optimising the contribution of the queensland nursing ... · profession in intelligent debate ......
TRANSCRIPT
Optimising the contribution of the
Queensland nursing workforce

• Setting the scene – realising nursing potential
• Living with uncertainty
• Working to “full scope”
• NMBA Professional Practice Framework –
supporting your nursing practice
• “Ladies and gentlemen, our challenge is this:
• To learn from our history and not make the mistakes of the past when
there is a future out there with nothing but promise...
• To think clearly about the practice of the profession and how it fits with
the world’s realities …
• To question all that we take for granted about the way things are and
propose the way things ought to be because there’s nothing stopping
us..
• …A quote from Mark Twain
• “Do what is right. It will please some people and astonish the rest”
• The late Donna Diers, Professor Emerita, Yale University
• “Speaking of Nursing”, 2004, p.112
• I am convinced that we face a set of unavoidable crises which are already visible to those who care to look beyond the dominant headlines.
• These crises are due to our past successes rather than our failures.
• We have achieved what we wanted to.
• We have, unfortunately so far failed to recognize that it is now time to move on and to seize the new opportunities which are currently available to us.
• We urgently need to rework our concepts of success.
• (Robert Theobald, 1998)
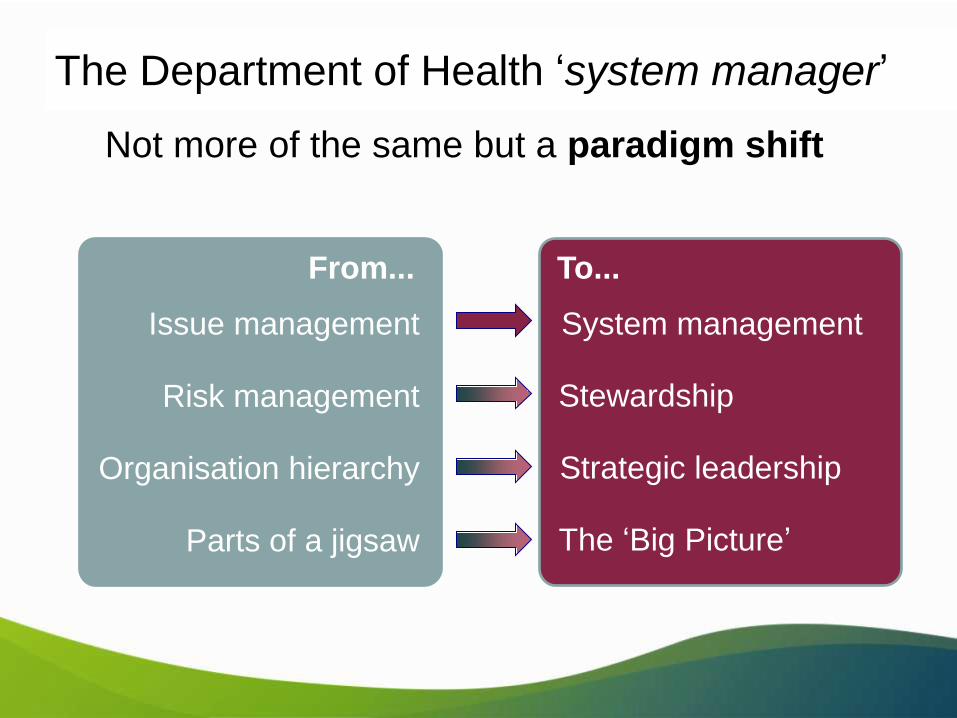
Issue management System management
From... To...
Not more of the same but a paradigm shift
The Department of Health ‘system manager’
Risk management Stewardship
Organisation hierarchy Strategic leadership
Parts of a jigsaw The ‘Big Picture’

The potential for nursing – why now ?
•Times of great uncertainty are also times of great potential
•Your government already has it’s blueprint out there and much of its focus is on work that is properly and appropriately nursing work
•Primary health care (not primary care) is a key strategic focus
•Working to full scope is not only mooted but committed to
•“clinicians need to work to their full scope of practice. We will challenge the “myths” of what is possible and be open to new ways of working and
models of care” (p.27)
•Note it says “full scope”.
•This is extremely positive. In many areas nurses and midwives have been unable to practise to full scope. This is a great opportunity to demonstrate just what we can do.
International comparison and contexts
•Canadian Nurses’ Association (CNA) National Expert Commission on Nursing (2012)
•Expert Commission had non-nursing co-chairs and was made up of leaders in nursing, medicine, business, law, academia, economics and health policy.
•Commission toured the country and took electronic and written submissions asking the Canadian public what was their vision and needs for health care and what role they saw nurses playing in that vision
•The Canadian public’s three goals for a transformed health care system are:
•“To move beyond episodic, urgent and emergency acute care models to provide accessible, integrated health –related services and programs;
•To base it on a foundation of patient- and family-centred primary health care, accessible, as much as possible, in the home and community; and
•To ensure quality by using the most up-to-date technology, evidence, clinical guidelines and best practices” (CNA, p.27)
Models of care to effectively meeting Canadian needs should ....
•Be centred on what individuals and families need, rather than how providers and organisations want to function
•Treat the individual as a whole person, part of a family and a community, not just a collection of body parts and problems
•Broaden the health –care systems beyond hospitals and other institutions to offer care in the community and at home
•Address social, economic, environmental and indigenous determinants of health –especially poverty, housing, food insecurity and social exclusion – that play such major roles in determining our individual health
•Draw upon the progress made in Canada to develop public health and population –based policies and programs to ensure the greatest possible health outcomes for all Canadians
•Ensure all health professionals, including nurses, work to their full scope of practice
•Be financed from public health insurance and monitored for effectiveness and efficiency
•(CNA, 2012, p.7)

Ethos
of collective
non-
responsibility
Practice zone
of abrogation
Ethos of
Individual
accountability
Practice
zone of isolation
or alienation
Ethos of collegial
generosity
Practice zone of
mutual trust and
Collaboration
So how have we responded to challenges
in the past?
Chiarella, (2007)
• We are all responsible for our own practice
• When we see change coming towards us, doing nothing is a choice and every choice carries consequences
• When things take us by surprise we still have a choice - how we respond
• There is a real need to engage both the public and the profession in intelligent debate - but about healthcare, not about nursing
• This requires much stronger alliances with consumer groups than nurses have previously made
• We need to “get political” – not being interested in politics is a profoundly political act
Dealing with collective non-responsibility

• “Politics is the process and method of making decisions for
groups. Although it is generally applied to governments,
politics is also observed in all human group interactions
including corporate, academic, and religious.” (Wordnet,
Princeton)
• Big “P” Politics usually refers to the government of states
and other political units
• Small “p” politics usually refers to social relations involving
authority or power
Getting political –some definitions
• Decisions about health are made every day
• Nurses, being the single largest group in health, are impacted on by those decisions
• Therefore we need to be politically active in order to influence them
• Ministers need good advice
• Ministers’ diaries are full every day –with somebody giving them advice
• Ministers want to be re-elected –they don’t want to make mistakes
Why should we care about Big P politics?

• Because we are involved in them every single day
• Admittedly we can’t control everything that happens to us
• BUT…
• We can influence a lot of it
• AND
• We can certainly choose how we respond
• AND
• We can think how we might manage it better next time!
Why should we care about small p politics?
• Putting nursing issues into a wider perspective
• Learning to speak with authority
• Encouraging debate and strategy
• Encouraging political development
• Becoming policy entrepreneurs
Small p politics – skills for taking
responsibility
• We are already revisiting our models of practising nursing
• Imagining that nobody ever carries the burdens we carry can make us bitter and twisted
• That doesn’t help us but it also doesn’t help retention
• An investment in retention is an investment in the future of our own health care
• We only need to retain one nurse in every five not to have a 2025 shortage
• We need to see ourselves more clearly within the “systems” issues in health
Dealing with the isolation of individual
accountability
• Recognition that no-one professional group has a monopoly on safety or care
• An understanding that scope of practice is not defined by tasks
• Informed collaborative national debate on health resource distribution
• A greater sense of public-professional partnerships in health care
• Improved projections for future health demographics and needs
• Better access to informed debate
Creating collegial generosity
• To work to full scope you need to understand your professional practice
framework that has been endorsed by the Nursing and Midwifery Board
of Australia
• This includes:
• The competency standards for registered nurses
• The Code of Conduct for nurses in Australia
• The Code of Ethics for nurses in Australia
• The registration standards, especially PII, CPD and RoP
• The decision –making framework for nurses (DMF)
• The professional boundaries advice for nurses
• The mandatory notification scheme under the National Law
• http://www.nursingmidwiferyboard.gov.au/
Working to “full scope”
• The registered nurse demonstrates competence in the provision of
nursing care as specified by registration requirements, National Board
standards and codes, educational preparation, relevant legislation and
context of care.
• The registered nurse practises independently and interdependently,
assuming accountability and responsibility for their own actions and
delegation of care to enrolled nurses and health care workers.
• Delegation takes into consideration the education and training of
enrolled nurses and health care workers and the context of care.
(NMBA/ ANMC, 2006)
Description of the registered nurse on
entry to practice
• The registered nurse provides evidence-based nursing care to people of
all ages and cultural groups, including individuals, families and
communities.
• The role of the registered nurse includes promotion and maintenance of
health and prevention of illness for individuals with physical or mental
illness, disabilities and/or rehabilitation needs, as well as alleviation of
pain and suffering at the end stage of life.
• The registered nurse assesses, plans, implements and evaluates
nursing care in collaboration with individuals and the multidisciplinary
health care team so as to achieve goals and health outcomes.
• The registered nurse recognises that ethnicity, culture, gender, spiritual
values, sexuality, age, disability and economic and social factors have
an impact
• (NMBA/ ANMC, 2006)
• The national competency standards for the registered nurse are the core
competency standards by which your performance is assessed to obtain and
retain your registration as a registered nurse in Australia.
• As a registered nurse, these core competency standards provide you with the
framework for assessing your competence, and are used by the National Board
to assess competence as part of the annual renewal of registration, to assess
nurses:
– • educated overseas seeking to work in Australia
– • returning to work after breaks in service, or
– • involved in professional conduct matters.
• The National Board may also apply the competency standards in order to
communicate to consumers the standards that they can expect from nurses.
But they are not ONLY the standards for practice at entry
to the profession
• Professional practice
• Critical thinking and analysis
• Provision and coordination of care
• Collaborative and therapeutic practice
The domains of practice
• Relates to the coordination, organisation and provision
of nursing care that includes the assessment of individuals/
groups, planning, implementation and evaluation of care.
• 5. Conducts a comprehensive and systematic nursing
assessment
• 5.1 Uses a relevant evidence-based assessment framework
to collect data about the physical socio-cultural and mental
health of the individual/group:
• 5.2 Uses a range of assessment techniques to collect
relevant and accurate data:
• 5.3 Analyses and interprets assessment data accurately:
Provision and coordination of care
• 6. Plans nursing care in consultation with individuals/
groups, significant others and the interdisciplinary
health care team
• 6.1 Determines agreed priorities for resolving health
needs of individuals/groups:
• 6.2 Identifies expected and agreed individual/group health
outcomes including a time frame for achievement:
• 6.3 Documents a plan of care to achieve expected
outcomes:
• 6.4 Plans for continuity of care to achieve expected
outcomes

• 7. Provides comprehensive, safe and effective evidence-based nursing care to achieve identified individual/group health outcomes
• 7.1 Effectively manages the nursing care of individuals/ groups:
• 7.2 Provides nursing care according to the documented care or treatment plan:
• 7.3 Prioritises workload based on the individual/group’s needs, acuity and optimal time for intervention:
• 7.4 Responds effectively to unexpected or rapidly changing situations
• 7.5 Delegates aspects of care to others according to their competence and scope of practice
• 7.6 Provides effective and timely direction and supervision to ensure that delegated care is provided safely and accurately:
• 7.7 Educates individuals/groups to promote independence and control over their health
• 7.8 Uses health care resources effectively and efficiently to promote optimal nursing and health care

• 8. Evaluates progress towards expected
individual/group health outcomes in consultation with
individuals/groups, significant others and
interdisciplinary health care team
• 8.1 Determines progress of individuals/groups toward
planned outcomes:
• 8.2 Revises the plan of care and determines further
outcomes in accordance with evaluation data:

• 9. Establishes, maintains and appropriately concludes therapeutic
relationships
• 9.1 Establishes therapeutic relationships that are goal directed and recognises
professional boundaries:
• 9.2 Communicates effectively with individuals/groups to facilitate provision of
care
• 9.3 Uses appropriate strategies to promote an individual’s/ group’s self-esteem,
dignity, integrity and comfort:
• 9.4 Assists and supports individuals/groups to make informed health care
decisions
• 9.5 Facilitates a physical, psychosocial, cultural and spiritual environment
that promotes individual/group safety and security:
• 10. Collaborates with the interdisciplinary health care team to
provide comprehensive nursing care
• 10.1 Recognises that the membership and roles of health care teams
and service providers will vary depending on an individual’s/group’s
needs and health care setting:
• 10.2 Communicates nursing assessments and decisions to the
interdisciplinary health care team and other relevant service providers:
• 10.3 Facilitates coordination of care to achieve agreed health
outcomes
• procedures.
• 10.4 Collaborates with the health care team to inform policy and
guideline development
• The national decision-making framework, developed in the context of
national workforce strategies promoting diversity, flexibility and
responsiveness in the workforce, reflects a whole-of-health workforce
perspective.
• It consists of two parts.
• The first is a set of principles that form the foundation for the
development and evaluation of decision-making tools.
• The second contains two templates for decision-making tools, one for
nursing (registered and enrolled nurses) and one for midwifery, in
recognition of the differences between the two professions.
The decision making framework
• A profession’s scope of practice is the full spectrum of roles, of actions,
responsibilities, activities and decision-making capacity that individuals
within that profession are educated, competent and authorised to
perform.
• Some functions within the scope of practice of any profession may be
shared with other professions or other individuals or groups.
• The scope of practice of all health professions is influenced by the wider
environment, the specific setting,
• A national framework for the development of decision-making tools for
nursing and midwifery practice incorporates legislation, policy,
education, standards and the health needs of the population.
• The scope of practice of an individual is that which the individual is
educated, authorised and competent to perform.
Scope of practice

• The scope of practice of an individual nurse or midwife may
be more specifically defined than the scope of practice of
their profession.
• To practise within the full scope of practice of the profession
may require individuals to update or increase their
knowledge, skills or competence.
• Decisions about both the individual’s and the profession’s
practice can be guided by the use of decision-making tools.
• When making these decisions, nurses and midwives need
to consider their individual and their respective profession’s
scope of practice.
Decision-making tools:
• 1. guide nurses and midwives in making decisions about everyday
practice and changes to practice over time to meet the health needs of
the community
• 2. facilitate planning, negotiation and implementation of practice change
for individuals or groups of nurses and midwives to meet the health
needs of the community
• 3. acknowledge that the promotion and provision of quality health
services for individual consumers and for the broader community are
the drivers for change in practice
• 4. enhance safety and quality when integrated with a comprehensive
approach to managing risk
The national principles
Decision-making tools:
• 5. recognise and apply to all domains and contexts of practice
• 6. facilitate responsiveness to consumers’ needs by health workers through
changes to the repertoire of skills of individuals or groups by:
– • evolution of new practice areas/capabilities
– • negotiation among health workers and between health workers and
employers
– • making or accepting delegations.
• Decision-making tools:
• 7. acknowledge the following determinants of practice and how they may limit or
enable practice change:
– • legislated authority or restrictions on professional practice
– • professional standards of practice
– • evidence for practice
– • individual capability (knowledge, skill and competence) for practice
– • contextual/organisational support for practice
• 8. that are a part of the professional practice frameworks used by the National
Board and in the self assessment of practice, state explicitly and transparently
the role of the tools in circumstances where a nurse or midwife may be called to
account for their practice decisions.