orders management project (omp): …ioe481/ioe481_past_reports/f0506.pdfrecommendations for...
TRANSCRIPT

Orders Management Project (OMP):
Recommendations for Implementing Computer Workstations atUniversity of Michigan Hospital and C.S. Mott Children’s Hospital
Final Report
December 15, 2005
Client:Karen McConnell, Business Analyst, OMP Deployment Team
Mary Filipek, Project Manager, OMP Deployment Team
Coordinator:Mary Duck, Senior Management Consultant
Programs & Operations Analysis
Prepared by:
L’Rai Arthur MensahJonathan GarrettVanessa HudsonVeronica Lucas

Table of Contents
Executive Summary .3
Introduction 6
Goals and Objectives 6
Background 6
Project Scope 7
Approach & Methodology 7
Findings 8
Supplemental Information on CPOE Systems 8
Variation in Physician Workflow 9
Consideration of Home and Overflow Services 10
Alternatives Considered 12
Final Recommendation 13
Action Plan 14
Appendices
A: Screenshot of Sunrise Clinical Manager software 15
B: Acute Care Units within Scope 16
C: CPOE at St. Joseph Mercy, Ann Arbor, MI 17
D: Computerized Physician Order Entry Research 18
E: Mobile Computing Options for Implementing of CPOE 20
F: Observations During Rounds 21
G: Cost Analysis 22
2

Executive Summary
The University of Michigan Hospitals use a paper system for organizing patient information andphysician orders, but will be transitioning to a computerized physician order entry (CPOE)system in the near future. The Orders Management Project (OMP) will be implementingsoftware that will assist hospital staff in managing medication orders electronically in order toimprove the quality and safety of patient care. The CPOE system, Eclipsys’ Sunrise ClinicalManager XA, will allow caregivers to electronically order tests, procedures, and medications.Physicians may also receive decision support information about drug interactions and patientallergies. This system will be available beginning in March 2006.
The OMP team has given our student team the task of providing recommendations for thenumber and type of computer workstations on 21 units in the University Hospital and C.S. MottChildren’s Hospital that will facilitate this transition for physicians. Using qualitative andquantitative data from current rounding practices, a detailed analysis with a proposal for thefuture system has been compiled.
Findings
The OMP student team interviewed nurse managers from each unit to determine peak workflowtimes and observed current order entry processes by shadowing physicians during these times.We also gathered supplemental information on CPOE systems and devices. Our findings aresummarized below.
Supplemental mn/àrmation on CPOE Systems• Saint Joseph Mercy Flospital’s CPOE system has been in place for ten years. XyLoc
cards are used to maintain HIPAA security requirements by allowing physicians towirelessly authenticate.
• Hospitals wishing to implement a successful CPOE system must consider existing orderwriting practices in order to facilitate a smooth transition for medical staff.
• Personal digital assistants, computers on wheels, fixed computers, and tablet PCs arecurrently the common devices used by healthcare systems for the CPOE software.Computers on wheels are perceived to be the most practical device because of mobilityand full screen size.
Variation in Physician Workjlow• Rounding practices vary based on the type of service.• Medicine units round between 8 am. and 11 am., typically without charts.• Surgery units round with their charts, between 6 a.m. and 8 am.
Consideration ofHome and Overflow Services• All hospital units have home services, with additional beds available for overflow from
other units.• Physicians need to have access to the CPOE system on multiple floors.
3
Alternatives Considered
After examining our data and observations, the team developed three possible solutions fordetermining the number of computers needed for physicians on each unit.
L Determine the number of computers needed based on the maximum number of teamsthat could be on the unit at any given time.
2. Provide the same amount of computers on each floor in similar locations. The numberwould be based on whether the unit was a medicine, surgical, or pediatric unit.
3. Determine the number of computers needed based on the number of home services onthe unit. These computers would then be supplemented with one or two other devicesfor overflow services.
Final Recommendation & Action Plan
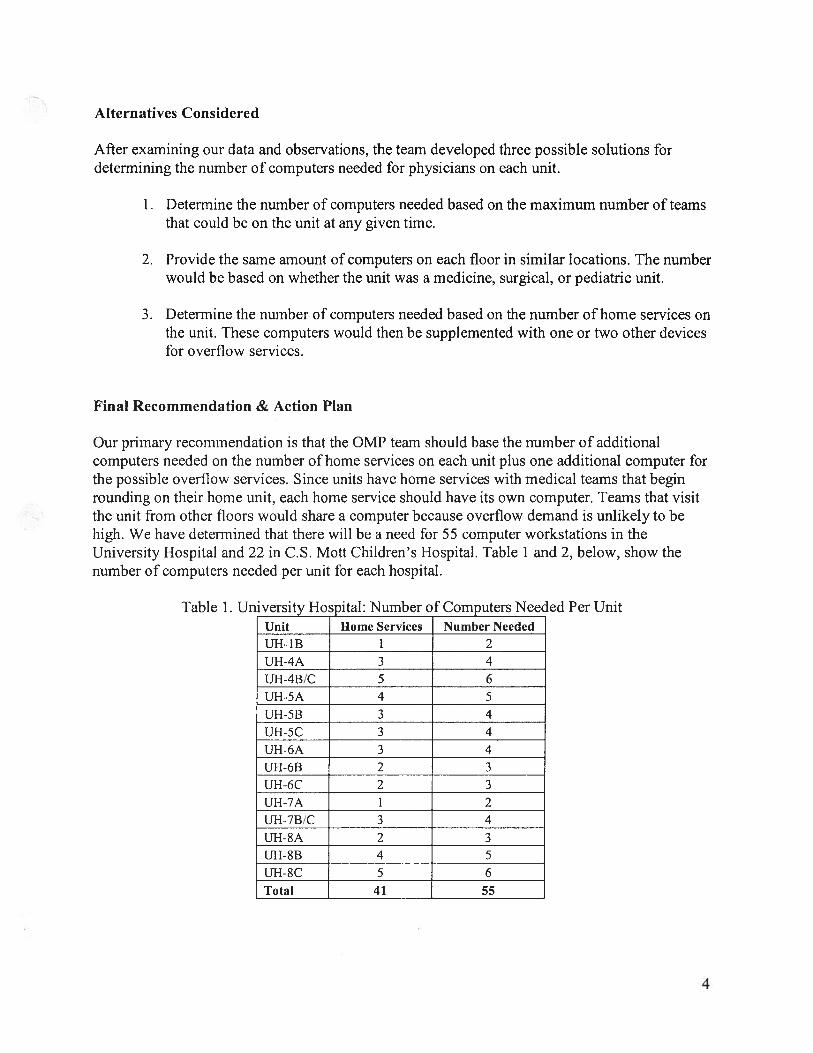
Our primary recommendation is that the OMP team should base the number of additionalcomputers needed on the number of home services on each unit plus one additional computer forthe possible overflow services. Since units have home services with medical teams that beginrounding on their home unit, each home service should have its own computer. Teams that visitthe unit ifom other floors would share a computer because overflow demand is unlikely to behigh. We have determined that there will be a need for 55 computer workstations in theUniversity Hospital and 22 in C.S. Mott Children’s Hospital. Table 1 and 2, below, show thenumber of computers needed per unit for each hospital.
Table 1. University Hospital: Number of Computers Needed Per UnitUnit Home Services Number Needed
UH-1B 1 2
UH-4A 3 4
UH-4B!C 5 6
UH-5A 4 5
UH-5B 3 4
UH-5C 3 4
UH-6A 3 4
U1-I-6B 2 3UH-6C 2 3UI-1-7A 1 2U1-1-7B!C 3 4
U1-1-SA 2 3
UH-8B 4 5
UH-8C 5 6
Total 41 55
4

Table 2. CS. Mott Children’s Hospital: Number of Computers Needed per UnitUnit Services Number NeededMott-Birthing Center 3 3Mott-5E 5 5Mott-5W 4 4Mott-6 6 6Mott-7 4 4Total 22 22
Due to the current variation in the order writing process, we recommend that the OMP team reanalyze physician workflow once computers have been implemented. At that time, additionalcomputers can be ordered as needed. Physician order writing practices are expected to changeonce as the hospitals transition from paper to paperless order entry. The OMP team should alsoconsider the following:
• Physicians would prefer tablet PCs. The team should continue working with Eclipsys inorder to provide software that can be implemented on tablet PCs.
• Units may have to reorganize to provide storage space for accommodating additionaldevices.
• Physicians have concerns about multiple logins during rounds. The team should considera wireless authentication system, which can be implemented using XyLoc cards orexisting M-Cards. This will help decrease rounding time, while maintaining HIPAAstandards.
5

Introduction
Currently, the University of Michigan Hospitals rely heavily on a paper system for managingpatient information and physician orders. Medical staff write orders in the patient charts duringrounds. The Orders Management Project (OMP) is in the process of implementing software thatwill allow caregivers to manage orders electronically to improve the quality and safety of patientcare. This report gives a detailed account of our findings and analysis of physician workflow andordering practices. It also presents our conclusions and final recommendations for the numberand type of additional workstations that will meet physician needs in the University Hospital andC.S. Mott Children’s Hospital.
Goals and Objectives
To determine the quantity and type of the new computer workstations, we have completed thefollowing tasks:
• Studied current order entry processes on various units• Determined potential demand for the new system• Researched types of devices for the orders entry software
We have developed recommendations to facilitate the hospitals’ transition from a paper to anelectronic ordering system in times of high demand. If implemented, the recommendations willresult in:
• Increased medical staff efficiency by reducing the time to write and access orders• Improved employee and patient satisfaction
Background
The University of Michigan Hospitals’ transition to a Computerized Physician Order Entry(CPOE) system reflects a growing trend among hospitals and healthcare systems. The OrdersManagement Project team was formed to investigate and implement a system that wouldaccommodate the needs of the University and C.S. Mott’s Children’s Hospital. The OMP teamconsists of more than 100 individuals working in several clinical departments, nursing units,Medical Center Information Technology (MCIT) and other areas. The OMP team will beimplementing Eclipsys’ CPOE software, Sunrise Clinical Manager XA, beginning in March2006. There are plans to install computer workstations in each patient room and to install SunriseClinical Manager onto all existing computers throughout both of the hospitals.
Hospital CPOE systems are considered to be a technical solution to medication-ordering errorsthat can result in hazardous drug interactions and dosage quantities. CPOE provides an organizedand efficient means of transferring data between medical staff throughout the hospital. TheCPOE system also includes an updatable knowledge library, which will help nurses and doctorstreat patients according to the most recent research findings for their conditions. For example,before prescribing a drug, the physician would be prompted with a series of drugs that may beused to treat the current condition and/or prevent the condition from reoccurring. This method isknown as “evidence-based medicine,” which ensures that patients get the best treatment at the
6

exact point of care. A screenshot of the Sunrise Clinical Manager software is included inAppendix A.
The following key issues with the current paper system are driving the need for this initiative:• Physicians and caregivers are unable to attain patient order information easily and
quickly.• Patient intbrmation may be inaccurate due to the length of time between when
information was learned and when it was recorded.• Uniform patient order entry system is needed throughout health system.
We assisted the Orders Management Project team by recommending the number of additionalcomputer workstations needed for physicians, especially during rounds.
Project Scope
This project involved observing 21 acute care units within the University Hospital and C.S. MottChildren’s Hospital (see Appendix B for a complete list). We collected data during roundingtimes when charts were in high demand to determine the maximum number of staff who willneed access to a computer workstation.
Intensive Care, Ancillary, and Psychiatric units were excluded from this project. Any taskconnected to the technical implementation or functional details of the new system wasconsidered to be outside the scope of this project. Also, we did not develop standardized workmethods for entering orders during rounds.
Approach and Methodology
To determine the optimal number and type of workstations for each unit, we performed thefollowing steps:
1. Gathered supplemental information on CPOE systemsThe OMP student team researched CPOE systems that have been implemented invarious health care settings and also visited St. Joseph Mercy Hospital in Ann Arbor,MI to gain a better understanding of their CPOE system. We also researched variousdevices commonly used with CPOE systems.
2. Determined peak workflow timesThe nurse manager of each of the 21 units was interviewed to determine the numberof services offered on each unit as well as the number of teams that may roundsimultaneously. We also inquired about their current order entry process. The nursemanager recommended days and times for observing peak rounding. Pharmacy datawas used to verify these peak rounding times. Information was also gathered on howrounds normally occur and how and when orders are written.
3. Shadowed medical teams performing rounds
7

Data was collected for each service during the peak times recommended by the nursemanager in order to assess the workflow. The first unit was observed by the entireOMP student team and the remaining 20 units were divided among the team, witheach student observing 5 units. While observing, the following data was recorded:
• Number of teams performing rounds concurrently on the unit• Number of medical staff on each team• Number of staff needing access to charts
4. Analyzed interviews and observationsWe analyzed the workflow and developed possible options for choosing the numberof computers needed based on the existing rounding practices of each team and themaximum number of staff needing access to the system during peak hours.
5. Developed recommendationsBased on the team’s observations and analysis, we developed recommendations forthe number and type of workstations that will best facilitate writing and retrievingorders in each unit after the implementation of the electronic ordering system. Thecost of devices was also taken into consideration during the recommendation phase.
Findings
The OMP student team has collected data by performing a literature search on CPOE systems,visiting a hospital with an established CPOE system, and observing teams on rounds. Weresearched medication ordering trends and obtained cost information for the possible types ofdevices that are being considered.
Supplemental Information on CPOE Systems
Saint Joseph Mercy Hospital in Ann Arbor, MI has a CPOE system that has been in place for 10years. The hospital currently uses their paper charts in addition to the computerized order entrysystem. There are no computers located in the patient rooms. In the next 5 to 6 months, thehospital will be transitioning to a paperless system. To maintain HIPAA security requirements,the hospital has made use of wireless authentication technology by providing XyLoc cards totheir staff. The XyLoc cards allow medical staff to wirelessly login to the CPOE system if theyare in close proximity to a computer. This allows quick access to the system to enter orders, andsimilar technology could be implemented at the University of Michigan Health System, possiblyusing existing M-Cards. A more detailed summary of the findings is located in Appendix C.
Two articles, Comparison of time spent writing orders on paper with computerized physicianorder entry and The effects of CPOE on ICU work/low: an observational study were relevant toour project. In summary, CPOE systems may increase order writing time and interrupt currentworkflow processes. A detailed study of the current order writing system and providing staffwith clear explanations of the system before implementing CPOE can help to avoid these andother problems. A detailed summary of these articles is located in Appendix D.
8

We also researched mobile computing options for implementing CPOE, as an alternative to fixedcomputers. Table I summarizes perceived advantages and disadvantages based on an interviewwith Dr. Thomas Gravelyn during our site visit to Saint Joseph Mercy Hospital and an articlefrom the Journal of Healthcare Information Management which can be found in Appendix E.
Table 1. Advantages and Disadvantages of Various CPOE DevicesType of Device Advantages Disadvantages
Personal Data Assistant • Long battery life • Small screen size(PDA) • Low cost • Limited web browser functionality
• User familiarityCOWs (Computer on • Full Screen Size • Awkward to hold & use whileWheels) • Increased web browser walking/standing
Functionality • Heavy to hold over long period of time
Tablet PC • Lightweight • Short battery life. Stylus makes drop down menus • Limited space in patient room to seteasily accessible down Tablet PC. Lighting causes glare on screen
Variation in Physician Workflow
Through observations and interviews conducted on each of the 21 units, we discovered that thereis some variation in the way medical teams perform rounds. We developed a flow chart todisplay the general rounding process, shown below in Figure 1.
Medical students prepare for rounds and Team of attending physicians, residents,collect information off of patient charts. interns, students, nurses begins rounds.
Students report on patient status.
1Attending physician/resident discussespatient and requests orders.
‘1r
Intern or student writes orders. Thesemust be signed by the intern.
‘1rTeam enters patient room and administerscare.
Figure 1. General Rounding Process for Teams
9

Adult and Pediatric Surgery units have peak rounding times between 6 a.m. and 8 a.m., whileMedicine units have peak rounding times occur between 8 a.m. and 11 a.m. Also, roundingteams on the Surgery units carried patient charts along with them during rounds, while teams onthe Medicine units did not carry charts with them. A detailed summary of our observationsduring rounds can be found in Appendix F.
Pharmacy data was used to verify our peak rounding times. Figure 2, below, shows the totalamount of medication orders per hour for the pharmacies in University Hospital and C.S. MottChildren’s Hospital. This data represents the average number of orders over the weeks of July17, 2005 and the week of September 11, 2005. The grey dotted lines on the graph help toillustrate that peak ordering time occurs in the morning hours for most of the pharmacies. Thereis a difference of about one to two hours from when the physicians perform rounds and whenorders are entered in the pharmacy because the paper orders are collected every hour and thenprocessed.
2500 -.
2000
U)
a,1500
1000
500 -
00123456
Figure 2. Medication Orders at All Hospital Pharmacies
The University Hospital line represents the total number of orders from three pharmacies: UH5,UH6, and UH8. UH5 serves patients on floors 4 and 5, UH6 serves patients on floors 6 and 7,and UHS serves patients on floors 8 and 9. The UH6 and Mott pharmacies are open 24 hours perday.
Consideration of Home and Overflow Services
Through observations and interviews, we found that there may be multiple services rounding oneach unit. Each unit has a certain number of patient beds available for each home service. Anyadditional patients belonging to a service may have to move into overflow space on other units.This causes some physicians to carry charts with them to multiple floors during rounding. Figure1, below, shows the number of services per unit for the University Hospital, based on our
SourceUMHS Pharmacy Dept.
7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Weeksof7/17/05&9/11/05
Hour of the Day
10

observations. It is decomposed into the number of home services and the total number of
10
U) 8-E
1—6I.
E 3z 2
10
4? 4) c:;? ‘ coO /\ \ coo‘s \3S
\ \ \S \SFigure 1. University Hospital: Number of Services per Unit (Home and Overflow)
Figure 2, below, shows the number of services per unit at C.S. Mott Children’s Hospital.
Mott-Birthing Mott-5E Mott-5W Mott-6 Mott-7Center
Figure 2. CS. Mott Children’s Hospital: Number of Services per Unit
services, home plus overflow services.
Source:OMP 5tudent TeamObservations10/2/05-11/5/05
Source:OMP Student TeamObservations10/2/05-11/5/05
6
U,
E
I—.4-04I0.0 3Ez
0 -f
6
4 4
i4t--. ov.
11

The variation in the amount of services on each unit, which can be seen in Figures 1 and 2, hadto be taken into consideration when developing our alternative solutions and finalrecommendations.
Alternatives Considered
After making observations, completing our literature search, and analyzing our data, our teambrainstormed three alternative solutions for determining the number of computers to implementon each unit.
Number of Computers = Number of Services Possibly on Unit
The first alternative we considered was to base the number of computers needed on the numberof services that could potentially be performing rounds simultaneously on each unit. Thisalternative would involve a mix of fixed computers and computers on wheels (COWs). Having acomputer available for each team would ensure that all teams would have access to a computer atany time and not have to wait to write orders. This option could potentially lead to a surplus ofcomputers that remain unused because it is unlikely that every service will have a team roundingat the same time. We have observed that surgical teams round early in the morning (6 a.m. — 8a.m.) and finish rounds at a set time each day to get to the operating room on time. Medicineteams begin later in the morning (8 am. — 11 am.) and can round throughout the day. Also,during our observations of the units, we noticed that there is a limited amount of storage space,so there may not be enough room for the computers this alternative would require.
Number of Computers = A Uniform Number for Each Unit
The second alternative considered was to place the same number of fixed computer workstationsin similar locations on each floor in the hospital. Saint Joseph Mercy Hospital in Ann Arbor, MIhas their CPOE system set up with two computers on each unit in the same location, on a shelfbuilt into the wall. While this alternative would provide standardization across the hospital, it isnot realistic because units such as 4B/C and 7B/C at the University Hospital are busier with moreservices and teams needing access to the computers. Determining an optimal number ofcomputers for each unit would be challenging. Bottlenecks may also be created by using auniform number on each unit.
Number of Computers = Home Services + 1 for Overflow Services
The final alternative we considered was to base the number of computers on the number of homeservices for each unit. One additional computer should be installed to accommodate overflowservices that may have teams rounding on the unit. Each home service would have a computerand if the team needed to travel to another floor during rounds, orders could be entered on thatunit’s overflow computer. This option ensures that home teams will have sufficient access tocomputer workstations. One additional computer may not be enough for some units, but the needfor more computers could be evaluated with a follow-up study once the OMP team beginsimplementation.
12

Final Recommendation
Our team considered the three alternatives above and developed three criteria that should beconsidered for making our final recommendation. The main criteria for the number of additionalcomputers were the potential to accommodate existing physician workflow and amount of spaceneeded. We also considered the cost for computer components. Table 2 gives unit costs for thedifferent types of computers the OMP team is considering. We took this information intoconsideration when developing our final recommendations. A detailed cost analysis can be foundin Appendix G.
Table 2. Computer Component CostsItem Unit Cost ($)Fixed computer $ 1,554.00Laptop $ 1,912.00Extended 10-Hour Battery $ 250.00Laptop Cart (small footprint) $ 547.00
*Q(e: CO W—Lap1op + Laptop Cart
We recommend that the OMP team base the number of additional computers needed forphysicians on the number of home services on each unit plus one additional computer for thepossible overflow services. Since medical teams begin rounding on their home unit, each homeservice should have one computer. Teams that visit the unit from other floors would share onecomputer because the demand for that overflow computer will be staggered throughout the day.Also, teams that travel to other floors often conclude rounds in a conference room on their homeunit. Surgery units would benefit from the mobility of COWs because of time constraints forphysicians writing orders on these units. Because medicine units have a less time-restrictedrounding practice, we recommend fixed computers, especially because they are less expensive.
We have determined that there will be a need for 77 total computer workstations, 22 for C.S.Mott Children’s Hospital and 55 for the University Hospital. Recommendations for each unit inthe two hospitals are shown in Table 3 and 4 below.
Table 3. C.S. Mott Children’s Hospital: Number of Computers Needed per UnitUnit Services Number NeededMott-Birthing Center 3 3Mott-5E 5 5Mott-5W 4 4Mott-6 6 6Mott-7 4 4Total 22 22
13

Table 4. University Hosoital: Number of Computers Needed per UnitUnit Home Services Number NeededUH-1B 1 2UH-4A 3 4IJH-4B/C 5 6UH-5A 4 5UH-5B 3 4UH-5C 3 4
UH-6A 3 4
UH-6B 2 3UH-6C 2 3UH-7A 1 2U1-1-7B/C 3 4UH-8A 2 3UH-8B 4 5UH-8C 5 6Total 41 55
Action Plan
Currently, there is a lot of variation in the order writing process. We have observed orders beingwritten by one person per team, teams breaking up into smaller teams and then writing orders,and also physicians taking notes on all of their patients before writing orders. All of thesepractices are subject to change once the new CPOE system is implemented and available tophysicians. Therefore, after implementing the CPOE system, we recommend that the OMP teamre-analyze physician workflow and purchase additional computers if there are significantbottlenecks.
In addition, we recommend the OMP team continue to consider the use of Tablet PCs, whichmay be more realistic than COWs for surgery units. Physicians on these units want to completerounds as fast as possible in order to be in the operating room by a certain time. Not havingtablets available may increase the time they spend writing orders. Tablet PCs would requiresignificantly less storage space than necessary for COWs and fixed computers.
14

Appendix A: Screenshot of Sunrise Clinical Manager software
iI
ii
$1
:
tq
;cj’.t: -.?ei
g
42
1.t
i:ç;jL’)f
r
4—‘ 6
c
-it— $
x1:;fJ:i :r— - ti.-i t5
‘ wL1k..4 LiCC
4.1
-iI:1
,—HL
II jtL
<Ft: .•1 ;çti A
-
I:cib 4:
: Ltii
ii’ ;lt’ar
‘
-z
Ii®i4l, Ill
L
13
.1-{II Ii }LJ !!U CC =
;r]j- .. 1-H. :L Hr
6-1
C
1ci
L
N
Oi
ciiii
U
-4
InCl
-I4
[1
USCc,C
U
C
(CI
I—I
[4
.1)
-J
ChI
5:3
13LIU
4
Pci
-3C
-1c
CI
4
LIC
ci
ciCC
C,J‘0
P
Wi
C
CSC
8
C
U
C
a
II)
9)ii(9UIc
‘Cii
Ua’
UtU
-‘A
cit
lat
Ut
C
-S.4C
C
44I
‘VU
‘F
CC
50I
-13-F --
5> ci
.o3
C
‘itJ9:n
4-
(4
C)
-‘C
14)CC
C
(3
ciC
II
Cl-I
8C
iC
81II
CD
U
4)
U
S9:U
cc
(Al
C
5LiI
ciC
cci
CC
I)
-SC
CCC
30’cCI_-iSbSI
-It
C
S-C
I‘C‘1’
a.
IIC
I
‘C,1-
41
C-‘.1
C
Lii2ICCCC
U8U)
LI,
C-9)UI
‘I)
-‘8Oj
ill
—
I-B fr)
I
8-ci
‘I.
I!
‘13 -13
1? 5C4’ [(lCDSt-s
I-’ CI0 U’ -I)iiCC C
15

Appendix B: Acute Care Units within Project Scope
Unit Category ServiceUH-1B Trauma TB Acute CareUH-4A Surgical Neuro, Neurosurgery, OtolaryngologyUH-4BC Surgical Vascular Surgery, Thoracic SurgeryUH-5A Surgical OrthopedicsUH-5B Surgical Vascular Surgery, Internal MedicineUH-5C Surgical Transplant, GI SurgeryUH-6A Rehab Adult RehabilitationUH-6B Medicine Acute Care Medicine, GIUH-6C Medicine Pulmonary, Internal MedicineUH-7A Research Clinical Research CenterUH-7BC Medicine Cardiology Medicine, Stepdown Unit, TelemetryUH-8A Oncology Heme, One, Bone Marrow, InfusionUH-8B Oncology Gyn, Oncology SurgeryUH-8C Surgical General Surgery, MedicineMott-4E Women Birthing CenterMott-4W Women Birthing CenterMott- 5 E Ped Surgical Cardio/ThoracicMott-5W Peds General Med, Surgery 0-18 yrsMott-6 Peds Pediatric Med/SurgMott-7 Peds Heme/Onc/Bone Marrow TransplantMott -7E Women Birthing Center Overflow
16

Appendix C: CPOE at St. Joseph Mercy Hospital, Ann Arbor, MI
Date: October 24, 2005Time: 2pm — 3pmContact: Dr. Thomas Gravelyn, MD, MBA
(gravel yttrinity-health.org)
Below are the main observations from our site visit to Saint Joseph Mercy Hospital.
• The CPOE system has been in running for 10 years.• The number of patients per floor, number of services, and nurse to patient ratio were all
considered when determining the number of computer workstations.• Each unit has 2 computer workstations per wing of 20 patients. Nurse workstations have
—5- 10 computers and physicians have more computers located in conference roomsthroughout the hospital.
• Clinicians are using the CPOE system in addition to paper charts. Thus, physicians writeorders down then enter them in after logging into a workstation in the hallway or in aconference room.
• In the next 5-6 months, the hospital will be transitioning to paperless system and orderswill only he able to be entered at the computer workstations. A team is currentlyanalyzing the number of additional workstations that will be needed to preventbottlenecks in the future.
• There are no computers in patient rooms. There were concerns that patients and hospitalemployees might have access to patient information or abuse the system by surfing theinternet.
• For the ICU, a XYLOC card that the doctors wear on their badges allows for wirelesslogin to certain computer workstations and all systems are shut down when the doctorleaves the area to ensure HIPAA compliance.
Note: XyLoc cards are produced by Ensure Technologies Inc., headquartered in Ann Arbor, MI,that specializes in the development of intelligent security solutions. More information about thiscompany and their technologies is available at their website, http://www.ensuretechcom.
17

Appendix D: Computerized Physician Order Entry (CPOE) Research
Article 1
In 2001, a study was done by an information systems group from Massachusetts GeneralHospital to assess the effect of CPOE implementation on physician time use. The physician orderentry system was implemented at the hospital in November 1998. The information systems groupmeasured time spent before and after CPOE and the impact of CPOE on hospital staff.
The group found that the time required to write orders was longer with the order entry systemthan with the paper system, but the interns spent less time performing clerical duties after orderentry implementation. Also, order entry did not decrease the time spent with patients and internsspent more time with patients arid less time with other physicians. On the contrary, the studyfound that physician order entry reduced medication error rate by at least 50%.
The study concluded that “order entry results in a transfer of work.” Physicians may spend alonger time entering orders in the computer, but other medical housestaff (such as pharmacy andadministration staff) benefit from clearer and readily available orders. The group suggests thathospitals wishing to implement CPOE should provide staff with clear explanations of advantagesand disadvantages and to also establish a commitment to making the application as fast aspossible.
Reference:Shu K., Boyle D., Spurr C., Horsky J., Heiman H., O’Connor P., Lepore J., Bates D.W.“Compansion of time spent writing orders on paper with computerized physician order entry.”Medifo Proc of 10/Il World Congress on Medical Informatics 2001; 84: 1207 — 1211.
Article 2
In 2003, a research team at the Stanford University Department of Medicine conducted anobservational case study to assess the effects of CPOE on healthcare team workflow. Theyobserved the work patterns of 50 individuals on an ICU care team, including physicians, nursingstaff, two pharmacists, and a respiratory therapist.
The study found that the CPOE system increased the coordination load among physicians andnurses and added verification tasks. The system required that the physician enter the order aswell as sign it, which created a delay in getting the orders to the nurse. Thus, the nurse had tofrequently find the attending physician to ensure that an order had been entered. Therefore,policy was changed to allow physicians to enter orders for all patients on the ward, whichfacilitated quicker delivery.
There was also some difficulty with the computational interface, which varies by CPOE systemmanufacturer. The structured data required of CPOE prevents errors, but may rely on a cognitivetemplate of classifying orders that is not shared by the physicians. Logging in to the system alsoproved to be inconvenient. The system included a timed logout for security purposes, which
18

caused some physicians to enter orders in others’ logged-in sessions instead of having to log inagain themselves. Therefore, physicians “signed” orders which they had not indeed entered.
The distance to the computers also created some interruptions in workflow for the care team. Thephysicians and nurses frequently had to travel between the bedside and the work area in order toenter the orders into the computer, since printers were not centrally located in the ICU. Becauseof this distance, some orders were out-of-sync with the actual work process.
Overall, the study demonstrated that while there are benefits to CPOE such as error reductionand guideline adherence, the implementation of the system may interrupt current workflowprocesses. It is important to do observational workflow studies to design CPOE systems that donot create more errors and “achieve the full potential benefit for improved patient safety.”
Reference:Cheng, C.H., Goldstein, M.K., Geller E., Levitt, R.E. “The effects of CPOE on ICU workflow:an observational study”. AMIA Annu Symp Proc. 2003: 50 — 154.
19

Appendix E: Mobile Computing Options for Implementing CPOE
In the Fall 2005 edition of the Journal ofHealthcare Information Management, an articledescribed a pilot study of the experiences of six clinical pharmacists at the University ofMichigan Medical Center, as they incorporated tablet PCs into their workflow. Before decidingto use tablet PCs, PDAs and traditional laptop computers were also considered. PDAs had thelongest battery life but the tiny screen size and the inadequacies of the web browser made it notfeasible. Since the clinical software that will be used is web-based, PDAs were notrecommended.
Next, traditional laptop PCs were evaluated. Clinical Pharmacists were impressed by the screensize and ability to easily navigate the software, but issues of portability and securityauthentication became overwhelming. Laptop PCs contain permanently attached keyboardswhich limited the workers ability to record information while performing rounds since flatsurfaces were not always available. For security reasons, clinical pharmacists had to repeatedlylogin. Based on these reasons laptop PCs were eliminated during the pre-pilot phase.
Tablet PCs typically come in two different styles, slate and convertible. The slate contains onlyone rectangular piece without a keyboard and the convertible has an attached keyboard that canswivel and be stored behind the screen. The convertible type was not used in the actual pilotstudy, due to the extra weight of the keyboard. Additionally, the slate model contained abiometric authentication device which allowed clinicians to login quickly using their thumbprint.
Responses to the implementation of tablet PCs were both positive and negative. Cliniciansreported greater accuracy in recording patient data and they experienced little difficulty adjustingto the devices. However, many clinicians experienced problems using the tablets wirelessinternet service when traveling into elevators and stairwells due to a lack of wirelessconnectivity. They were often required to login again and some lost information. The finalconcern clinicians expressed was the ability to physically secure the tablet devices and preventthefts. Clinicians suggested that constant reminders and perhaps training are absolutelynecessary to ensure that hospitals experience minimal losses.
Reference:McCreadie, Scott. R, McGregory, Michael E. “Experiences Incorporating Tablet PCs intoClinical Pharmacists’ Workflow”. Journal of Healthcare Information Management. Fall 2005:32-37.
20

Appendix F: Observations During Rounds
University Hospital
Time Observed Did teams NumberDate Observed Number of round with needing access
Unit Observed (A.M.) Teams charts? to chartslB 11/1/2005 7:30-8:30 1 yes 24A 11/10/2005 7:30-8:30 3 no 24B/C 11/10/2005 7:30-8:30 4 yes 25A 10/26/2005 7:30 - 8:30 2 yes 2SB 11/10/2005 7:30-8:30 4 no 2Sc 11/10/2005 7:30-8:30 3 yes 26A 11/1/2005 7:00-8:30 n1a no 16B 11/2/2005 7:00-8:30 3 no 16C 11/3/2005 7:00 - 8:30 3 no 17A 10/25/2005 8:00 - 9:30 n/a no 17B/C 10/21/2005 8:00 - 9:00 3 no 18A 11/7/2005 8:30-9:30 2 no8B I 1/7,2005 9:30 - 10:00 1 no 18c 10/14/2005 6:45-7:45 3 yes 1
C.S. Mott Children’s Hospital
Time Observed Did teams NumberDate Observed Number of round with needing access
Unit Observed (A.M.) Teams charts? to chartsBirthingcenter 10/29/2005 9:00- 11:00 2 no 1SE 10/18/2205 6:00 - 8:00 2 yes5W 10/25/2005 6:15-7:45 3 yes 16 11/8/2005 6:20-7:30 3 yes 17 11/8/2005 6:20-7:30 4 yes 1
21

Appendix G: Cost Analysis
Item Unit Cost ($)CPU, Monitor, Standard Keyboard, & Optical Mouse - Fixed $ 1,554.00D610 Laptop $ 1,912.00Extended 10-Hour Battery $ 250.00Laptop Cart (small footprint) $ 547.00
Laptop D610 Laptop ÷ Extended 10-hour battery + Laptop cart (small footprint) = $2,709
University HospitalUnit Home Number Needed Cost - Fixed Cost - COWUH-1B 1 2 $3,108.00 $5,418.00UH-4A 3 4 $6,216.00 $10,836.00UH-4B/C 5 6 $9,324.00 $16,254.00UH-5A 4 5 $7,770.00 $13,545.00UH-5B 3 4 $6,216.00 $10,836.00UH-5C 3 4 $6,216.00 $10,836.00UH-6A 3 4 $6,216.00 $10,836.00UH-6B 2 3 $4,662.00 $8,127.00UH-6C 2 3 $4,662.00 $8,127.00UH-7A 1 2 $3,108.00 $5,418.00UH-7B/C 3 4 $6,216.00 $10,836.00UH-8A 2 3 $4,662.00 $8,127.00UH-8B 4 5 $7,770.00 $13,545.00UH-8C 5 6 $9,324.00 $16,254.00Total 41 55 $85,470.00 $148,995.00
C.S. Mott Children’s HospitalUnit Services Number Needed Cost - Fixed Cost - COWMott-Birthing Center 3 3 $4,662.00 $8,127.00Mott-5E 5 5 $7,770.00 $13,545.00Mott-5W 4 4 $6,216.00 $10,836.00Mott-6 6 6 $9,324.00 $16,254.00Mott-7 4 4 $6,216.00 $10,836.00Total 22 22 $34,188.00 $59,598.00
Number Needed = # of Home Services + 1 computer for Overflow
Fixed CowGrand Total $119,658.00 $208,593.00
22