orthodontic treatment for a mandibular prognathic girl … · mandibular retrognathism; increased...
TRANSCRIPT

Journal of the Formosan Medical Association (2013) 112, 801e806
Available online at www.sciencedirect.com
journal homepage: www.jfma-onl ine.com
CASE REPORT
Orthodontic treatment for a mandibular
prognathic girl of short stature undergrowth hormone therapyChin-Yun Pan a,b, Ting-Hung Lan a,b,c, Szu-Ting Chou a,b,Yu-Chuan Tseng a,b, Jenny Zwei-Chieng Chang d,e,Hong-Po Chang a,b,*
aDepartment of Dentistry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwanb School of Dentistry, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, TaiwancDepartment of Dentistry, Antai Tian-Sheng Memorial Hospital, Tong-Kang Town,Pingtung County, TaiwandDepartment of Dentistry, National Taiwan University Hospital, Taipei, TaiwaneDepartment of Dentistry, School of Dentistry, National Taiwan University, Taipei, Taiwan
Received 7 April 2010; received in revised form 30 May 2010; accepted 30 May 2010
KEYWORDSgrowth hormone;idiopathic shortstature;
mandibularprognathism;
maxillary deficiency;skeletal Class IIImalocclusion
* Corresponding author. DepartmentE-mail address: [email protected].
0929-6646/$ - see front matter Copyrhttp://dx.doi.org/10.1016/j.jfma.201
This report presents a case of a 12-year-old girl with maxillary deficiency, mandibular progna-thism, and facial asymmetry, undergoing growth hormone (GH) therapy due to idiopathic shortstature. Children of short stature with or without GH deficiency have a deviating craniofacialmorphology with overall smaller dimensions; facial retrognathism, especially mandibular ret-rognathism; and increased facial convexity. However, a complete opposite craniofacial patternwas presented in our case of a skeletal Class III girl with idiopathic short stature. The ortho-dontic treatment goal was to inhibit or change the direction of mandibular growth and stimu-late the maxillary growth of the girl during a course of GH therapy. Maxillary protraction andmandibular retraction were achieved using occipitomental anchorage (OMA) orthopedic appli-ance in the first stage of treatment. In the second stage, the patient was treated with a fixedorthodontic appliance using a modified multiple-loop edgewise archwire technique of asym-metric mechanics and an active retainer of vertical chin-cup. The treatment led to an accept-able facial profile and obvious facial asymmetry improvement. Class I dental occlusion andcoincident dental midline were also achieved. A 3½-year follow-up of the girl at age 18 showeda stable result of the orthodontic and dentofacial orthopedic treatment. Our case shows that
of Dentistry, Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung 80756, Taiwan.tw (H.-P. Chang).
ight ª 2012, Elsevier Taiwan LLC & Formosan Medical Association. All rights reserved.2.07.021

802 C.-Y. Pan et al.
Figure 1 Height growth
the OMA orthopedic appliance of maxillary protraction combined with mandibular retraction iseffective for correcting skeletal Class III malocclusion with midface deficiency and mandibularprognathism in growing children with idiopathic short stature undergoing GH therapy.Copyright ª 2012, Elsevier Taiwan LLC & Formosan Medical Association. All rights reserved.
Introduction treatment. The main purpose of this case report was to
Growth hormone (GH) is a polypeptide hormone, secretedby the anterior part of the hypophysis, and plays a majorrole in craniofacial and skeletal growth.1 Since biosynthetichuman GH obtained by genetic recombination becamewidely available in 1985,2 clinicians have been working toextend the use of recombinant human GH for short-staturechildren with classic GH deficiency to as many categories ofshort-stature children as possible. Therefore, its applica-tion in children was widened to various diseases such asTurner or Noonan syndromes, chronic renal failure, childrenborn small for their gestation age, PradereWilli syndrome,and idiopathic short stature.1,2 Cephalometric studies ofchildren with GH deficiency have shown the followingcraniofacial characteristics: small anterior and posteriorcranial base dimensions, steep mandibular plane angle, andsmall mandibular sizes including the total mandibularlength and smaller ramal height.3,4 Orthodontists shouldunderstand the characteristics of craniofacial morphologyin idiopathic short-stature children and the effects of GHtherapy on these patients prior to beginning orthodontic
curve5 for patient.
present an orthodontic case of skeletal Class III girl,undergoing GH therapy due to idiopathic short stature.
Case report
A 12-year-old girl came to our hospital with a protrudedmandible and everted lower lip as the chief complaint. Shehad been diagnosed as having idiopathic short stature atage 10. The patient had a normal birth height and weightfor her gestational age. However, she showed a slow post-natal growth rate and short stature. The hand-wrist radio-graph showed that her skeletal age was delayed by 1 year2 months compared with the chronologic age of 10. Clinicalor laboratory evidence revealed no systemic disease ofdysmorphic features. She received GH treatment ata medical center in Kaohsiung for 4 years, starting at age10. The GH treatment was effective, and she had prom-inent somatic growth until her menstruation commenced atage 13. The patient was initially 126 mm below the fifthpercentile of body height for Taiwanese girls of age 105;during the GH therapy, she moved up 135.5 mm into the15th percentile at age 11; and 146 and 151.2 mm at age 12and 13, respectively; and 154 mm into the 20th percentilewhen GH therapy ended at age 14, which was maintainedthrough age 15e18 (Fig. 1). The patient’s weight, initially22.2 kg, increased to 26.5 kg below the fifth percentile ofbody height for Taiwanese girls of age 10 and 11, respec-tively, and increased to 32, 35.6, and 37.2 kg around thefifth percentile, and then to 38.5, 39.5, and 41 kg whichwere below the fifth percentile of age 14, 15, and 18,respectively (Fig. 2).5
Orthodontic examination showed that the girl hadanterior crossbite and skeletal Class III malocclusion (T1)(Fig. 3 and Table 1). She had a concave facial profile withmaxillary deficiency and mandibular prognathism, andfacial asymmetry with the mandible deviated to the right
Figure 2 Weight growth curve5 for patient.
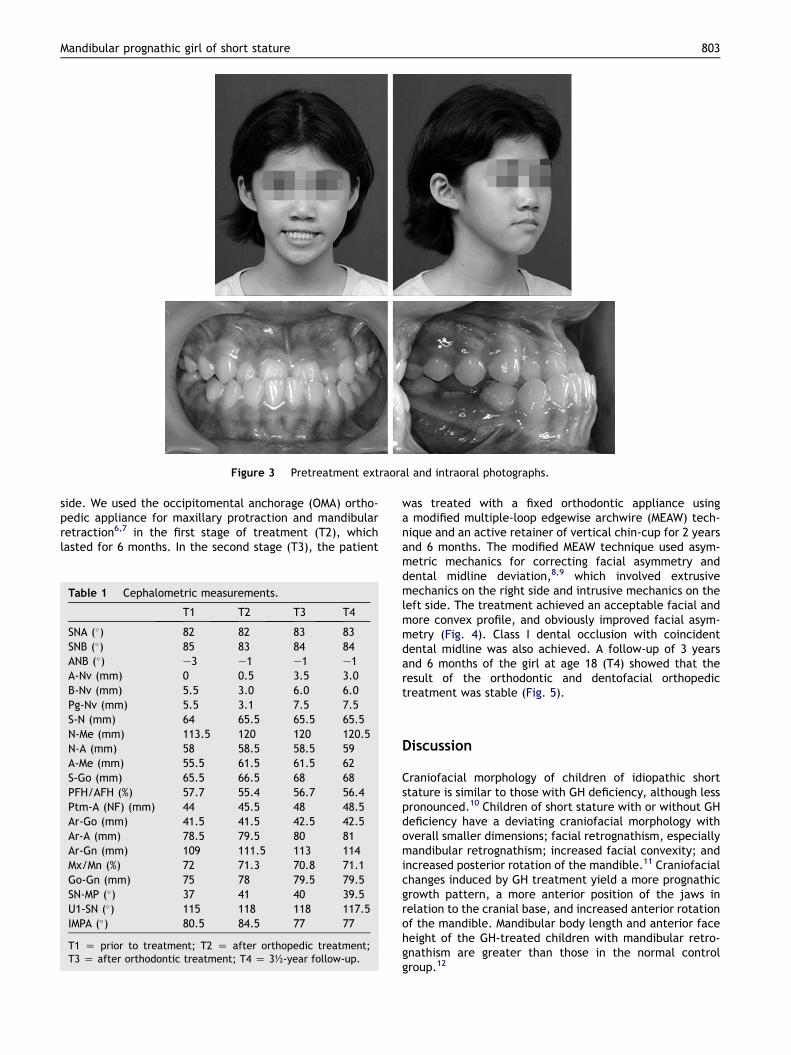
Figure 3 Pretreatment extraoral and intraoral photographs.
Mandibular prognathic girl of short stature 803
side. We used the occipitomental anchorage (OMA) ortho-pedic appliance for maxillary protraction and mandibularretraction6,7 in the first stage of treatment (T2), whichlasted for 6 months. In the second stage (T3), the patient
Table 1 Cephalometric measurements.
T1 T2 T3 T4
SNA (�) 82 82 83 83SNB (�) 85 83 84 84ANB (�) e3 e1 e1 e1A-Nv (mm) 0 0.5 3.5 3.0B-Nv (mm) 5.5 3.0 6.0 6.0Pg-Nv (mm) 5.5 3.1 7.5 7.5S-N (mm) 64 65.5 65.5 65.5N-Me (mm) 113.5 120 120 120.5N-A (mm) 58 58.5 58.5 59A-Me (mm) 55.5 61.5 61.5 62S-Go (mm) 65.5 66.5 68 68PFH/AFH (%) 57.7 55.4 56.7 56.4Ptm-A (NF) (mm) 44 45.5 48 48.5Ar-Go (mm) 41.5 41.5 42.5 42.5Ar-A (mm) 78.5 79.5 80 81Ar-Gn (mm) 109 111.5 113 114Mx/Mn (%) 72 71.3 70.8 71.1Go-Gn (mm) 75 78 79.5 79.5SN-MP (�) 37 41 40 39.5U1-SN (�) 115 118 118 117.5IMPA (�) 80.5 84.5 77 77
T1 Z prior to treatment; T2 Z after orthopedic treatment;T3 Z after orthodontic treatment; T4 Z 3½-year follow-up.
was treated with a fixed orthodontic appliance usinga modified multiple-loop edgewise archwire (MEAW) tech-nique and an active retainer of vertical chin-cup for 2 yearsand 6 months. The modified MEAW technique used asym-metric mechanics for correcting facial asymmetry anddental midline deviation,8,9 which involved extrusivemechanics on the right side and intrusive mechanics on theleft side. The treatment achieved an acceptable facial andmore convex profile, and obviously improved facial asym-metry (Fig. 4). Class I dental occlusion with coincidentdental midline was also achieved. A follow-up of 3 yearsand 6 months of the girl at age 18 (T4) showed that theresult of the orthodontic and dentofacial orthopedictreatment was stable (Fig. 5).
Discussion
Craniofacial morphology of children of idiopathic shortstature is similar to those with GH deficiency, although lesspronounced.10 Children of short stature with or without GHdeficiency have a deviating craniofacial morphology withoverall smaller dimensions; facial retrognathism, especiallymandibular retrognathism; increased facial convexity; andincreased posterior rotation of the mandible.11 Craniofacialchanges induced by GH treatment yield a more prognathicgrowth pattern, a more anterior position of the jaws inrelation to the cranial base, and increased anterior rotationof the mandible. Mandibular body length and anterior faceheight of the GH-treated children with mandibular retro-gnathism are greater than those in the normal controlgroup.12

Figure 4 Post-treatment extraoral and intraoral photographs.
Figure 5 Three-and-a-half-year follow-up extraoral and intraoral photographs.
804 C.-Y. Pan et al.
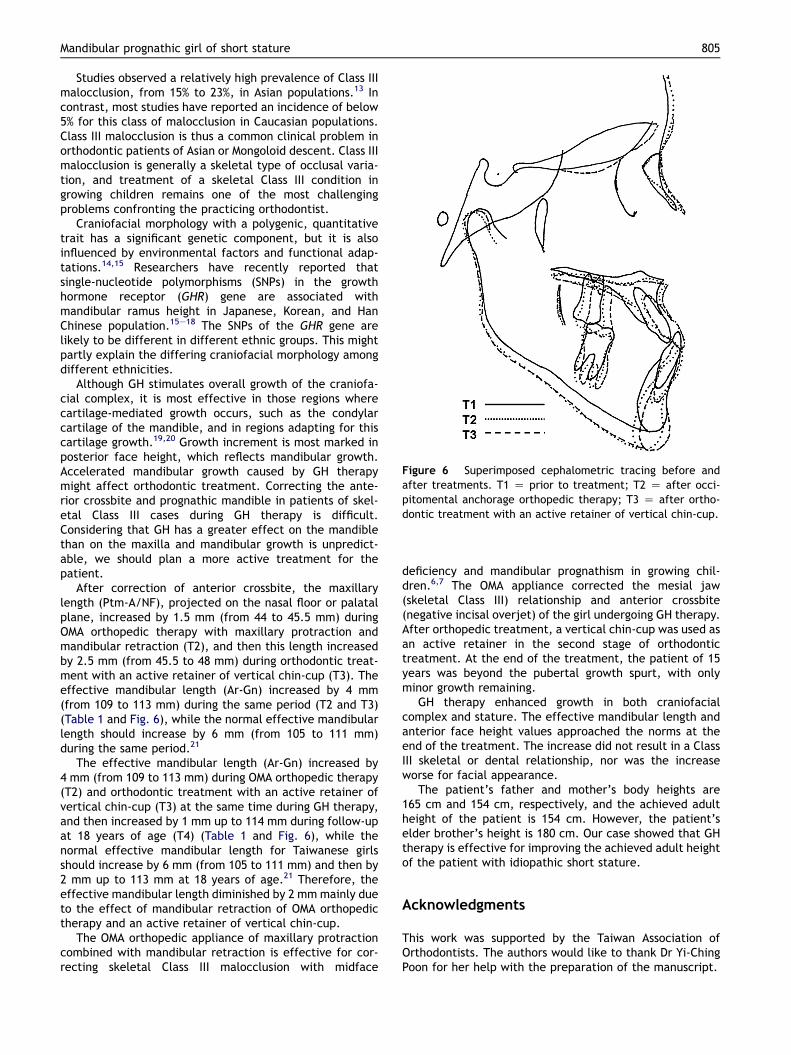
Figure 6 Superimposed cephalometric tracing before andafter treatments. T1 Z prior to treatment; T2 Z after occi-pitomental anchorage orthopedic therapy; T3 Z after ortho-dontic treatment with an active retainer of vertical chin-cup.
Mandibular prognathic girl of short stature 805
Studies observed a relatively high prevalence of Class IIImalocclusion, from 15% to 23%, in Asian populations.13 Incontrast, most studies have reported an incidence of below5% for this class of malocclusion in Caucasian populations.Class III malocclusion is thus a common clinical problem inorthodontic patients of Asian or Mongoloid descent. Class IIImalocclusion is generally a skeletal type of occlusal varia-tion, and treatment of a skeletal Class III condition ingrowing children remains one of the most challengingproblems confronting the practicing orthodontist.
Craniofacial morphology with a polygenic, quantitativetrait has a significant genetic component, but it is alsoinfluenced by environmental factors and functional adap-tations.14,15 Researchers have recently reported thatsingle-nucleotide polymorphisms (SNPs) in the growthhormone receptor (GHR) gene are associated withmandibular ramus height in Japanese, Korean, and HanChinese population.15e18 The SNPs of the GHR gene arelikely to be different in different ethnic groups. This mightpartly explain the differing craniofacial morphology amongdifferent ethnicities.
Although GH stimulates overall growth of the craniofa-cial complex, it is most effective in those regions wherecartilage-mediated growth occurs, such as the condylarcartilage of the mandible, and in regions adapting for thiscartilage growth.19,20 Growth increment is most marked inposterior face height, which reflects mandibular growth.Accelerated mandibular growth caused by GH therapymight affect orthodontic treatment. Correcting the ante-rior crossbite and prognathic mandible in patients of skel-etal Class III cases during GH therapy is difficult.Considering that GH has a greater effect on the mandiblethan on the maxilla and mandibular growth is unpredict-able, we should plan a more active treatment for thepatient.
After correction of anterior crossbite, the maxillarylength (Ptm-A/NF), projected on the nasal floor or palatalplane, increased by 1.5 mm (from 44 to 45.5 mm) duringOMA orthopedic therapy with maxillary protraction andmandibular retraction (T2), and then this length increasedby 2.5 mm (from 45.5 to 48 mm) during orthodontic treat-ment with an active retainer of vertical chin-cup (T3). Theeffective mandibular length (Ar-Gn) increased by 4 mm(from 109 to 113 mm) during the same period (T2 and T3)(Table 1 and Fig. 6), while the normal effective mandibularlength should increase by 6 mm (from 105 to 111 mm)during the same period.21
The effective mandibular length (Ar-Gn) increased by4 mm (from 109 to 113 mm) during OMA orthopedic therapy(T2) and orthodontic treatment with an active retainer ofvertical chin-cup (T3) at the same time during GH therapy,and then increased by 1 mm up to 114 mm during follow-upat 18 years of age (T4) (Table 1 and Fig. 6), while thenormal effective mandibular length for Taiwanese girlsshould increase by 6 mm (from 105 to 111 mm) and then by2 mm up to 113 mm at 18 years of age.21 Therefore, theeffective mandibular length diminished by 2 mmmainly dueto the effect of mandibular retraction of OMA orthopedictherapy and an active retainer of vertical chin-cup.
The OMA orthopedic appliance of maxillary protractioncombined with mandibular retraction is effective for cor-recting skeletal Class III malocclusion with midface
deficiency and mandibular prognathism in growing chil-dren.6,7 The OMA appliance corrected the mesial jaw(skeletal Class III) relationship and anterior crossbite(negative incisal overjet) of the girl undergoing GH therapy.After orthopedic treatment, a vertical chin-cup was used asan active retainer in the second stage of orthodontictreatment. At the end of the treatment, the patient of 15years was beyond the pubertal growth spurt, with onlyminor growth remaining.
GH therapy enhanced growth in both craniofacialcomplex and stature. The effective mandibular length andanterior face height values approached the norms at theend of the treatment. The increase did not result in a ClassIII skeletal or dental relationship, nor was the increaseworse for facial appearance.
The patient’s father and mother’s body heights are165 cm and 154 cm, respectively, and the achieved adultheight of the patient is 154 cm. However, the patient’selder brother’s height is 180 cm. Our case showed that GHtherapy is effective for improving the achieved adult heightof the patient with idiopathic short stature.
Acknowledgments
This work was supported by the Taiwan Association ofOrthodontists. The authors would like to thank Dr Yi-ChingPoon for her help with the preparation of the manuscript.

806 C.-Y. Pan et al.
References
1. Krysiak R, Gdula-Dymek A, Bednarska-Czerwi�nska A, Okpie�n B.Growth hormone therapy in children and adults. PharmacolRep 2007;59:500e16.
2. Shimon I. Growth hormone replacement for adult growthhormone deficiency. Expert Opin Pharmacother 2003;4:1977e83.
3. Poolee AE, Greene IM, Buschang PH. The effect of growthhormone therapy on longitudinal growth of the oral facialstructures in children. Prog Clin Biol Res 1982;101:499e516.
4. Cantu G, Buschang PH, Gonzalez JL. Differential growth andmaturation in idiopathic growth-hormone-deficient children.Eur J Orthod 1997;19:131e9.
5. Chen W, Tsai CY, Chen AC, Wu SF, Lin TW, Lin HC. Growthcharts of Taiwanese youth: norms based on health-relatedphysical fitness. Mid Taiwan J Med 2003;8(Suppl. 2):S85e93.
6. Chang HP, Lin HC, Liu PH, Chang CH. Geometric morphometricassessment of treatment effects of maxillary protractioncombined with chin cup appliance on the maxillofacialcomplex. J Oral Rehabil 2005;32:720e8.
7. Lin HC, Chang HP, Chang HF. Treatment effects of occipito-mental anchorage appliance of maxillary protraction combinedwith chincup traction in children with Class III malocclusion.J Formos Med Assoc 2007;106:380e91.
8. Chang HP. Orthodontic and orthopedic treatment of mandibularlateral displacement. J Taiwan Assoc Orthod 1995;7:19e24.
9. Pan JY, Chang HP. Orthodontic treatment of mandibularprognathism and lateral displacementda case report.J Taiwan Assoc Orthod 2007;19:56e63.
10. Spiegel RN, Sather AH, Hayles AB. Cephalometric study ofchildren with various endocrine diseases. Am J Orthod 1971;59:362e75.
11. Kjellberg H, Beiring M, Wikland KA. Craniofacial morphology,dental occlusion, tooth eruption, and dental maturity in boys
of short stature with or without growth hormone deficiency.Eur J Oral Sci 2000;108:359e67.
12. Kjellberg H, Wikland KA. A longitudinal study of craniofacialmorphology in idiopathic short stature and growth hormone-deficient boys treated with growth hormone. Eur J Orthod2007;29:243e50.
13. Chang HP, Tseng YC, Chang HF. Treatment of mandibularprognathism. J Formos Med Assoc 2006;105:781e90.
14. Chou ST, Tseng YC, Pan JY, Chang JZ, Chang HP. Craniofacialskeletal dysplasia of opposite-sex dizygotic twins. J FormosMed Assoc 2011;110:342e6.
15. Yamaguchi T, Maki K, Shibasaki Y. Growth hormone receptorgene variant and mandibular height in the normal Japanesepopulation. Am J Orthod Dentofacial Orthop 2001;119:650e3.
16. Zhou J, Lu Y, Gao XH, Chen YC, Lu JJ, Bai YX, et al. The growthhormone receptor gene is associated with mandibular height ina Chinese population. J Dent Res 2005;84:1052e6.
17. Kang EH, Yamaguchi T, Tajima A, Nakajima T, Tomoyusu Y,Watanabe M, et al. Association of the growth hormonereceptor gene polymorphisms with mandibular height ina Korean population. Arch Oral Biol 2009;54:556e62.
18. Tomoyasu Y, Yamaguchi T, Tajima A, Nakajima T, Inoue I,Maki K. Further evidence for an association between mandib-ular height and the growth hormone receptor gene in a Japa-nese population. Am J Orthod Dentofacial Orthop 2009;136:536e41.
19. Pirinen S. Endocrine regulation of craniofacial growth. ActaOdontol Scand 1995;53:179e85.
20. van Erum R, Mulier M, Carels C, Verbeke G, de Zegher F.Craniofacial growth in short children born small for gestationalage: effect of growth hormone treatment. J Dent Res 1997;76:1576e86.
21. Fan YC. A study of radiographic cephalometric analysis andTaiwanese standards. Thesis, Graduate Institute of Dentistry,National Taiwan University, 1995.