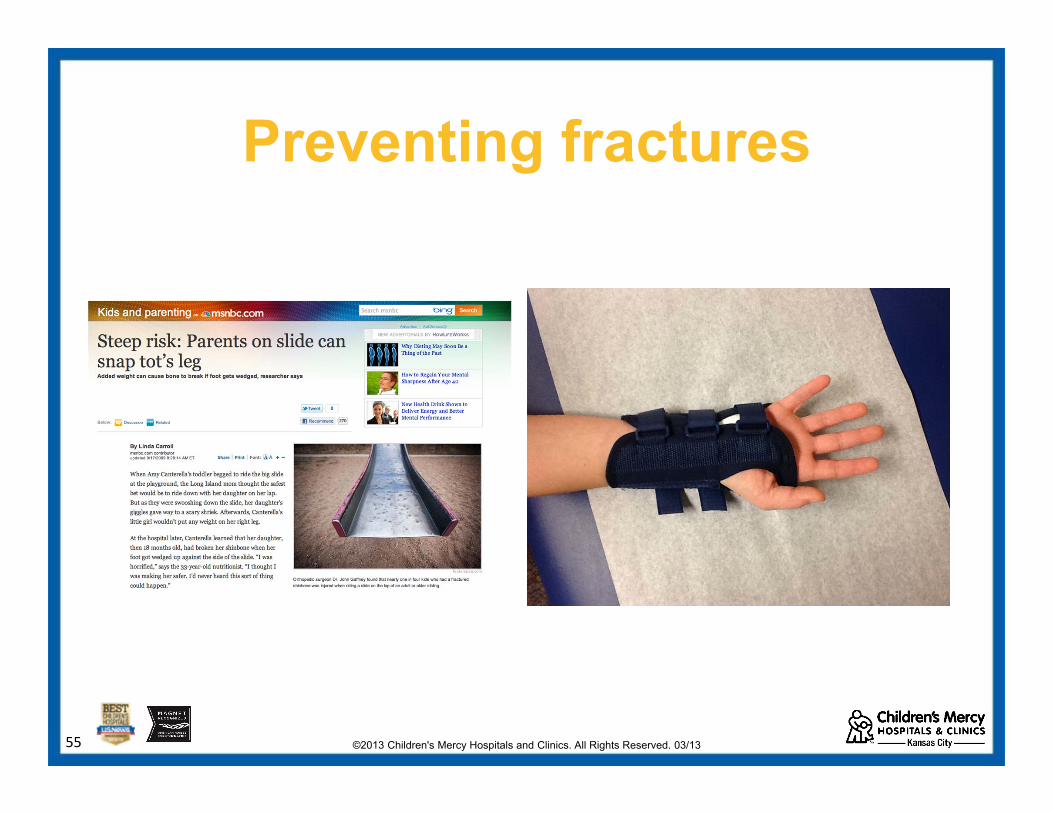
Preventing fractures

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1356
Summary• The pediatric bone is unique and the
forces may change during bony development
• Proper fracture recognition and initial management is important in urgent care
• Removable splinting wonderful for many fractures
©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1357
Sports Medicine Center (816) 701-HURT (4878)
• Stress fractures
• Sports-related concerns– Exercise induced
bronchospasm
– Spondylolysis
– Mono in the athlete, etc
• Sports-related fractures
• Acute sports-related injuries & dislocations
• Sports-related concussion
• Overuse syndromes

©2013 Children's Mercy Hospitals and Clinics. All Rights Reserved. 03/1358
Questions ?