oregon health policy board agenda 3... · • the health plan quality metrics committee was...
TRANSCRIPT

Conference Call Number: 1-888-808-6929 Public Participant Code: 915042#
Oregon Health Policy Board AGENDA
October 3, 2017 OHSU Center for Health & Healing
3303 SW Bond Ave, 3rd floor Rm. #4 8:30 a.m. to 12:00 p.m.
# Time Item Presenter Purpose
Old
Bu
siness
1 8:30 Welcome, Minutes Approval, Calendar Review
Zeke Smith, Chair Action
2 8:40 OHA Report Pat Allen Executive Director, OHA
Update &
Informational
3 8:50 Committee Liaison & Consult Updates
Board Members Update &
Informational
4 9:10 Health Plan Quality Metrics Workplan Update
Kristen Dillon, M.D. Director Columbia Gorge CCO & Committee Chair Shaun Parkman OHA, Committee Vice-Chair
Update & Potential Vote
5 9:55 Public Testimony Chair Smith Public
Testimony
6 10:05 Break
New
Bu
siness
7 10:20 Behavioral Health Collaborative Status & Update
Royce Bowlin, OHA Behavioral Health Policy Director Mark Bradshaw CEO, AllCare
Discussion & Informational
8 11:20 CCO 2.0
Pat Allen Executive Director, OHA Jeremy Vandehey OHA Interim Health Policy & Analytics Division Director
Update & Informational
9 12:00 Adjourn Chair Smith

Conference Call Number: 1-888-808-6929 Public Participant Code: 915042#
Next meeting: November 7, 2017 Astoria City Hall 1095 Duane Street Astoria, OR 97103 8:30 a.m. to 2:00 p.m.
Everyone is welcome to the Oregon Health Policy Board meetings. For questions about accessibility or to request an accommodation, please call 541-999-6983 or write [email protected]. Requests should be made at least 48 hours prior to the event. Documents can be provided upon request in an alternate format for individuals with disabilities or in a language other than English for people with limited English skills. To request a document in another format or language please call 541-999-6983 or write to [email protected]

Oregon Health Policy Board DRAFT September 12, 2017
OHSU Center for Health & Healing 3303 SW Bond Ave, 3rd floor Rm. #4
8:30 a.m. to 12:00 p.m.
Item
OHPB video and audio recording
To view the video, or listen to the audio link, of the OHPB meeting in its entirety click here. Agenda items can be reviewed at time stamp listed in the column below.
Welcome and Call To Order, Chair Zeke Smith
Present:
Board members present: Chair Zeke Smith, Vice-Chair Carla McKelvey, Brenda Johnson, Felisa Hagins, John Santa, Oscar Arana
The Board voted to approve the August minutes.
Acting Director’s Report, Patrick Allen, OHA
Patrick Allen introduced himself to the Board in his role as acting Director for the agency. Director Allen previously served as the Director of the Department of Consumer and Business Services. He also introduced the new staff at OHA:
Jeremy Vandehey – Health Policy & Analytics Interim Director Dawn Jagger – Administrator of External Relations Laura Robison – Chief Financial Officer Chris Kutz - Chief Operating Officer Director Allen spoke about the direction of the agency and the need for continuing the work that is ongoing.
00:08:45
OHPB Committee Liaison Update
Each OHPB member who serves as a liaison or consultant gave a brief update on their respective OHPB committee, collaborative or workgroup.
Carla McKelvey gave an update on the primary care payment reform collaborative. A subcommittee has convened to work on the clinic case studies, which will provide insight into best practices on health care innovation, care improvement and payment reform.
Carla McKelvey also gave an update on the Health Care workforce committee, which is in the midst of overseeing implementation of HB 3261. A major focus area of this work includes a statewide workforce needs assessment.
00:15:02

Oregon Health Policy Board DRAFT September 12, 2017
OHSU Center for Health & Healing 3303 SW Bond Ave, 3rd floor Rm. #4
8:30 a.m. to 12:00 p.m.
John Santa gave update on the Health Plan Quality Metrics Committee. The committee continues to review and deliberate candidate measures for an aligned statewide quality measures set and thus far has focused on measures of prevention/early detection
Brenda Johnson gave an update on the Behavioral Health Collaborative. Five specific workgroups (governance and finance; standards of care and competencies; workforce; peer-delivered services; health information technology) have continued the work of the BHC to develop more in-depth implementation plans and recommendations.
OHPB Committee Planning, Jeff Scroggin, OHA, Trevor Douglass, OHA, Leann Johnson, OHA Trevor Douglass gave a presentation on the various efforts at OHA related to pharmacy issues. The Board requested that OHA staff return to the next meeting with more clarity on the interventions and recommendations to move the state more aggressively forward to address the issue of high-cost drugs. Oscar Arana provided a Health Equity Committee update. There was a substantial pool of applicants for the Health Equity Committee, and he shared their proposed membership with the OHPB for review and approval. Board accepted slate for Health Equity Committee as presented.
00:38:23
Health Information Technology Committee (HITOC) Update & Recommendations, Susan Otter, OHA, Erick Doolen, HITOC, Amy Henniger, HITOC, Grag Van Pelt, Oregon Health Leadership Counsel
The panel provided an update on HITOC, shared the work completed over the past year and presented their strategic plan for review by the OHPB.
The Board voted to accept the plan and recommendations with three additions:
1. More information on patient access and engagement, and any progress made in these areas
2. Addressing the role of HIT in health equity
1:36:30

Oregon Health Policy Board DRAFT September 12, 2017
OHSU Center for Health & Healing 3303 SW Bond Ave, 3rd floor Rm. #4
8:30 a.m. to 12:00 p.m.
Next meeting: October 3, 2017 OHSU Center for Health & Healing 3303 SW Bond Ave, 3rd floor Rm. #4 8:30 a.m. to 12:00 p.m.
3. Describing the role of HIT in overall efforts to contain costs and provide better value.
All members were in favor.
CCO 2.0 Planning & Discussion, Patrick Allen, OHA, Jeremy Vandehey, OHA
Pat and Jeremy shared information about the CCO 2.0 conversations. OHA is considering whether the CCO contracts should be extended a year, in order to provide more time for the development of the new CCO five-year contracts. Another topic of consideration is whether the process will utilize an RFA (Request for Application; non-competitive) or RFP (Request for Proposal; competitive) during procurement.
The OHPB asked for further information and decisions on timelines by the next meeting.
03:03:48
Public Testimony
Jim Slater from Care Oregon
John Mullen from Oregon Law Center
1:26:40
Adjourn

Health Plan Quality Metrics Committee
Progress Report to the Oregon Health Policy Board
KRISTEN DILLON, M.D. , CHAIR SHAUN PARKMAN, VICE CHAIR
O C T O B E R 3 , 2 0 1 7
1

Overview
• Committee Charge and Impact
• Committee Membership, Mission & Vision
• Approach – Near Term and Longer Term
• Work Plan (Board approval requested)
2

Committee Charge• The Health Plan Quality Metrics Committee was established by Senate Bill 440
(2015) as the single body to align and specify the quality measures that may be used by the state in health plan purchasing:
• Coordinated care organizations for Medicaid • The Oregon Health Insurance Marketplace (the health insurance exchange)• The Oregon Educators Benefit Board (OEBB)• The Public Employees’ Benefit Board (PEBB)
3

OREGON HEALTH POLICY BOARD
4

ImpactQuality measures adopted by the HPQMC will impact care delivered to nearly 1.5 million Oregonians
Nearly $180 million are allocated for CCO quality measure inventive payments. This amount will increase as other state programs, such as PEBB and OEBB, begin to incorporate greater dollars at risk tied to quality measure performance in their contracts
5
Coordinated Care Organizations almost 1.0 million
Public Employees Benefit Board (PEBB) 139,000
Oregon Educators Benefit Board (OEBB) 153,000
Oregon Health Insurance Marketplace (Exchange plans) 155,000

Committee Charge• SB 440 specifies that the committee prioritize:
• Measures adopted by other state or national organizations• Measures that rely on existing data systems, and• Measures that can be reported in a timely manner
• The committee articulated additional criteria to guide its work, including that the aligned measures set:
• Represent the array of services that affect health• Represent the diversity of patients enrolled in the health plans• Be collectively parsimonious (set is limited in number of measures) • Include measures with transformative potential
6

Committee Charge• Issues of concern for committee members that were not included in the
charge from SB 440:• Reducing redundancy and subtle differences among quality metrics in use• Decreasing reporting burden for health care providers • Remedying the lack of metrics that address areas such as health equity, social determinants
of health, and health outcomes• Recognition that most validated measures focus on health care processes and may not drive
health outcomes or system transformation.
7

Committee MembershipSB 440 defines fifteen committee seats, with committee members appointed by the Governor:
◦ Oregon Health Authority (OHA, 1 seat)◦ Oregon Educators Benefit Board (OEBB, 1 seat)◦ Public Employees’ Benefit Board (PEBB, 1 seat)◦ Department of Consumer and Business Services (DCBS, 1 seat)◦ Health care providers (2 seats) ◦ Hospitals (1 seat) ◦ Insurers, large employers, or multiple employer welfare arrangements (1 seat)◦ Health care consumers (2 seats)◦ Coordinated care organizations (2 seats)◦ Health care research expert (1 seat)◦ Health care quality measurement expert (1 seat)◦ Mental health and addiction services expert (1 seat)
8

Committee Vision & MissionThe committee created and adopted the following to guide their work.
Vision
Aligned measurement to promote optimum health and wellbeing for all Oregonians.
Mission
Improving physical, behavioral and dental health for individuals and communities through meaningful and timely quality measures to guide health care purchasing and value.
9

Approach – Near Term• Assess current national and state quality measures to identify measures that are
validated, benchmarked, and present opportunity for improvement in Oregon.
• Prioritize measures already in use in Oregon
• Leverage existing work and partnerships, including:• CCO Metrics & Scoring Committee• Public Health Advisory Board• Hospital Performance Metrics Advisory Committee• Medicaid Advisory Committee Oral Health Workgroup • Behavioral Health Collaborative Data Workgroup
• Seek recommendations where other committees and workgroups have identified or developed measures related to social determinants, equity, and health outcomes
10

Approach – Near Term• Release a draft aligned measures set in early 2018
• Seek comment to inform efforts to refine the draft set
• Complete a final initial aligned measures set during Spring 2018
• Potentially release measures set as a work in progress or partial set, with the committee continuing to work on areas where the set is incomplete
• Establish an ongoing process for refining and maintaining the statewide aligned measures set
11

Approach – Longer Term• Address the tension created because current measures do not sufficiently
address critical aspects of health:• Social determinants• Equity & disparities• Outcomes• Other historically neglected areas of quality measurement, including specialty care,
behavioral health, dental health
• Establish an ongoing process to refine the measure set, with the intention of shifting toward adoption of more transformational measures
12

Approach – Longer Term• Progress toward truly transformational measures will require work to mitigate
a variety of challenges• Using novel data sources, including sources that exist outside the health care system • Data capture challenges (demographic data, health outcomes)• Statistical unreliability related to small population sizes, including for measures that focus
on disparities in specific subpopulations
• The committee expects to leverage partnerships and may charter workgroups to support this work
• Endorsed the creation of a workgroup, supported by the Children’s Initiative, to explore options for a measure of kindergarten readiness
• Maintaining close communication with Metrics and Scoring Committee
13

Draft Work PlanMonth ActivitiesOctober 2017 Continue review of candidate measures identified through assessment of existing state and national measure sets
Recommendations from the Hospital Performance Metrics Advisory Committee
November 2017 Continue review of candidate measures identified through assessment of existing state and national measure sets
Recommendations from Metrics & Scoring
Recommendations from Public Health Advisory Board
December 2017 Complete review of candidate measures and assess initial draft measure set in full
• Verify alignment with committee’s criteria
• Identify gaps/areas with insufficient measures for further research
• Discuss committee policy with regard to measure technical specifications
Dental health recommendations (State Dental Director, input from Medicaid Advisory Committee Oral Health Workgroup)
January 2018 Status report from Kindergarten Readiness Workgroup
Recommendations from the Behavioral Health Collaborative Data workgroup
Finalize and release draft version of initial measures set for stakeholder review and commentFebruary 2018 Review and consider stakeholder comment, refine draft measure setMarch 2018 Review and consider stakeholder comment, refine draft measure setApril 2018 Finalize initial measures set
Define process and timing for ongoing annual refinement and maintenance of measure set
14

Question
What is the Board’s guidance for the committee’s near term and longer term work to establish an aligned statewide measure set?
15

ContactMargaret Smith-Isa, MPP
Program Coordinator, PEBB and Staff to Health Plan Quality Metrics Committee
(503) 378-3958
The Health Plan Quality Metrics Committee meets the second Thursday of each month. Meeting agendas, materials, minutes and recordings can be found on the committee website:
http://www.oregon.gov/oha/HPA/ANALYTICS/Pages/Quality-Metrics-Committee.aspx
16

Health Plan Quality Metrics Committee Membership October 3, 2017
Name Title Organizational Affiliation Location by
County Maggie Bennington-Davis Chief Medical Officer Health Share of Oregon Multnomah Description/Background: Maggie currently serves as the Chief Medical Officer with Health Share of Oregon. Maggie has served on the CCO Metrics and Scoring Committee as both a member and the Chair of the committee. Kristen Dillon Director PacificSource Columbia Gorge CCO Hood River Description/Background: Kristen currently serves as the Director of the Columbia Gorge CCO, employed by PacificSource Community Solutions since 2015. Prior to that, Kristen was an owner of an independent primary care practice in Hood River where she worked as a family physician for 15 years. Kristen continues to work in a limited capacity at the frontier clinic in Sherman County. Benjamin LeBlanc Chief Medical Officer Providence Medical Group Multnomah Description/Background: Benjamin currently serves as physician and Chief Medical Office for Providence Medical Group in Oregon. Benjamin has been with Providence for 18 years in various roles, including faculty for residency training, electronic health record and software design consultant for quality improvement, and physician manager responsible for achieving quality outcomes. Additionally, Benjamin works with government and private payers to design and implement pay for performance programs and develop reimbursement strategies focused on improved outcomes. Lynnea Lindsey Director of Behavioral Health Services Legacy Health Multnomah Description/Background: Dr. Lindsey currently serves as the Director of Behavioral Health Services for Legacy Health. Lynnea is a licensed psychologist with two decades of experience working in Oregon healthcare at both a clinical and operational/administrative level. Lynnea has worked as a consultant to several CCOs and health plans as well as provider organizations in Oregon to develop programs to clinically and financially support as well as evaluate the work of integrated physical and behavioral health services. Lynnea has worked with a variety of state committees as well. Lynnea is currently the chair of the Integrated Behavioral Health Alliance of Oregon (IBHAO) and board member of CCO Oregon. Jeff Luck Associate Professor Oregon State University Benton Description/Background: Jeff Luck, MBA, PhD is Associate Professor of Health Management and Policy at Oregon State University’s College of Public Health and Human Sciences. He is Chair of the Oregon Public Health Advisory Board and a past member of the OHA Metrics and Scoring Committee. Melinda Muller Clinical Vice President for Care Transformation Legacy Health Multnomah Description/Background: Melinda currently serves as the Clinical Vice President for Care Transformation at Legacy Health. Melinda has been a primary care physician in Oregon for 20 years. Melinda has 10 years of experience measuring and demonstrating improvement with HEDIS, STARS and other internal measures within primary care. Melinda led the transformation of the primary care clinics to become medical homes, certified by Oregon as well as NCQA.
1

Health Plan Quality Metrics Committee Membership October 3, 2017
Raj Mummadi Chief of Quality for Ambulatory Care and Population Health Kaiser Permanente Northwest Region Multnomah Description/Background: Raj currently serves as the Chief of Quality for Ambulatory Care and Population Health at Kaiser Permanente Northwest Region. Raj is also a clinical gastroenterologist in practice for over 10 years. Prior to joining Kaiser Permanente, Raj was a teaching faculty at OHSU. Raj has graduate level training in outcomes research, epidemiology and biostatistics as part of his graduate degree in clinical investigation. Ana Quiñones Assistant Professor OHSU-PSU School of Public Health Multnomah Description/Background: Ana currently serves as an Associate Professor in the Department of Family Medicine at OHSU with a secondary appointment in the OHSU-PSU School of Public Health. Ana is also an affiliate investigator for the Portland Veterans Affairs Health Care System. Bhavesh Rajani Medical Director Yamhill CCO Yamhill Description/Background: Bhavesh currently serves as the Medical Director for Yamhill CCO. Previously, Bhavesh was in a leadership role at Providence Medical Group. With a background in family practice, Bhavesh has a strong knowledge basis on the impact of metrics determination on primary care related work. Colleen Reuland Director Oregon Pediatric Improvement Partnership
(OPIP) Multnomah
Description/Background: Colleen currently serves as the Director of OPIP as well as an instructor in the pediatrics department at OHSU. Colleen has spent her 19 year career focused on applied quality measurement and improvement activities. Colleen has lead the development and implementation of a number of standardized metrics that have been implemented at the state, health plan, provider and community-level and have been endorsed by the National Quality Form Forum and National Quality Measures Clearing house. Colleen brings experience having served on and observed several state committees in the past including the Primary Care Payment Reform Collaborative and the Measuring Success Work Group. Hannah Rosenau Program Director Oregon Foundation for Reproductive Health Multnomah Description/Background: Hannah currently serves as the Program Director for the Oregon Foundation for Reproductive Health/NARAL Pro-Choice Oregon. Hannah’s passion is for social justice and women’s health brought her work at OFRH to improve health care delivery systems in the state. Through her work at OFRH Hannah has been part of the One Key Question® initiative which has been a flagship program to improve preventive reproductive health care through pregnancy intention screening. Chiqui Flowers Administrator DCBS Oregon Health Insurance Marketplace Marion Description/Background: Chiqui currently serves as the Administrator of the Oregon Health Insurance Marketplace. Chiqui joined Oregon’s Marketplace in 2013 and has been a part of implementing every open enrollment effort since the first year. Chiqui was also instrumental in designing, implementing and operating the Oregon program that facilitates Medicaid-equivalent coverage for low-income COFA islanders. Jon Collins OHA Representative (Interim) Oregon Health Authority Marion
2

Health Plan Quality Metrics Committee Membership October 3, 2017
Description/Background: Jon Collins currently serves as the Director of Health Analytics for the Oregon Health Authority. Jon has been a part of OHA in various roles of leadership associated with the government healthcare field for the past 17 years. Prior to joining OHA, Jon served as the quality improvement manager for a rural managed care company contracted for Medicaid behavioral health services in Oregon. Jon is an accomplished researcher and maintains an adjunct appointment with OHSU’s psychiatry department. Shaun Parkman Vice-Chair PEBB Multnomah Description/Background: Shaun serves as an evaluation specialist in the Oregon Public Health Division and is a member of the Service Employees International Union (SEIU), Local 503. Shaun also currently serves as Vice-Chair of the Public Employees’ Benefit Board (PEBB) and have served on the Board since 2015. Shaun is a Southern/Midwest transplant and have loved living in Portland since 2010. Shaun stays active by hiking with his wife and daughter. Tom Syltebo Member OEBB Multnomah Description/Background: Tom is a retired physician who has worked in Oregon healthcare as a primary care physician, hospital chief of staff, operations medical director, and medical group liaison. He represented Kaiser Permanente before the OEBB Board for five years as KP Northwest Region's Clinical Quality Representative, and continues to participate with Oregon Health Care Quality Corporation/Healthinsight Oregon, an organization dedicated to providing comprehensive, actionable, statewide medical information to all stakeholders.
Demographic Information
15 Total
Gender: 8 female; 7 male Race: Asian/Pacific Islander (2); Latina/Hispanic (1); White (12) Ethnicity: Hispanic (1); Non-Hispanic (14) Geography: Multnomah County (10); Hood River (1); Benton (1); Yamhill (1); Marion (2) Disability: Disability (0)
3

Oregon’s Behavioral Health System:An Action Plan for the
21st Century Royce Bowlin, OHA, Behavioral Health Director
Mark Bradshaw, AllCare
October 3, 2017

BehavioralHealth Collaborative (BHC)
What will be covered?
1.Behavioral Health Collaborative (BHC) Overview 2.Accountability Structure3.BHC Work Group Deliverables & Status Update4.Timeline & Communication Plan5.Questions
2
BEHAVIORAL HEALTH POLICY Health Policy and Analytics

Oregon’s Current Behavioral Health Status
3
36% of teenagers
perceive no risk from smoking a
pack of cigarettes a day
14.6%Of teenagers experienced a
major depressive
episode in the last year
Suicide is the
2nd leading cause of death
for young adults in Oregon
4.5% of adults had
serious thoughts of suicide last
yearOregon ranks
4thnationally in opioid use
Illicit drug use among
teenagers is
2.5% higher than national
average
Binge drinking among
teenagers is
2.5% higher than
national average
35.8% of teenagers
perceive no risk from smoking a
pack of cigarettes a day
Only 46% of adults who
receive mental health help, say
it helps
7%Of Oregonians
over 12 experience
alcohol dependence or
abuse
11% of Oregonians
dependent on illicit drugs
receive treatment
Only 45%of youth who had a major depressive
episode receive treatment
Oregon is
ranked 14thnationally in
youth suicide

4
Going forward: A behavioral health systemthat works for all OregoniansPriorities• Improve behavioral health outcomes
for consumers• Improve equitable access to effective
services in every part of the state• Improve efficiency and cost-effectiveness
in services• No wrong door approach• Mental health and substance services are
seamlessly tied to all aspects of care• Focus on prevention and health promotion• System-wide accountability for
improved outcomes

BHC Recommendations OverviewRecommendations will transform behavioral health system so that all Oregonians (both Medicaid and non-Medicaid) will be served by a coordinated care model for behavioral health needs.
5
• Focused on person and family• Fully integrated behavioral health
with physical and oral health• Build on existing efforts and
complement, not duplicate• Reduce administrative burden and
system complexity• Shared financial risk • Outcomes that are measurable and
sustainable
6
BEHAVIORAL HEALTH POLICY Health Policy and Analytics

BHC RecommendationsRecommendations will transform behavioral health system so that all Oregonians (both Medicaid and non-Medicaid) will be served by a coordinated care model for behavioral health needs.
7
1. Governance and Finance: Regional governance model for behavioral health
2. Standards of Care and Competencies
3. Workforce4. Information Exchange and
Coordination of Care
BEHAVIORAL HEALTH POLICY Health Policy and Analytics

BHC Work Group Deliverables & Status
Updates
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
8

Governance and Finance Work GroupDeliverables: (Completed 8/31/17)• Define Single Point of Shared Accountability and define elements of
Single Plan of Shared Accountability
(To be completed Sept/Oct 2017)• Identify incentives Risk / Benefit sharing• Ensure alignment of contracts
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
9

Governance and Finance Work GroupUpdate
Four phased approach to development and implementation of the regional behavioral health Single Point of Shared Accountability (SPOSA):
Phase 1: Letter of Intent (LOI)
Phase 2: Community-based priorities and rationale
Phase 3: Action Plan
Phase 4: Performance and Reporting
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
10
Standards of Care and Competencies Work Group
Deliverables: (Completed 8/31/17)• Established core competencies for providers
(To be completed Sept/Oct 2017)• Established minimum standards of care, stateside standards for
assessment, placement and billing criteria. • Established minimum standards for care coordination and payment
mechanisms are in place for care coordination to meet the minimum standards.
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
11

Standards of Care and Competencies Work Group Update• Core competencies for providers
• Endorsed existing standards from the Substance Abuse and Mental Health Services Administration (SAMHSA) and the University of Colorado Eugene Farley Center.
• Minimum Standards of Care• Statewide standards for assessment, placement and billing criteria.
• Care Coordination • Establish minimum standards for care coordination. • Ensure payment mechanism is in place for care coordination to meet the
minimum standard, including travel time.
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
12
Workforce Work Group
Deliverables: (Completed 8/31/17)• Recommend recruitment and retention strategies.
(To be completed Sept/Oct 2017)• Recommend standards for a well-trained behavioral health
workforce, inclusive of certified, licensed and unlicensed, peer support specialists and community health workers throughout the state.
13
BEHAVIORAL HEALTH POLICY Health Policy and Analytics

Workforce Work Group Update
• Workforce assessment– Farley Center
• Retention and recruitment– Loan repayment programs– Outreach efforts– Trainings
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
14

Peer Delivered Services Work GroupDeliverables: Completed 8/31/17• Establish system standards and expectations for Peer Delivered
Services (PDS) workforce.• Establish the certification/licensure program for becoming a PDS
supervisor.• Minimum standards and ongoing training requirements for peer
support specialist competence and training.• Monitor for effective and appropriate use of employing peer
services.• Research methodologies to establish target ratio of PDS to
members.– PDS Core Team will be submitting recommendations on target
ratio of peer support specialist to member based on setting.
15
BEHAVIORAL HEALTH POLICY Health Policy and Analytics

Peer Delivered Services Work Group Update• System Standards
• Standardized Training Model
• Supervision
(Enter) DEPARTMENT (ALL CAPS)(Enter) Division or Office (Mixed Case)
16

Health Information Technology Workgroup
Deliverables: • Advance the implementation of technology to further care
coordination across the state and behavioral health system.
• Identify ways for the state and regional collaborations to support the continued adoption and utilization of electronic health records and information sharing across payers and platforms.
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
17

Health Information Technology Update
• Completed environmental scan of Health Information Technology (HIT) use by behavioral health agencies– Preliminary results– Key informant interviews underway
• In December, the Health Information Technology Oversight Committee will review report on behavioral health and HIT– Identify gaps and opportunities– Additional recommendations for supporting behavioral health
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
18

Commercial Health Plans
Deliverables: • Work plan will be developed upon completion of Parity Policy
Academy.• Will include technical assistance from OHA’s Transformation
Center to educate providers about parity.
• OHA will work with Department of Consumer and Business Services and commercial payers to identify the states collective authority to integrate commercial and publicly insured behavioral health efforts to produce results, efficiencies and parity compliance.
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
19

Data Work Group
Deliverables:Work to begin October 2017 • Develop an outcomes-focused, person-centered behavioral health
measurement framework to assess the impact of integrated services.
• Align outcomes measurement with identified standards for behavioral health.
• OHA will work with its current systems to coordinate information and track progress and outcomes across the state.
• Work group will submit recommendations to the Health Plan Quality Metrics Committee for metrics to hold the CCOs accountable.
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
20

Transformation Center
• Series of webinars– Data sharing– Organizing local structures around shared outcomes– Blended funding models– Using data to improve services– Ensuring equity and transparency within the governance model
• Learning Collaborative– One day event– Hiring, retaining and using peer delivered services
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
21

BHC Timeline
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
22

Implementation Timeline
23

Phase Four
• OHA Core Team
• Contract changes for CMHPs and CCOs
• Oregon Administrative Rule changes
BEHAVIORAL HEALTH POLICY Health Policy and Analytics
24

Questions?
Draft 9/28/17
Draft Discussion Document for CCO Contracting
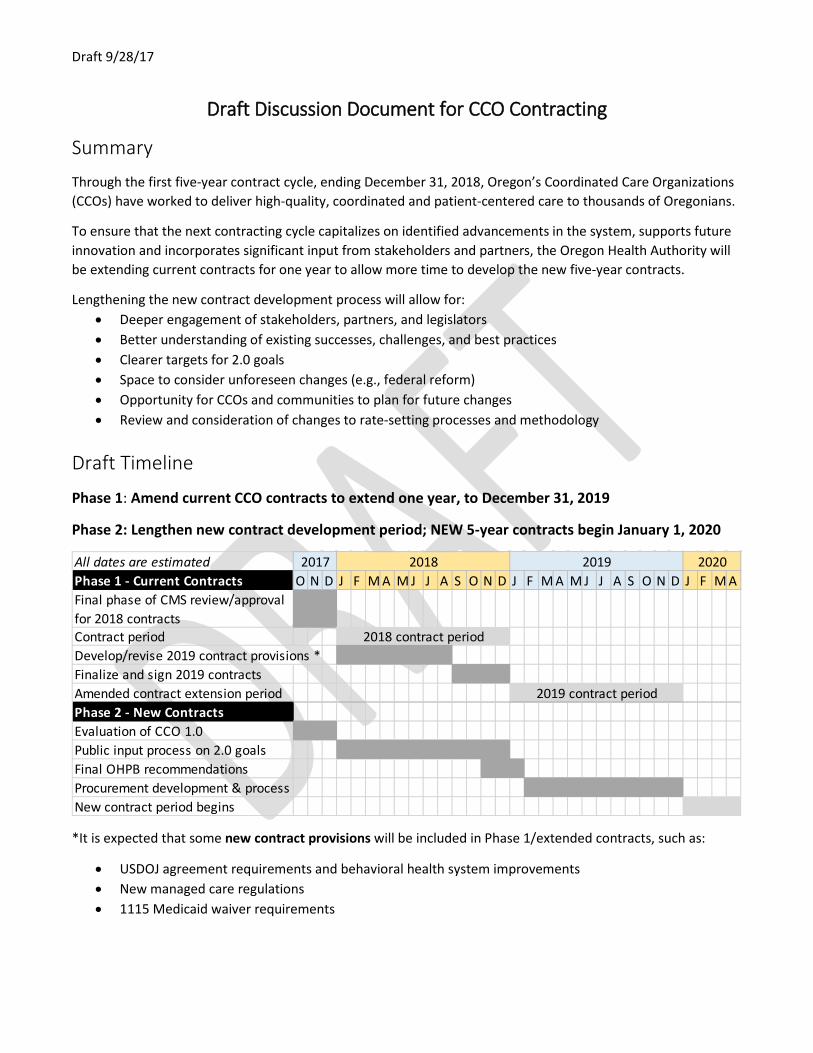
Summary
Through the first five-year contract cycle, ending December 31, 2018, Oregon’s Coordinated Care Organizations (CCOs) have worked to deliver high-quality, coordinated and patient-centered care to thousands of Oregonians.
To ensure that the next contracting cycle capitalizes on identified advancements in the system, supports future innovation and incorporates significant input from stakeholders and partners, the Oregon Health Authority will be extending current contracts for one year to allow more time to develop the new five-year contracts.
Lengthening the new contract development process will allow for: • Deeper engagement of stakeholders, partners, and legislators • Better understanding of existing successes, challenges, and best practices • Clearer targets for 2.0 goals • Space to consider unforeseen changes (e.g., federal reform) • Opportunity for CCOs and communities to plan for future changes • Review and consideration of changes to rate-setting processes and methodology
Draft Timeline
Phase 1: Amend current CCO contracts to extend one year, to December 31, 2019
Phase 2: Lengthen new contract development period; NEW 5-year contracts begin January 1, 2020
*It is expected that some new contract provisions will be included in Phase 1/extended contracts, such as:
• USDOJ agreement requirements and behavioral health system improvements • New managed care regulations • 1115 Medicaid waiver requirements
All dates are estimatedPhase 1 - Current Contracts O N D J F M A M J J A S O N D J F M A M J J A S O N D J F M AFinal phase of CMS review/approval for 2018 contractsContract periodDevelop/revise 2019 contract provisions *Finalize and sign 2019 contractsAmended contract extension periodPhase 2 - New ContractsEvaluation of CCO 1.0Public input process on 2.0 goalsFinal OHPB recommendationsProcurement development & processNew contract period begins
2017 2018 2019
2018 contract period
2019 contract period
2020

Draft 9/28/17
Policy recommendation areas identified for further development
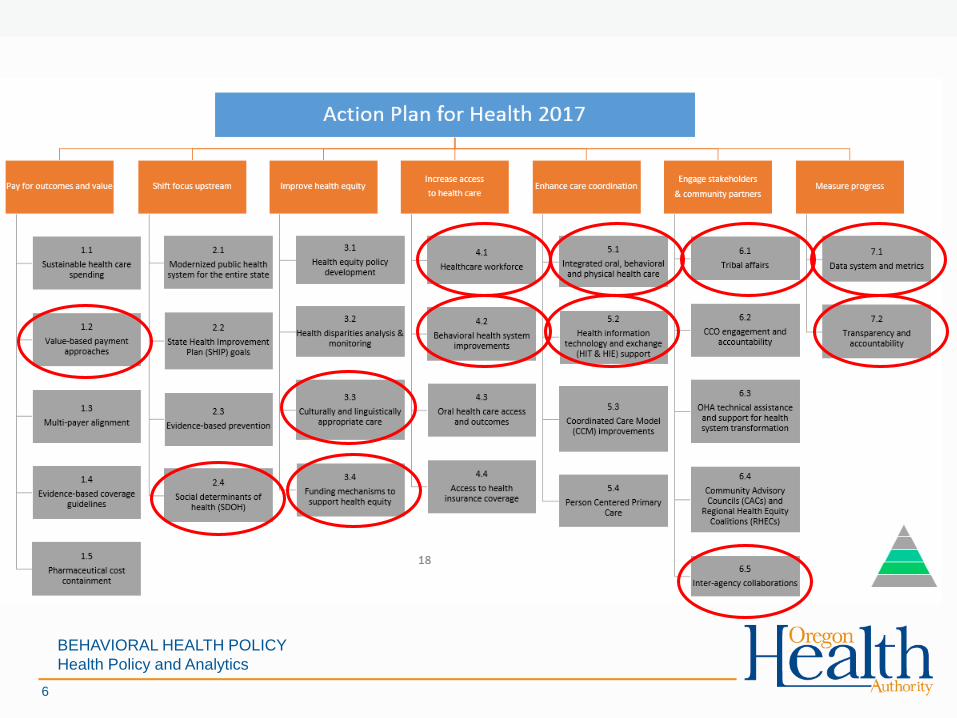
Oregon’s CCOs have demonstrated their commitment to innovation, community, and health care quality, and the next round of contracts offers an opportunity to build on those efforts and drive Oregon further in health system transformation and innovation. The Oregon Health Policy Board has recommended developing the following policy areas, in alignment with the foundational strategies from the 2017-2019 Action Plan for Health in order to inform the future direction of coordinated care in Oregon:
Pay for outcomes and value
• Maintain focus on achieving a sustainable rate of growth • Implement recommendations from the value-based payment roadmap (expected April 2018) • Address high-cost drugs • Align policy goals with financial incentives
Shift focus upstream
• Set standards for investment and reporting of health-related services • Further identify opportunities for CCOs to impact the social determinants of health • Partner with public health and community based organizations
Improve health equity
• Improve data collection and transparency of data, especially related to health disparities • Focus on member experience, measurement, reporting and outcomes for people of color, children and
specific populations
Increase access to care
• Continue to invest in prevention and primary care efforts, including PCPCHs • Improve workforce training, diversity, and retention, especially in underserved and rural communities • Identify and remove barriers for Traditional Health Worker utilization • Improve the behavioral health care system
Enhance care coordination
• Accelerate integration of physical health care, behavioral health care, and oral health care • Ensure CCOs are utilizing and exchanging health information technology in ways that improve care • Improve collaboration between CCOs and other partners in the system of care (e.g., long-term services
and supports, early learning hubs, corrections, schools, etc.)
Engage stakeholders & community partners
• Allow space for locally-driven flexibility and decision-making • Improve community access and input through enhanced transparency and accountability • Strengthen partnerships between CCOs and Community Advisory Councils (CACs)
Measure progress
• Align, report and monitor health outcome and quality measures • Standardize fiscal reporting and set expectations for percentage of investment of profit margins