otolith and bppv use file - university of floridaapplied vestibular anatomy 29 head moves to the...
TRANSCRIPT

2/3/2016
1
How the Labyrinth Works…
11
Inner Ear: “On Top of a Long Stalk”
Vestibular Function SCCs:
©2012 MFMER | slide-13
• Semicircular canals• Translates angular rotation movements of
the head around the pivot point of the neck• Information used by the CNS to coordinate:
• Eye movements• Upper torso movement• Hand movements while moving
• See aVOR app in the iTunes Store
Vestibular Function Otoliths:
©2012 MFMER | slide-14
Micro-Structure of the Macula
Utricle Encoding: Static Tilt and Acceleration
www.utdallas.edu/~tres/integ/ sen5/sense_5.html

2/3/2016
2
Primary Goal of Otolith Organs
• Anti-gravity muscle tone • Vestibular Spinal Reflexes (VSR)
• Vestibular Ocular Reflexes :• Maintain registration of the retina with
gravitational vertical • Horizontal meridian of the retina aligns
automatically with the horizon
Macula: Linear Translations and Low Frequency Tilts
• Sensitive to movements about the...
•Hips•Ankles
• Play an important role in maintaining upright stance
Ocular Tilt Reaction
Modified from: Brandt & Dietrich, 2000, in S.J. Herdman, Vestibular Rehabilitation
Vestibulo-Macular Ocular Reflex
Goal: Keep eyes aligned with gravitational vertical
Common Otolith Disorders
• BPPV• Most common cause of vertigo in adults
• Superior vestibular nerve “neuro-laybrinthitis”• Second most common cause of dizziness
• Clinically:• “Neuronitis”
• Vestibular symptoms only• “Labyrinthitis”
• Auditory and vestibular symptoms
21
Major Nerves In The Internal Auditory Canal (IAC)
FN
CN
SVN
IVN
Facial N. - Superior & AnteriorCochlear N. - Inferior & AnteriorSuperior Vestibular N.Inferior Vestibular N.
A P

2/3/2016
3
Vestibular Tests and Eighth Nerve BranchesWe can now measure all sensory structures and nerve branches of the inner ear
• Audiological Evaluation
• Caloric response
• oVEMP
• cVEMP• vHIT
• Cochlea• Horizontal SCC (SVN)
• Utricle (SVN)• Saccule (IVN)• All SCCs (SVN/IVN)
©2012 MFMER | slide-23
Vestibular Study
• Normal• Ocular motor• (-) positional
nystagmus -50 -40 -30 -20 -10 0 10 20 30 40 50
Warm
Cold
Caloric Responses 80% LEFT WEAKNESS
Left Right
©2012 MFMER | slide-24
Absent cVEMP on LEFT Absent oVEMP on LEFT
Summary Points Three SSC
Encode angular rotation about cervical spine◦ Two otolith organs
Encode linear translations and drive strong neck and spine muscle reflexes.
Vestibular Nerve: LSU on top!
Vestibular nuclei (VN) and cerebellum involved with VOR / VSR / autonomic tone
Applied Vestibular Anatomy
25
Ways to Understand the Vestibulo-Ocular Reflex
Applied Vestibular Anatomy
26
Right Semi-Circular Canal Cup • Cup is in the place of the right
SSC•Handle is in the position of the ampulla•Cap represents endolymphposition before any head movement
• Note position of the utricle (medial)
Applied Vestibular Anatomy
27
Head Moves to the left... Ampulla moves with the
head (to the left)◦Cap does not move, but changes position relative to the ampulla due to head movement (curved arrow)
It “lags behind” the head movement
Endolymph moves through the ampulla, away from the utricle
Applied Vestibular Anatomy
28

2/3/2016
4
Head Moves to the Right• Ampulla moves with the head
(to the right)•Cap does not move, but changes position relative to the ampulla due to head movement
• Endolymph moves through the ampulla, toward from the utricle
Applied Vestibular Anatomy
29
Head Moves to the Right
The long arrow (endolymph) does not change its orientation…neither do the eyes.
Vestibular eye movements lawfully reflect relative movement of endolymph in the SCCs
Applied Vestibular Anatomy
30
Vestibulo-Ocular Reflex (VOR)
Shepard and Telian 1995Applied Vestibular Anatomy
31
Semicircular Canal aVOR
• Goal:• Maintain visual stability (visual image on
retina) despite “angular” head movements about cervical spine
Applied Vestibular Anatomy
32
Semicircular Canal aVOR
• Three orthogonal SSCs reflect movements in three dimensions
• Three SCCs pairs (left and right) are coplanar
• When one SCC is stimulated, its coplanar complement is inhabited
Applied Vestibular Anatomy
33
A word about nerve firing rates...
Applied Vestibular Anatomy
34

2/3/2016
5
Applied Vestibular Anatomy
35
Firing Rate Example (Hypothetical)
100 100
0
100
200
300
400
500
600
Left Ear Right Ear
• When the head is still, both nerves fire at about 100 spikes/sec.
Applied Vestibular Anatomy 36
Firing Rate Example (Hypothetical)
5
200
0
100
200
300
400
500
600
Left Ear Right Ear
• Head turns to the right at a velocity of 40 degrees / sec,
• Discharge rate increases in the right (leading) ear
• Discharge rate decreases in the left (lagging) ear
Applied Vestibular Anatomy 37
Firing Rate Example (Hypothetical)
5
200
0
100
200
300
400
500
600
Left Ear Right Ear
• The brain interprets this asymmetry in nerve output between ears as a head movement to the right at 40 deg/sec.
• The brain moves the eyes to the left at 40 deg/sec
• vestibular slow phase movement of nystagmus
Applied Vestibular Anatomy 38
Firing Rate Example (Hypothetical)
0
400
0
100
200
300
400
500
600
Left Ear Right Ear
• When the head turns to the right at 100 deg/sec.
• The right nerve firing rate jumps up
• The left ear cannot change
• You can’t fire less than zero times / sec ;-)
Applied Vestibular Anatomy 39
Firing Rate Example (Hypothetical)
0
400
0
100
200
300
400
500
600
Left Ear Right Ear
• Any angular head movement that exceeds a critical velocity is encoded entirely by the leading ear.
• The “lagging ear” contributes little to the VOR at high velocities of rotation
Applied Vestibular Anatomy 40

2/3/2016
6
How Is This Helpful?…. Head Thrust Test
(+)
(-)
Jacobson et.al.,Applied Vestibular Anatomy
41
Ecological Approach to Vestibular Evoked Eye Movements
• Vestibular evoked eye movements are designed to:
• Maintain gaze stability during unexpected head / body movements
• Maintain eye orientation so that the horizon lines up with the horizontal meridian of the retina
42
Applied Vestibular Anatomy
A Model...
Right Left
Applied Vestibular Anatomy
43
PHA
PHARight Left
Applied Vestibular Anatomy
44
SSC Planes
Six SSCs are matched in complement pairs -three planes…◦ Two Horizontal◦ Right Anterior and Left
Posterior
(RALP)◦ Left Anterior and Right
Posterior
(LARP)
RALPLARP
Right Left
Applied Vestibular Anatomy
45
Law of Reciprocal Innervation
• Head movements that stimulate the nerve of one canal, inhibit output in the complementary canal
• Leading Ear Excites• Lagging Ear Inhibits
RALPLARP
Right Left
Applied Vestibular Anatomy
46
2/3/2016
7
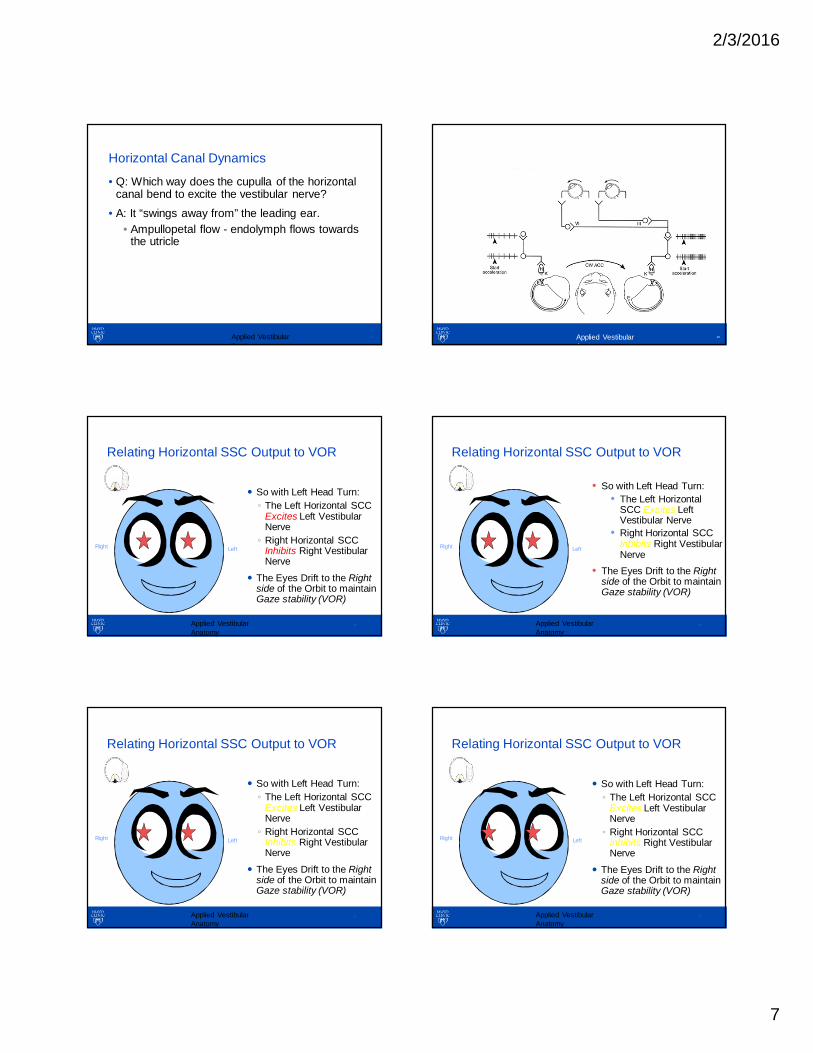
Horizontal Canal Dynamics
• Q: Which way does the cupulla of the horizontal canal bend to excite the vestibular nerve?
• A: It “swings away from” the leading ear.• Ampullopetal flow - endolymph flows towards
the utricle
Applied Vestibular Anatomy
47
Horizontal Canal Dynamics
Applied Vestibular Anatomy
48
Relating Horizontal SSC Output to VOR
So with Left Head Turn:◦ The Left Horizontal SCC
Excites Left Vestibular Nerve ◦ Right Horizontal SCC
Inhibits Right Vestibular Nerve
The Eyes Drift to the Right side of the Orbit to maintain Gaze stability (VOR)
Right Left
Applied Vestibular Anatomy
49
Relating Horizontal SSC Output to VOR
Right Left
• So with Left Head Turn:• The Left Horizontal
SCC Excites Left Vestibular Nerve
• Right Horizontal SCCInhibits Right Vestibular Nerve
• The Eyes Drift to the Right side of the Orbit to maintain Gaze stability (VOR)
Applied Vestibular Anatomy
50
Relating Horizontal SSC Output to VOR
So with Left Head Turn:◦ The Left Horizontal SCC
Excites Left Vestibular Nerve ◦ Right Horizontal SCC
Inhibits Right Vestibular Nerve
The Eyes Drift to the Right side of the Orbit to maintain Gaze stability (VOR)
Right Left
Applied Vestibular Anatomy
51
Relating Horizontal SSC Output to VOR
So with Left Head Turn:◦ The Left Horizontal SCC
Excites Left Vestibular Nerve ◦ Right Horizontal SCC
Inhibits Right Vestibular Nerve
The Eyes Drift to the Right side of the Orbit to maintain Gaze stability (VOR)
Right Left
Applied Vestibular Anatomy
52

2/3/2016
8
Relating Horizontal SSC Output to VOR
At some point, gaze stability cannot be maintained and a saccade moves the eyes to a new fixation target…◦ Nystagmus “Fast
phase”◦ Not Vestibular Induced
Right Left
Applied Vestibular Anatomy
53
Understanding Vertical SSCs
• “Goals” of VOR• Maintain Gaze stability
despite head movement• Maintain eyes oriented to
the horizon• Gravitational
Horizontal should line up with horizontal meridian of retina
RALPLARP
Right Left
Applied Vestibular Anatomy
54
• What Kind of Eye Movement Is Necessary When Moving in the “Right - Anterior , Left Posterior” (RALP) Plane?
Applied Vestibular Anatomy
55
RALP Movement
• Turn Head 45o to Left
• RALP Movement:• Tilt Forehead Down• Look Straight
Ahead• What Do Eyes Do?
Right Left
Applied Vestibular Anatomy
56
RALP Movement
• Turn Head 45o to Left
• RALP Movement:• Tilt Forehead Down• Look Straight
Ahead• What Do Eyes Do?
Right Left
Applied Vestibular Anatomy
57
RALP Movement
• Turn Head 45o to Left
• RALP Movement:• Tilt Forehead Down• Look Straight
Ahead• What Do Eyes Do?
Right Left
Applied Vestibular Anatomy
58

2/3/2016
9
RALP Movement
• Right Eye elevates
• Slight Counter Clockwise Torsional eye movement (relative to the patient)Right Left
Applied Vestibular Anatomy
59
RALP Movement
• At some point, gaze stability cannot be maintained and a saccade moves the eyes to a new fixation target…
•Nystagmus “Fast phase”•Not Vestibular Induced
Right Left
Applied Vestibular Anatomy
60
RALP Movement This is the Effect of Right
Anterior Canal Stimulation (When looking to the right):◦ Right Eye elevates◦ Slight Counter-clockwise
Torsional “Slow phase” eye movement (relative to the patient)Right Left
Applied Vestibular Anatomy
61
RALP Movement
When looking to the left of Right Anterior Canal Stimulation provokes:◦ Minimal vertical
movement◦ Counter-clockwise
Torsional “Slow phase” eye movement (relative to the patient)
Right Left
Applied Vestibular Anatomy
62
RALP Eye Movements
• Vertical component changes with direction of gaze
• Eye movement remains “in the plane of” the dependent canals (Arrow)
RALPLARP
Right Left
Applied Vestibular Anatomy
63
RALP Plane Movements
Looking LeftLooking Right
- Plane of rotation is the same regardless of gaze direction- Trajectory of the pupil depends on direction of gaze
Applied Vestibular Anatomy
64

2/3/2016
10
Vertical Canal Cupula
• How does the cupula of the leading vertical canal move when the head tilts in the RALP plane?
Applied Vestibular Anatomy
65
Vertical Canal Dynamics
• It “falls” toward the head tilt.• Ampullofugal Flow or Flow away from the
utricle.
Parnes et.al, 2003
Applied Vestibular Anatomy
66
Summary Point: #1
• Vestibular Induced Eye Movements:• Maintain gaze stability during unexpected
head / body movements• Maintain eye orientation so that the horizon
lines up with the horizontal meridian of the retina
Applied Vestibular Anatomy
67
Summary Point: #2
• In Angular Head Movements• The leading canal excites the vestibular
nerve • Lagging canal suppresses vestibular nerve
firing• Provokes a slow eye movement in the
opposite direction of the head movement (Ewald).
• The leading canal will drive eye movements in response to fast accelerations (Ewald).
Applied Vestibular Anatomy
68
Summary Point: #3
• For horizontal or “yaw” type of excitatory movements, the cupula lags behind the leading ear
• For vertical movements (RALP or LARP planes), the cupula falls in the direction of the head movement
Applied Vestibular Anatomy
69
BPPV Induced Eye Movements
Applied Vestibular Anatomy
70

2/3/2016
11
Benign Paroxysmal Positional Vertigo (BPPV)
• Intense but transient vertigo provoked by moving into specific head positions
• Most common cause of vertigo• Accompanied by a characteristic nystagmus• Thought to be caused by debris in the
semicircular canals• Can be treated by a simple in office
procedure
71Applied Vestibular Anatomy
Understanding BPPV Induced Eye Movements
• Simple forms are easy to recognize:• Posterior SSC BPPV is torsional, with the
top pole of the eye rolling to the floor.• For more complicated types of nystagmus:
• Relate the eye movement to the type of head movement that would normally drive the eyes in that direction.
• “Analogous Equivalent Movement”
72Applied Vestibular Anatomy
Applied Vestibular Anatomy
73
Dix-Hallpike or Nylen Maneuver
Furman and Cass “Benign Paroxysmal Positional Vertigo.” NJM 1999.
Characteristic Response
• Torsional nystagmus (rolling eye movement) & vertiginous sensation
• Onset latency (5-45 sec)• Crescendo then fatigues
(typically within 30 sec)• Symptoms extinguish (adapt)
over repeated trials
Applied Vestibular Anatomy
74
Analogous Equivalent Head Movement
• Analogous equivalent head movement• Visualize which semicircular canals would be
stimulated or inhibited during such a movement
• This will tell you where the debris rests in the labyrinth.
75Applied Vestibular Anatomy
Posterior Canal BPPV
• Eye movement:•Top of eye rolls to the floor
•Counter clockwise (relative to the patient)
•Up beating component, >in the contralateral eye
• Eye movement is analogous to falling in the plane of the involved posterior canal
Applied Vestibular Anatomy
76

2/3/2016
12
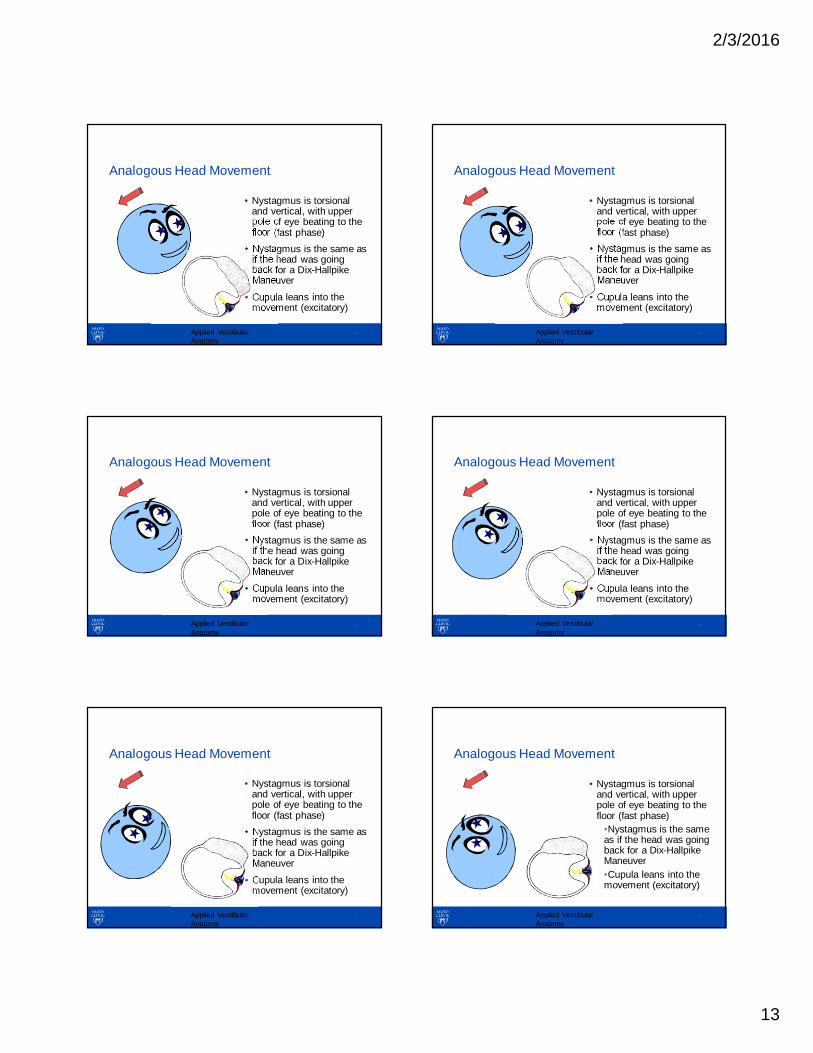
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
77
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
78
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
79
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
80
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
81
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
82
2/3/2016
13
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
83
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
84
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
85
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
86
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
87
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
•Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver•Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
88

2/3/2016
14
Analogous Head Movement
• Nystagmus is torsional and vertical, with upper pole of eye beating to the floor (fast phase)
• Nystagmus is the same as if the head was going back for a Dix-Hallpike Maneuver
• Cupula leans into the movement (excitatory)
Applied Vestibular Anatomy
89
Right Posterior Canal BPPV
Applied Vestibular Anatomy
90
Head in the Dependent Position
• Same up and clockwise (relative to the patient) torsional nystagmus as when moving into the Dix-Hallpike position from sitting.
• Onset delay• Upward component
greatest with gaze to the left
Applied Vestibular Anatomy
91
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
92
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
93
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
94

2/3/2016
15
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
95
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
96
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
97
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
98
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
99
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
100

2/3/2016
16
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
101
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
102
Debris Falls From the Pull of Gravity
Cupula bends Same Up and Clockwise
(relative to the patient) Torsional Nystagmus as when moving into the Dix-Hallpike Position From Sitting.◦Onset delay◦Upward component greatest with gaze to the left
Applied Vestibular Anatomy
103
Posterior Canal Variety
• Eye movement is analogous to falling in the plane of the involved posterior canal
•Top of eye rolls to the floor
•Counter clockwise (relative to the patient)
•Up beating component, >in the contralateral eye
Applied Vestibular Anatomy
104
Dizzy!
Dizzy! Could be Dizzy!
Epley ManeuverRight Posterior Canal
Applied Vestibular Anatomy
105
Superior Canal Variations
Modified from: Furman & Cass Benign Paroxysmal Positional Vertigo. NJM, 341:21 1999
Applied Vestibular Anatomy
106

2/3/2016
17
Applied Vestibular Anatomy
107
Contralateral SC-BPPV Quick Rules of Thumb
• For vertical / torsional nystagmus…
• Up-beating eye implies the contralateral posterior canal
• Down-beating eye implies the ipsilateral anterior canal
Applied Vestibular Anatomy
108
Back to our Case
• Why the Down Beating Nystagmus on Dix –Hallpike?
©2012 MFMER | slide-109
Back to our Case
• Right Anterior Canal BPPV
©2012 MFMER | slide-110
Detecting Anterior Canal BPPV
Side Lying Maneuver with the Nose Down
AC-BPPV
• Try a reverse Epley Maneuver• Example is for left anterior canal...
Applied Vestibular Anatomy
112

2/3/2016
18
Epley Omniax® System
©2012 MFMER | slide-113
Down Beating Positional Nystagmus
• Central:• Enhances with hyperventilation • Enhances with lateral eye position• Seldom with torsional Component• Rare
• Anterior Canal• Torsional component variably present with
eye position• More common
©2012 MFMER | slide-114
Canalithiasis Treatments (Bed Side):
• Posterior Canal
• Horizontal Canal
• Anterior Canal
• Epley
• Barrel roll
• Reversed Epley
• Deep Head tilt
From: Baloh, R. W. (1998) “Dizzy Patients: The Varieties of Vertigo”in: Hospital Practice, http://www.hosppract.com/issues/1998/06/dmmbal.htm
Epley Omniax® System
©2012 MFMER | slide-116
Treatment Outcome
• Down beating nystagmus diminished with EpleyChair Treatment.
• Patient not so unsteady when first getting up in the morning.
• Still unsteady on feet
©2012 MFMER | slide-117
Fig. 9 Simplified schematic diagram of some of the possible pathways underlying the cVEMP and oVEMP responses and the patternof the asymmetry of n10 and p13 after complete and partial unilateral vestibular loss. It is consistent with the evidence from <ce...
Ian S. Curthoys
A critical review of the neurophysiological evidence underlying clinical vestibular testing using sound, vibration and galvanic stimuli
Clinical Neurophysiology, Volume 121, Issue 2, 2010, 132 - 144
http://dx.doi.org/10.1016/j.clinph.2009.09.027

2/3/2016
19
VEMP Response Absence by Age
cVEMP
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100
Prob
ablit
y of
an
Abse
nt R
espo
nse
Age (Yrs)
FEMALE MALE
oVEMP
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100
Prob
ablit
y of
an
Abse
nt R
espo
nse
Age (Yrs)
FEMALE MALE
oVEMP and BPPV Age of Onset
oVEMP BPPV
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100
Prob
ablit
y of
an
Abse
nt R
espo
nse
Age (Yrs)
FEMALE MALE
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100
Prob
ablit
y of
BPP
V
Age (Yrs)
MALE FEMALE