oral health knowledge, attitudes and practices among ... · 4 abstract background: oral hygiene is...
TRANSCRIPT

ORAL HEALTH KNOWLEDGE, ATTITUDES AND
PRACTICES AMONG STUDENTS IN TWO SECONDARY
SCHOOLS IN LAIKIPIA COUNTY.
INVESTIGATOR:
NDAIGAH SERAH
BDS LEVEL III
V28/1964/2010
A community dentistry research project submitted in partial fulfillment of the Bachelor of
Dental Surgery (BDS) of the University of Nairobi.

ii
SUPERVISORS
PROF.LOICE W .GATHECE. BDS., MPH., PhD.(Nbi).
DEPARTMENT OF PERIODONTOLOGY /COMMUNITY AND PREVENTIVE
DENTISTRY,
SCHOOL OF DENTAL SCIENCES,
UNIVERSITY OF NAIROBI.
Dr.ANDREW WETENDE. BDS., MDS. (Nbi)
KENYATTA NATIONAL HOSPITAL.
iii
DECLARATION AND SUBMISSION FOR APPROVAL
I Serah Wanjiru Ndaigah hereby solemnly declare that this is my original work and that it has
not been submitted by any other person for research purposes, degree or otherwise in any
other college/University.
Signed……………. Date…………….
SUPERVISORS APPROVAL
This project has been submitted in partial fulfillment of Bachelor of Dental Surgery Degree
with our approval as University of Nairobi supervisors.
Prof. Loice Gathece
Signed…………………. Date………………………..
Dr Andrew Wetende
Signed………………….. Date……………….

iv
DEDICATION
This project is dedicated to my parents, Ruth Nyambura and Charles Ndaiga

v
ACKNOWLEDGEMENT
I would like to express my sincere gratitude to the Almighty God for health and wellbeing
throughout my research.
Special thanks to my supervisors Prof Loice Gathece and Dr Andrew Wetende for their
guidance and advice in research.
To everyone who may have contributed directly or indirectly to the success of this research
work especially my father, Mr. Charles Muraga.

vi
List of Abbreviation
BDS Bachelor of dental surgery
DMFT Decay, missed, filled teeth
GB Gigabyte
KNH Kenyatta National Hospital
SPSS Statistical Package for Social Sciences
UON University of Nairobi
DEFINATION OF TERMS
Oral health status- caries experience, gingival inflammation, flourosis status and prosthetic
status.

2
TABLE OF CONTENTS
SUPERVISORS .......................................................................................................................................... ii
DECLARATION AND SUBMISSION FOR APPROVAL ................................................................................ iii
SUPERVISORS APPROVAL ....................................................................................................................... iii
DEDICATION ........................................................................................................................................... iv
ACKNOWLEDGEMENT ............................................................................................................................. v
List of Abbreviation ................................................................................................................................ vi
DEFINATION OF TERMS ........................................................................................................................... 1
ABSTRACT ................................................................................................................................................ 4
Background ......................................................................................................................................... 4
Objective: ............................................................................................................................................ 4
Study design ........................................................................................................................................ 4
Study area ........................................................................................................................................... 4
Methodology ....................................................................................................................................... 4
Results ..................................................................................................................................................... 4
Conclusions ............................................................................................................................................. 5
CHAPTER 1 .............................................................................................................................................. 6
1.0 Introduction .................................................................................................................................. 6
2.0 Literature Review .......................................................................................................................... 7
CHAPTER 2 .............................................................................................................................................. 9
2.0 Statement of the Problem........................................................................................................... 9
2.1 Justification of the Study ............................................................................................................... 9
2.2 Objectives: .................................................................................................................................... 9
Main objective: ............................................................................................................................... 9
Specific objectives: .......................................................................................................................... 9
2.3 Null Hypothesis ......................................................................................................................... 10
2.4 Variables ...................................................................................................................................... 11
CHAPTER 3 ............................................................................................................................................ 12
3.0 MATERIALS AND METHODS ........................................................................................................ 12

3
3. Study Area ................................................................................................................................ 12
3.2 Study Design ............................................................................................................................ 12
3.3 Sample Size ............................................................................................................................. 12
3.4 Inclusion Criteria ..................................................................................................................... 13
3.5 Exclusion Criteria ..................................................................................................................... 13
3.6 Study Population ..................................................................................................................... 13
3.7 Data Collection Instruments and Techniques ......................................................................... 14
3.8 Data Analysis and Presentation ............................................................................................. 14
3.9 Logistics ................................................................................................................................... 14
3.10 Ethical Consideration .................................................................................................... 14
3.11 Perceived Benefits ........................................................................................................ 14
3.12 Problems Anticipated .................................................................................................... 15
3.13 Minimizing errors .................................................................................................................. 15
CHAPTER 4 ............................................................................................................................................ 16
RESULTS ............................................................................................................................................ 16
Part A................................................................................................................................................. 16
Part B ................................................................................................................................................. 20
CHAPTER 5 ............................................................................................................................................ 28
5.1 DISCUSSION ................................................................................................................................. 28
Part A ............................................................................................................................................. 28
Part B. ............................................................................................................................................ 29
5.2 CONCLUSION ........................................................................................................................... 30
5.3 RECOMMENDATIOS ................................................................................................................ 30
REFERENCES .......................................................................................................................................... 31
.............................................................................................................................................................. 31
Appendix I ............................................................................................................................................. 32
Appendix II ............................................................................................................................................ 36
Appendix III ........................................................................................................................................... 37
Appendix IV ........................................................................................................................................... 38

4
ABSTRACT
Background: Oral hygiene is essential for the wellbeing of a person. However, lack of
knowledge and negative attitude may lead to lack of or poor practice of oral hygiene.
Objective: To determine oral health knowledge, attitudes and practices among students in
two secondary schools in Laikipia County.
Study design: A descriptive cross-sectional study carried out among secondary school
students.
Study area: The study was conducted in Marmanet and Gatundia secondary schools in
Nyahururu, Laikipia County.
Methodology: A total of 288 secondary school students were selected using stratified
random sampling method. A self administered questionnaires and clinical examination forms
were used to collect data.
Results
There were a total of 288 students recruited in the study. Majority(87%) of the students had
good knowledge regarding their oral health status. The Dmft was 2.25 with a caries
experience of 50.0%.The prevalence of gingivitis was 88%.6.2% of the students had oral
mucosal ulcerations while flourosis prevalence was 48.0%.Only one student had a partial
denture prosthesis.
Discussion
The prevalence of dental caries was 50% which was consistent with other studies done in
Zimbabwe where the caries experience was 59%.This could be attributed to low dental care
awareness and expensive restorative treatment. The prevalence of gingivitis was higher
(88%) than that done in other studies in Juja where the prevalence was 50%.The high
flourosis in this study could be attributed to high levels of fluoride in Rift valley springs
where the respondents get drinking water. About 98% of the respondents brushed their teeth
as they had adequate knowledge on oral health practices. Some respondents reported using
other materials like salt and charcoal in brushing which was also reported in other studies
hypothesized to social economic factors and traditional beliefs.
5
Conclusions
Majority of the students had good knowledge regarding their oral health practices. The most
common mucosal lesion was mucosal ulcerations. About 50% of the respondents had dental
flourosis with more than half having gingival inflammation. Only one patient had a partial
denture .
Recommendations
Establishment of oral health education programs in the school curriculum that will be aimed
at educating students on oral hygiene practices.

6
CHAPTER 1
1.0 Introduction
Oral health is defined as the absence of disease and optimal functioning of the mouth and its
tissues, in a manner that preserves the highest level for self-esteem. Oral health describes a
standard which enables an individual to eat, speak and socialize without disease. Dental
caries and periodontal disease are the major oral diseases in the world. The prevalence of
dental caries in the world is 60-70%. Recently, it is low in American countries and higher in
the African countries with the prevalence in Kenya being 52%.The prevalence of
periodontitis in Kenya is however low about 1-10% with no increase in the recent past1.
Oral health knowledge is considered a prerequisite for health related practices. According to
the World health organization data bank, by 2012 , average for dental caries DMFT values
were 3.(1) In a study done among black adolescents in California, the mean percent correct
on the dental health questions was 55.0%.2 In another study done in Japan, answers indicated
that adolescents know the importance of tooth brushing and dental service utilization.
However, their knowledge about dental sealants and fluoride was inadequate. It was also
concluded that knowledge and perceptions related to oral health are strongly influenced by
the environment, norm and culture3. A study done in Tanga, Tanzania, more than three
quarters of the study population had adequate knowledge on causes, prevention and signs of
dental caries.However, only 2.4% had acceptable practice on brushing teeth. There were
similar findings in UK and Kuwait4.
The study aims at assessing oral health knowledge, attitudes and practices among students in
two secondary schools in Laikipia County. The findings from this study could be used for
planning oral health education programs in school.
7
2.0 Literature Review
Oral health is an integral part of general health. Oral health status has a direct impact on
general health and conversely, general health influences oral health. The worldwide
prevalence of dental caries is 60-90% for school going children and 100% for adults. Severe
periodontitis may result in tooth loss usually found in 15-20% of middle aged (35-44) years
in adults. Oral diseases in children and adults are higher in poor and disadvantaged
population. Risk factors include unhealthy diet, tobacco use, harmful alcohol and poor oral
hygiene. Oral cancers contribute to 10 cases out of 100000 with the prevalence higher in men
than women. Tobacco and alcohol are the predisposing factors of oral cancers.1
In a study done in Kuwait among secondary school students, 56.5% scored below mean on
oral health knowledge with only 43.5% scoring above mean. Generally, knowledge on oral
health was poor. There was no difference in knowledge of oral health between genders
because both genders were equally educated. On the practices, only 52.2% of the students in
the study population visited a dentist when they were in pain. In a study done in Chicago in
2006 by Bretz and Krebs on the effects on dental flossing and brushing on gingival bleeding
and halitosis found that the two greatly reduced after a two week oral health programme.2
Gingival bleeding was reduced by 38% and halitosis also reduced. In a control group that did
not floss as part of their daily routine, gingival bleeding sites increased by 4%. They therefore
concluded that gingival bleeding and halitosis are the first signs of poor oral hygiene that may
lead to further periodontal problems and the best way to prevent periodontal diseases was
through oral hygiene home care and routine dental visits.3,4
In a study done in Tanzania on oral health knowledge and practices among secondary school
students in Tanga, Tanzania, 93.4% were reported to have an acceptable level of practice and
sugary food consumption.98.1% of the participants had adequate knowledge on the
importance of dental checkups; however, there was no statistical significant difference
observed between ages or sex.4.3% of the students reported use of other items for cleaning
like tooth picks.
In a study done by Okemah .K.A on oral health knowledge and oral hygiene practices among
school children in Uasni-Gichu district, 92% claimed to brush their teeth. About 48% brushed
their teeth at least twice daily. Female students brushed more frequently than their male

8
counterparts. Use of tooth paste was reported by 39.9% of the students. Less than half of the
students knew the causes of teeth decay and how to prevent it 7
A study done by Prof. Kaimenyi et al on oral hygiene practices and dental health awareness
of Kenyan school children aged 9-15 years revealed that 93% of the children used a tooth
brush with a tooth paste. 10% of the children knew that bacteria could cause dental caries and
87% of the children knew that dental caries and periodontal diseases could be prevented [5].
Since comprehensive programs on oral health care is still lacking in Kenya among high
school students, as in the case of North Jordan and Uganda which are developing countries,
more dental health education is needed to improve their oral hygiene standards. 6
Consequently, the purpose of this study is to investigate the oral hygiene attitudes,
knowledge and practices among high school students in Laikipia County, Kenya which will
provide data for use in designing programmes with the aim of improving the oral health
among the high school students in Kenya 7, 8

9
CHAPTER 2
2.0 Statement of the Problem
Knowledge, attitudes and devotion of people to effective oral health practices are very
important for good oral health and lack of any of these three factors results in poor oral
health. The latter predisposes the people to oral diseases which cause loss of teeth if not
managed properly. Loss of teeth is detrimental to the quality of life: physically, socially as
well as psychologically.
This therefore, necessitates education to the students on the effective oral health which in turn
will change their negative attitudes towards some oral health practices. Consequently; they
will put into practice whatever they will have learnt and improve their oral health. If this is
not done, then it may result in a high incidence of oral diseases hence degrading their quality
of life.
2.1 Justification of the Study
Very little information about knowledge, attitude and oral health practices is available for
Kenyan schools .The study aims at determining oral health knowledge, attitudes and practices
among students in two secondary schools in Laikipia County. The information is necessary as
it will indicate how much needs to be done for intervention measures o be instituted. The
findings may be used to intervene and improve knowledge, attitude and practices towards the
oral health among students.
2.2 Objectives:
Main objective:
To determine oral health knowledge, attitudes and practices among students in two secondary
schools in Laikipia county.
Specific objectives:
1. To determine the level of knowledge on oral hygiene among secondary school
students.
2. To assess oral health status of secondary school students.
3. To determine the attitude of secondary school students towards their oral health.
10
4. To determine oral hygiene practices among secondary school students.
2.3 Null Hypothesis
Oral hygiene knowledge and attitudes of secondary school students does not influence their
oral health practices.
11
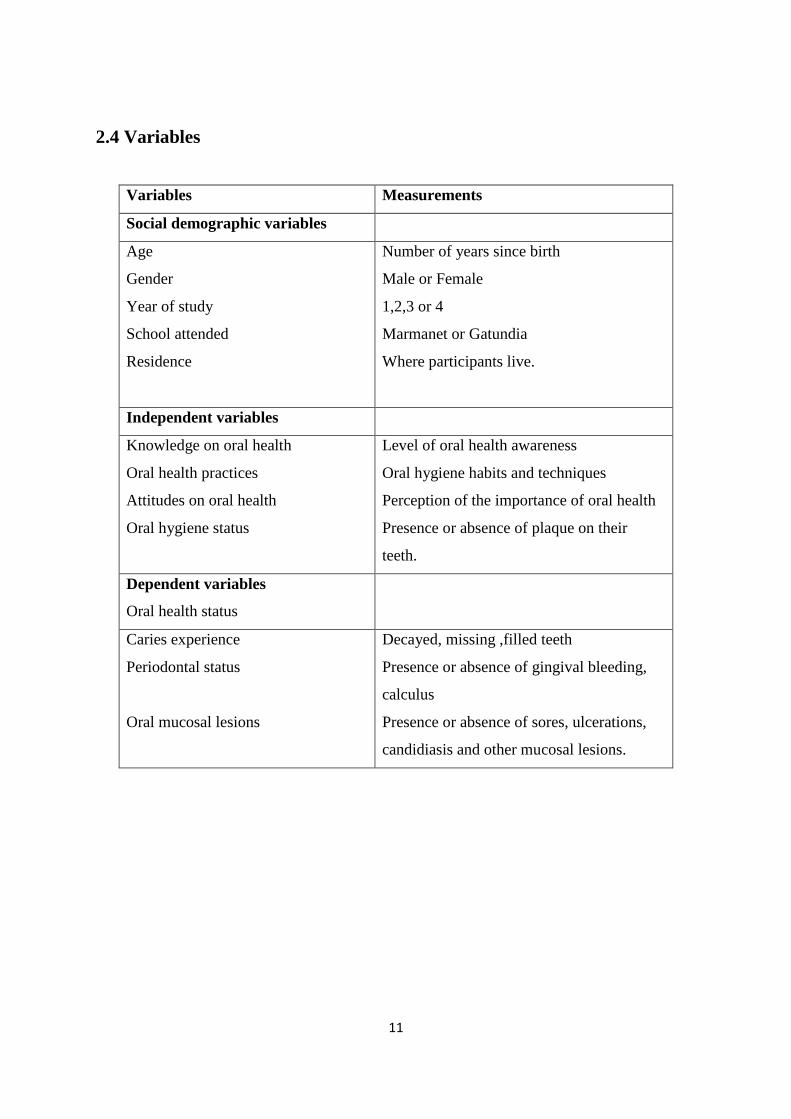
2.4 Variables
Variables Measurements
Social demographic variables
Age
Gender
Year of study
School attended
Residence
Number of years since birth
Male or Female
1,2,3 or 4
Marmanet or Gatundia
Where participants live.
Independent variables
Knowledge on oral health
Oral health practices
Attitudes on oral health
Oral hygiene status
Level of oral health awareness
Oral hygiene habits and techniques
Perception of the importance of oral health
Presence or absence of plaque on their
teeth.
Dependent variables
Oral health status
Caries experience
Periodontal status
Oral mucosal lesions
Decayed, missing ,filled teeth
Presence or absence of gingival bleeding,
calculus
Presence or absence of sores, ulcerations,
candidiasis and other mucosal lesions.
12
CHAPTER 3
3.0 MATERIALS AND METHODS
3. Study Area
The study was conducted in Gatundia secondary school and Marmanet secondary school in
Marmanet location, Laikipia County.LaikipiaCounty is located in the rift valley in Kenya.
Laikipia County borders SamburuCounty to the north and Baringo County to the west. It
covers an area of9, 462.0 Km 2.It has a population of 399,227 (Male – 49.8 %, Female – 50.2
%). Poverty level is rated 46 % (Rural & Urban).Secondary school students enrolment
number is 22,091.Gatundia secondary school is located 12 km from Nyahururu town next to
Gatundia shopping centre. Marmanet secondary school is located 7km from Nyahururu town
and is next to Oljabet shopping Centre on Nyahururu-Rumuruti road.
3.2 Study Design
Descriptive cross sectional study using secondary school based study groups.
3.3 Sample Size
Prevalence of tooth brushing habit among high school students is 50%.(J.T, 1993)
MedJ.1993; 70(2)67-70)
Confidence level chosen for this study is 95%
The sample size for the study will be computed from the following formula:
N=
Where;
Z= the value corresponding to 95% confidence level.
C=1-confidence level
P=Prevalence of teeth brushing habits among high school students
Therefore:

13
N=
= 384.2
=
=
=288
288 students took part in the study. 144 students from each student.
Sampling Methods
Stratified random sampling was used to select students, 144 students from each school.
Students were picked randomly from each class using a table of random numbers.
3.4 Inclusion Criteria
1. Students attending the two schools.
2. Students who consent to participate in the study.
3.5 Exclusion Criteria
1. Students not attending the two schools.
2. Students who decline to consent.
3.6 Study Population
Marmanet and Gatundia secondary school form 1-4 students were included in the study.
14
3.7 Data Collection Instruments and Techniques
Self-administered questionnaires were used to collect data. The researcher distributed the
questionnaires to the students and collected them once the students completed answering
all the questions. The questionnaires were filled from a separate room to avoid
interferences from participants. Data collection also involved intra oral examination and
recorded in clinical examination forms.
3.8 Data Analysis and Presentation
Data was analyzed using the Statistical Package of Social Sciences (SPSS) .Means,
percentages and ratios were calculated and cross tabulation used to compare different
variables and the results presented by use of charts, tables and texts.
3.9 Logistics
A bus will be used to travel from Nairobi to the study area. Accommodation will be
sought at Gatundia, 2km from the study area. There will be a site visit a day before actual
collection of data begins.
3.10 Ethical Consideration
1. Approval was sought from the University of Nairobi/Kenyatta National Hospital
Ethical and research committee.
2. Permission was sought from the school administration through the principal of the
school to carry out the study.
3. Participation in the study was on voluntary basis and Informed consent was sought
from the students.
4. All information was treated with utmost confidentiality.
5. Participants were free to decline or withdraw from participating in the study at any
time during the study period.
3.11 Perceived Benefits
1. The findings could be used to put measures in place to improve the level of oral health
knowledge, attitudes and practices among high school students which may lead to
better oral health.
2. The research proposal is in partial fulfillment of the BDS degree of the University of
Nairobi.

15
3.12 Problems Anticipated
1. Financial constraints.
2. Timeline constrains for the study.
3.13 Minimizing errors
1. The questionnaires were pretested.
2. Randomization during selection of the respondents
3. There was a restriction of respondents to ensure that only those who meet the
inclusion criteria were included in the study.
16
CHAPTER 4
RESULTS
4.1 Social demographic information
Due to inability to match the questionnaire and the clinical examination form,the data
presentation has been divided into two parts.
Part A
A total of 127 participants were recruited in the study. Of these 63(49.6%) were males and
64(50.4%) were females. The age ranged between 14 -21 years with a mean of 17.10 + 1.712
SD years. Females were slightly younger (Mean17.10 +1.386 SD years) than males (Mean
17.09 +1.585 SD years) .However the difference was not statistically significant (t=-0.69,
p=0.95).Figure 1 shows gender distribution.

17
Key
Age groups
Group 1- 14-16 years
Group 2- 17-19 years
Group 3- 20-22 years
Figure 1.Males and females by demographic variables.
4.2Caries experience
Half 63(50.00%) of the participants had dental caries. The prevalence was higher 32(51.8%)
for the females than for the males 31(48.4%). There was no statistical significance between
caries experience and the demographic variables. The table 1 below shows that the main
component of the Dmft was Decay with an overall mean of 1.27SD+ 1.84.There is evidence
of unmet needs with even those going to hospital having extraction as the mode of
treatment. Males were more affected (Mean 1.35 SD+1.94) than females (Mean
1.16SD+1.73).In addition, the younger age group of between 14-16 years were more
affected (Mean 2.32SD+1.42) than the older age group(Mean 1.5SD+1.57).The table below
shows caries experience by demographic variables.
18
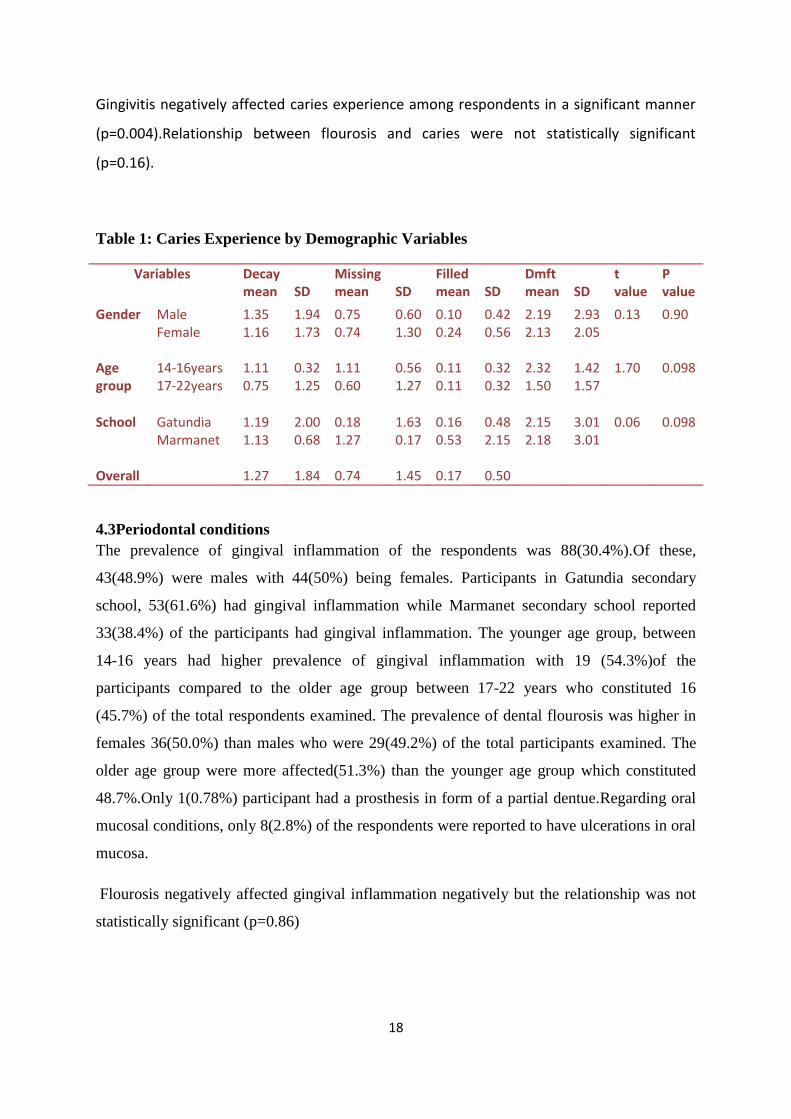
Gingivitis negatively affected caries experience among respondents in a significant manner
(p=0.004).Relationship between flourosis and caries were not statistically significant
(p=0.16).
Table 1: Caries Experience by Demographic Variables
Variables
Decay mean
SD
Missing mean
SD
Filled mean
SD
Dmft mean
SD
t value
P value
Gender
Male Female
1.35 1.16
1.94 1.73
0.75 0.74
0.60 1.30
0.10 0.24
0.42 0.56
2.19 2.13
2.93 2.05
0.13 0.90
Age group
14-16years 17-22years
1.11 0.75
0.32 1.25
1.11 0.60
0.56 1.27
0.11 0.11
0.32 0.32
2.32 1.50
1.42 1.57
1.70 0.098
School Gatundia Marmanet
1.19 1.13
2.00 0.68
0.18 1.27
1.63 0.17
0.16 0.53
0.48 2.15
2.15 2.18
3.01 3.01
0.06 0.098
Overall 1.27 1.84 0.74 1.45 0.17 0.50
4.3Periodontal conditions
The prevalence of gingival inflammation of the respondents was 88(30.4%).Of these,
43(48.9%) were males with 44(50%) being females. Participants in Gatundia secondary
school, 53(61.6%) had gingival inflammation while Marmanet secondary school reported
33(38.4%) of the participants had gingival inflammation. The younger age group, between
14-16 years had higher prevalence of gingival inflammation with 19 (54.3%)of the
participants compared to the older age group between 17-22 years who constituted 16
(45.7%) of the total respondents examined. The prevalence of dental flourosis was higher in
females 36(50.0%) than males who were 29(49.2%) of the total participants examined. The
older age group were more affected(51.3%) than the younger age group which constituted
48.7%.Only 1(0.78%) participant had a prosthesis in form of a partial dentue.Regarding oral
mucosal conditions, only 8(2.8%) of the respondents were reported to have ulcerations in oral
mucosa.
Flourosis negatively affected gingival inflammation negatively but the relationship was not
statistically significant (p=0.86)

19
Table 2 Gingival inflammation and flourosis status.
Variables Gingival inflammation
Present Absent N(%) N(%)
X2 P value
Gender Male Female
48.9 50.0
52.1 50.0
0.54 0.76
Age 14-16 years 17-22 years
54.0 45.7
46.0 54.3
4.23 0.40
School Gatundia Marmanet
61.6 38.4
28.9 61.6
11.27 0.001
Flourosis
Present Absent N (%) N (%)
Gender Male Female
49.2 50.0
54.1 50.0
7.14 0.85
Age 14-16 years 17-22 years
48.7 51.3
52.3 48.7
1.61 0.66
School Gatundia Marmanet
51.6 48.4
48.4 51.6
5.04 0.54
4.4Oral mucosal conditions
When examined for pathologies in the oral cavity, the only abnormal condition examined was
ulceration3(%) males while 5(%) were females .In addition,2(%) of males had the
ulcerations on the vermillion border and 2(%) on the lip while 3(%) of females having
ulcerations on the vermillion border and 2(%) of the ulcerated lesions being located on the
lip. Only 1(%) lesion was found on the buccal mucosa of a female respondent.

20
Figure 2.Distribution of mucosal lesions by site among males and females.
Part B
Social demographic information
. A total of 288 students were recruited in the study that filled the questionnaire. Of these
144(50%) were males and 144(50%) were females. The age ranged between 14 -21 years
with a mean of 17.10 + 1.712 SD years. Females were slightly younger (Mean17.10 +1.386
SD years) than males (Mean17.09 +1.585 SD years) .However the difference was not
statistically significant (t=-0.69, p=0.95).Figure 1 shows gender distribution of the
participants.
21
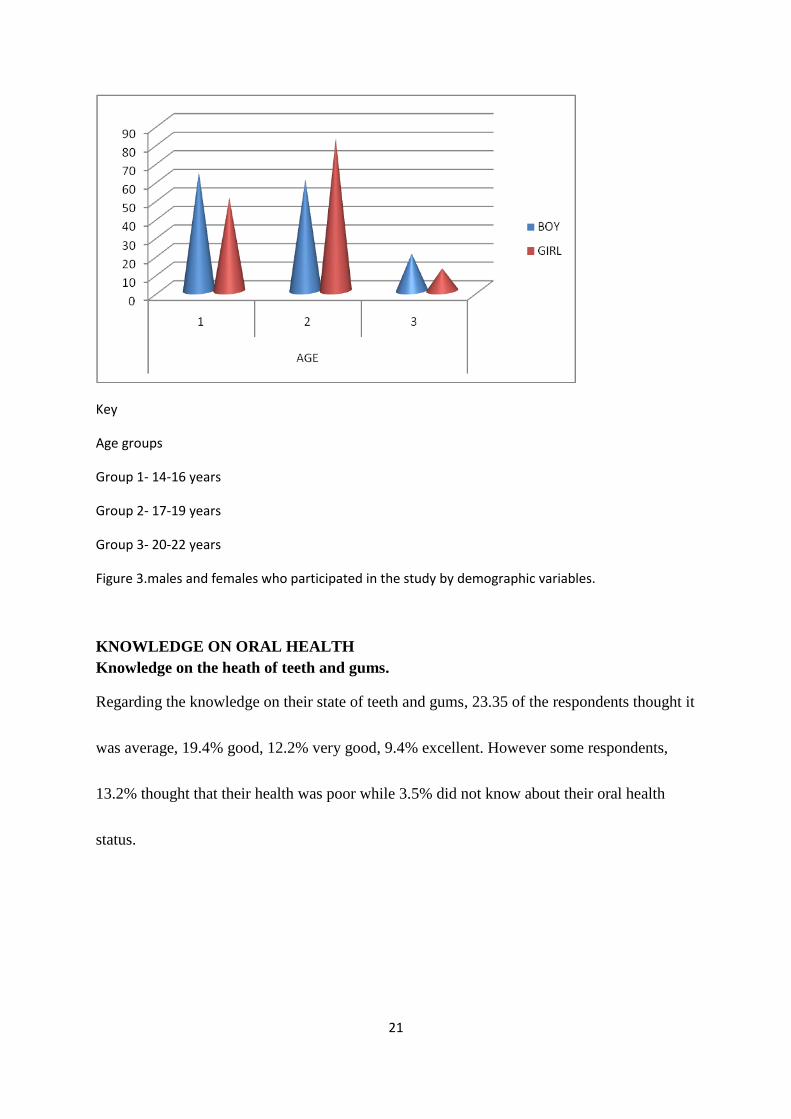
Key
Age groups
Group 1- 14-16 years
Group 2- 17-19 years
Group 3- 20-22 years
Figure 3.males and females who participated in the study by demographic variables.
KNOWLEDGE ON ORAL HEALTH
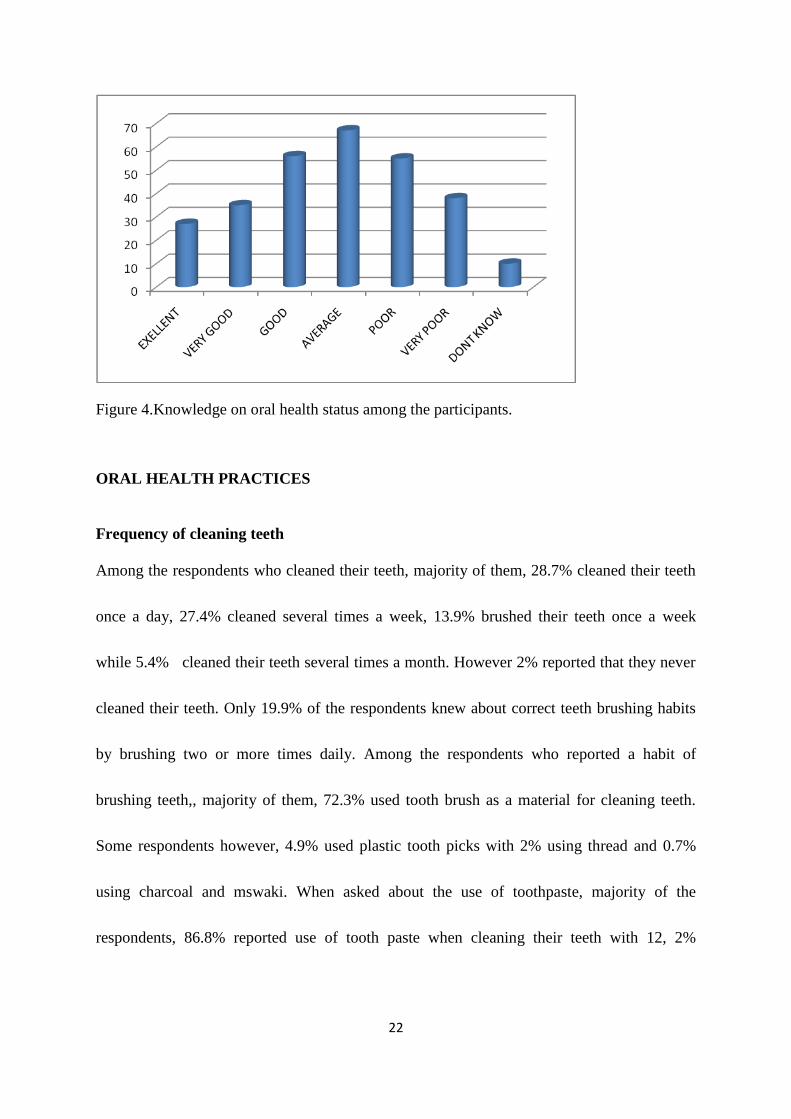
Knowledge on the heath of teeth and gums.
Regarding the knowledge on their state of teeth and gums, 23.35 of the respondents thought it
was average, 19.4% good, 12.2% very good, 9.4% excellent. However some respondents,
13.2% thought that their health was poor while 3.5% did not know about their oral health
status.
22
Figure 4.Knowledge on oral health status among the participants.
ORAL HEALTH PRACTICES
Frequency of cleaning teeth
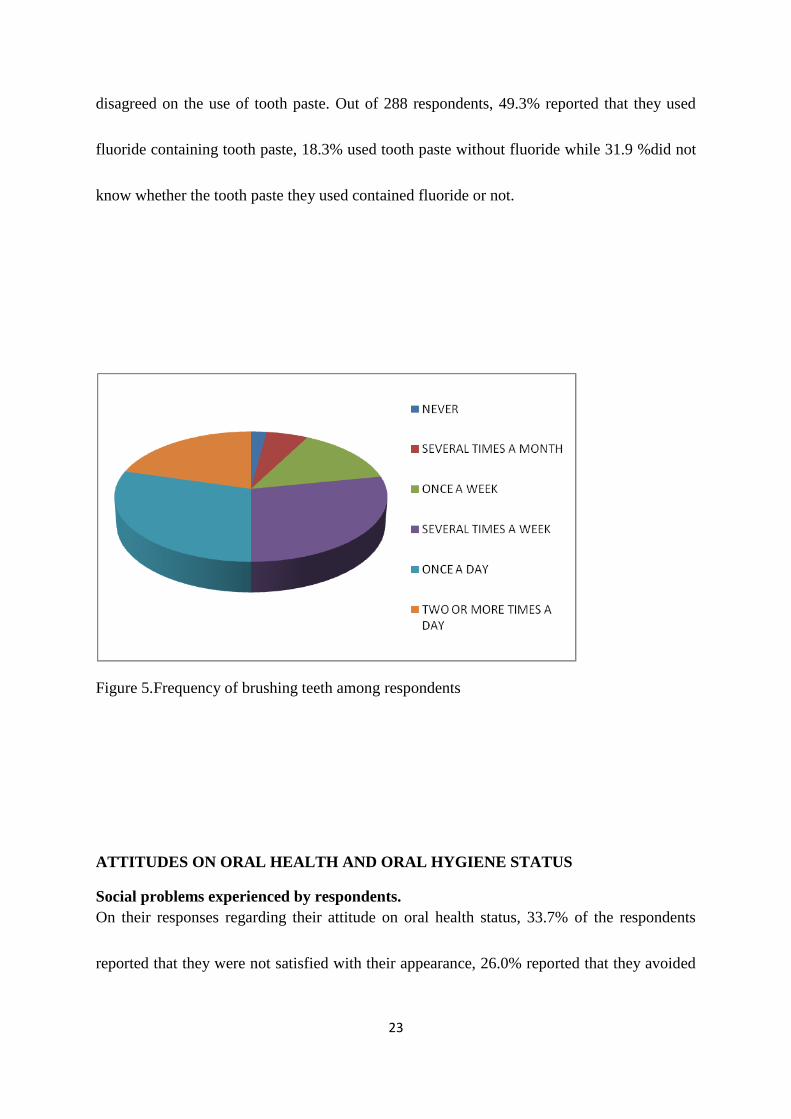
Among the respondents who cleaned their teeth, majority of them, 28.7% cleaned their teeth
once a day, 27.4% cleaned several times a week, 13.9% brushed their teeth once a week
while 5.4% cleaned their teeth several times a month. However 2% reported that they never
cleaned their teeth. Only 19.9% of the respondents knew about correct teeth brushing habits
by brushing two or more times daily. Among the respondents who reported a habit of
brushing teeth,, majority of them, 72.3% used tooth brush as a material for cleaning teeth.
Some respondents however, 4.9% used plastic tooth picks with 2% using thread and 0.7%
using charcoal and mswaki. When asked about the use of toothpaste, majority of the
respondents, 86.8% reported use of tooth paste when cleaning their teeth with 12, 2%
23
disagreed on the use of tooth paste. Out of 288 respondents, 49.3% reported that they used
fluoride containing tooth paste, 18.3% used tooth paste without fluoride while 31.9 %did not
know whether the tooth paste they used contained fluoride or not.
Figure 5.Frequency of brushing teeth among respondents
ATTITUDES ON ORAL HEALTH AND ORAL HYGIENE STATUS
Social problems experienced by respondents.
On their responses regarding their attitude on oral health status, 33.7% of the respondents
reported that they were not satisfied with their appearance, 26.0% reported that they avoided

24
smiling because of their teeth, 25.7% had a problem with their self esteem because other
children made fun of their teeth, 8.3% had a problem with biting hard foods while 4.7%
reported difficulty in chewing hard foods.
Figure 6. Distribution of social problems experienced by respondent
Dental problems experienced for the past 12 months
Regarding toothache experienced in the past 12 months, 29.9% of the respondents reported
that they had not experienced toothache,18.28% had experienced oftenly,16.7 %had rarely
experienced toothache while 14.6% had occasionally experienced pain a tooth.However,16%
did not know whether they had experienced toothache or not.

25
Figure 7. Dental problems experienced by respondents for the past 12 months
Reason for dental visit
Regarding reasons for dental visit. 64.6% of the respondents reported that they went to see a
dentist because something was wrong, 20.8% visited as part of follow up treatment while
4.2% reported that they did not remember the reason for visiting a dentist.

26
Figure 8. Reason for dental visit for the past 12 months
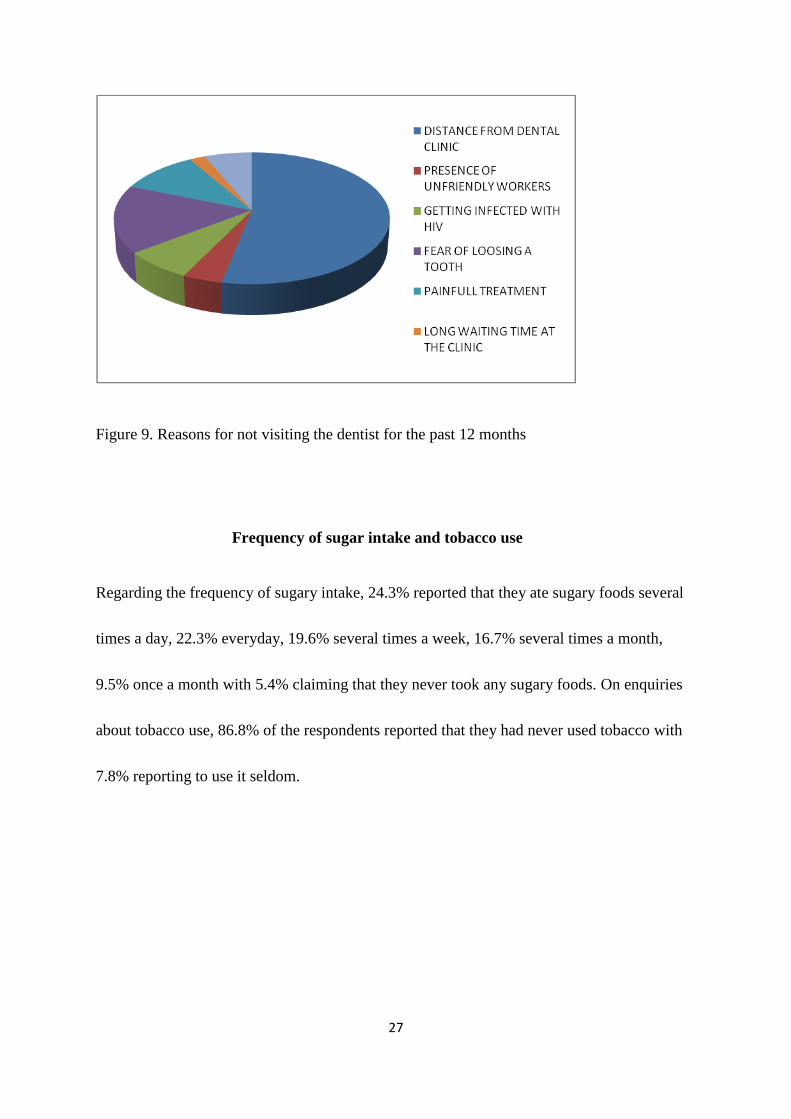
Reasons for not visiting the dentist
Out of the respondents who reported that they had not been to a dentist, 53.1% of them was
because of the distance from the dental clinic, 16.7% had fear of losing a tooth as the main
reason for not visiting a dentist, 10.45% had fear of painful treatment, 6.3% said that
treatment was very costly and hence could not visit a dentist. In addition, 7.3% feared
infection with HIV while 2.7% did not visit a dentist because of presence of unfriendly
workers.
27
Figure 9. Reasons for not visiting the dentist for the past 12 months
Frequency of sugar intake and tobacco use
Regarding the frequency of sugary intake, 24.3% reported that they ate sugary foods several
times a day, 22.3% everyday, 19.6% several times a week, 16.7% several times a month,
9.5% once a month with 5.4% claiming that they never took any sugary foods. On enquiries
about tobacco use, 86.8% of the respondents reported that they had never used tobacco with
7.8% reporting to use it seldom.

28
CHAPTER 5
5.1 DISCUSSION
Part A .Oral health status
A total of 127 secondary school students with an age range of 14-21 and a mean age of 17.10
years participated in the study. Females were slightly more 64 (50.4%) than males63
(49.6%).Majority of the students belonged to the 14-17 years age group. In a similar study
done in Tanga Tanzania to assess knowledge, attitudes and oral health practices among
secondary school students, a total of 785 secondary school students with an age group of 14-
22 years and mean age of 16.9 years participated in the study. There was a similarity with the
demographic values with females being slightly more (50.3%) than males (49.8%).In another
study done in Kuching in Malasya,results showed that there was no significant difference in
oral health knowledge between genders(p=0.03).
According to this study, the prevalence of dental caries was 50%.This paralleled a study done
among school children in Zimbabwe with caries experience reported to be 59% though this
was slightly higher than similar studies done in Kenya. This is attributed to consumption of
high-sugar containing products and inadequate oral health practices like mechanical plaque
control during brushing. In addition, the high numbers of untreated teeth may be as a result of
low priority placed on oral health care compared with other needs. In a study documented in
the international dental journal done to assess major oral diseases affecting children in Kenya,
the prevalence of dental caries was reported to be 39.1% with no filled teeth while the Dmft
was 1.51± 2.2550 with a decayed component of 1.48 .This was relatively lower with what
was reported in this study (2.52+2.5) with a decayed component of 1.70.In addition, the filled
component of Dmft was very low. This could be attributed to low dental care awareness,
inaccessibility to dental health care facilities and expensive restorative treatment with the
commonest mode of treatment being extractions giving a high rise in the missed component
of Dmft.
The prevalence of gingival inflammation in this study was 30.4%.This low compared with a
study done in Kitale among 12 year old children which reported a prevalence of 77%.The
difference could be attributed to higher level of knowledge on health with better practices
among secondary school students as compared to 12 year old children. There was no
significant difference between males and females with gingival inflammation.
29
The report of this study showed that 48.03% of the students had flourosis. Dental flourosis
was equally distributed among students from both schools. This parallels with a study done to
assess dental caries, flourosis and periodontal status among children in Juja rural area in
Kenya which reported a prevalence of 50%.The older age group (17-21years) were more
affected than the younger age group (14-16years).This is consistent with a study carried out
in Northern hilly state of India where it was observed that the prevalence of dental flourosis
had a linear relationship with the increasing age. Prevalence and severity of flourosis with
respect to gender showed no statistically significant difference. High flourosis prevalence is
hypothesized to high levels of fluoride in Rift valley springs and rivers in Laikipia County.
According to the report in this study, the prevalence of oral mucosa condition was 6.29%
with traumatic ulceration being ranked the most common (100%). In a study done in Kenya
in the prevalence of oral mucosal lesions, the results were consistent with the ones of this
study with females being affected more (3.9%) than males (2.36%) in the younger age group.
However, there was a difference in the most common lesion with hyperkeratosis being ranked
first in Kenya (26%).
Part B. Oral health knowledge, attitudes and practices
288 students were recruited in the study and filled questionnaires. 98% of the participants
brushed their teeth with only 19.9% brushing at least twice a day..This was consistent with a
similar study done in UasinGishu district where 92% of the students claimed they brushed
their teeth with about 48% brushing at least twice daily. In this study, use of tooth paste was
reported by 86.8% compared to the study done in UasinGishu where only 38.6% of the
participants reported to use tooth paste when brushing teeth. This could be attributed to a
higher social economical status among students in Laikipia County compared to UasinGishu
where only a few students could afford toothpaste. Majority of students in this study (72.3%)
used tooth brush as the commonest mode of brushing teeth. This was contrary with findings
from another study done in Tanzania and Nigeria where plastic toothbrushes were commonly
used and preferred to the wooden tooth brush (mswaki). The use of the plastic toothbrush by
students in this study may be related to the purpose of one wanting to be modern. However,
the reported use of charcoal and salt by few participants (0.7%) could be related to
socioeconomic factors of parents or traditional beliefs that they assist in improving ones oral
health status.

30
5.2 CONCLUSION
The prevalence of dental caries was 50.0% while the Dmft overall was 2.52 with a decay
component of 2.52+2.5. The commonest mode of treatment was dental exactions for those
who attended clinic. Gingival inflammation was observed in 30.4% of the students examined.
The prevalence of flourosis in this population was reported to be 48.03% with with mucosal
lesions being reported to be 6.29%.Majority of the students had knowledge on their oral
health status. Most of the students however did not carry out good oral hygiene practices and
only visited the dentist when in pain. Majority of the students who had never visited a dentist
reported that it was due to long distance to the dental clinic. Most of the students had sugary
foods in their diet at least once a day and a few students used tobacco.
5.3 RECOMMENDATIOS
1. Establishment of oral health education programmes in the school curriculum that will
be aimed at educating students on oral hygiene practice measures. Emphasis on the
importance of regular dental visits as part of preventive measures against diseases like
dental caries which lead to early tooth loss which in turn will lead to malocclusion.
2. Emphasis on the importance of regular dental visits as part of preventive measures of
diseases like dental caries that lead to early tooth loss which will in turn lead to
malocclusion.

31
REFERENCES
1. Akrebs, W. A. Effects of dental flossing and tooth brushing on gingival bleeding. Journal of
Periodontology , (2006). 1386-91.
2.J.T, K. Oral hygiene habits and dental health awareness of kenyan school children aged 9-15 years.
East African Medical Juornal ,(1993). 67-70.
3.Alev Aksoy Dogan.Michaud Dental University.Oral heath status of school going children. Journal of
Oral Science, (2010). 2177-184 .
4.PE, A. T. Oral situation of school children, mothers and school teachers in Saudi Arabia.
International journal of dentistr,. (2002). 168-7.
5.Wandera M, T. T. Baseline survey of oral health awareness of Kenyan school children in Uganda.
Africa Health Science , (2003). 19-22.
6.OkemwA K .A, Gatongi P.M, and J. K. Rotich, The oral health knowledge and oral hygiene practices
among primary school children age 5–17 years in a rural area of UasinGishu district, Kenya, East
African Journal of Public Health, (2010). 187–190,.
7. KahabukaF.K and MbawalH.S, Oral health knowledge and practices among Dar es Salaam
institutionalized former street children aged 7–16 years, International Journal of Dental
Hygiene, (2006). 174–178.
8. Nalweyiso Robinson PG, N, Busingye J, Whitworth J. Subjective impacts of dental caries and
flourosis in rural Ugandan children. Community Dent Health,(2005) .22-231
32
Appendix I
QUESTIONNARE Modified from WHO.
First I would like you to answer some questions concerning yourself and
your teeth
1. cccccclaq
FORM: 1 2 3 4 SEX: Boy Girl
2.
How old are you today? (Years)
3.
How would you describe the health of your teeth and gums?
Teeth Gums
Excellent .................................................................................................... 1
Very good .................................................................................................... 2
Good .................................................................................................... 3
Average .................................................................................................... 4
Poor .................................................................................................... 5
Very poor .................................................................................................... 6
Don't know .................................................................................................... 9
4.
How often during the past 12 months did you have toothache or feel discomfort on account of your
teeth?
Often 1
Occasionally 2
Rarely 3
Never 4
Don't know 9

33
5.
How often did you go to the dentist during the last 12 months? (Including orthodontist) (Tick one alternative only)
Once 1
Twice ............................................................................................................ 2
Three times ................................................................................................... 3
Four times .................................................................................................... 4
More than four times .................................................................................... 5
I had no visit to dentist during the last 12 months ........................................ 6
I have never received dental care/visited a dentist ....................................... 7
I don't know/don't remember ........................................................................ 9
If you did not visit the dentist during the last 12 months, go on to question 7
6.
What was the reason of your last visit to the dentist? (Tick one alternative only)
Something was wrong/pain or troubles with teeth or gums ......................... 1
It was part of follow-up treatment ................................................................ 2
It was part of follow-up treatment ................................................................ 2
I don't know/don't remember ........................................................................ 9
7. If you have not visited a dentist for the last one-year, what are the reasons?(multiple answers are not
allowed)
Distance from the dental clinic ..................................................................... 1
Presence of unfriendly dental workers ......................................................... 2
Getting infected with HIV ............................................................................ 3
Fear of losing a tooth ........................................................................................ 4
Painful treatment ......................................................................................... 5
Long waiting time at the clinic ..................................................................... 6
Treatment too costly ..................................................................................... 7
Painful treatment .......................................................................................... 8
Others specify………………………………………………………………….
8.
How often do you clean your teeth? (Tick one alternative only)
Never ............................................................................................................ 1
Several times a month (2-3 times) ................................................................ 2
Once a week ................................................................................................. 3
34
Several times a week (2-6 times) ................................................................. 4
Once a day .................................................................................................... 5
2 or more times a day ................................................................................... 6
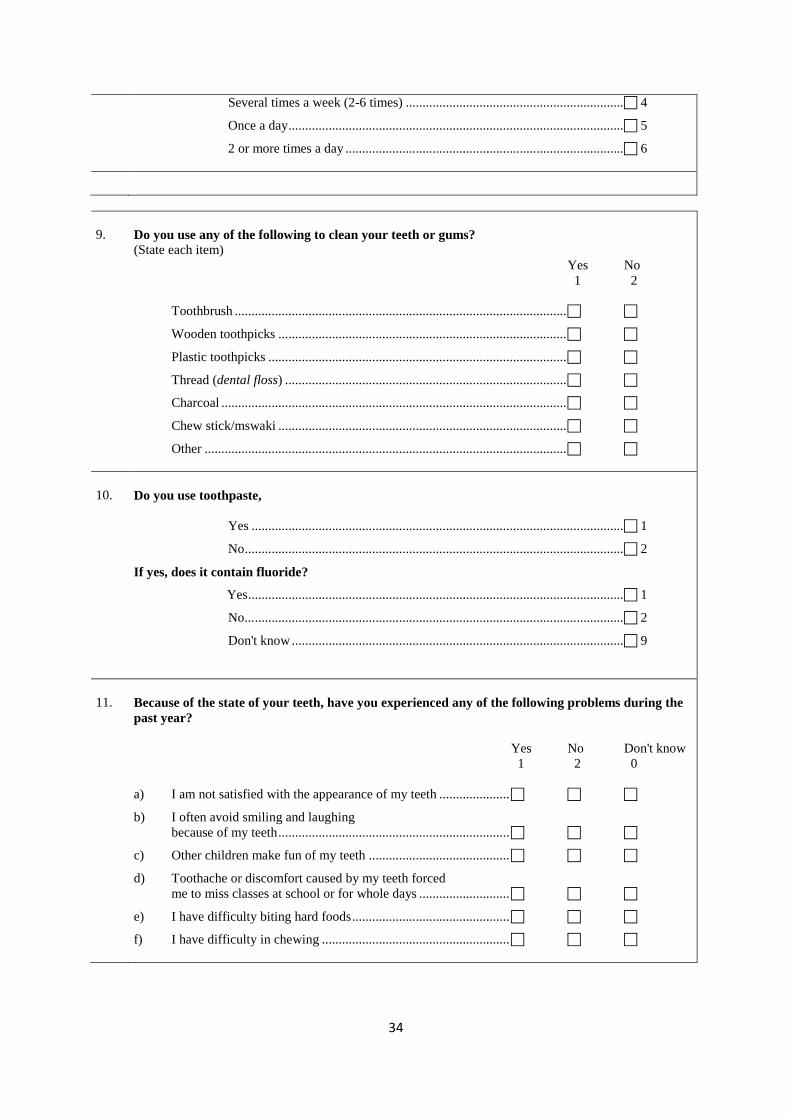
9.
Do you use any of the following to clean your teeth or gums?
(State each item)
Yes No
1 2
Toothbrush ...................................................................................................
Wooden toothpicks ......................................................................................
Plastic toothpicks .........................................................................................
Thread (dental floss) ....................................................................................
Charcoal .......................................................................................................
Chew stick/mswaki ......................................................................................
Other ............................................................................................................
10.
Do you use toothpaste,
Yes ............................................................................................................... 1
No ................................................................................................................. 2
If yes, does it contain fluoride?
Yes ................................................................................................................ 1
No... .............................................................................................................. 2
Don't know ................................................................................................... 9
11.
Because of the state of your teeth, have you experienced any of the following problems during the
past year?
Yes No Don't know
1 2 0
a) I am not satisfied with the appearance of my teeth .....................
b) I often avoid smiling and laughing
because of my teeth .....................................................................
c) Other children make fun of my teeth ..........................................
d) Toothache or discomfort caused by my teeth forced
me to miss classes at school or for whole days ...........................
e) I have difficulty biting hard foods ...............................................
f) I have difficulty in chewing ........................................................
35
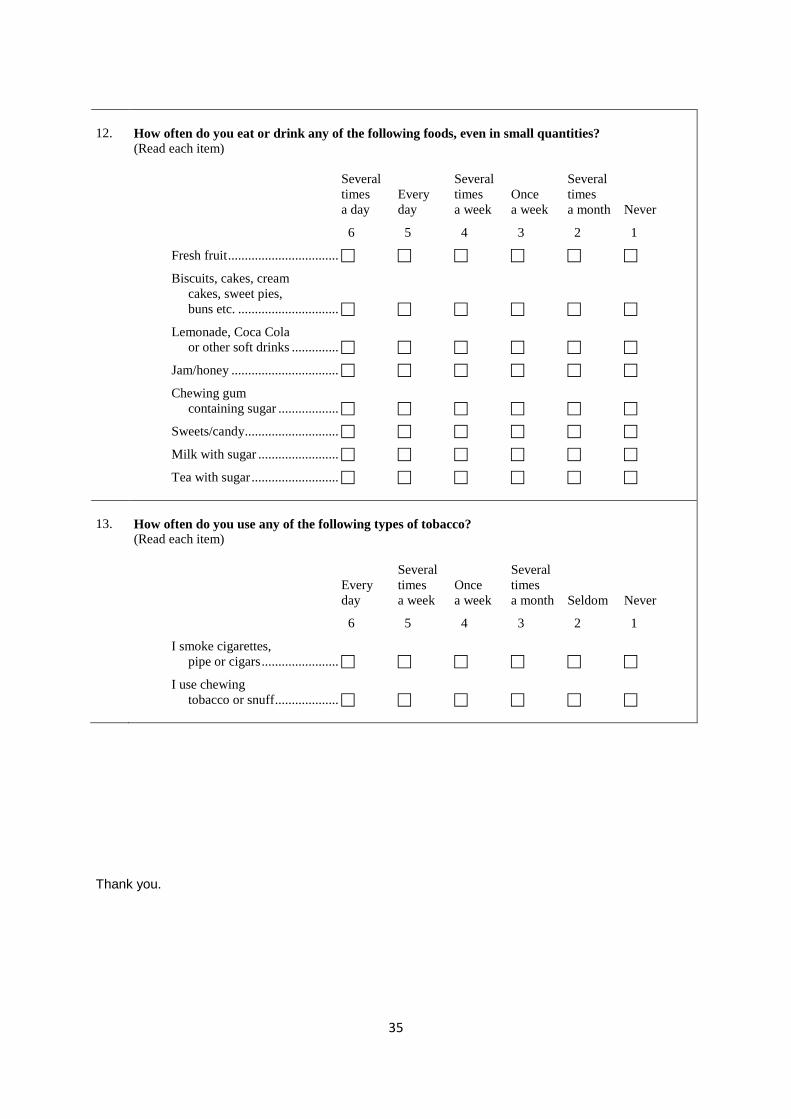
12.
How often do you eat or drink any of the following foods, even in small quantities? (Read each item)
Several Several Several
times Every times Once times
a day day a week a week a month Never
6 5 4 3 2 1
Fresh fruit .................................
Biscuits, cakes, cream
cakes, sweet pies,
buns etc. ..............................
Lemonade, Coca Cola
or other soft drinks ..............
Jam/honey ................................
Chewing gum
containing sugar ..................
Sweets/candy ............................
Milk with sugar ........................
Tea with sugar ..........................
13.
How often do you use any of the following types of tobacco? (Read each item)
Several Several
Every times Once times
day a week a week a month Seldom Never
6 5 4 3 2 1
I smoke cigarettes,
pipe or cigars .......................
I use chewing
tobacco or snuff ...................
Thank you.

36
Appendix II
KNOWLEDGE,ATTITUDES AND ORAL HEALTH PRACTICES AMONG
STUDENTS IN TWO SECONDARY SCHOOLS IN LAIKIPIA COUNTY.
LETTER TO THE PRINCIPAL.
I am a third year undergraduate dental student at the University of Nairobi, School of Dental
Sciences. I request you to allow me to use the students in your school in a study that will
form part of my degree work. The study will include filling out a questionnaire and an
intraoral examination. Only the students who consent will participate in the study. There will
be no material gain after participation in the study and the results will be used for research
purposes only and no invasive procedure will be undertaken on the students. Your permission
and their participation will be highly appreciated.
Yours sincerely
Ndaigah Serah
37
Appendix III
STUDENTS CONSENT FORM
I am a third year undergraduate dental student at the University of Nairobi, School of Dental
Sciences. Am carrying out a study on oral health knowledge, attitudes and practices among
two secondary schools in Laikipia County. I request you to take part in a study that will form
part of my degree work. The study will include filling out a questionnaire and an intraoral
examination. Only the students who consent will participate in the study. . I will assist all the
students in filling the questionnaire. Intraoral examination will be carried out using sterile
instruments and gloves will be used for every student. There will be no material gain after
participation in the study and the results will be used for research purposes only and no
invasive procedure will be undertaken on the students
CONSENT STATEMENT.
I do hereby freely consent to take part in the study. The procedure has been explained to me
and I understand that no harm will be caused to me and there will be no material gain from
the study. Also, I can withdraw participation at any time without any harm. Am informed and
understand that all the information gathered from me will be treated with utmost
confidentiality.
Signed………………….. Date……………………..
STUDENT

38
Appendix IV
Clinical examination form (Modified from WHO)
Country Year Month Day
Identification Examiner
(1) (4) (5) (6) (7) (10) (11) (21) (22)
GENERAL INFORMATION Name: OTHER DATA (Specify and
Provide codes)
Age in years (23) (24) No. years in school (28) (29) (31)
Sex (M = 1, F = 2) (25) (32)
Ethnic group (26)
Occupation (27) (33)
ORAL MUCOSA
CONDITION 0 = No abnormal condition
1 = Malignant tumour (oral cancer)
2 = Leukoplakia 3 = Lichen planus
4 = Ulceration (aphitous, herpetic, traumatic) 5 = Acute necrotizing gingivitis
6 = Candidiasis
7 = Abscess 8 = Other condition (specify if possible) .................................
9 = Not recorded
DENTITION STATUS
55 54 53 52 51 61 62 63 64 65
18 17 16 15 14 13 12 11 21 22 23 24 25 26 27 28
Crown (40) (55)
(56) (71)
Root
85 84 83 82 81 71 72 73 74 75
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38 Crown
(72) (87)
(88) (103)
(34) (37)
(35) (38)
(36) (39)
LOCATION
0 = Vermillion border
1 = Commissures
2 = Lips
3 = Sulci
4 = Buccal mucosa
5 = Floor of mouth
6 = Tongue
7 = Hard and/or soft palate
8 = Alveolar ridges/gingiva
9 = Not recorded Primary Permanent
Teeth teeth
Crown Crown/Root Status
A 0 0 Sound
B 1 1 Decayed
C 2 2 Filled, with decay
D 3 3 Filled, no decay
E 4 – Missing, as a
Result of caries
– 5 – Missing, any other
reason
39
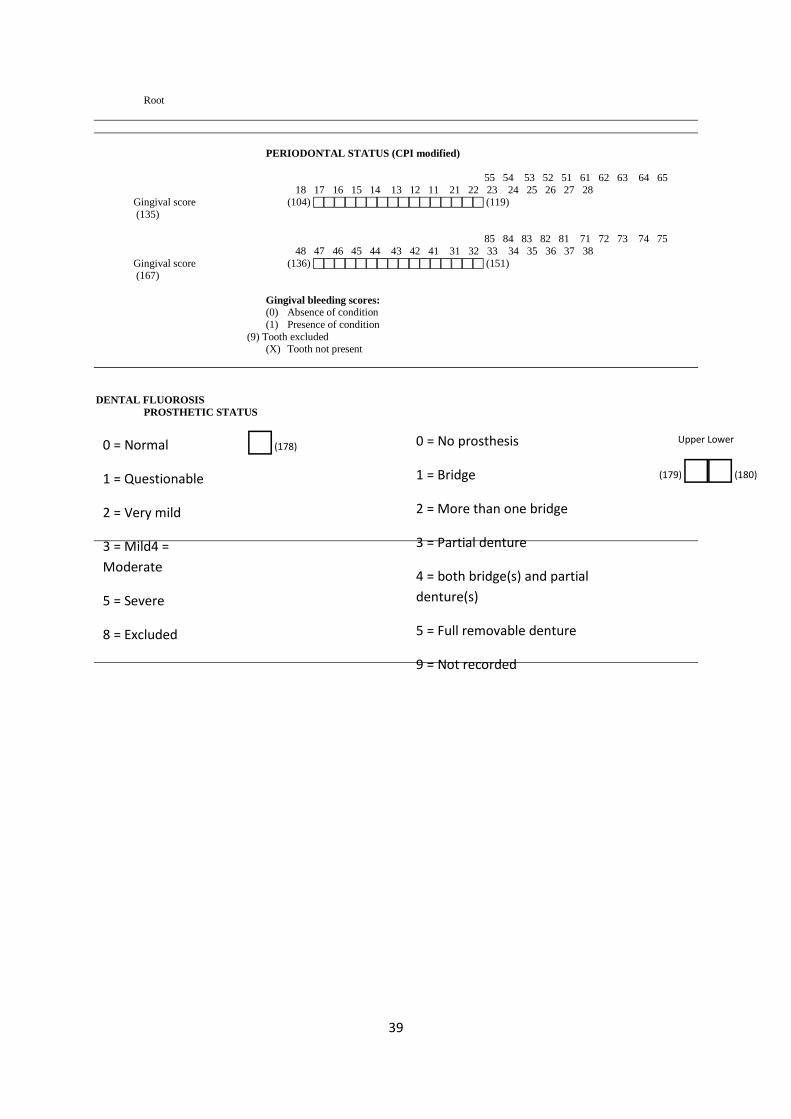
Root
PERIODONTAL STATUS (CPI modified)
55 54 53 52 51 61 62 63 64 65
18 17 16 15 14 13 12 11 21 22 23 24 25 26 27 28 Gingival score (104) (119)
(135)
85 84 83 82 81 71 72 73 74 75
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38
Gingival score (136) (151) (167)
Gingival bleeding scores:
(0) Absence of condition
(1) Presence of condition
(9) Tooth excluded (X) Tooth not present
DENTAL FLUOROSIS
PROSTHETIC STATUS
0 = Normal
1 = Questionable
2 = Very mild
3 = Mild4 =
Moderate
5 = Severe
8 = Excluded
9 = Not recorded
(178)
0 = No prosthesis
1 = Bridge
2 = More than one bridge
3 = Partial denture
4 = both bridge(s) and partial
denture(s)
5 = Full removable denture
9 = Not recorded
Upper Lower
(179) (180)

40