osteoarthritis
TRANSCRIPT

V.Lokeesan, BSNT.Assistant lecturerFHCS,EUSL.

Osteoarthritis (OA)• OA is the most common form of
arthritis and the most common joint disease
• Known as degenerative joint disease or osteoarthrosis
• Most of the people who have OA are older than age 45, and women are more commonly affected than men.
• OA most often occurs at the ends of the fingers, thumbs, neck, lower back, knees, and hips.

OA has been classified as….
• Primary (idiopathic)– No prior event or disease related to the OA
• Secondary– Resulting from previous joint injury or
inflammatory disease
• Distinction between primary and secondary OA is not always clear

OA
OA is a disease of joints that affects all of the weight-bearing components of the joint:

Osteoarthritis (OA) - Definition
Osteoarthritis may result from wear and tear on the joint
•The normal cartilage lining is gradually worn away and the underlying bone is exposed.

Age
• Age is the strongest risk factor for OA. Although OA can start in young adulthood, if you are over 45 years old, you are
at higher risk.
Female gender
• In general, arthritis occurs more frequently in women than in men. Before age 45, OA occurs more frequently in men;
after age 45, OA is more common in women. OA of the hand is particularly common among women.
Joint alignment
• People with joints that move or fit together incorrectly, such as bow legs, a dislocated hip, or double-jointedness, are
more likely to develop OA in those joints.
OA – Risk Factors

Hereditary gene defect
• A defect in one of the genes responsible for the cartilage component collagen can cause deterioration of cartilage.
Joint injury or overuse caused by physical labor or sports
• Traumatic injury (ex. Ligament tears) to the knee or hip increases your risk for developing OA in these joints. Joints
that are used repeatedly in certain jobs may be more likely to develop OA because of injury or overuse.
Obesity
• Being overweight during midlife or the later years is among the strongest risk factors for OA of the knee.
OA – Risk Factors

Genetic andhormonalfactors
Other
Mechanicalinjury
Chondrocyte response
Release of cytokines
Stimulation, production and release of proteolyticenzymes, metalloproteases, collagenase
Resulting damage predisposes tomore....
Previous jointdamage

OA – Articular Cartilage
Articular cartilage is the main tissue affected OA results in:
•Increased tissue swelling•Change in color•Cartilage fibrillation•Cartilage erosion down to subchondral bone


Asymmetrical joint space narrowing from loss of articular cartilage
The medial (inside) part of the knee is most commonly affected by osteoarthritis.
OA – Radiographic Diagnosis

OA – Symptoms• OA usually occurs slowly - It may be many years
before the damage to the joint becomes noticeable
• Only a third of people whose X-rays show OA report pain or other symptoms:
– Steady or intermittent pain in a joint – Stiffness that tends to follow periods of inactivity, such as sleep
or sitting – Swelling or tenderness in one or more joints [not necessarily
occurring on both sides of the body at the same time] – Crunching feeling or sound of bone rubbing on bone (called
crepitus) when the joint is used

Diagnostic Findings
• You'll need to describe your symptoms in detail, including the location and frequency of any pain
• Examination of the affected joints• X-rays or other imaging studies• blood tests are used to rule out other forms of
arthritis


Medical Management
• No treatment halts the degenerative process• preventive measures can slow the progress– weight reduction– prevention of injuries– perinatal screening for congenital hip disease, and
occupational modifications.
• Conservative treatment measures– use of heat– weight reduction, joint rest and avoidance of joint
overuse– orthotic devices to support inflamed joints
(splints, braces)– postural exercises and aerobic exercise

PHARMACOLOGIC THERAPY• Pharmacologic management of OA is directed
toward symptom management and pain control
• Initial analgesic therapy is acetaminophen• Nonselective NSAIDs• Opioids and intra-articular corticosteroids• glucosamine and chondroitin - which are
thought to improve tissue function and retard breakdown of cartilage

Surgical management
• Osteotomy (to alter the force distribution in the joint)
• Arthroplasty• viscosupplementation (the reconstitution of
synovial fluid viscosity)- Hyaluronic acid• Tidal irrigation (lavage)- of the knee involves
the introduction and then removal of a large volume of saline into the joint through cannulas.

Proximal Tibial Osteotomy
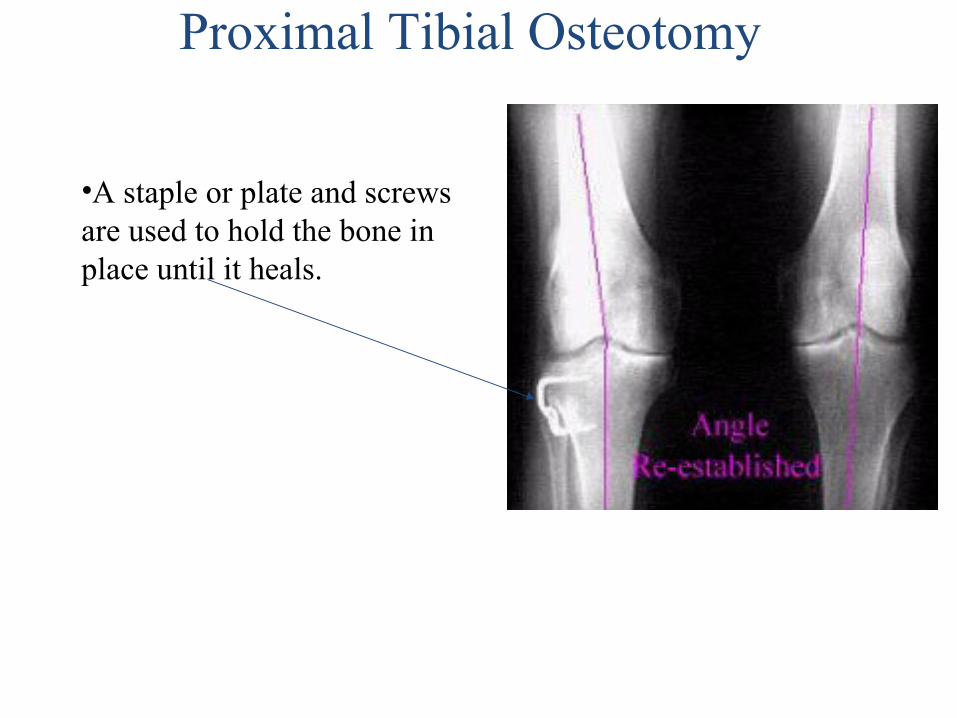
Proximal Tibial Osteotomy
•A staple or plate and screws are used to hold the bone in place until it heals.

•The ends of the femur, tibia, and patella are shaped to accept the artificial surfaces. •The end result is that all moving surfaces of the knee are metal against plastic
Total Knee Replacement

Total Knee Replacement

•OA is a condition which progresses slowly over a period of many years and cannot be cured•Treatment is directed at decreasing the symptoms of the condition, and slowing the progress of the condition
•Functional treatment goals:•Limit pain•Increase range of motion•Increase muscle strength
OA – Disease Management

OA – Non-operative Treatments
•Pain medications•Physical therapy•Walking aids•Shock absorption•Re-alignment through orthotics•Limit strain to affected areas

Nursing ManagementNursing Assessment for Osteoarthritis
• Activity / Rest– Joint pain due to movement, tenderness
worsened by stress on the joints, stiffness in the morning, usually occurs bilaterally and symmetrically functional limitations that affect lifestyle, leisure, work, fatigue, malaise.
– Limitation of movement, muscle atrophy, skin: contractor / abnormalities in the joints and muscles.

• Cardiovascular– Raynaud's phenomenon of the hand (eg litermiten
pale, cyanosis and redness on the fingers before the color returned to normal.
• Ego Integrity– Stress factors of acute / chronic (eg, financial jobs,
disability, relationship factors.– Hopelessness and helplessness (inability
situation).– Threats to the self-concept, body image, personal
identity, for example dependence on others.

• Food / Fluids– The inability to produce or consume food or
liquids adequately nausea, anorexia.– Difficulty chewing, weight loss, dryness of mucous
membranes.
• Hygiene– The difficulties to implement self-care activities,
dependence on others.

• Neurosensory– Tingling in hands and feet, swollen joints
• Pain / comfort– The acute phase of pain (probably not
accompanied by soft tissue– swelling in the joints. chronic pain and stiffness
(especially in the morning).
• Social Interaction– Damage interaction with family or others, the
changing role: isolation.
• Counseling / Learning– Family history of rheumatic– The use of health foods, vitamins, cure disease
without testing– History pericarditis, valve lesion edge. Pulmonary
fibrosis, pleuritis.

Nursing Diagnosis
• Acute / Chronic pain related to distention of tissue by the accumulation of fluid / inflammatory process, synovial joints.

• Assess pain; note the location and intensity of pain (scale 0-10).
• Write down the factors that accelerate and signs of non-verbal pain.
• Give the hard mattress, small pillow. Elevate bed when a client needs to rest / sleep.
• Help the client take a comfortable position when sleeping or sitting in a chair.

• Monitor the use of a pillow.• Help clients to frequently change positions.• Help the client to a warm bath at the time of
waking.• Help the client to a warm compress on the
sore joints several times a day.

• Monitor temperature compress.– Encourage the use of stress management
techniques such as progressive relaxation therapeutic touch, visualization, self hypnosis guidelines imagination, and breath control. Engage in activities of entertainment that is suitable for individual situations.
• Give the drug before activity / exercise that is planned as directed.
• Assist clients with physical therapy.

• Impaired Physical Mobility related to skeletal deformities, pain, discomfort, decreased muscle strength.

• Monitor the level of inflammation / pain in joints
• Maintain bed rest / sit if necessary• Schedule of activities to provide a rest period
of continuous and uninterrupted night time sleep.
• Assist clients with range of motion active / passive and resistive exercise and isometric if possible.

• Slide to maintain an upright position and sitting height, standing, and walking.
• Provide a safe environment, for example, raise the chair / toilet, use a high grip and tub and toilet, the use of mobility aids / wheelchairs rescue.
• Collaboration physical therapist / occupational specialist.

• Anxiety related to operative procedures• Risk for infection related to long term use of
corticosteroids • Risk for injury related to mobility changes
secondary to osteoarthritis • Knowledge deficit about condition, prognosis
and treatment needs related to lack of information.

Thank you