orthognathic surgery of adults and facial aesthetics · to each case, functional and esthetic...
TRANSCRIPT
Address for correspondence:
J.-B. CHARRIER,Department of Cervico-maxillo-facial surgery78, avenue du General Le-clerc,94275 Kremlin-Bicetre Cedex, [email protected]
DOI: 10.1051/odfen/2012202 J Dentofacial Anom Orthod 2012;15:302� RODF / EDP Sciences
1
Orthognathic surgery ofadults and facial aesthetics
Jean-Baptiste CHARRIER
ABSTRACT
Orthognathic surgery has as its objective the repositioning of basal bone inthe framework of maxillo-mandibular deformities. Its results are both estheticand functional. For adults, improved aesthetics results is becoming increasinglyimportant in these procedures to the point where some patients seek only anesthetic amelioration and not a functional one. To achieve their aestheticpurpose, it is becoming progressively more necessary for orthodontists, oralsurgeons, and general dentists to collaborate effectively in a well-coordinatedeffort. In what has now become a true sub-specialty, orthognathic surgeonsmust master the complementary techniques of rhinoplasty, osseous apposition,aesthetic facial surgery, fat injection or injectable anti-aging tratments. In thisarticle we propose a diagnostic classification based on the aesthetics of theadult smile and describe the therapeutic modalities appropriate for eachelement.
KEY WORDS
Orthognathic surgery,
Aesthetics of the face,
Orthodontic and orthognathic treatment.
1 – INTRODUCTION
Orthognathic surgery, or surgery of max-illo-mandibular bones, has for its purposecorrection of malpositions of basal bone andthe malocclusions that is often associatedwith them.
Conflicts of interest declared by author: NONEArticle received: 12-2011.
Accepted for publication: 02-2012.
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2012202

The objectives of this multi-disci-plinary team care are both functional,re-establishment of static and dy-namic occlusal capacities; and mor-phological, a stable restitution of theskeletal balance of the face, which, aswe shall see, most often focuses onesthetic improvement of the visage.
This management of dento-facialskeletal anomalies is accomplishedby a multi-disciplinary team based onclose collaboration between surgeonand orthodontist who ask other parti-cipants to join in their endeavors.Surgeons cannot achieve balancedrestructuring of skeletal elements un-less preliminary stages of dental treat-ment have been completed inaccordance with a rigorous treatmentplan elaborated by surgeons andorthodontists assisted by generalpractitioners, implantologists, andspeech therapists or other teachingspecialists.
This type of morpho-functional sur-gery of the face has developed con-siderably over the past 15 years,particularly for adults, because of thegreat improvement in orthodontictechniques, in surgical osteosynthesismaterials, and the systemization ofsurgical techniques and also becauseof a better integration of the multi-disciplinary protocol, especially withregard to orthodontics and surgery,and amelioration of functional re-edu-cation methods. That is why this typeof treatment that was only a few yearsago daunting to practitioners andprospective patients, is being prac-
ticed routinely in many dentofacialorthopedic offices and clinical centers.
In this article we don’t intend topresent an exhaustive orthodontic-andorthognathic treatment approach butinstead we plan to review the basis forand the philosophy of these proce-dures that, above all, consist of a jointeffort whose success depends uponeffective collaboration between mem-bers of a multi-disciplinary team. Weshall offer an esthetic ‘‘extra-oral’’clinical approach not focused on oc-clusal anomalies but on anomalies of
the positions of teeth within the
smile and the therapeutic options thatwe have at our disposal for placing
those teeth in correct positions
within the smile.
In the first section of this article weshall outline the objectives of theorthodontic-and orthognathic treat-ment, we shall make clear what kindof an assessment is needed to estab-lish such protocols, and we shalldescribe different indications for treat-ment in response to the varyingpositions of teeth within the smile.
To conclude, we shall discuss theimplications of planning highly indivi-dualized surgical procedures based onclinical and esthetic analyses of everypatient. To support this innovativeapproach we shall then show therecords of clinical cases for whichwe have not strictly adhered to tradi-tional notions of contact betweenupper and lower lips at rest and thenormalization of the maxillary occlusalplane.
2 – GENERAL COMMENTS
The term ‘‘orthognathic’’ comesfrom the Greek ortho (straight) and
gnathos (jaw). This straight jaw sur-gery developed only recently, largely
JEAN-BAPTISTE CHARRIER
2 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

during the exuberant growth of med-ical and dental science over the lastthirty years, when it emerged frommaxillo-facial surgery, to become asub-specialty of its own, orthognathicsurgery was aided by collaboration ofdento-facial orthopedic colleagues.This joint effort of surgeons andorthodontists has made it possiblefor team members to establish cor-rective treatment plans with precisionand to execute them with rigor.
Beauty, which is a central conceptin all cultures, and physical appear-ance have always played key roles inthe development of individual selfesteem, in the establishment of inter-personal relations, and even the qual-ity of life, are, accordingly carefullyconsidered in these treatment plans.So the competence of orthognathicsurgeon in no way limits itself to amechanical occlusal or stomatologicalapproach but integrates knowledge ofthe techniques of cosmetic surgery ofthe visage with procedures for cor-recting basal bone. The orthognathicsurgeon is, above all, a surgeon of theface who is philosophically committedto incorporating surgery of the jawswith plastic surgery and reconstruc-tion of the face.
2 – 1 Vertical analysis
From a frontal view, the maxillo-mandibular jaws, composed of thetwo maxillary bones and the mandible,occupy the middle and lower thirds ofthe face. Artists consider the face tobe divided in three stages of equalheight, whose respective cutaneouslimits are the anterior zone of theinsertion of the hairline, the upper
border of the eyebrows, the sub-nasalpoint, and the sub-mental point. Thearea of activity of orthognathic sur-geons is primarily the lower third ofthe face, which is itself divided intothree stages of equal height:– the first stage extends from the
from the free edge of the columellato the intercommisural line of thelips;
– the two other stages extend fromthe intercommisssural line to thefree edge of the chin (Fig. 1).
2 – 2 Sagittal analysis
In the sagittal plane, a lack ofbalance of the profile is often corre-lated with a lack of facial balance. Theesthetic considerations of the profileof the visage act so that a harmoniousvisage ought to be presented. Currentesthetic standards seek, above all, topresent the lower third of the face thatis synonymous with youth. Actually,from an esthetic point of view ‘‘any-thing that retreats grows older, every-thing that advances rejuvenates.’’Why do older people look old? Be-cause of the atrophy of fatty cheektissue and drooping of the cheek’scutaneous covering that reduce theprojection of the middle stage of theface and because loss of teethdeprives lips of support as bi-maxillaryretrusion takes place.
Accordingly, there is often a correla-tion between the esthetic approachfor the visage of the face and theprofile because the normo-divergenttransfacial profile with contact of theupper and lower lips at rest corre-sponds most closely to contemporaryesthetic norms.
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 3
In addition to establishing a stablefunctional occlusion, orthognathicsurgeons tend to have esthetic objec-tives that include creating verticalbalance between various facial unitswith a major focus on obtaining lip
contact at rest and assuring thestability of treatment by having labialmuscles bundles act as a retainingforce, and providing good nasal venti-lation when lips are closed at rest. Inthe absence of bilabial contact, the
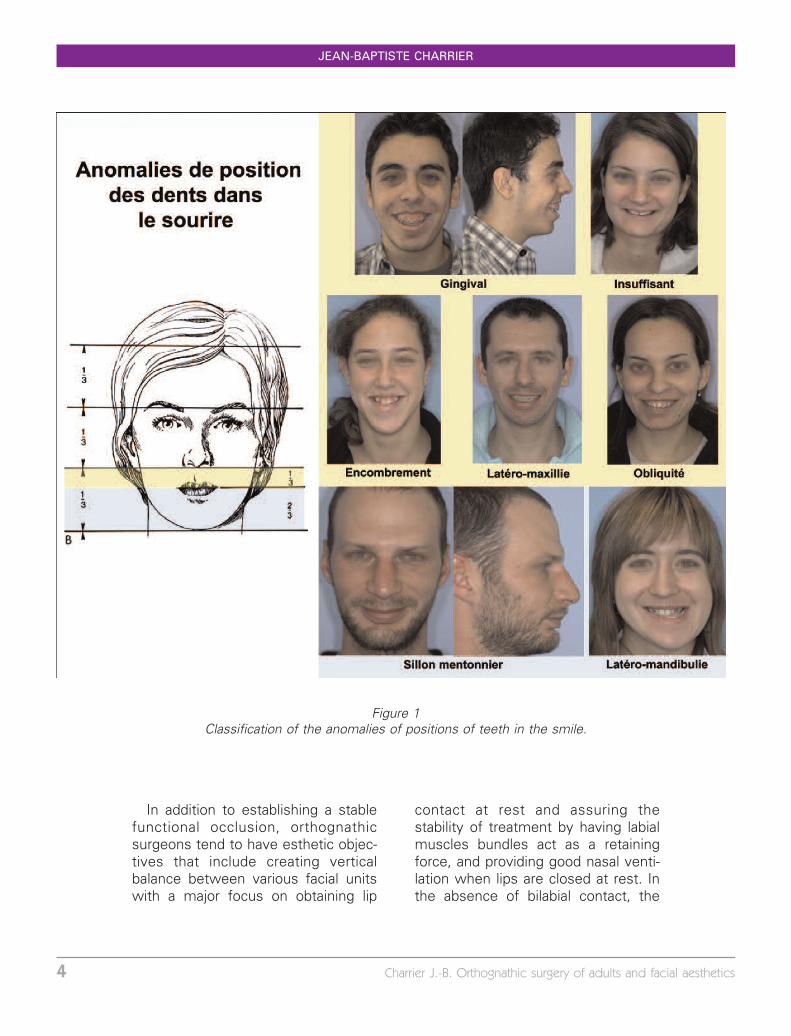
Figure 1Classification of the anomalies of positions of teeth in the smile.
JEAN-BAPTISTE CHARRIER
4 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

law of least effort induces children tochoose mouth breathing leaving thetongue free to push against teeth andrisk of making them progressivelymore mobile. Moreover, a sponta-neous lips closed posture at restconfers a relaxed and refreshed ap-pearance to the visage and improvesthe esthetic aspect of the entire face.
A continuous thrusting of the ton-gue between the incisor teeth can
loosen them perceptibly and somepatients keep this up for years. Toprevent this from happening, thetreatment team must arrange for ananterior deep bite and try to trainpatients to permanently control theirtongues from passing between upperand lower teeth. Otherwise someextent of relapse is inevitable.
3 – ANOMALIES OF TOOTH POSITION IN THE SMILE: ASSESSMENT ANDTREATMENT PLAN
As a smile unfolds, the lips part andthe upper lip reveal the maxillaryanterior teeth between the right andleft premolars. Normally, the upperincisors are fully visible right up to thegingival festoon line. Uncovering ofteeth in faulty smiles can range fromshowing too much gingiva, a gummysmile, to an insufficient revealing ofteeth or to oblique or asymmetricrevealing of teeth associated with atilted occlusal plane.
The orthognathic surgeons’ compe-tence in treating is limited to adjustingthe position, the dimensions, or thevolume of the lips. They can improvesmiles by modifying basal bone ineither or both jaws. They can reposi-tion teeth in the smile and achievecontact between upper and lower lipsat rest to give the visage a harmoniousand relaxed appearance.
Surgeons must also set, accordingto each case, functional and estheticobjectives to correct any antero-pos-terior or transverse disharmonies aswell as asymmetries.
3 – 1 Treatment plan
All team members must participatein the systematic elaboration of treat-ment plans for patients presentingmaxillo-mandibular disharmonies. Inroutine practice, this assessment willinclude the following points.• General evaluation of the patient
Patients who are candidates forpossible orthodontic-surgical treat-ment are usually in good health.However, since these procedures aresometimes offered to patients ofsomewhat advanced years, treatmentplanners must make a systematicsearch for any existing diseases,especially cardio-pulmonary diseases,that may be severe especially inprospective patients with ventilationproblems like sleep apnea.
The team must make a thoroughpresentation to patients about theadvantages, inconveniences, and risksinherent in these therapies.
Potential hemostasis problemsmust be carefully evaluated through
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 5

questioning patients and using pro-thrombin testing or the internationalnormalized ratio (INR) because thissurgery can potentially cause hemor-rhaging.
Then treatment planners shouldcomplete their general evaluation ofpatients by a scrupulous analyses oftheir dental histories and, only after allthis, begin the preliminary orthodontictreatment, during which a furtherstudy of the patient’s tolerance fortreatment, state of oral hygiene, anddental and periodontal health.
Taking into account its affect onmicrocirculation and the healing pro-cess, it is indispensable to informpatients of the harmful effect ofconsuming tobacco, and that theymust cease using it at least onemonth before treatment begins.• Socio-physiological evaluation
It is essential for the team toundertake socio-physiological evalua-tions of patients before beginning anysurgical or orthodontic therapy. Thecourse is going to be long and arduousfor the patients, and they must be wellmotivated from the start. These thera-pies are markedly different from ortho-dontic treatment alone.
Patients must understand that oncetreatment begins it will be difficult toreverse course especially since someskeletal modifications change the vi-sage profoundly.
We believe it is advisable for psy-chologists to review the overall com-mitment that is involved particularlybecause most patients’ primary rea-son for seeking therapy is to obtainesthetic benefits.
They may find it difficult to compre-hend the occlusal and morphological
aspects of therapy if they have nobackground in medicine. Of course,we are prepared and quite willing toshow them records of patients treatedfor problems similar to their own sothat they can gain a good perspectiveof what to expect.
And, of course, it is important toprepare patients for the prospect ofpreparatory orthodontic treatmentseemingly worsening their appear-ance as the teeth are prepared toharmonize with the surgical protocolbut that the final post-surgical resultwill provide the desired favorablechanges.
Good understanding and coopera-tion between patients and all treat-ment team members is a key elementin successful therapy.• Evaluation of facial aesthetics
Practitioners evaluate facial aes-thetics from both frontal and profileaspects. They then inform patients thattheir orthodontic-and orthognathictreatments will change their visagesalmost always in the direction ofharmonizing facial equilibrium that isin improving both their frontal and theirprofile appearances. In particular, thetreatment team must evaluate thethree stages of the face (frontal, med-ian third, and chin) in estimating theirrespective lack of balance in the frontaland sagittal planes and their possibleasymmetries in the frontal plane.
The important points in the estheticevaluation of patients are:– Bilabial contact at rest and the
possible distance that separatesthe two lips in a perfectly relaxedvisage. When patients cannot ea-sily close their lips at rest, whenthey close them forcibly that leads
JEAN-BAPTISTE CHARRIER
6 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

to a contraction of chin musclesthat gives the visage a strainedlook;
– The existence (or lack of) a gummysmile that is considered unsightlywhen it is excessive;
– The presence, or lack of, midlinesymmetry of upper and lower ante-rior teeth and the position of chin;The initial assessment is always
supported by standardized photos ofthe visage in frontal, and right and leftthree quarter and profile views as wellas by complete intraoral photographs.• Radiological assessment
X-rays taken include a profile cepha-logram, a panoramic film, and fullmouth periapical series taken withlong cone technique.
Examiners can assess basal bone inits antero-posterior and vertical as-pects from a profile cephalogram.Numerous methods, including theDelaire, Downs, Steiner, Ballard, Sas-souni, and Ricketts analyses are avail-able for making precise antero-posterior calculations of mandibularand maxillary basal bone anomaliesand for studying facial divergences inthe vertical plane; all elements criticalfor elaboration of a treatment plan.
The frontal cephalogram is used toevaluate asymmetries.
With the panographic radiograph,examiners can make a rapid assess-ment of possible dental caries, areasof infection, and the presence ofimpacted teeth but this X-ray doesnot replace the full series of periapicalfilms. If an osteotomy is contem-plated, any necessary third molarremovals should be performed sixmonths before the scheduled proce-dure so that the extraction sites,which are the zones of the osteotomy
osseous consolidation, can fill in be-fore surgery or, as an alternative, thesurgeon can remove wisdom toothbuds as an initial step in the osteot-omy. Dentists must place the denti-tions of patients scheduled forpreparatory orthodontic treatment inexcellent condition by extracting allnon-restorable teeth, making appropri-ate restorations for all teeth requiringthem, executing a scrupulous prophy-laxis, and performing periodontalor endodontic treatment whereindicated.
The great strides made in recentyears in the use of cone beamcomputed tomography and the devel-opment of three-dimensional softwareprograms for assessing the mandibleand the maxilla, as well as the devel-opment of pre-operative simulationtechniques have all contributed tothe probable imminent elimination ofprofile cephalograms as surgicalevaluation tools.• Evaluation of the occlusion
Examiners assess patients’ occlu-sions in all three planes of space,antero-posterior, transverse, and ver-tical in establishing one of the funda-mental elements for formulating atreatment plan. To accomplish thisand document any possible dento-maxillo-facial anomalies they mustestablish a stable maxillo-mandibularreference position. When asymme-tries seem to be present they mustbe careful to detect the presence offalse or functional bites that may becausing false lateral positions of themandible.
They must carefully explain to pa-tients before preparatory orthodontictreatment begins that this phase ofdecomposition and coordination of the
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 7

arches will often tend to exaggerateocclusal discrepancies, at least in theantero-postero sense, and give theappearance that therapy has goneawry so that patients won’t be dis-couraged by this necessary pre-opera-tive stage.
Dentists should not undertake oc-clusal equilibration, especially when ill-fitting crowns are present, until theremoval of orthodontic appliances.Placement of implant, if needed,should also be deferred until the endof treatment.• Evaluation of the TMJ and of
functional problems
Before any treatment is undertakendentists should assess the action ofthe TMJs in relation to occlusion inopening and closing of the jaw and inantero-postero, vertical, propulsive,and diduction movements. Dentiststhen list symptoms associated withthe TMJ so that they can be consid-ered schematically in an orthodontic-and orthognathic treatment designedto stabilize, even eliminate TMD pro-blems by equilibrating occlusal forces,except in the rare instances when itaggravates them.
In order to search for a possiblenasal obstruction, an examination ofthe nasal fossas must be made andcompleted by a nasofibroscopy. Ifsymptoms suggest the presence of anocturnal ventilatory obstruction, aventilatory polygraph will be needed.In some cases where there is markednasal deviation, a correction of theseptum can be carried out a fewmonths before the planned osteotomybecause minor septal deviations cancorrected during a Fort 1 osteotomiesmore serious ones cannot. They re-
quire an adapted pre-prepared path-way performed under videoscopiccontrol through an endonasal route.
The orthodontist studies the pos-ture and volume of the tongue at restand during deglutition to discern pos-sible abnormal swallowing that wouldrequire re-education that would, mostfrequently be undertaken at the end oftreatment. However, in some cases itis advisable for speech therapists orkinesitherapists to begin it before orduring orthodontic therapy.
In our practice, during the firstconsultation we discuss with thepatients the three fundamental build-ing blocks that assure the effective-ness and stability of this type ofsurgico-orthodontic therapy: surgeryand orthodontics that are intimatelycoordinated but most, independentlyachieve certain goals, and also the re-training of tongue posture and ofswallowing that are the patient’s life-long responsibility, any lapse of whichcould provoke relapse of the originalmalocclusion.
The functional evaluation, which isas important as the occlusal andesthetic evaluations, requires a goodunderstanding of the functions ofventilation and of speech. The objec-tive of our protocols is not just to haveobtained a good result at the time ofremoval of orthodontic appliances butone that will stand the test of time byhaving eliminated bad habits andventilatory anomalies.
At the end of various therapystages, we review our treatment planwith the patient in conjunction with allmembers of the treatment team. Itseems to us essential that we gain theconfidence of patients during the
JEAN-BAPTISTE CHARRIER
8 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

initial consultation and also their com-plete agreement with and cooperationwith an arduous and lengthy protocol.
3 – 2 – Classification ofanomalies and positionof teeth in the smile
We describe the principal anomaliesof position of teeth in the smile belowin terms of an ‘‘extra-oral’’ surgicalclinical approach to the lower third ofthe face, site of the principal action ofthe orthognathic surgeon. This is anarbitrarily chosen vertical approach tothe frontal visage of the face; anysagittal anomalies, the visage of theprofile, are almost always combinedand coordinated with frontal faults.The lower third of the face is itselfdivided into three stages. We deal firstwith the superior third and nextcorrect the lower two thirds (Fig. 1).• Disharmony of the upper third
It is imperative that any manage-ment of these anomalies must includea surgical procedure for the maxilla.– Gummy smile All smiles that
reveal more than two mm ofgingiva are included in this cate-gory. This gingival exposure lends asomewhat comical character to aperson’s visage, which, if pro-nounced, can be upsetting to thatindividual. Patients of North Africanand Spanish descent are particularlysensitive on this subject. Manyadults have consulted us about anoccasional gummy smile that is notassociated with an occlusal anom-aly. Psychological management ofthese patients must be executedwith extreme care because theirgoal is exclusively esthetic and the
morphological change will be criti-cal. Furthermore, the transforma-tion of the visage generated bysurgery will modify the patient’spersonality in the eyes of othersbecause they will have lost theircomical facial expression.
– Insufficient smile: The upper inci-sors are not visible over their entirelength making the smile look olderthan he actually is. Sometimesthese patients have had premolarsextracted as a component of ortho-dontic treatment in an effort toavoid surgery but were not satisfiedwith the result. If any adjustment ofmaxillary vertical dimension is con-templated, the surgeon will have touse bone grafts in order to avoid anunstable result, one readily subjectto relapse.
– Crowding: which gives the smile adisorderly aspect. Surgical expan-sion of the maxilla ultimately asso-ciated with corticotomies, maymake it possible for the treatmentteam to avoid extracting teeth.
– Latero-maxilla, or maxillary
asymmetry: which can result fromagenesis or loss of teeth unilaterally(the term ‘‘latero-maxillo,’’ widelyused by surgeons does not actuallyexist in accepted nomenclature,unlike the term ‘‘latero-mandible.’’Latero-maxilla refers to asymme-tries of the upper arch with adiscrepancy between the uppermidline and the sagittal midline ofthe visage.) In contrast to themandibular midline, which is unno-ticed in a smile, an off-centermaxillary midline can be quite un-attractive. If orthognathic surgery iscontemplated, there is no need forthe orthodontist to attempt to cor-rect this discrepancy.
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 9
– Tilting of the maxillary occlusal
plane: this anomaly of position ofthe teeth in the smile, whichtongue thrusting can cause, isparticularly unsightly. Frequentlyteeth in this posture can becomestiffed. To correct this tilting thetreatment team must deal with itsevery aspect otherwise instabilityand relapse are possible.
• Disharmony of the lower third
It is imperative that management ofthese anomalies includes surgery ofthe mandible and/or of the chin area.– Latero-mandible: With the mand-
ible displaced toward one side,there is usually a discrepancy be-tween upper and lower midlines.This type of smile problem requires
unilateral or bilateral osteotomy,sometimes associated with oss-eous adjustment of the chin area.
– Excessively marked If the labio-chin groove is too deep and, asoften happens, is associated with ashort lower third of the and a ClassII division 2 malocclusion, the vi-sage will present a closed andhostile aspect. So surgeons lowerchin with the aid of a bone graftin conjunction with mandibularsurgery.
In cases of combined anomaliesof insufficiency or excess or upperand lower stages, we usually doboth maxillo and mandibular surgicalprocedures.
4 – SURGICAL TECHNIQUES
The principal osteotomy techniquesinclude segmentary and complete os-teotomies of the maxillary table and themandible, and also the more recenttechnique of single interdental cortico-tomies, all, except the corticotomies,performed under general anesthesiawith naso-tracheal intubation. Sur-geons always gain access intraorallythus leaving no visible facial scars. Thechoice of the surgical approach em-ployed depends on the establishedtreatment plan but may be modifiedduring the course of preparatory ortho-dontic treatment in accordance withocclusion achieved by orthodonticforces and residual growth potential.
4 – 1 – Mandibular osteotomies
• Epker’s trans-ramal sagittal
osteotomy
Epker modified the original mandib-ular trans-ramal osteotomy thatDalpont and Obwegeser describedby proposing an internal corticotomyincision on the ramus in a lowerposition than those of his predeces-sors, at a point facing the Spix spinewhere the mandibular nerve entersthe mandible4,5.
And it is in the mandible thatsurgeons most frequently employ thisintervention where its objective is toseparate the dental arch and the tworami from the body of the mandible,while always respecting the osseouspassage of the inferior alveolar nerve.The nerve’s route starts buccallybehind the upper lip in the form of abird’s wing so that it can take a V-Yshape as the lips close. The osseousincision line is more or less high,situated in the position that best
JEAN-BAPTISTE CHARRIER
10 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics
allows the surgeon to mobilize themaxillary sector for advancement, im-paction, lowering, distalizing, or re-centering in cases of rotation orwhatever other position is desired.The specific risk for this procedure isthat the anesthetized palatal pediclewill have sequellae affecting the pa-late and the upper teeth.
For adults and some other patientswith narrow palates, it may be advi-sable to use surgically assisted rapidpalatal expansion before the majorsurgery to gain the required trans-verse width. This procedure demandsthe same surgical time as a Le Fort 1but not the lowering of the maxillarytable.• Schuchardtsegmented osteotomy
With this osteotomy surgeons canessentially mobilize the premolar mo-lar segments bilaterally with the goalof intruding them to correct an anterioropen bite. They can also tilt crownsbuccally or palatally as a separateprocedure or in conjunction with in-gression of the maxillary table. Thespecific risk of this procedure is that itmight cut off the vascular supply ofthe posterior teeth. But with the newpossibilities of orthodontists movingteeth in hitherto impossible waysthanks to anchorage supplied by min-iscrews and the introduction of corti-cotomies, the need for the this type ofsegmented osteotomy has greatlydiminished.• Wassmund’ssegmentedosteotomy
With this osteotomy and the ac-companying extraction of the upperfirst bicuspids, surgeons can retractthe incisor-canine bloc. With it theycan also tilt those anterior teethlabially or palatally as a single proce-
dure or as a component of the retrac-tion. Surgeons begin this procedure byfirst by making two buccal verticalincisions near the necks of the firstpremolars to gain access to the piri-form orifices by tunneling through thefibro-mucosa at the junction of themaxilla and the premaxilla. The oss-eous section requires delicate touchfrom surgeons especially since theaccess view is so limited. This type ofosteotomy demands an intimate col-laboration between surgeon andorthodontist up until and after removalof the arch wire at which time a splintprepared on a set-up can be used asmeans of setting and supporting bonyfragments until plates can be screwedinto place to control osteosynthesis.The improvements of orthodontic cap-abilities thanks to secure anchoragehave also reduced the indications forthis type of osteotomy. The specificrisk for Wassmund procedure is rela-tively frequent loss of nervous sensa-tion of the anterior bloc of teeth.
4 – 2 Corticotomies
A relatively recent surgical techni-que is the creation of superficial uni-cortical alveolar corticotomies, aroundindividual teeth, before the applicationof orthodontic forces to them as ameans of accelerating their move-ment. These delicate incisions passmesially and distally to the buccal andpalatal borders of the alveolus aroundthe teeth at 3 mm below the rootapices2,3,6. Surgeons must be carefulnot to abuse medullary bone surround-ing the periodontal ligaments of af-fected teeth. Thus liberated, teethmove rapidly in response to light
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 11
forces, applied, preferably to self-ligat-ing brackets. These corticotomies canbe performed in conjunction with thepre-orthodontic extraction of wisdomteeth or surgically assisted rapid pala-tal expansion. At the present timecorticotomies conducted with theminimally invasive technique of piezo-surgery are enjoying a major surge inusage and, in our opinion deservedlyso, because we have found they cuttreatment time in half.
4 – 3 – Follow-ups to surgery
Modern orthognathic surgery,which patients tolerate quite well,requires a one to two day hospitalstay for one jaw procedure and two tothree days for surgery of both jaws.
Post-surgery status of patients isusually uneventful and if pain persistsit is easily controlled with mild analge-sics. Moderate facial edema, of vary-ing intensities, usually peaks 72 hafter surgery and disappears afterabout ten days. Most patients do notrequire post-operative fixation of thejaws, loose, easily removed, integer-maxillary elastics usually suffice. Be-cause post-operative oral hygiene isimportant, patients are asked to cleantheir teeth with a water jet type ofappliance in addition to a surgicaltoothbrush beginning the morningafter the procedure. They can eat onlyliquid foods for a week, then softfoods for the next ten days. Four to sixweeks after orthognathic surgery pa-tients can resume a normal diet.
5 – COMPLEMENTARY TECHNIQUES AND CLINICAL CASES
Surgeons may want to use supple-mentary surgical procedures afterorthognathic surgery in order to im-prove aesthetics of the visage.
5 – 1 – Rhino-septoplasty
While an endo-nasal septoplastymay sometimes precede orthognathicsurgery must follow it for the samereason that a builder does not con-struct the roof before pouring thefoundation. Similarly the nose is sup-ported by the maxilla and its correctionmust await the surgical adjustment ofthe upper jaw. Some surgeons per-form the rhinoplasty in the samesession the orthognathic procedure isaccomplished but we do not agreewith this combination because sur-
gery of basal bone requires nasalintubation, which makes endo-nasalaccess for a rhinoplasty difficult.Moreover, the edema provoked byseparation of the rising branches ofthe maxilla and the osteosynthesisfollowing a Le Fort 1 procedure makeany nasal surgical procedure impre-cise and risky. Surgeons can safelyundertake this intervention designedto complete the esthetic improvementof the visage 8 to 12 months afterremoval of the orthodontic appliance(Patient n� 3).
5 – 2 – Injection of centrifugedfatty tissue and filler
The injection of centrifuged fat, orlipostructure, that Coleman first
JEAN-BAPTISTE CHARRIER
12 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics
described, can be used to improve theappearance of the visage or, as Cole-man put it, apply rejuvenation in asyringe, especially in the zygomaticarea. It must be done at a safedistance from the site of the osteot-omy and can be performed at thesame time as the rhinoplasty. Othersynthetic filling materials, such ashyaluronic acid, polylactic acid, orbotulin toxin have been used foresthetic purposes, such as wrinkleremoval, with well documented good,but relatively short lasting results.
5 – 3 – Osseous apposition andsinus filling
Alveolar osseous grafts, which areused for edentulous areas, can becompleted before surgery as is donefor sinus filling that must be com-pleted before a Fort 1 is started orafter removal of orthodontic appli-ances.
Implantologists, prosthodontists,and technicians who construct set-ups on articulators most work in closecollaboration in treating complexedentulous cases by following a care-fully defined treatment plan but theimplants themselves are almost neverpositioned until all other treatment iscompleted.
5 – 4 – Clinical cases
• Patient n� 1
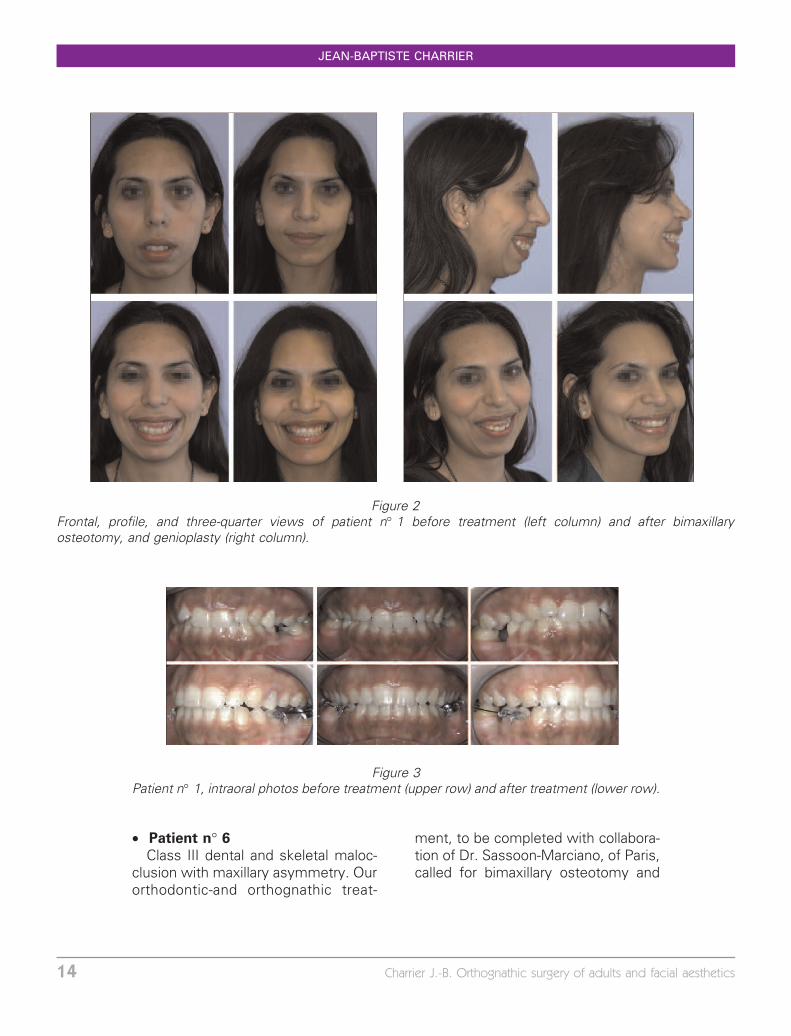
Gummy smile, with excess anteriordimension with no occlusal anomalies.Patient wanted only esthetic improve-ment. With the cooperation of Dr. DePape of Paris we prepared an ortho-dontic-and orthognathic treatment that
called for a bimaxillary osteotomy anda genioplasty. Before and after facialand intraoral photographs are shownbelow in Figures 2 and 3.• Patient n� 2
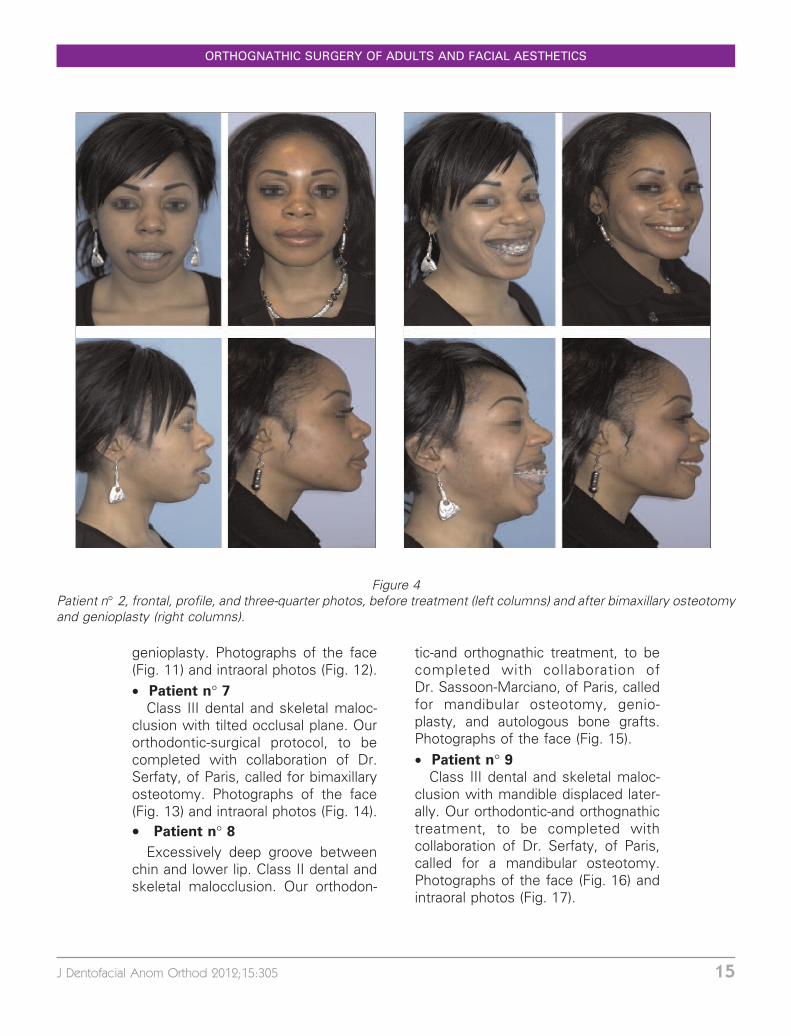
Gummy smile, with excess anteriorvertical dimension and no malocclu-sion. She wants only esthetic im-provement. Our orthodontic-andorthognathic treatment, to be per-formed in collaboration with Dr. Bedarof Drancy, calls for a bimaxillaryosteotomy and a genioplasty (Fig. 4).• Patient n� 3
Insufficient smile, Class II dental andskeletal. Our orthodontic-and orthog-nathic treatment, to be completed withcollaboration of Dr. Popelut, of Melun,called for bimaxillary osteotomy, auto-logous bone grafts, and then a rhino-plasty. Frontal, profile, and threequarter photos (Fig. 5) and intraoralphotos (Fig. 6).• Patient n� 4
Insufficient smile, Class II dental andskeletal. Our orthodontic-and orthog-nathic treatment, to be completed withcollaboration of Dr. Ohana-Toledano, ofSuresnes, called for bimaxillary osteot-omy and autologous bone grafts.Photographs of the face (Fig. 7) andintraoral photos (Fig. 8).• Patient n� 5
Crowding of teeth, in a Class IIskeletal and dental malocclusion withmaxillary asymmetry and a mandiblethat was laterally displaced after it wasfractured when she was a child. . Ourorthodontic-and orthognathic treat-ment, to be completed with collabora-tion of Dr. Bedar of Drancy maxillarypalate splitting, corticotomies, bimax-illary osteotomy, and a genioplasty.Facial photos (Fig. 9) and intraoralphotos (Fig. 10)
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 13
• Patient n� 6
Class III dental and skeletal maloc-clusion with maxillary asymmetry. Ourorthodontic-and orthognathic treat-
ment, to be completed with collabora-tion of Dr. Sassoon-Marciano, of Paris,called for bimaxillary osteotomy and
Figure 2Frontal, profile, and three-quarter views of patient n� 1 before treatment (left column) and after bimaxillaryosteotomy, and genioplasty (right column).
Figure 3Patient n� 1, intraoral photos before treatment (upper row) and after treatment (lower row).
JEAN-BAPTISTE CHARRIER
14 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics
genioplasty. Photographs of the face(Fig. 11) and intraoral photos (Fig. 12).• Patient n� 7
Class III dental and skeletal maloc-clusion with tilted occlusal plane. Ourorthodontic-surgical protocol, to becompleted with collaboration of Dr.Serfaty, of Paris, called for bimaxillaryosteotomy. Photographs of the face(Fig. 13) and intraoral photos (Fig. 14).• Patient n� 8
Excessively deep groove betweenchin and lower lip. Class II dental andskeletal malocclusion. Our orthodon-
tic-and orthognathic treatment, to becompleted with collaboration ofDr. Sassoon-Marciano, of Paris, calledfor mandibular osteotomy, genio-plasty, and autologous bone grafts.Photographs of the face (Fig. 15).• Patient n� 9
Class III dental and skeletal maloc-clusion with mandible displaced later-ally. Our orthodontic-and orthognathictreatment, to be completed withcollaboration of Dr. Serfaty, of Paris,called for a mandibular osteotomy.Photographs of the face (Fig. 16) andintraoral photos (Fig. 17).
Figure 4Patient n� 2, frontal, profile, and three-quarter photos, before treatment (left columns) and after bimaxillary osteotomyand genioplasty (right columns).
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 15
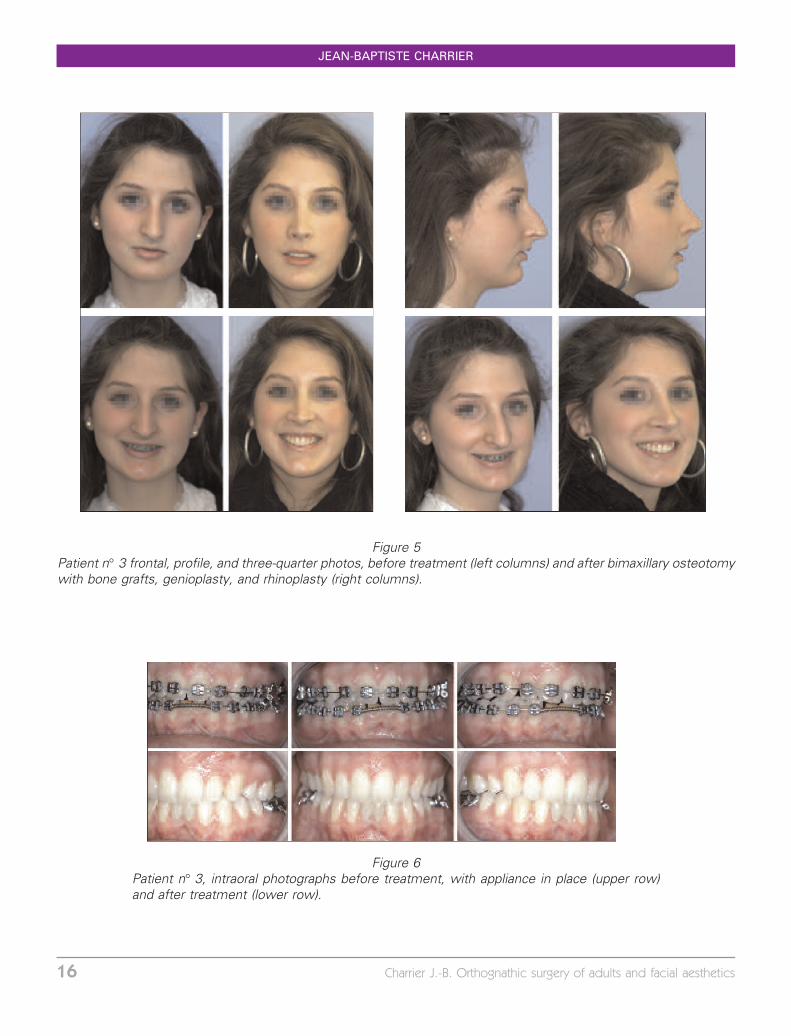
Figure 5Patient n� 3 frontal, profile, and three-quarter photos, before treatment (left columns) and after bimaxillary osteotomywith bone grafts, genioplasty, and rhinoplasty (right columns).
Figure 6Patient n� 3, intraoral photographs before treatment, with appliance in place (upper row)and after treatment (lower row).
JEAN-BAPTISTE CHARRIER
16 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics
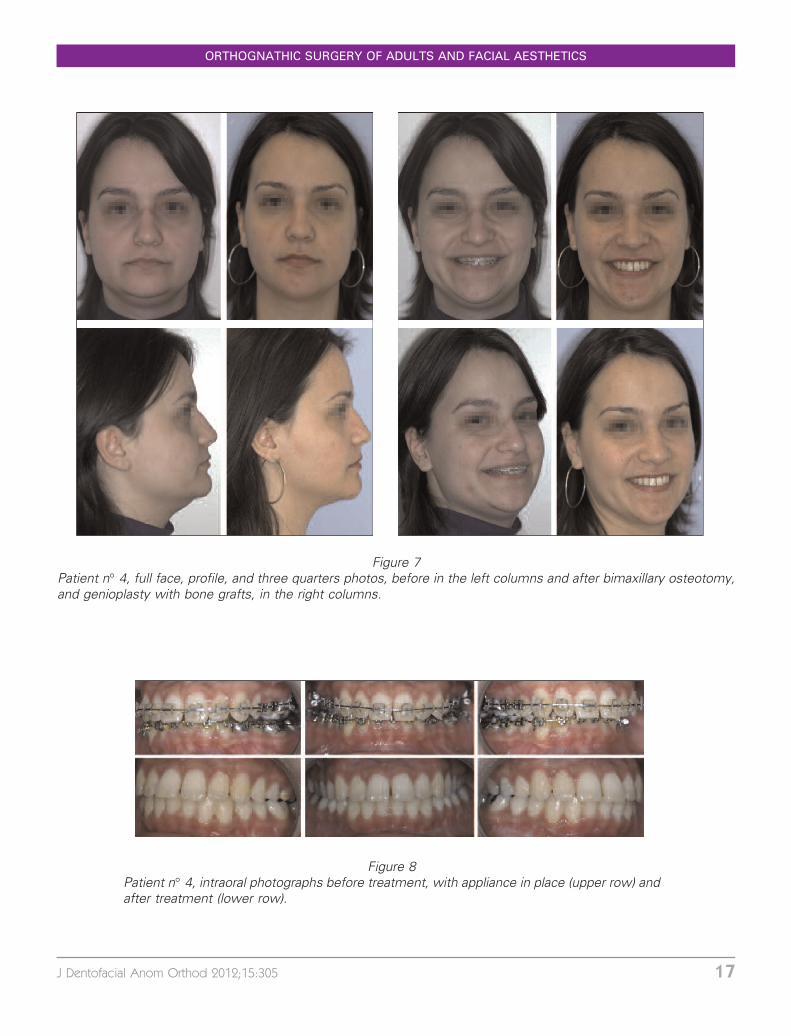
Figure 7Patient n� 4, full face, profile, and three quarters photos, before in the left columns and after bimaxillary osteotomy,and genioplasty with bone grafts, in the right columns.
Figure 8Patient n� 4, intraoral photographs before treatment, with appliance in place (upper row) andafter treatment (lower row).
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 17
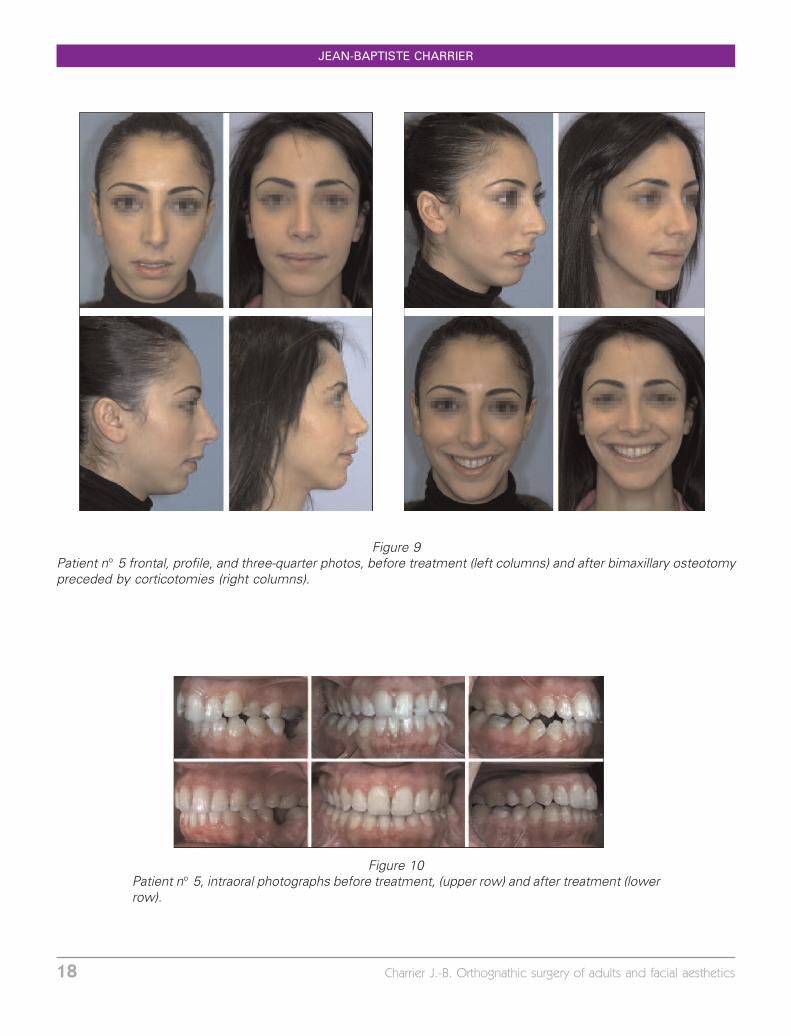
Figure 9Patient n� 5 frontal, profile, and three-quarter photos, before treatment (left columns) and after bimaxillary osteotomypreceded by corticotomies (right columns).
Figure 10Patient n� 5, intraoral photographs before treatment, (upper row) and after treatment (lowerrow).
JEAN-BAPTISTE CHARRIER
18 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics
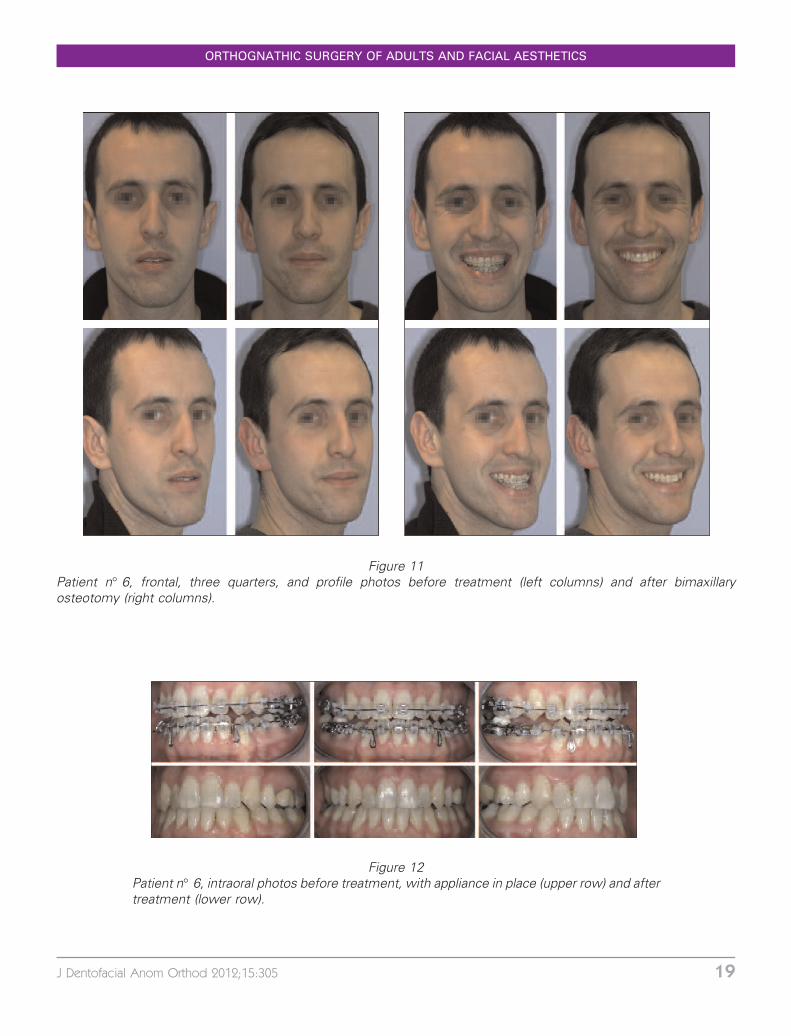
Figure 11Patient n� 6, frontal, three quarters, and profile photos before treatment (left columns) and after bimaxillaryosteotomy (right columns).
Figure 12Patient n� 6, intraoral photos before treatment, with appliance in place (upper row) and aftertreatment (lower row).
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 19

Figure 13Patient n� 7, frontal, three quarters, and profile photos before treatment (left columns) and after bimaxillaryosteotomy (right columns).
Figure 14Patient n� 7, intraoral photos before treatment, with appliance in place (upper row) and aftertreatment (lower row).
JEAN-BAPTISTE CHARRIER
20 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

6 DISCUSSION AND PERSPECTIVES
6 – 1 – Orthognathic surgery andfacial aesthetics
In modern orthognathic surgeryesthetic values are given as muchconsideration as problems of occlu-sion and of basal bone. Treatmentplans are no longer established to dealexclusively with occlusal discrepan-
cies but are also based on under-standing of and assessments of theanatomy of the bones and soft tissuesof the face, particularly with regard tothe nose whose cartilaginous struc-ture is supported by the maxilla. As anexample of the issues involved, weknow that for the same amount ofsurgical advancement of the maxilla
Figure 15Patient n� 8, frontal, profile, and three-quarters facial photographs before treatment (left columns) and aftermandibular osteotomy and genioplasty with bone grafts (right columns).
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 21

Figure 16Patient n� 9, frontal, profile, and three-quarters facial photographs before treatment (left columns) and aftermandibular osteotomy (right columns).
Figure 17Patient n� 9, intraoral photos before treatment, (upper row) and after treatment (lower row).
JEAN-BAPTISTE CHARRIER
22 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics

the consequences for the nose arequite different for the visage of aCaucasian than they are for the visageof a Black. For Blacks, the point of thenose is essentially cutaneous andderives only modest support fromthe cartilaginous septum and theinferior lateral cartilages. The conse-quences for Blacks of maxillary ad-vancement are often, accordingly, anenlargement of the wing of the noseand a lowering of the nasal tip withclosing of the naso-labial angle, whichis highly unaesthetic. It is thereforenecessary for Blacks with Class IIIdental and skeletal malocclusions tobe treated with surgical setback of themandible rather than by maxillaryadvancement. For the Caucasian vi-sage, on the other hand, the rigidity ofthe inferior lateral cartilages and thesupport of the septum have a ten-dency to project the tip of the noseforward and open the naso-labial angleduring a maxillary advancement caus-ing a positive esthetic result, if theadvancement is not too great. It is forthis reason that in cases of severemandibular prognathism, it is best forsurgeons to devise a treatment planbased on a bimaxillary osteotomy witha modest maxillary advancementcombined with a modest mandibularset-back rather than a strong maxillaryadvancement (see Fig. 13, with itsprofile photographs of patient n0 7who did not have a rhinoplasty).
Treatment plans for this type ofsurgery must be highly individualized,based on a careful clinical and estheticanalysis of each patient.
It is useful to examine examples ofanother circumstance in which es-thetic considerations should take pre-ference over functional issues, the
insufficient smile. We believe thatantero-posterior malocclusions with-out open bite, whether they are ClassII or Class III, have little tendency torelapse because of faulty tongueposture or action, if the growth periodhas ended. For these patients, thelabial and masseter muscle bundlesare often hypertonic. For some ofthem it might be advisable to concen-trate on stability and esthetic improve-ment even without achieving lipcontact at rest. So, in certain judi-ciously selected cases to leave thelips parted after conclusion of surgical-orthodontic treatment. Take for exam-ple patient n0 3 (Fig. 5) who hadpresented with an excessively shortupper lip associated with an insuffi-cient smile. In order to ameliorate hersmile, a maxillary bone graft wasrequired and, eventually, a rhinoplastywas performed. A satisfactory resultwas achieved but, at rest, her lipsremained slightly parted. A year and ahalf after removal of orthodontic appli-ances, her occlusion remains stableand she is still fully satisfied with theesthetic result achieved.
6 – 2 – Perspectives
Many researchers are now asses-sing three dimensional cephalo-metrics using special software forincorporating scanner or cone beamdata in their three dimensional recon-structions of maxillo-facial anatomicstructures. The major benefit of theseprograms resides in the possibility ofprecisely planning osteotomy opera-tive procedures, of using them toconstruct intermediary spl ints,and, thus, controlling operative posi-tioning of the maxillae thanks to digital
ORTHOGNATHIC SURGERY OF ADULTS AND FACIAL AESTHETICS
J Dentofacial Anom Orthod 2012;15:305 23

surgical navigation. These systemsare still in the development stageand remain too cumbersome for dayto day practice but in our clinicaldepartment we are engaged of clinicalstudies of these three dimensionalsystems.
Alveolar corticotomies are an effi-cient method of reducing orthodontictreatment time. With them orthodon-tists can move teeth more rapidly withlighter forces. At the close of treat-ment, the osteogenesis that tran-
spires increases the stability of theresult. But operative indications forcorticotomies must be scrutinizedcarefully2,3,6. In our experience thisminimally invasive, totally secure, andperfectly well tolerated approach pro-vides a significant reduction of treat-ment time.
A protocol for a nationwide clinicalhospital research program for cortico-tomies is currently active in France andits results should deliver precise pro-spective evaluations of this technique.
7 – CONCLUSION
Orthognathic surgery, today a dis-tinct specialty of its own, depends forthe smooth execution of its orthodon-tic-and orthognathic treatment on theintimate collaboration of all the mem-ber of its interdisciplinary teams.
In addition to that cooperation, theefficiency of that team effort requiresfrom each team member mutual andprogressively improving understand-
ing to the functioning of all the otherparticipants.
For adult patients, esthetic consid-erations form the most importantaspect of contemplated orthognathicsurgery. So all team members mustbe prepared to coordinate their effortsto satisfy the aesthetic demands oftheir joint operation even if thatrequires their taking precedence overfunctional and occlusal objectives.
REFERENCES
1 Bell WH. Modern practice in orthognathic and reconstructive surgery. Philadelphia: WBSaunders Company, 1992.
2 Charrier JB, Borhani Bryon F, Racy E, Steve M, Monteil JP, Bobin S. Traitementorthodontique accelere par corticotomies alveolaires chirurgicales chez l’adulte.International Orthodontics 2008;6:355-73.
3 Sitbon MC, Dunglas C, Charrier JB. Orthodontie acceleree par corticotomies alveolaires :approche clinique et experimentale. Rev Orthop Dento Faciale 2009;43:189-198.
4 Epker BN, Fish LC. Dentofacial deformities: integrated orthodontic and surgicalcorrection. St Louis: CV Mosby Company, 1986.
5 Obwegeser HL. Mandibular growth anomalies. Berlin Heidelberg : SpringerVerlag,2001.
6 Thierry M, Charrier JB. Les corticotomies alveolaires, principes et applications cliniques.International Orthodontics 2008;6:343-54.
7 Triaca A, Minoretti R, Saulacic N. Mandibula wing osteotomy for correction of themandibular plane: A case report. Br J Oral Maxillofac Surg 2010 Apr;48(3):182-4.
JEAN-BAPTISTE CHARRIER
24 Charrier J.-B. Orthognathic surgery of adults and facial aesthetics