osteomyelitis of the mandible this statement isdifficult to
TRANSCRIPT
OSTEOMYELITIS OF THE MANDIBLEBased on a lecture delivered at the Royal College of Surgeons of England
on19th February, 1948
by
S. H. Wass, M.S., F.R.C.S.Assistant Surgeon to Guy's Hospital
THE COMMONEST CAUSE of osteomyelitis of the mandible is dental infection,an extension of apical or peri-apical disease resulting in spreading in-flammation of bone. Osteomyelitis also follows infected fractures of themandible and occasionally complicates infected cysts. It can occur froma blood-stream infection, particularly in infants or young children, andrarely from metastatic invasion of the mandible in a patient sufferingfrom acute osteomyelitis of another bone. Cases of osteomyelitis of themandible arising by direct extension from a staphylococcal boil on thechin have also been recorded. Dental infection, however, is by far themost important cause and my further remarks will be confined to thistype of the disease.
OSTEOMYELITIS OF DENTAL ORIGINThere has been a great increase in the incidence of osteomyelitis of dental
origin since the early years of the war. Statistical evidence in support ofthis statement is difficult to obtain but the following figures illustrate myown experience with the disease. In the 10-year period 1933-1942,51 patients were admitted to the wards of Guy's Hospital suffering fromosteomyelitis of the mandible. This is an average of 5-1 patients per yearunder the care of all the surgeons and dental surgeons together, lessthan one per year for each surgeon. In the succeeding five years, 1943-1947, I treated 57 patients myself, an average of 11-4 patients per yearfor a single surgeon; and in 51 of these 57 patients the osteomyelitiswas due to dental infection. In other words, 1 have had the opportunityof treating personaly more patients with osteomyelitis of the mandiblein the last five years than were treated by the whole staff of Guy's Hospitalduring the preceding 10 years. One cannot fail to be impressed by thesefigures and the experience of other surgeons confirms my belief in theabsolute increase in the incidence of dental osteomyelitis. It behoves us,therefore, to study the factors which cause the development of osteo-myelitis, ponder upon its increasing frequency, and consider what stepscan be taken to prevent it.
AEtiologyOsteomyelitis of dental origin almost invariably arises from apical or
peri-apical disease. Apical infection in relation to a live tooth causessymptoms which are easily recognised. If these symptoms are ignored,or do not become apparent because the tooth is dead, the apical infectionmay spread through the bone to produce a cellulitis of the soft tissues
48
OSTEOMYELITIS OF THE MANDIBLE
or an alveolar abscess. This is the commonest acute infection of the jawand must not be confused with osteomyelitis ; primary soft-tissue infectionis seldom followed by bony disease, even in neglected cases. In onlythree of my 51 patients has osteomyelitis followed a primary alveolarabscess. It is a mystery why such spreading infection so commonlyreaches the soft tissues without producing bony disease but it is a fortunatehappening, for otherwise osteomyelitis of the jaw would be the scourgeof humanity.
In some cases, however, spreading peri-apical infection does involve thebone of the jaw and osteomyelitis becomes established. Can we explainwhy this happens in only the minority of cases ? Bone is a tissue normallyresistant to the spread of apical disease; osteomyelitis will only developif the infecting organism is of a particular variety or virulence, or if thereis lowering of the general resistance of the patient or local resistance ofthe bone.The common organism causing osteomyelitis of the mandible is the
staphylococcus aureus, but in the jaw it is seldom highly virulent. Eventhe most severe cases of dental osteomyelitis are not complicated bysepticemia or pyxemia and do not show the degree of constitutionaldisturbance which is present in acute osteomyelitis of the long bones.It cannot be assumed, therefore that the development of osteomyelitisof the mandible is due to the virulence of the infecting organism alone;and the mere presence of the staphylococcus aureus in an apical areadoes not necessarily mean that bony disease will occur. The organismmay lie dormant, showing no tendency to invade the bone; and whenit does cause spreading inflammation a simple alveolar abscess resultsmore commonly than osteomyelitis.As in all infections, therefore, the onset of osteomyelitis must be deter-
mined by the outcome of the battle between the pathogenic organismsand the general and local resistance of the tissues of the host. Generalresistance to infection is a term impossible to define, depending as itdoes upon natural and acquired immunity and all the factors whichaffect such immunity. It is known that severe anmmia, and other blooddiseases such as leukemia, are associated with diminished resistance toinfection, particularly within the buccal cavity; but in my series of 51patients with dental osteomyelitis there has been no example of severeblood disease. Minor degrees of anemia, however, have been commonand they also may be associated with lowered resistance. Experiencein other fields has led me to believe that the war-time dietary has produceda diminished resistance to pyogenic infection. The increase in the numberof cases of osteomyelitis of the mandible has only been apparent sinceabout 1942 and I feel convinced that a state of subclinical under-nutrition,the result of prolonged restrictions of diet, is an important factor in accoun-ting for an otherwise inexplicable increase in the incidence of this disease.The factors affecting local resistance within the bone of thejaw are equally
difficult to study with scientific accuracy. Infection around a buried root
49
S. H. WASS
or dead tooth may be complicated by the development of a chronic formof osteomyelitis, even after a lapse of many years. On other occasions,however, buried roots or dead teeth cause no trouble; and osteomyelitis isknown to occur from infection of live teeth. It is unconvincing, therefore, toassert that buried roots or dead teeth act as so-called " irritants " whichdiminish local resistance to infection.Mowlem (1944) has pointed out that the mandible shows an anatomical
feature predisposing to the spread of infection and accounting for thefrequent occurence of osteomyelitis in the lower jaw compared with itsrelative rarity in the upper jaw. Apart from small arteries from theperiosteum, the mandible derives its entire blood supply from a singleartery running horizontally in a bony canal. The maxilla, on the otherhand, is supplied by a series of vertically disposed segmental arteries.It follows, therefore, that infection and inflammatory exudate in themandibular canal may cause thrombosis of the main artery, thus cuttingoff the entire blood supply of the bone and preventing the developmentof a defensive inflammatory reaction. In the maxilla, with its multiplearteries of supply, collateral circulation is free and resistance of the boneto spreading infection is not so hampered by vascular thrombosis. Theseanatomical features undoubtedly affect the relative incidence of osteo-myelitis in the upper and lower jaws, but they do not account for theincreased number of cases of osteomyelitis of the mandible in recentyears.
Before leaving the question of local resistance to infection the relationbetween dental extractions and the development of osteomyelitis must bediscussed. In my series of 51 cases of osteomyelitis of dental origin,two-thirds, or 34 cases, followed dental extraction. Of these 34 post-extraction cases, 18, or over 50 per cent., showed evidence that thedental treatment leading up to the development of the disease had beenof poor quality. Whilst good dentistry may be followed by osteomyelitis,bad dentistry, in my opinion, is an important factor in diminishinglocal resistance and increasing the likelihood of onset of the disease.The following typical history of a patient with osteomyelitis bears outthis contention. The patient complains of throbbing toothache, clearlyindicating the presence of an apical abscess, yet local submucous analgesiais employed. The extraction itself is unskilful and is accompanied bybreaking of crown or roots. The operator, under the same local analgesic,then causes further injury by using elevators to complete the extraction.Pain and swelling of the jaw follow this treatment and adjacent teeth areremoved in the mistaken belief that they are responsible for the symptoms.This story is no exaggeration, it occurs time and again. The danger oflocal analgesia in the presence of sepsis is well known. Traumaticextractions of the type described must tend to cause vascular thrombosisand lead to the spread of infection. Pain and swelling after extractionshould be a warning that osteomyelitis may have developed and in thepresence of bone infection further extractions, even of loose teeth, should
50
OSTEOMYELITIS OF THE MANDIBLE
not be performed until attention has been directed to the bony diseaseitself. Yet one or more of these basic principles was ignored in 18 of my34 patients with post-extraction osteomyelitis.
DIAGNOSISThere are two main clinical varieties of osteomyelitis of the mandible.
One can be called diffuse or spreading osteomyelitis, the other chroniclocalised osteomyelitis.
(1) Diffuse orspreading osteomyelitis is usually considered to be "acute,"but the use of this adjective is misleading. As already pointed out,osteomyelitis of the mandible, even in its most severe form, is notcomparable with acute osteomyelitis of a long bone. It is not complicatedby septicaemia or pyiffiia and is not accompanied by high fever orserious constitutional disturbance. It is a subacute disease with low feverand only a mild degree of toxemia.The majority of cases follow dental extraction. My series includes 33
examples of this subacute type and 25 of them followed extraction ofteeth. The remainder occurred without any extraction taking place orhad symptoms suggestive of osteomyelitis before dental treatment wasgiven. Most cases in which no extraction had been performed showedevidence of a dead tooth at the site of infection. The disease affects thetwo sexes equally and occurs at all ages, though rare in children. Myyoungest patient was 16 years of age, my oldest 60, and two-thirds ofthe patients belonged to the 20-40 age group.The symptoms cause attention to be sought early, but from three weeks
to two months is the common duration of symptoms before a diagnosisis made. Pain and swelling are constant features and trismus is presentif the disease affects the molar region or ascending ramus of the jaw.Pain may be severe and is of the constant boring type characteristic ofbony inflammation. Evidence of involvement of the inferior dental nerveis forthcoming when pain is referred to the ear or numbness occurs inthe mental region. The swelling is of two types. In some cases there isswelling of the bone with minimal cedema of the soft tissues. This swellingis due to periosteal thickening or the formation of subperiostealgranulation tissue or new bone, and is associated with tenderness in theaffected region of the jaw. In other cases bony swelling is masked bygross cedema of the soft tissues due to secondary cellulitis, and abscessformation may take place in neglected cases. This variety is difficult todistinguish from a simple alveolar abscess unless there is radiographicevidence of bone disease, and in my experience it carries a worse prognosisthan that in which the soft tissues remain relatively unaffected. Thereis often a purulent discharge into the mouth, through a tooth socket orsecondary sinus, and the occurrence of this discharge may be associatedwith disappearance of pain due to relief of tension within the bone.
Radiographic confirmation of the diagnosis is not forthcoming in theearly stages of the disease, an important point to remember. The first
51
S. H. WASS
radiographic sign is loss of bony detail, giving a mottled or moth-eatenappearance, often only appreciated when compared with normal radio-graphs taken at an earlier stage of the disease. The area of bonedestruction gradually becomes more extensive but even at relatively latestages sequestration may not be evident radiographically; small sequestraare frequently masked by the density of the cortical bone of the jaw.In some late cases, however, dense sequestra are visible and a pathologicalfracture may be seen. The earliest radiographic evidence of bonedestruction seldom appears until bone infection has been in progressfor three weeks. A clinical diagnosis of osteomyelitis may be possibleearlier than this when bony swelling is present, but when soft tissueswelling predominates it is difficult, if not impossible, to distinguishbetween osteomyelitis and alveolar abscess in the first three weeks. Ifincision of a soft tissue abscess is followed by disappearance of allsymptoms and signs, osteomyelitis is not present. Some alveolar abscesses,however, pursue a relatively chronic course and suppuration is slow totake place; in such cases it is only if good radiographs show no bonydisease after swelling has been present for three or four weeks that it canbe certain osteomyelitis will not develop. In these cases difficulty may alsoarise from the radiographic appearance of a small flake of alveolar boneat the site of an extraction. This flake of bone is frequently mistaken fora sequestrum but in fact it is traumatic in origin; a sequestrum is neverevident radiographically in three weeks and such an appearance in theearly stages of swelling of the jaw is not evidence of osteomyelitis.
(2) Chronic localised osteomyelitis of the mandible differs markedlyfrom the diffuse or spreading type of the disease. The onset of chronicosteomyelitis is insidious, the symptoms are not so severe and a periodof many months may elapse before the patient seeks advice. Dentalextraction precedes the onset of symptoms in only 50 per cent. of thesecases. In other cases the patient may have been edentulous for as longas 35 years, yet even in these circumstances the infection may commencearound a buried root.
Chronic osteomyelitis also affects the two sexes equally, but occurs inpatients of an older average age than those affected by the subacute type.In my own cases no patient was below 40 and the majority were over50 years of age. Pain and swelling of the jaw are again the main symptoms.The pain, however, is not usually severe, does not radiate to the ear andnumbness in the mental region is seldom noticed. The swelling is morelocalised and usually of the bony type with local tenderness. Some softtissue induration may be present and an external sinus develop, thus causingdifficulty in differentiating the disease from actinomycosis. Radiographs,however, will serve to distinguish these two conditions. The bone appearsnormal in actinomycosis, while in chronic osteomyelitis there is alwaysradiographic evidence of bony destruction by the time the patientpresents himself for treatment.
52

OSTEOMYELITIS OF THE MANDIBLE
The radiographic changes in chronic osteomyelitis of the mandible areextremely varied. The disease may affect the alveolar margin alone,usually with sequestrum formation. Less commonly the inferior marginof the jaw is involved. In other cases there is a localised area of bonedestruction in the mandible, in relation to a buried root and surroundedby an area of sclerosis, an appearance similar to that of Brodie's abscess.If the area of disease affects a narrow segment of the body of the mandiblepathological fracture may be present. Occasionally, a more diffuse areaof the jaw is involved and shows intermingling zones of rarefaction andsclerosis, with or without sequestration.
TREATMENT(a) Diffuse or spreading osteomyelitis. Before Mowlem (1944) advocated
radical surgery for this type of disease the age-long teaching had beenalmost exclusively in favour of expectant conservative treatment. Mostpatients were thus exposed to unnecessary and prolonged suffering,morbidity or total disability extending over many months or years,multiple minor surgical interventions to drain abscesses or removesequestra, and often an end-result of permanent disfigurement. Thisconservative treatment is dead and should never be resurrected.There is great danger, however, that it will be resurrected under cover
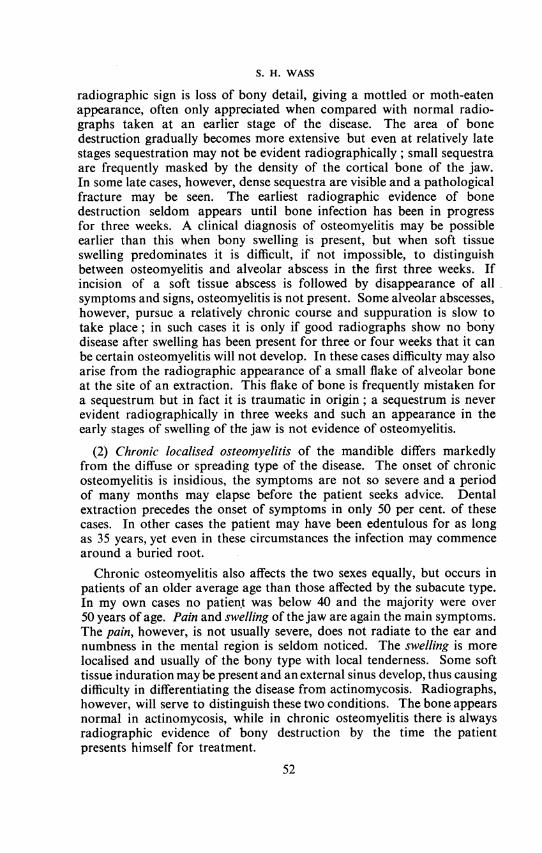
of that modern panacea, penicillin. Greer Walker (1947) prophesied that" the use of penicillin systemically without surgical interference will bethe method of choice in the future." This is a statement of grave import-ance, for in my experience systemic penicillin, without surgical interfer-ence, does not stay the relentless progress of the disease. On many occa-sions I have seen patients with subacute osteomyelitis of the mandiblegiven full doses of penicillin, and, although pain was sometimes relieved,bone destruction proceeded unchecked, the area of disease extended andeven pathological fracture occurred in some cases. The radiographs inFig. 1 illustrate the dangers of delay in operative treatment whilstpenicillin is being administered. This patient had subacute osteomyelitisfollowing extraction of the left lower first molar tooth. Two weeks afterthe extraction a correct diagnosis was made because of persistent pain inthe jaw, bony swelling and tenderness, and a discharge of pus from thesocket. A full course of systemic penicillin was begun and the lowerradiograph, taken at this time, shows minimal bone destruction. Theupper radiograph, taken after eleven days of penicillin therapy, showsextensive disease from the second molar to the first premolar region, apathological fracture has occurred, and a large portion of alveolar marginhas separated as a sequestrum. In spite of early diagnosis, early exhibitionof full doses of penicillin, relief of tension within the bone by free drainageof pus into the mouth, and an infection by a staphylococcus subsequentlyshown to be penicillin-sensitive, this gross extension of disease took place.
In my opinion Greer Walker has made the mistake of trying to comparesubacute osteomyelitis of the mandible with acute osteomyelitis of a long
53
S. H. WASS
Fig. 1. Radiographs of osteomyelitis of the mandible. Lower: Two weeks after onsetof infection, showing localised disease in the first molar region. Upper: Eleven dayslater, after full course of systemic penicillin, showing extension of disease with
sequestration.
bone, and these two conditions are not strictly comparable. In acuteosteomyelitis of a long bone penicillin undoubtedly rids the blood streamof infection and controls the systemic manifestations of the disease. Inthese respects it has proved a life-saving measure. In osteomyelitis of themandible there is no blood stream infection or serious systemic disturbanceand penicillin has no life-saving role to play. In osteomyelitis of a longbone penicillin will only, with certainty, produce resolution of the localdisease if given within 24 or 48 hours of the onset; given later in thedisease local infection may still progress and late operations of one typeor another will often be necessary; whilst if the penicillin is not givenuntil radiographic evidence of bone disease is present, surgery will almostalways be required.
In osteomyelitis of the mandible the same remarks are true. If penicillincould be given within 24 or 48 hours of the onset of swelling of the jawthere is no doubt that osteomyelitis could often be aborted, but thediagnosis of osteomyelitis of the jaw cannot be made at this early stage.
54

OSTEOMYELITIS OF THE MANDIBLE
When the diagnosis is considered in such cases and penicillin given withsuccess, I believe that many simple alveolar abscesses are aborted whilstcredit for curing osteomyelitis is claimed. It is, of course, ideal to recognizeacute and subacute swellings of the mandible within 24 or 48 hours andto give penicillin in full doses; nevertheless, in many cases the penicillinwill have been given unnecessarily and in others it may so mask thedeveloping physical signs as to delay the diagnosis and proper surgicaltreatment of spreading osteomyelitis. When penicillin is given later than48 hours after the onset of swelling of the jaw, and certainly when it isgiven after the appearance of radiographic evidence of bone disease, itwill seldom cure osteomyelitis of the mandible without accessory surgicalinterference. In these later stages of osteomyelitis vascular thrombosisis likely to have occurred; and as the mandible is supplied by a singleartery access of the drug, even to a sensitive organism, cannot be guaran-teed. If bone necrosis is present, although the organism is reached andinhibited by penicillin, sequestra themselves will keep up a suppurativeinflammation of bone and surgery will be required to eradicate the disease.
I believe, therefore, that the treatment of subacute osteomyelitis ofthe mandible should be by systemic penicillin combined with radicaloperation. The operation aims to remove all diseased bone andgranulation tissue and to relieve tension, thus preventing further spreadof the disease. I also believe that operation should be performed at theearliest opportunity, as soon as a definite diagnosis can be made. If thedisease is suspected but a definite diagnosis cannot be made, penicillinshould be given. The patient should then be kept under close clinicaland radiological observation and operation undertaken as soon as thepresence of bone necrosis is established. Only by these methods can theextent of the disease be kept within minimal limits and pathologicalfracture prevented with certainty. By waiting until gross bone destructionis present the operation itself may cause fracture of a jaw alreadyweakened by extensive disease. Although the majority of pathologicalfractures unite quickly after the eradication of infection, a minority failto unite altogether; and in any case a pathological fracture considerablyprolongs the period of treatment.
(b) Chronic osteomyelitis. In cases of chronic localised osteomyelitisof the mandible the subject of treatment is less controversial. On accountof the sclerosis of bone present in these cases it is generally agreed thatpenicillin will not gain access to the infected area and that surgicalinterference is required. If the disease is confined to the alveolar marginan intra-oral approach is used, but in most other cases, and in the vastmajority of cases of diffuse or spreading osteomyelitis, I am in favour ofan external approach on account of the better access it affords.
RESULTSTo substantiate my claims for the merits of operative treatment, the
following brief review of results is submitted. I have treated 51 cases of
55

S. H. WASS
dental osteomyelitis, 33 of the subacute spreading variety and 18 chroniclocalised infections. All the patients have been subjected to operativeinterference and all have shown definite radiological evidence of bonedisease. A few patients were seen when swelling of the jaw had beenpresent only for two or three weeks, but the majority had had symptomsfor six weeks or more. In the chronic cases the disease had been inprogress for'several months. Many of the patients in both groups hadreceived penicillin treatment before coming under my care and it hadfailed to prevent extension of the pathological process.Among the 33 patients with subacute osteomyelitis, 15 showed swelling
of the bony type with minimal involvement of the soft tissues. These15 patients all had good results, and the external wound healed by firstintention in every case. Twelve of the 15 were free from symptoms andfit for work two weeks after operation. One patient had a pathologicalfracture before operation and this healed in four weeks. The other twopatients had to undergo second operations because insufficient bone hadbeen removed in the first instance, and they were away from work 8weeks and 10 weeks respectively. The remaining 18 patients with subacuteosteomyelitis showed gross swelling of the soft tissues around thejaw, and in these cases the disability period was more prolonged. Intwo of the patients, treated before penicillin was available, the woundwas packed open and allowed to heal by granulation; in both casessecond operations were necessary to remove more diseased bone and thedisability period in each case was three months. In three patients softtissue abscesses were incised before the bone operation was performed;the wounds after the bone operation healed by first intention but swellingwas slow to subside and the disability period was 8 to 10 weeks. Inthree further patients pathological fracture was a complicating feature,present before operation in one case and produced at operationin two; two of these patients obtained rapid union and were fit for work ineight weeks, but the third fracture remained un-united and two subsequentbone grafts failed. Eight patients in this group showed primary unionof their wounds and all swelling had subsided in 4-6 weeks. Twopatients required three operations each for recurrent infection of the boneor soft tissues, one as long as three years after the original operation;these patients therefore suffered recurring periods of disability but bothhad advanced disease before presenting for initial treatment.Among the 18 patients with chronic localised osteomyelitis, 14 showed
rapid healing and were back at work in 2-4 weeks. One patient requireda second operation for residual soft tissue abscess and complete recoverywas delayed for six weeks. The remaining three patients had eachdeveloped a pathological fracture before operation; one of these fracturesunited after splinting for two months, the other two remained un-unitedafter three months' immobilisation. Fortunately, these un-united fractureswere in the anterior region of the jaw and deformity was minimal; bothpatients had so little trouble that they refused a grafting operation.
56

OSTEOMYELITIS OF THE MANDIBLE
SUMMARY OF RESULTS
(a) Subacute (diffuse or spreading) osteomyelitis-33 cases.(1) 15 cases with bony swelling only (minimal involvement of
soft tissues):12 primary union of wounds: all signs and symptoms
disappeared in 2 weeks.1-pathological fracture before operation : disability 4 weeks.2-second operations required: disability 8 and 10 weeks.
(2) 18 cases with gross involvement of soft tissues:8-primary union of wounds: all signs and symptoms
disappeared in 4-6 weeks.2-pathological fractures (1 before, 1 at operation):
disability 8 weeks.3-preliminary incision of soft tissue abscesses : healed in
8-10 weeks.2 before penicillin available: wounds packed open:
disability 12 weeks.1-pathological fracture occurred at operation: remains
un-united: continuing disability.2-three operations each for recurring infection: recurrent
periods of disability.
(b) Chronic localised osteomyelitis-18 cases.14-primary union of wounds: all signs and symptoms
disappeared in 2-4 weeks.1-second operation for residual soft tissue abscess
disability 6 weeks.1-pathological fracture before operation: healed in 8 weeks.2-pathological fractures before operation: remain un-united
but no disability beyond 12 weeks.These results are not perfect and it is hoped that greater experience
will lead to improvement in the future. It is my thesis, however, that insubacute osteomyelitis of the mandible, the results of surgery combinedwith penicillin are better than those of penicillin alone; that in the casesreviewed surgery has succeeded where penicillin has failed; and thatpenicillin alone will continue to fail unless the limitations of its usefulnessare recognised.
REFERENCESMOWLEM, R. (1944) Brit. Med. J. 1, 517.WALKER, D. G. (1947) Proc. Roy. Soc. Med. 40, 309.
57