osteopathic medicine the hip - osteopedia.iao.beosteopedia.iao.be/uploads/heup_en_demo.pdf · 8 2....
TRANSCRIPT
Osteopathic Medicine
The Hip
Luc Peeters & Grégoire Lason
2
The Hip
Luc Peeters & Grégoire Lason All rights reserved. Osteo 2000 bvba © 2013. No part of this e-book may be reproduced or made
public by printing, photocopying, microfilming, or by any means without the prior written permission of the publisher.
Contact: Osteo 2000, Kleindokkaai 3-5, B – 9000 Ghent, Belgium
Mail: [email protected]
Web: http://osteopedia.iao.be and www.osteopathie.eu
Tel: +32 9 233 04 03 - Fax: +32 55 70 00 74
ISBN: 9789074400442
The International Academy of Osteopathy – I.A.O.
3
Content
1. Introduction ............................................................................................................ 7
2. Biomechanics ........................................................................................................ 8 2.1. General ............................................................................................................. 8 2.2. Mobility ............................................................................................................. 8
2.2.1. Range of Motion ......................................................................................... 8 2.2.2. Mobility Limiting Ligaments ...................................................................... 10 2.2.3. Muscles of the Hip .................................................................................... 13 2.2.4. The Hip in Gait .......................................................................................... 24
2.3. Stability .......................................................................................................... 24 2.3.1. Local Stability ........................................................................................... 24 2.3.2. Pelvic Stability .......................................................................................... 27 2.3.3. Core Stability ............................................................................................ 30
3. Hip Pain ................................................................................................................ 35 3.1. Sensory Innervation ...................................................................................... 35
3.1.1. Hip Capsule .............................................................................................. 35 3.1.2. Area Nervina ............................................................................................. 36
3.2. Inflammatory .................................................................................................. 37 3.2.1. Bursitis ...................................................................................................... 37 3.2.2. Iliopsoas Tendinitis ................................................................................... 40 3.2.3 Transient Synovitis .................................................................................... 41
3.3. Degenerative .................................................................................................. 42 3.3.1. Osteoarthrosis .......................................................................................... 42 3.3.2. Labral Tear ............................................................................................... 45
3.4. Rheumatic ...................................................................................................... 46 3.4.1. Rheumatoid Arthritis - RA ......................................................................... 46
3.5. Femoro-acetabular Impingement ................................................................ 48 3.6. Infectious ....................................................................................................... 49
3.6.1. Septic Arthritis .......................................................................................... 49 3.7. Snapping Hip Syndrome ............................................................................. 50 3.8. Deformations ................................................................................................. 50
3.8.1. Hip Dysplasia ............................................................................................ 50 3.8.2. Slipped Capital Femoral Epiphysis Syndrome (SCFE) ............................ 52 3.8.3. Legg-Calve-Perthes Disease .................................................................... 53 3.8.4. Avascular Necrosis - AVN ........................................................................ 55
3.9. Traumatic ....................................................................................................... 56 3.9.1. Hip Pointer ................................................................................................ 56 3.9.2. Avulsion Fracture ...................................................................................... 57 3.9.3. Stress Fractures ....................................................................................... 57
3.10. Piriformis Syndrome ................................................................................... 58
4
4. Lesions - Dysfunctions ....................................................................................... 61 4.1. Case History .................................................................................................. 61 4.2. Observation ................................................................................................... 62
4.2.1. General ..................................................................................................... 62 4.2.2. Observation of the Shortened Structures ................................................. 62 4.2.3. Observation of the Body Load .................................................................. 65 4.2.4. Observation of the Dominant Plane of the Failing Posture ....................... 66 4.2.5. Observation for Antalgic Position ............................................................. 67 4.2.6. Observation for Capsular Pattern ............................................................. 67 4.2.7. Observation of Gait ................................................................................... 67
4.3. Provoking and Testing Palpation ................................................................ 68 4.3.1. Clinical Examination of New-borns and Infants ........................................ 68 4.3.2. Palpation ................................................................................................... 70
4.4. Provocation Tests ......................................................................................... 70 4.4.1. Provocative Palpation of the Anterior Hip Capsule ................................... 70 4.4.2. Provocative Compression in the Hip Joint ................................................ 71 4.4.3. Provocative Compression in the Hip Joint – Side lying ............................ 72 4.4.4. Provocative Compression in the Hip Joint – Supine ................................. 72 4.4.5. Traction Test ............................................................................................. 73 4.4.6. Traction Test ............................................................................................. 73 4.4.7. Provocation Test of the Ventral Capsule .................................................. 74 4.4.8. Capsular Provocation ............................................................................... 74 4.4.9. Differentiation Test Hip – Sacroiliac Joint ................................................. 75 4.4.10. Differentiation Test Hip – Sacroiliac Joint (Fabere Test) ........................ 75 4.4.11. Sign of the Buttock ................................................................................. 76
4.5. Mobility Tests ................................................................................................ 76 4.5.1. Flexion Test .............................................................................................. 76 4.5.2. Extension Test .......................................................................................... 77 4.5.3. Abduction Test .......................................................................................... 77 4.5.4. Adduction Test .......................................................................................... 78 4.5.5. Internal Rotation Test ............................................................................... 78 4.5.6. External Rotation Test .............................................................................. 79 4.5.7. Elasticity Test of the medial Capsule ........................................................ 79
5. Techniques ........................................................................................................... 81 5.1. Mobilizations ................................................................................................. 81
5.1.1. General ..................................................................................................... 81 5.1.2. Mobilization of an Adduction Lesion ......................................................... 82 5.1.3. Mobilization of an Adduction Lesion ......................................................... 83 5.1.4. Mobilization of an Abduction Lesion ......................................................... 83 5.1.5. Mobilization of an Abduction Lesion ......................................................... 84 5.1.6. Mobilization of a Lesion in internal Rotation ............................................. 84 5.1.7. Mobilization of a Lesion in external Rotation ............................................ 85 5.1.8. Mobilization of a Lesion in Flexion ............................................................ 85

5
5.1.9. General capsular Stretch .......................................................................... 86 5.1.10. General capsular Stretch ........................................................................ 86
5.2. Muscle Energy Techniques - MET ............................................................... 87 5.2.1. General ..................................................................................................... 87 5.2.2. Massage on the Psoas ............................................................................. 88 5.2.3. MET on the Psoas .................................................................................... 89 5.2.4. MET on the Psoas .................................................................................... 90 5.2.5. Fascial Stretch of the Psoas ..................................................................... 91 5.2.6. Massage on the Iliacus ............................................................................. 92 5.2.7. MET on the Iliacus .................................................................................... 93 5.2.8. Fascial Stretch on the Iliacus .................................................................... 94 5.2.9. MET of the Rectus Femoris ...................................................................... 95 5.2.10. MET of the Hamstrings ........................................................................... 95 5.2.11. MET of the Hamstrings ........................................................................... 96 5.2.12. MET of the Gluteus Maximus ................................................................. 96 5.2.13. MET of the Abductors ............................................................................. 97 5.2.14. MET of the Abductors ............................................................................. 97 5.2.15. MET of the Adductors ............................................................................. 98 5.2.16. MET of the Adductors ............................................................................. 99 5.2.17. Massage of the Piriformis ....................................................................... 99 5.2.18. MET of the external Rotators ................................................................ 100 5.2.19. MET of the external Rotators ................................................................ 101 5.2.20. MET of the internal Rotators ................................................................. 102 5.2.21. MET of the internal Rotators ................................................................. 102
5.3. ‘Strain and Counterstrain Techniques - SCT’ ........................................... 103 5.3.1. General ................................................................................................... 103 5.3.2. Spasm of the Piriformis .......................................................................... 103 5.3.3. Spasm of the Iliacus ............................................................................... 104 5.3.4. Lesion in Extension ................................................................................ 104 5.3.5. Lesion in Abduction ................................................................................ 105 5.3.6. Lesion in Flexion ..................................................................................... 105 5.3.7. Lesion in Flexion ..................................................................................... 106 5.3.8. Spasm of the Adductors ......................................................................... 106 5.3.9. Inguinal Ligament ................................................................................... 107
6. Bibliography ....................................................................................................... 108
7. About the Authors ............................................................................................. 113
8. Acknowledgment ............................................................................................... 114
9. Osteopathic Terminology ................................................................................. 115 9.1. The Three Anatomical Axes ....................................................................... 115 9.2. The Three Anatomical Planes .................................................................... 116 9.3. Spinal Biomechanics .................................................................................. 117 9.4. General Abbreviations ................................................................................ 119

6
9.5. Specific Terms ............................................................................................. 120
10. All Video’s ........................................................................................................ 121
7
1. Introduction The hip joint is the articulation between the femur and the acetabulum of the pelvis and its primary function is to support the weight of the body in both static (e.g. standing) and dynamic (e.g. walking or running) postures.
The hip is a true ball-and-socket synovial and multiaxial joint surrounded by powerful muscles, enabling a wide range of motion in several planes while also exhibiting remarkable stability.
As the structural link between the lower extremities and the axial skeleton, the hips not only transmit forces from the ground up but also carry forces from the trunk, head and neck, and upper extremities. Consequently this joint is crucial to sport activities in which it is often exposed to many greater than normal axial and torsional forces.
This important joint needs therefore stability to withstand body load on the one hand and mobility to make us mobile and to eventually compensate dysfunctions in the low back and pelvic joints.
For those who are not familiar with the typical osteopathic terminology, we refer to chapter 9 at the end of this e-book.
8
2. Biomechanics (Bergman et al 2001, Byrne et al 2010, Denham 1959, Greenwald 1991, Johnston et al 1998, Moore 1992, Paul 1966)
2.1. General The hip joint has two major functions:
• Mobility: providing a good range of motions in the three planes in order to be able to move, walk, run and in order to eventually compensate for loss of mobility in other surrounding joints due to lesions or aging.
• Stability: providing a good equilibrium and spread of gravity forces when we stand in order to not overcharge different joints and soft tissues such as ligaments and muscles.
2.2. Mobility
2.2.1. Range of Motion
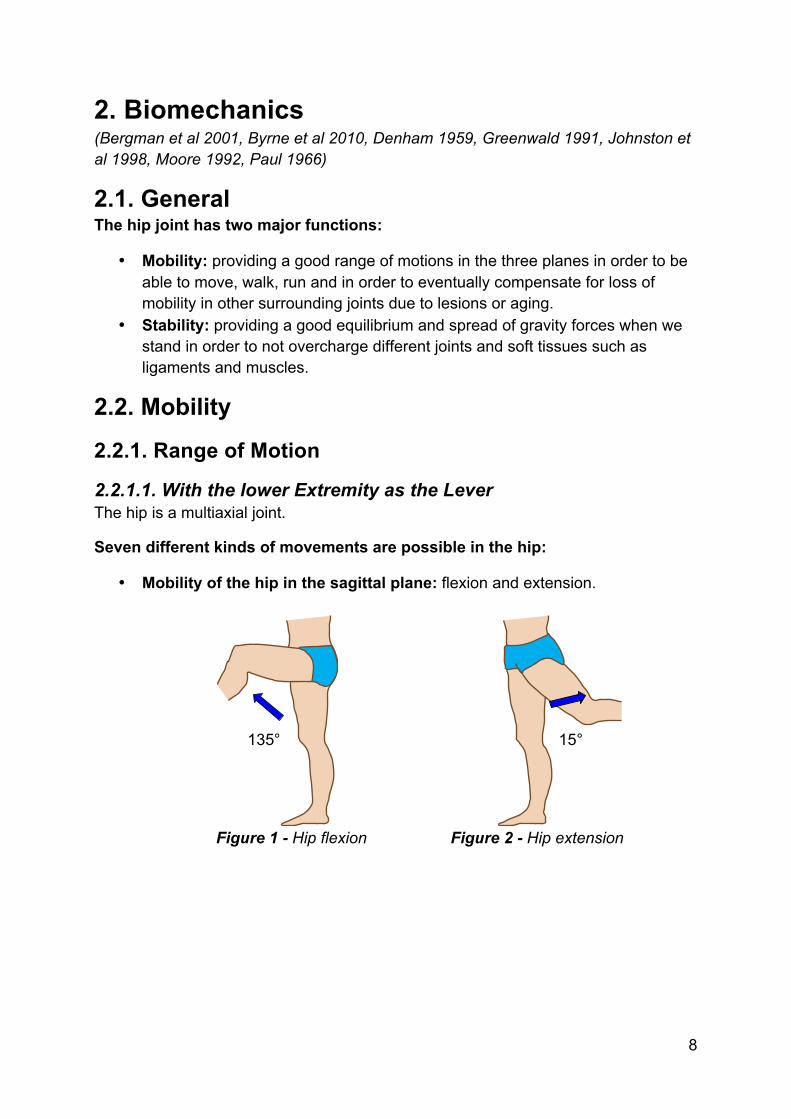
2.2.1.1. With the lower Extremity as the Lever The hip is a multiaxial joint.
Seven different kinds of movements are possible in the hip:
• Mobility of the hip in the sagittal plane: flexion and extension.
Figure 1 - Hip flexion Figure 2 - Hip extension
135° 15°

9
• Mobility of the hip in the frontal plane: abduction and adduction.
Figure 3 - Hip abduction Figure 4 - Hip adduction
• Mobility of the hip in the horizontal plane: external and internal rotation.
Figure 5 - Hip external rotation Figure 6 - Hip internal rotation
• Combination: circumduction.
45°
25° 45°
35°

10
2.2.1.2. With the Pelvis and the Spine as the Lever These hip movements are with the patient standing, the feet on the ground.
Pelvis Spine Hip joints Forward tilt Hyperextension Slight flexion Backward tilt Slight flexion Strong extension Shift left Sidebending right Right hip: abduction
Left hip: adduction Shift right Sidebending left Right hip: adduction
Left hip: abduction Rotation right Rotation left Right hip: internal rotation
Left hip: external rotation Rotation left Rotation right Right hip: external rotation
Left hip: internal rotation
2.2.2. Mobility Limiting Ligaments Iliofemoral ligaments (also called ligaments of Bigelow): they are the strongest ligaments in the body.
The iliofemoral ligament can be seen anterior to the hip in the form of an inverted Y. It spans, in a spiralling fashion, from its proximal attachment to the ilium to insert along the intertrochanteric line.
It is taut in extension and relaxed in flexion keeping the pelvis from tilting posteriorly in upright stance and limiting adduction of the extended lower limb.
It is the strongest ligament in the body with a tensile strength greater than 350N.
Pubofemoral ligament: lies inferior to hip joint and helps thicken the capsule. The pubofemoral ligament contributes to the strength of the anteroinferior portion of the capsule. It is a weaker ligament.
Ischiofemoral ligament: lies posterior to the hip joint, consist of a triangular band of strong fibres, helps thicken the capsule. The ischiofemoral ligament completes the main ligamentous constraints – from it ischial attachment medially it inserts laterally on the superolateral aspect of the femoral neck, medial to the base of the greater trochanter.
Zona orbicularis ligament: lies at the lower and back side of the capsule, forms a circular collar around the neck of the femur.
Transverse ligament of acetabulum: crosses the acetabular notch, fills in the gap of the inferior border of the acetabulum.
Ligament of femoral head: lies along the transverse acetabular ligament, attaches

11
to a small pit in the centre of the femoral head & acts when the hip is flexed and the thigh is externally rotated. The ligament of the femoral head (also called teres ligament) contributes little in the way of stability to the hip and can be torn in traumatic dislocations. It plays a role in joint nutrition. Its potential for degeneration is better appreciated with the increasing utilization of hip arthroscopy.
Figure 7 - Ligaments of the hip – anterior view
Figure 8 - Ligaments of the hip – posterior view
Iliofemoral lig.
Pubofemoral lig.
Iliac bone
Femur
Iliofemoral lig.
Ischiofemoral lig.
Zona orbicularis
Greater trochanter
Ilium
Femur
Lesser trochanter
Intertrochanteric crest

35
3. Hip Pain (Bethesda 2008, Birnbaum et al 1997, Campbell et al 2001, Dee 1969, Cotran 1999, Dabou 2007, Dee et al 1997, Eberhardt et al 1995, Ferguson et al 2003, Hoppenfeld 1980, Kim 1987, Kennedy et al 2009, Kumar & Clark 2002, McCarthy et al 2001, Nasser & Ewan 2001, Philippon et al 2007, Robinson et al 2003, Rossi & Metelli 2006, Salvi & Metelli 2006)
3.1. Sensory Innervation
3.1.1. Hip Capsule The anterior and posterior hip capsule is innervated differently.
The anteromedial innervation is from the articular branches of the obturator nerve.
The sensory articular branches of the femoral nerve innervate the anterior hip capsule.
The posterior capsule is innervated by the sciatic nerve, which in addition to the articular branches of the nerves to the quadratus femoris muscle innervates the posteromedial section of the hip joint capsule.
Moreover, articular branches of the superior gluteal nerve were found, which innervate the posterolateral section of the hip joint capsule.

36
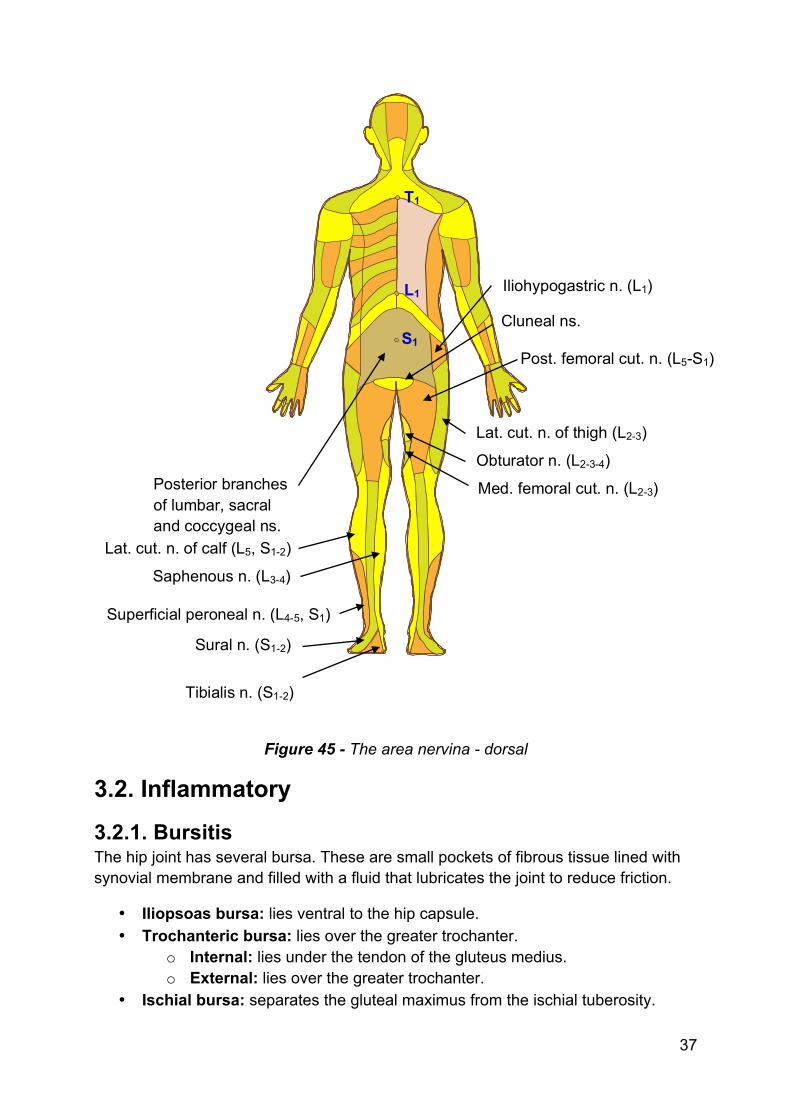
3.1.2. Area Nervina Area nervina are the skin areas innervated by the sensory branches of the peripheral nerves.
Figure 44 - The area nervina - ventral
Iliohypogastric n. (L1) Genitofemoral n. (L1-2)
Ilioinguinal n. (L1) Dorsal n. of penis (L1)
Lat. cut. n. of thigh (L2-3) Obturator n. (L2-3-4)
Med. femoral cut. n. (L2-3)
Lat. cut. n. of calf (L5, S1-2)
Saphenous n. (L3-4)
Superficial peroneal n. (L4-5, S1) Deep peroneal n. (L4-5)
Sural n. (S1-2)
Medial plantar n.
37
Figure 45 - The area nervina - dorsal
3.2. Inflammatory
3.2.1. Bursitis The hip joint has several bursa. These are small pockets of fibrous tissue lined with synovial membrane and filled with a fluid that lubricates the joint to reduce friction.
• Iliopsoas bursa: lies ventral to the hip capsule. • Trochanteric bursa: lies over the greater trochanter.
o Internal: lies under the tendon of the gluteus medius. o External: lies over the greater trochanter.
• Ischial bursa: separates the gluteal maximus from the ischial tuberosity.
T1
L1
S1
Iliohypogastric n. (L1)
Cluneal ns.
Posterior branches of lumbar, sacral and coccygeal ns.
Lat. cut. n. of thigh (L2-3)
Obturator n. (L2-3-4)
Med. femoral cut. n. (L2-3)
Post. femoral cut. n. (L5-S1)
Lat. cut. n. of calf (L5, S1-2)
Saphenous n. (L3-4)
Superficial peroneal n. (L4-5, S1)
Sural n. (S1-2)
Tibialis n. (S1-2)

61
4. Lesions - Dysfunctions (Peeters & Lason 2005) Lesion means that there is a loss of mobility. Dysfunction of the hip joints can cause complaints. Dysfunctions can be hyper- as well as hypomobilities.
4.1. Case History In the case history, the osteopath tries to identify the nature of the pain:
• Aching pain can be from a ligament, especially when occurring in the morning with morning stiffness. Also when it occurs after a longer period of immobilization (sitting or standing). Ligament complaints are also often associated with osteoarthrosis. Transient morning pain that subsides after the patient has taken a few steps, but which reappears with exercise such as walking longer distances or climbing stairs (exercise pain), is typical of degenerative hip disorders.
• Sharp pain on specific movements can be caused by muscle strain or inflammation, tendinitis or bursitis.
• Fatigue can be caused by bad posture and poor muscular balance. It can also be associated with arteriosclerosis, rheumatoid arthritis or cancer.
• Radiating pain indicates a neurogenic factor and can be radicular or pseudo radicular.
• Numbness or muscle weakness indicates compression or damage of a nerve. • Vague, sometimes irradiating pain in the legs during exercise can indicate an
ischemic neuralgia. The differential diagnosis should consider neurogenic claudication (in the presence of stenosis of the spinal canal) and vascular claudication (in the presence of peripheral vascular disease). With neurogenic claudication, the patient feels no pain when beginning exercise, and bending forward in a sitting position lessens the pain. Generally, the pain radiates symmetrically into both the front and back of the thigh. With vascular claudication, the patient reports more rapid onset with exercise, and distal rather than proximal pain. This will be accompanied by alterations in perfusion, and occasionally by murmurs detectable by auscultation over the femoral arteries.
• Bilateral pain in the hips can be associated with lumbar canal stenosis or rheumatic disease.
• Unstable walking can be associated with osteoarthrosis (Trendelenburg) but also with central neurological problems such as cervical myelopathy.
• Are there visceral signs associated with the hip pain?
62
• Nocturnal pain often indicates cancer, inflammation/infection or rheumatic disease.
The type of patient (child, adult, elderly, pregnant, peri-menopausal woman) can give information to the osteopath.
The onset of hip pain is important. Was there a trauma? Was the onset sudden or progressively worsening?
Where there recent infections?
Is there symptom magnification and psychological distress? (superficial or non-anatomical pain distribution, non-anatomic sensory or motor disturbance, inconsistent neurological signs, inappropriate or excessive verbalization of the pain).
4.2. Observation
4.2.1. General The general observation tries to identify:
• Muscular contour (asymmetry). • Muscular atrophy. • Swelling and/or erythema. • Other deformities. • Observational comparison bilateral. • Where are the somatic dysfunctions (more details in the e-book ‘Integration
and Applied Principles in Osteopathy’ of the same authors). • Observation of other joints such as the feet (position and eventual
deformations).
4.2.2. Observation of the Shortened Structures The osteopath observes the position of the hip in space with the patient standing. It is important is that he or she observes the location of the shortened structures.
For example:
• When the osteopath observes a hip position standing in external rotation, the shortened structures are on the posterior side of the joint, the overstretched structures on the anterior side.
• When the osteopath observes a hip position standing in internal rotation, the shortened structures are on the anterior side of the joint, the overstretched structures on the posterior side.
• When the osteopath observes a unilateral hip position standing in abduction, the shortened structures are on the lateral side, the overstretched structures on the medial side.

63
• When the osteopath observes a unilateral hip position standing in adduction, the shortened structures are on the medial side and the overstretched structures on the lateral side.
• When the osteopath observes one hip in abduction and one hip in adduction, the cause of the problem lies mostly in the lower lumbar spine in a shift lesion. The pelvis will then be positioned in a shift status.
Figure 72 - Pelvic shift to the left
The aim of this observation (of the shortened structures) is to see where locally can be treated. Local treatment can only be done on the shortened side (mobilization of manipulation).
The complaints of the patient can be on the shortened side as well as the overstretched side.
Hip in adduction
Hip in abduction
64
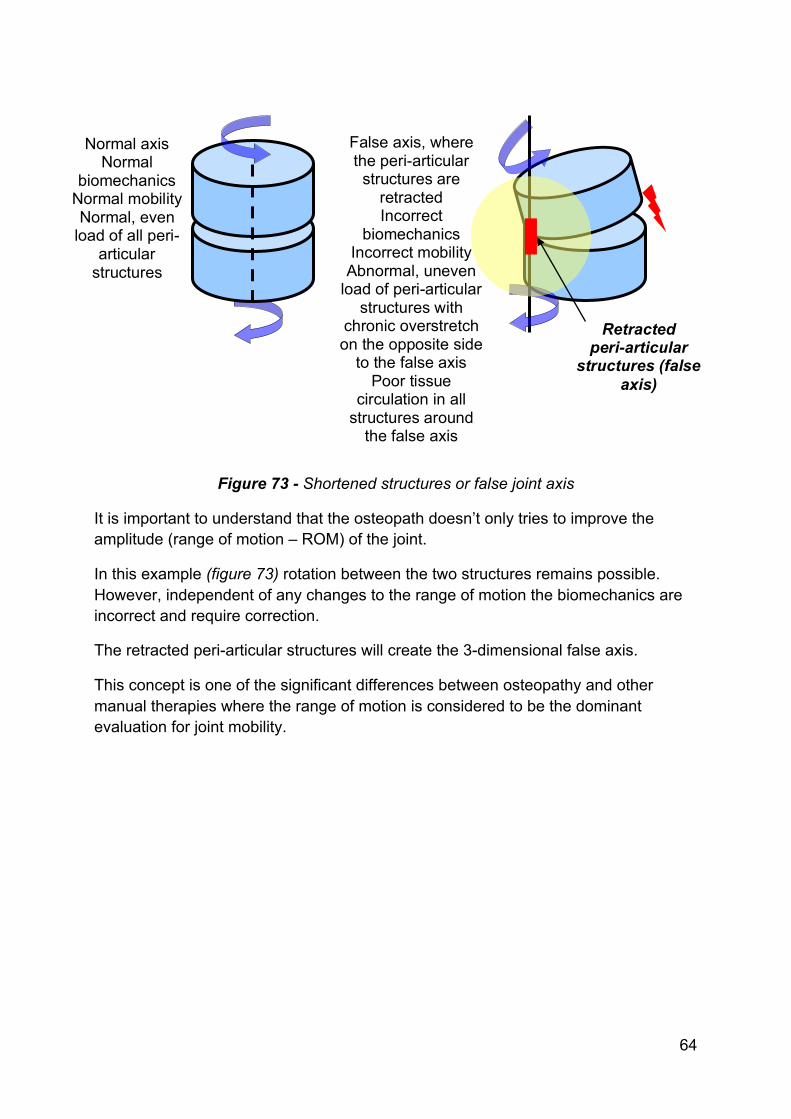
Figure 73 - Shortened structures or false joint axis
It is important to understand that the osteopath doesn’t only tries to improve the amplitude (range of motion – ROM) of the joint.
In this example (figure 73) rotation between the two structures remains possible. However, independent of any changes to the range of motion the biomechanics are incorrect and require correction.
The retracted peri-articular structures will create the 3-dimensional false axis.
This concept is one of the significant differences between osteopathy and other manual therapies where the range of motion is considered to be the dominant evaluation for joint mobility.
Normal axis Normal
biomechanics Normal mobility Normal, even
load of all peri-articular structures
False axis, where the peri-articular
structures are retracted Incorrect
biomechanics Incorrect mobility
Abnormal, uneven load of peri-articular
structures with chronic overstretch on the opposite side
to the false axis Poor tissue
circulation in all structures around
the false axis
Retracted peri-articular
structures (false axis)

65
4.2.3. Observation of the Body Load This observation is done with the patient standing and in the sagittal plane.
Figure 74 - Observation in the sagittal plane
Important in this observation is to see whether the central gravity line falls between the sacroiliac joint and the acetabula. Only then the pelvis and hips are stable in a sagittal plane.
Normal type The normal
central gravity line.
From external auditory
meatus to talo-navicular
joint.
Posterior type The central
gravity line falls too far posterior.
Anterior type The central gravity line falls
too far anterior.
66
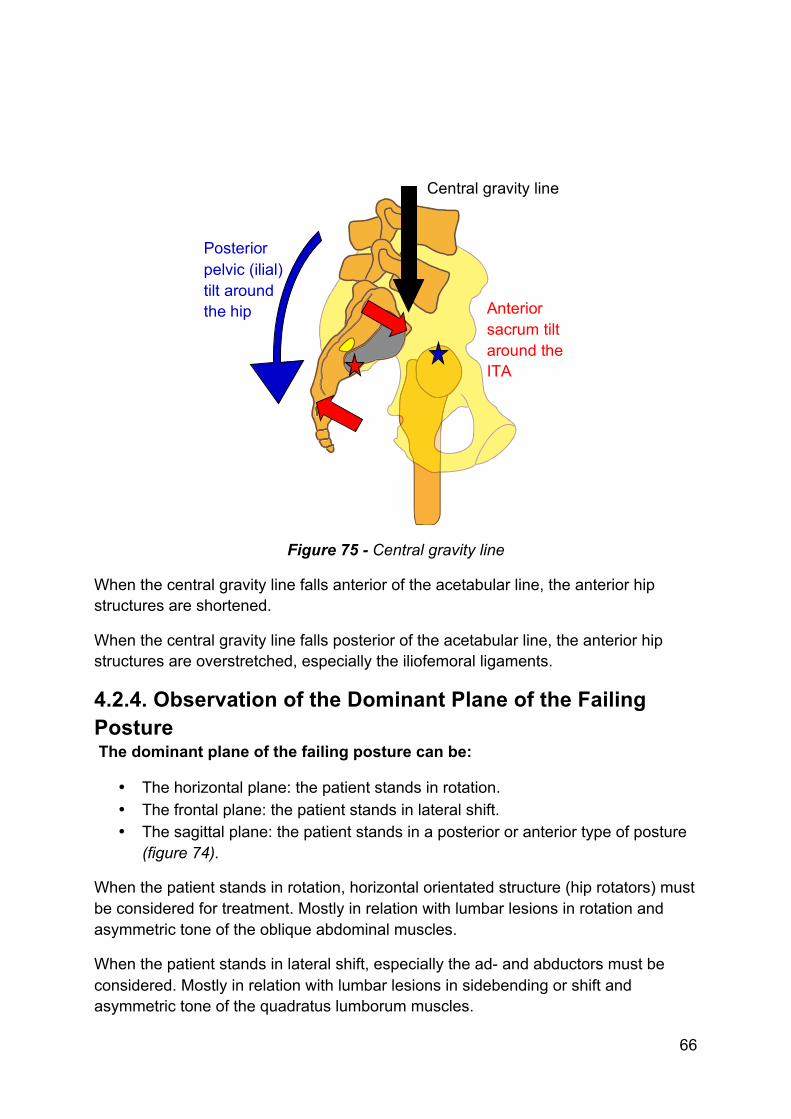
Figure 75 - Central gravity line
When the central gravity line falls anterior of the acetabular line, the anterior hip structures are shortened.
When the central gravity line falls posterior of the acetabular line, the anterior hip structures are overstretched, especially the iliofemoral ligaments.
4.2.4. Observation of the Dominant Plane of the Failing Posture The dominant plane of the failing posture can be:
• The horizontal plane: the patient stands in rotation. • The frontal plane: the patient stands in lateral shift. • The sagittal plane: the patient stands in a posterior or anterior type of posture
(figure 74).
When the patient stands in rotation, horizontal orientated structure (hip rotators) must be considered for treatment. Mostly in relation with lumbar lesions in rotation and asymmetric tone of the oblique abdominal muscles.
When the patient stands in lateral shift, especially the ad- and abductors must be considered. Mostly in relation with lumbar lesions in sidebending or shift and asymmetric tone of the quadratus lumborum muscles.
Posterior pelvic (ilial) tilt around the hip
Central gravity line
Anterior sacrum tilt around the ITA

81
5. Techniques 5.1. Mobilizations (Kutchera 1996, 2001, Maitland 2001, Peeters & Lason 2005)
5.1.1. General The aim of a mobilization is:
• Correction of the false axis in the joint by stretching retractions in the capsule and surrounding ligaments. This is done with enough specificity so that it is appropriate even in a joint that is hypermobile in other directions. In this way the biomechanical quality of the joint can be repaired and the overstretched soft tissues can be relaxed.
• Via rhythmical mobilizations and use of long lever techniques a drainage (improved circulation) of all soft tissues around the joint will occur. Near to the false axis (shortened structures) congestion of all tissue will still occur.
• The mobilization is done in a pain free and rhythmical manner. The aim is to normalize any hyperactivity of the sympathetic system in the surrounding tissues. Pain will increase this sympathetic activity further.
• Via rhythmical compression/traction the synovial production is stimulated which is a desirable reaction when treating arthrotic joints. This is also the reason why mobilizations of an arthritic joint are not suggested.
• Range of motion increase is not necessarily the primary aim of mobilization. It can even be relatively contra-indicated so as not to cause instability (especially of concern in arthritic joints).
The mobilization must be pain free so as to avoid increasing sympathetic activity further, which is contrary to the treatment goal. The mobilization must occur at the end of range so that a light tension is maintained in the tissues being treated. The mobilization is rhythmical and with circumduction where possible. If the aim is to stimulate synovial production, a light push/pull (compression/traction) technique is indicated. The mobilization is always done in the direction of the false axis (shortened structures) and according to the normal biomechanics of the joint. Hypermobile directions are avoided.

82
Contra indications • Inflammation or infection. • A joint with intra-articular swelling. Mobilization will only increase and worsen
the swelling. • Painful end of range. • In the direction of a structurally damaged capsule. • Directly following recent trauma.
5.1.2. Mobilization of an Adduction Lesion The patient is lying on the side.
The osteopath takes the leg of the patient as the lever of the technique and places his hand on the superolateral side of the greater trochanter.
He keeps the leg of the patient in the frontal plane of the patient.
With the lever, he takes up the slack and mobilizes with the external hand towards the retracted medial capsule.
A slight circumduction is performed.
The technique is done without causing pain.
Video 21 - Mobilization of an adduction lesion
83
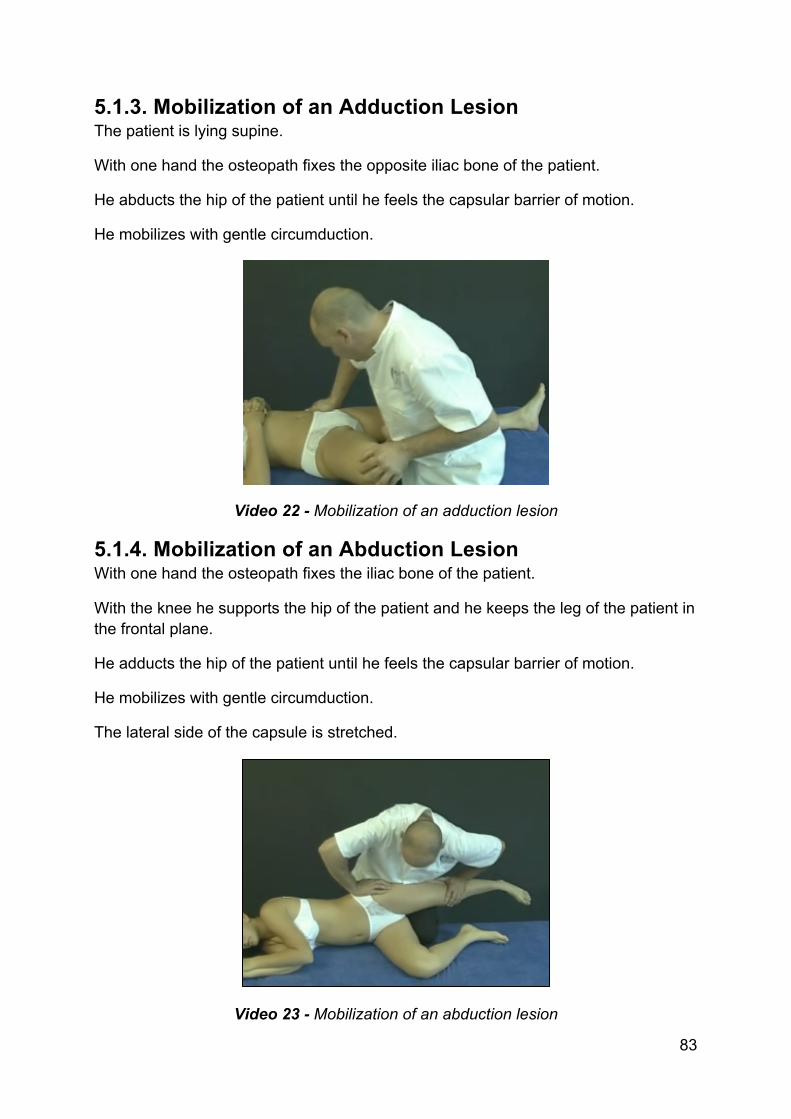
5.1.3. Mobilization of an Adduction Lesion The patient is lying supine.
With one hand the osteopath fixes the opposite iliac bone of the patient.
He abducts the hip of the patient until he feels the capsular barrier of motion.
He mobilizes with gentle circumduction.
Video 22 - Mobilization of an adduction lesion
5.1.4. Mobilization of an Abduction Lesion With one hand the osteopath fixes the iliac bone of the patient.
With the knee he supports the hip of the patient and he keeps the leg of the patient in the frontal plane.
He adducts the hip of the patient until he feels the capsular barrier of motion.
He mobilizes with gentle circumduction.
The lateral side of the capsule is stretched.
Video 23 - Mobilization of an abduction lesion

113
7. About the Authors
Grégoire Lason Luc Peeters Gent (B), 21.11.54 Terhagen (B), 18.07.55
Both authors are holders of university degrees, namely the Master of Science in Osteopathy (MSc.Ost. – University of Applied Sciences), and are very active with the promotion and academic structuring of osteopathy in Europe. In 1987 they began The International Academy of Osteopathy (IAO) and are, to this day, the joint-principals of this academy. The IAO is since several years the largest teaching institute for osteopathy in Europe. Both osteopaths are members of diverse professional organizations, including the American Academy of Osteopathy (AAO), the International Osteopathic Alliance (IOA) and the World Osteopathic Health Organization (WOHO), as part of their mission to improve osteopathic development. This osteopathic encyclopaedia aims to demonstrate the concept that a proper osteopathic examination and treatment is based upon the integration of three systems: the musculoskeletal, visceral and craniosacral systems.

123
This e-book is a product of Osteo 2000 bvba.
If you are interested in publishing an e-book or if you have questions or suggestions, please contact us:
Mail: [email protected]
Fax: +32 55 70 00 74
Tel: +32 9 233 04 03
Web Osteopedia: http://osteopedia.iao.be
Web The International Academy of Osteopathy – IAO: http://www.osteopathie.eu