optimal nutritional goals for the cancer...
TRANSCRIPT
Optimal Nutritional Goals for
the Cancer Survivor
W E N D Y D E M AR K - WAH N E F R I E D , P H D , R D
P R O F E S S O R AN D W E B B C H AI R O F N U T R I T I O N S C I E N C E S
AS S O C I AT E D I R E C T O R O F C AN C E R P R E V E N T I O N & C O N T R O L
U N I V E R S I T Y O F AL AB A M A AT B I R M I N G H AM
W O R K I N G E V E R Y D A Y T O P R O V I D E T H E H I G H E S T Q U A L I T Y O F L I F E F O R P E O P L E W I T H C A N C E R

Disclosures
AFFILIATION/FINANCIAL
INTERESTS
(prior 12 months)
CORPORATE
ORGANIZATION
Grants/Research Support: No
Corporate
Sponsorship
Scientific Advisory
Board/Consultant:
Speakers Bureau:
Stock Shareholder:
Other
Objectives By the end of this presentation, the observer should be able to…
• Recognize trends in cancer prevalence, mortality and survivorship.
• Identify common issues in cancer survivorship.
• Identify diet and physical activity guidelines for
cancer survivorship and outline the rationale that
supports them.
• List some of the gaps in knowledge related to
nutrition and cancer survivorship
• Identify reliable sources for nutrition and cancer
information.



Number of Cancer Survivors is Steadily
Rising Good News!
14.5 M!
Cancer Survivors at greater risk
- Progressive disease
- Second primaries
- Cardiovascular Disease
- Diabetes
- Osteoporosis
- Sarcopenia
- Functional decline
Cancer Survivorship:
The Bad News

% with Limitations:
Survivors vs. General Population
Hewitt, Rowland, Yancik. J Gerontol. 58:82, 2003

Possible Solutions
Diet Exercise
Depression
Fatigue
Adverse Body Composition
Functional Decline
Comorbidity
Recurrence Growing evidence Growing evidence
Possible benefit Probable benefit Convincing benefit

Cancer-Related Diet & Physical Activity
Recommendations
Rock et al. CA Cancer J Clin 2012; WCRF-AICR 2nd Expert Research Report, http://www.aicr.org
WCRF- AICR (2007) American Cancer Society (2012)
Weight Be as lean as possible without
becoming underweight
Achieve & maintain a healthy weight
Physical
Activity (PA)
Regular PA, >30 min/day Avoid inactivity; PA >150/week;
strength training 2 x week
Dietary
Pattern
Avoid sugary drinks. Limit
energy-dense foods (foods high
in sugar & fat, and low in fiber)
Eat more of a variety of
vegetables, fruits, whole grains
and legumes
Limit consumption of
processed & red meat
Diet High F&V & Whole Grains
• Choose foods & beverages in
amounts that achieve & maintain a
healthy weight
• Eat > 2.5 cups fruits & vegetables/day
• Whole vs. refined grains
• Limit consumption of processed & red
meat
Other Limit salty foods -
Alcohol If drink limit to 1-2 drinks/day If drink limit to 1-2 drinks/day
Supplements Do not use supplements to
protect against cancer

Weight Management & Energy
Balance
Anorexia/Cachexia
• Patients with select respiratory,
G.I. & childhood cancers
• Patients living with advanced
cancer
• Increasing weight to desired
range important for recovery,
well-being, functional status
• Diet & exercise key roles +/-
pharmacotherapy
Overweight/Obesity
• Risk factors for several
cancers, as well as cancer-
related mortality
• Increased weight at diagnosis
is a poor prognostic factor
• Weight gain common during &
after treatment–linked with co-
morbidity, functional decline &
maybe recurrent/progressive
CA
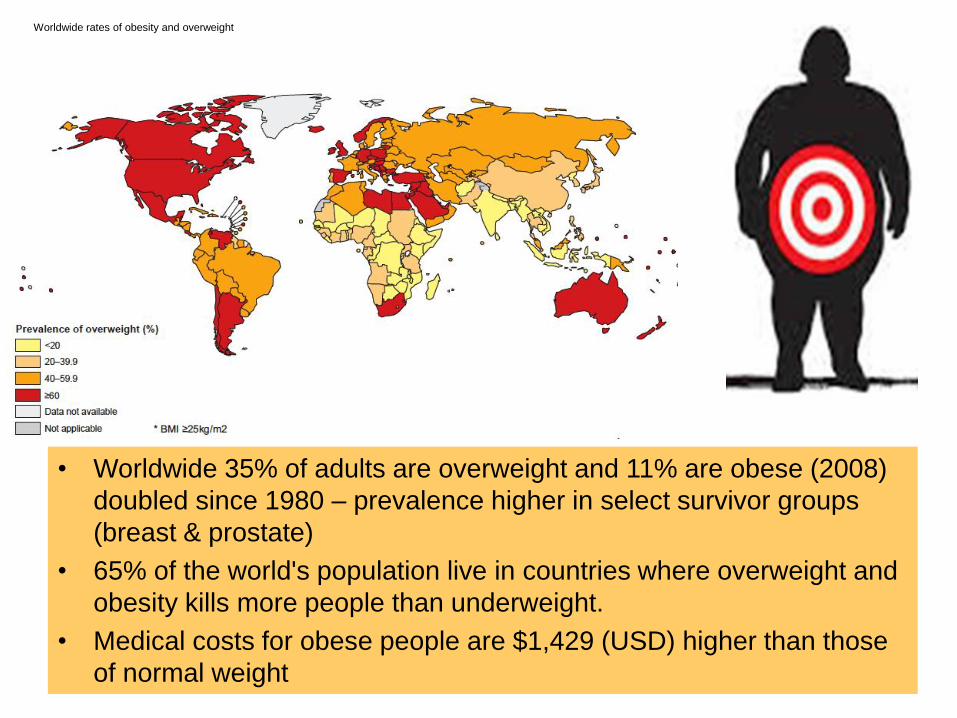
Worldwide rates of obesity and overweight
• Worldwide 35% of adults are overweight and 11% are obese (2008)
doubled since 1980 – prevalence higher in select survivor groups
(breast & prostate)
• 65% of the world's population live in countries where overweight and
obesity kills more people than underweight.
• Medical costs for obese people are $1,429 (USD) higher than those
of normal weight

Increases in Cancer Risk with Overweight & Obesity
0
20
40
60
80
100
120
140
160
Overweight Obesity
WHO: IARC 2002/WCRF –AICR 2007
Breast (post-menopause)
Colon Endometrium Kidney Pancreas Esophagus
Probable Evidence that Cancer of the Ovary & Gallbladder are Weight-Related
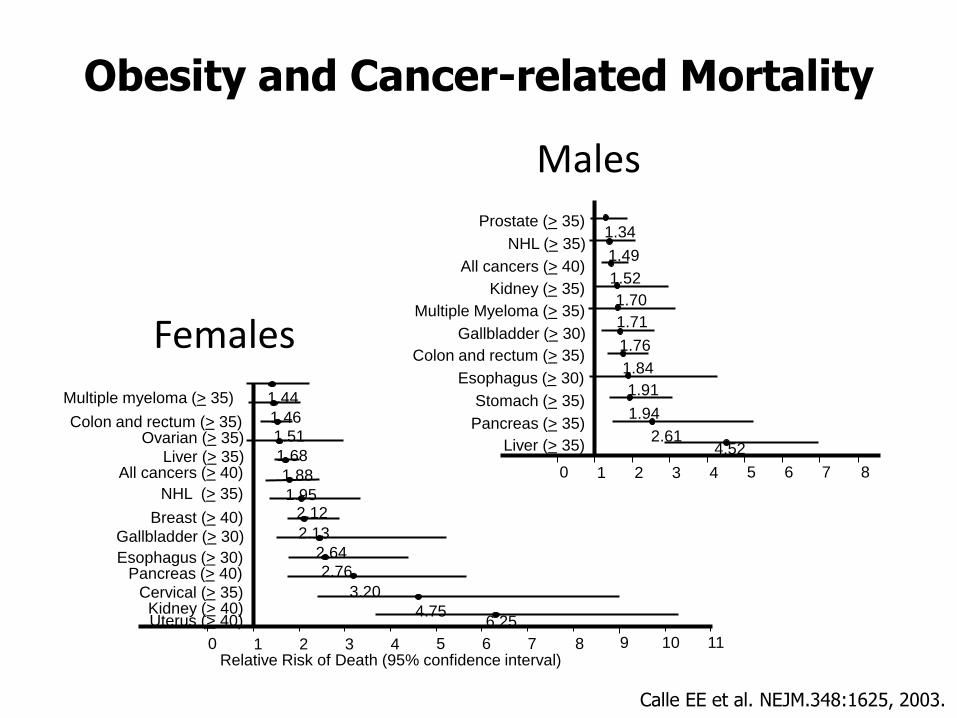
0 7 6 5 4 3 2 1 8
Prostate (> 35)
Multiple Myeloma (> 35)
Gallbladder (> 30)
Colon and rectum (> 35)
Esophagus (> 30)
Stomach (> 35)
Pancreas (> 35)
Liver (> 35)
NHL (> 35)
All cancers (> 40)
Kidney (> 35)
1.34
1.49
1.52
1.70
1.71
1.76
1.84
1.91
1.94
2.61 4.52
0 7 6 5 4 3 2 1 8 9 11 10
Multiple myeloma (> 35)
Colon and rectum (> 35)
Breast (> 40)
Gallbladder (> 30)
Esophagus (> 30) Pancreas (> 40)
Cervical (> 35) Kidney (> 40) Uterus (> 40)
Liver (> 35) All cancers (> 40)
NHL (> 35)
Ovarian (> 35)
1.44
1.46
1.51
1.68
1.88
1.95 2.12
2.13
2.64
2.76
3.20
4.75 6.25
Relative Risk of Death (95% confidence interval)
Obesity and Cancer-related Mortality
Females
Males
Calle EE et al. NEJM.348:1625, 2003.

Prognostic Effects of Weight Gain Among Individuals
with Breast and Prostate Cancer:
Results of 2 Meta-Analyses
Group
(year)
# of
studies
Sample RR (95% CI) for every 5 kg/m2
increase in BMI from pre- to
post-dx
Chan et
al. (2014)
82 213,075 women
with breast cancer
Breast CA Specific Mortality
1.29 (0.97-1.72)
Total Mortality
1.08 (1.01-1.15)
Cao & Ma
(2011)
6 cohort 18,203 men with
prostate cancer
Biochemical Recurrence
1.21 (1.11-1.31)
Prostate CA Specific Mortality
1.20 (0.99-1.46)
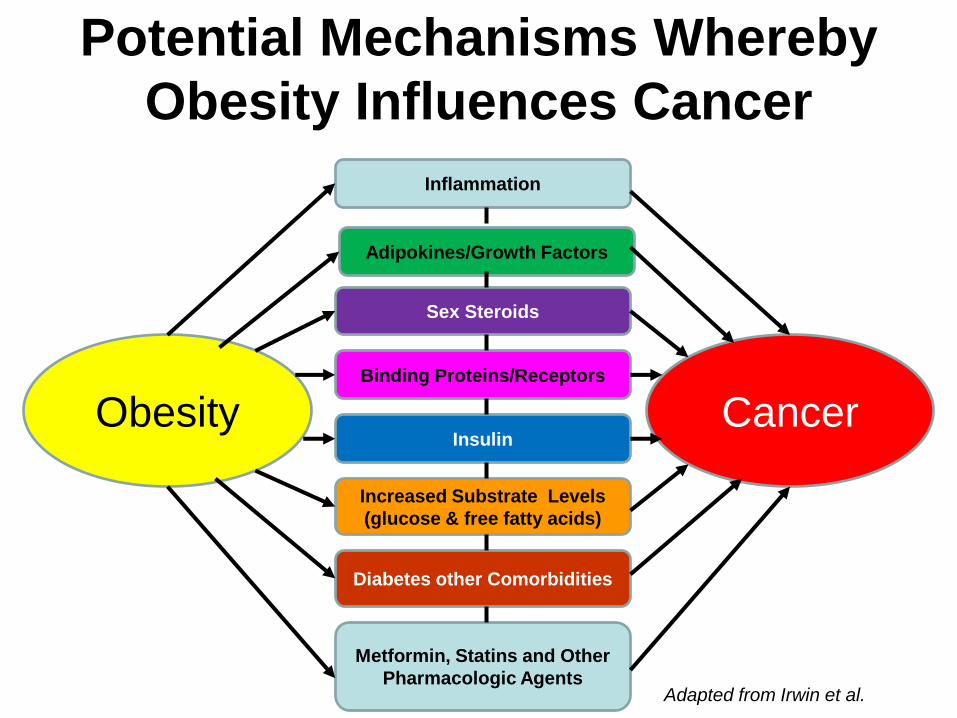
Potential Mechanisms Whereby
Obesity Influences Cancer
Obesity Cancer
Adipokines/Growth Factors
Inflammation
Sex Steroids
Insulin
Increased Substrate Levels
(glucose & free fatty acids)
Diabetes other Comorbidities
Binding Proteins/Receptors
Metformin, Statins and Other
Pharmacologic Agents Adapted from Irwin et al.

Weight Loss Interventions
• 1st trial de Waard 102 post-menopausal breast cancer survivors Europ J Cancer Prev 2:233, 1993
• 14 weight loss trials in breast cancer (2-18 months). No adverse events. 57% resulted in >5% loss of body weight. Clinically significant benefits in HbA1C, insulin, inflammatory markers, QoL, lipids, physical functioning and B/P with 5-9% weight loss.
• In field or in analysis SUCCESS-C pre/post breast cancer (n=1,400-1,600) 2-yrs, telephone counseling + mailed materials vs. mailed materials
LISA 336 post menopausal, telephone counseling + mailed materials vs. mailed materials
DIANA-5 pre/post breast cancer (n=1,417) 5-yrs, clinic-based vs. mailed materials
Choice 259 post menopausal – low CHO vs. low fat vs. control
ENERGY pre/post menopausal (N=692), Clinic based+ telephone counseling + mailed materials vs. standard care
Reeves M et al. Obesity Rev doi 10.1111/obr/12190 2014

Interest in Obesity & Cancer Increasing
IOM Workshop on Cancer Survival and Recurrence Oct 2011
2014 Nov 1;32(31):3568-74
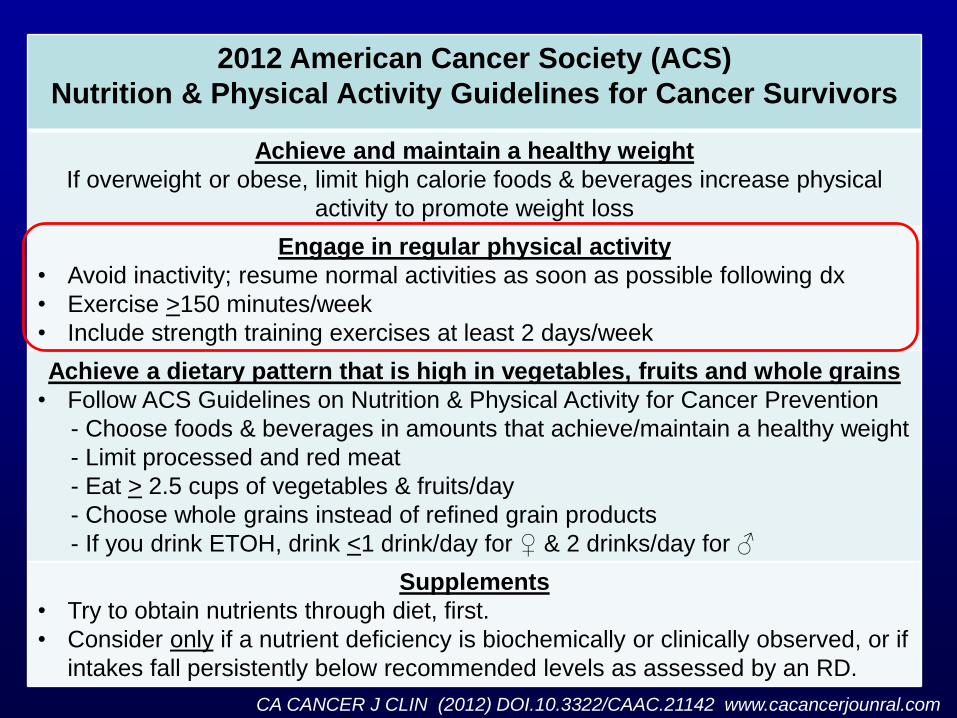
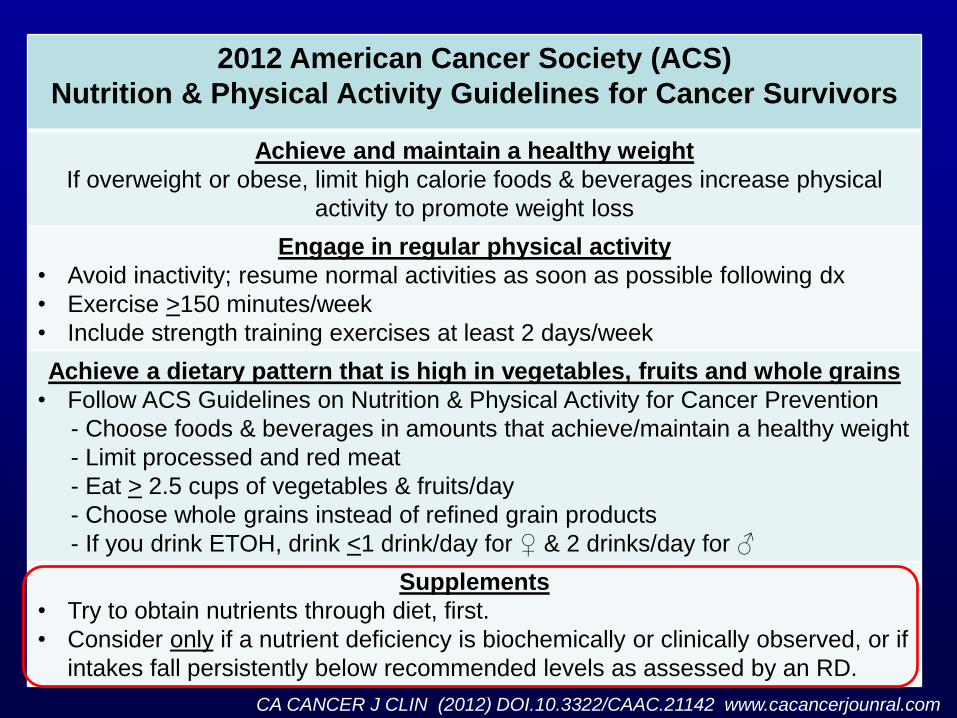
2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com

Cochrane Review: Exercise on Quality of Life Post-treatment
40 trials with 3694 participants Mishra et al. Cochrane Database Rev 2012
Outcome # studies/N Evidence Qual Positive effects
Overall QOL, <12 weeks 11/826 Low 0.48 (0.16-0.81)
Overall QOL, 6 mo 2/115 Moderate 0.46 (0.09-0.84)
Anxiety, <12 weeks 4/455 Low -0.26 (-0.4 to -0.07)
Emotional well being 8/632 Low 0.33 (0.05 to 0.61)
Fatigue, <12 weeks 10/745 Moderate -0.82 (-1.50 to -0.14)
Fatigue, 12 wks-6 mo 3/246 Low -0.42 (-0.83 to -0.02)
Pain, <12 weeks 4/289 Moderate -0.29 (-0.55 to -0.04)
Sexuality, 6 mo 2/193 Moderate 0.40 (-0.72 to -0.20)
Sleep disturbance, <12 weeks 8/438 Moderate -0.46 (-0.72 to -0.20)
Social functioning, <12 weeks 5/386 Very low 0.45 (0.02 to 0.87)
Social functioning, 6 months 2/110 Moderate 0.49 (0.11 to 0.87)

Forest plot of the relations of change in physical activity (PA) from
pre- to post-diagnosis to total mortality and cancer mortality.
Schmid D , and Leitzmann M F Ann Oncol 2014;25:1293-1311
© The Author 2014. Published by Oxford University Press on behalf of the European Society for
Medical Oncology. All rights reserved. For permissions, please email:
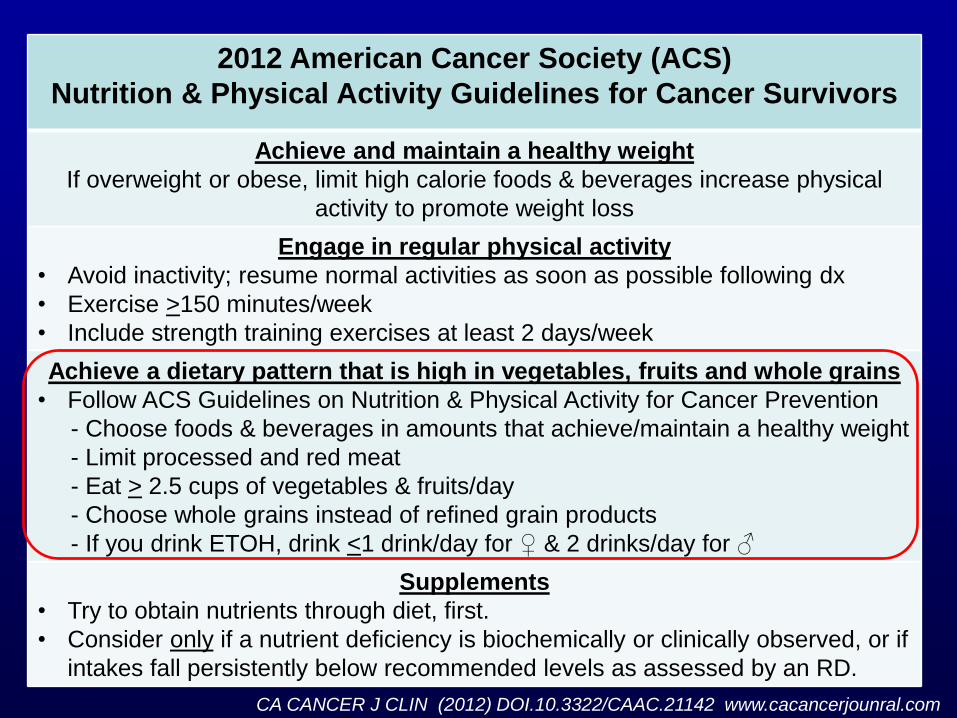
2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com

Red Meat Consumption & Cancer–Related
Mortality • Pooled analysis of 37,698 men from the Health Professionals
Follow-up Study and 83,644 women from the Nurses' Health Study
• 9464 cancer deaths during 2.96 million person-years of follow-up.
Q1
(ref)
Q2 Q3 Q4 Q5 P Trend HR (95% CI) for 1
svg day-1 increase
Total Red
Meat
1 1.05
0.98-1.12
1.09
1.02-1.16
1.16
1.08-1.24
1.19
1.11-1.28
<.001 1.10 (1.07-1.13)
Not
Processed
1 1.03
0.97-1.10
1.03
0.96-1.10
1.09
1.02-1.16
1.17
1.10-1.26
<.001 1.10 (1.06-1.14)
Processed 1 1.03
0.97-1.10
1.08
1.01-1.15
1.08
1.01-1.15
1.14
1.07-1.22
<.001 1.16 (1.09-1.23)
• Substitution estimates of 1 serving/day of other foods (e.g., fish, poultry, nuts,
legumes, low-fat dairy, and whole grains) for 1 serving/day of red meat were
associated with a 7% to 19% lower mortality risk. Estimates suggest that
9.3% of deaths in men and 7.6% in women could have been prevented at
follow-up if there was a reduction in 0.5 servings/day (~42 g/day) of red meat.
Pan A et al. Arch Intern Med March 12, 2012
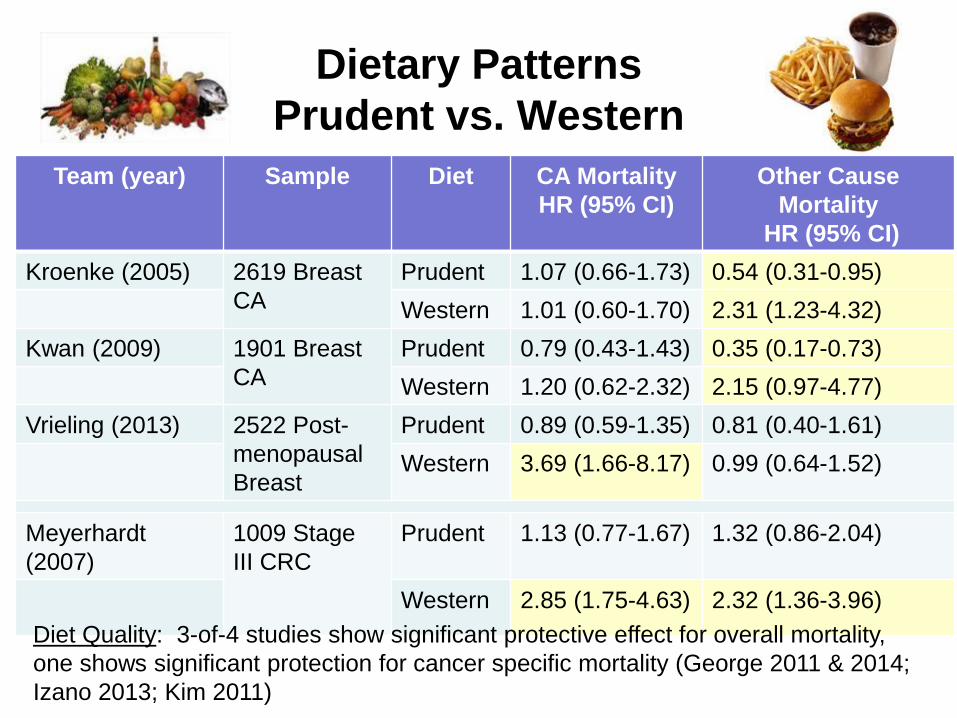
Dietary Patterns
Prudent vs. Western
Team (year) Sample Diet CA Mortality
HR (95% CI)
Other Cause
Mortality
HR (95% CI)
Kroenke (2005) 2619 Breast
CA
Prudent 1.07 (0.66-1.73) 0.54 (0.31-0.95)
Western 1.01 (0.60-1.70) 2.31 (1.23-4.32)
Kwan (2009) 1901 Breast
CA
Prudent 0.79 (0.43-1.43) 0.35 (0.17-0.73)
Western 1.20 (0.62-2.32) 2.15 (0.97-4.77)
Vrieling (2013) 2522 Post-
menopausal
Breast
Prudent 0.89 (0.59-1.35) 0.81 (0.40-1.61)
Western 3.69 (1.66-8.17) 0.99 (0.64-1.52)
Meyerhardt
(2007)
1009 Stage
III CRC
Prudent
1.13 (0.77-1.67)
1.32 (0.86-2.04)
Western 2.85 (1.75-4.63) 2.32 (1.36-3.96)
Diet Quality: 3-of-4 studies show significant protective effect for overall mortality,
one shows significant protection for cancer specific mortality (George 2011 & 2014;
Izano 2013; Kim 2011)
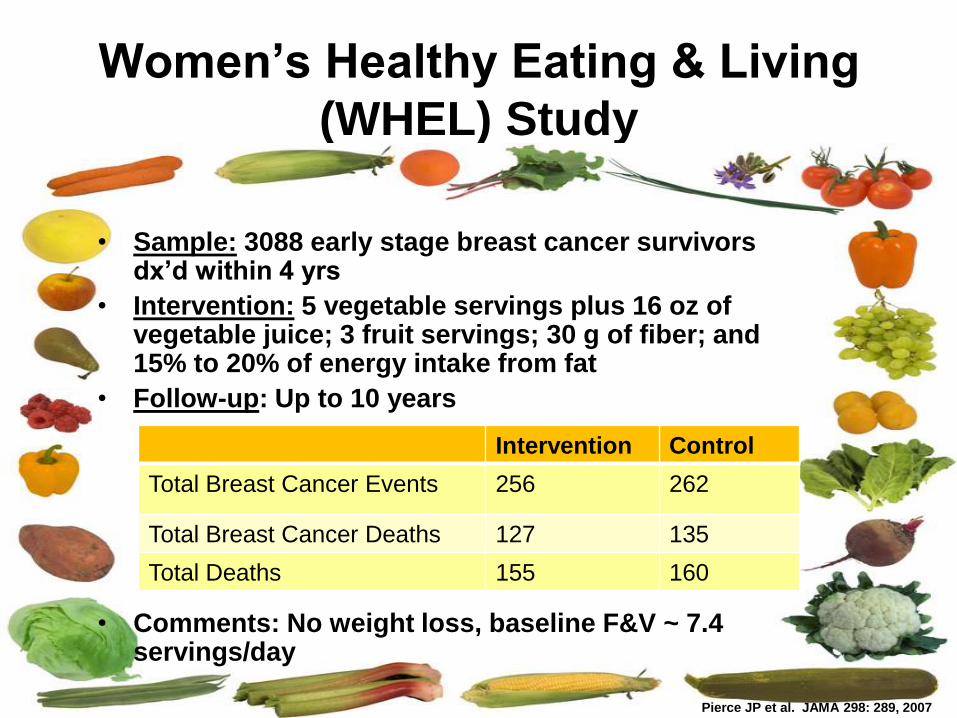
Women’s Healthy Eating & Living
(WHEL) Study
Pierce JP et al. JAMA 298: 289, 2007
• Sample: 3088 early stage breast cancer survivors dx’d within 4 yrs
• Intervention: 5 vegetable servings plus 16 oz of vegetable juice; 3 fruit servings; 30 g of fiber; and 15% to 20% of energy intake from fat
• Follow-up: Up to 10 years
• Comments: No weight loss, baseline F&V ~ 7.4 servings/day
Intervention Control
Total Breast Cancer Events 256 262
Total Breast Cancer Deaths 127 135
Total Deaths 155 160
Pierce JP et al. JAMA 298: 289, 2007

0
5
10
15
20
25
All Patients ER positive ER negative
Low Fat Diet
Regular Diet
Results of the Women’s Intervention Nutrition Study (WINS) Show Reduced Rates of Recurrence in Patients Assigned to a Low Fat Diet (n=2,437)
Chlebowski et al. JNCI 98:1767, 2006
P =.034 P =.277
P =.018
Recu
rren
ce R
ate
s (
% o
f p
op
ula
tio
n)
Alcohol
• Direct association with cancers of the kidney, head and neck and primary risk of breast cancer (“no amount of alcohol is safe”
• If you are a survivor of head and neck cancer you should not drink alcohol since it will increase your chance complication and reduce survival
• If you are a survivor of other cancers the choice is less clear – it may increase your risk of recurrence (breast cancer) but also decrease your risk of death due to cardiovascular disease
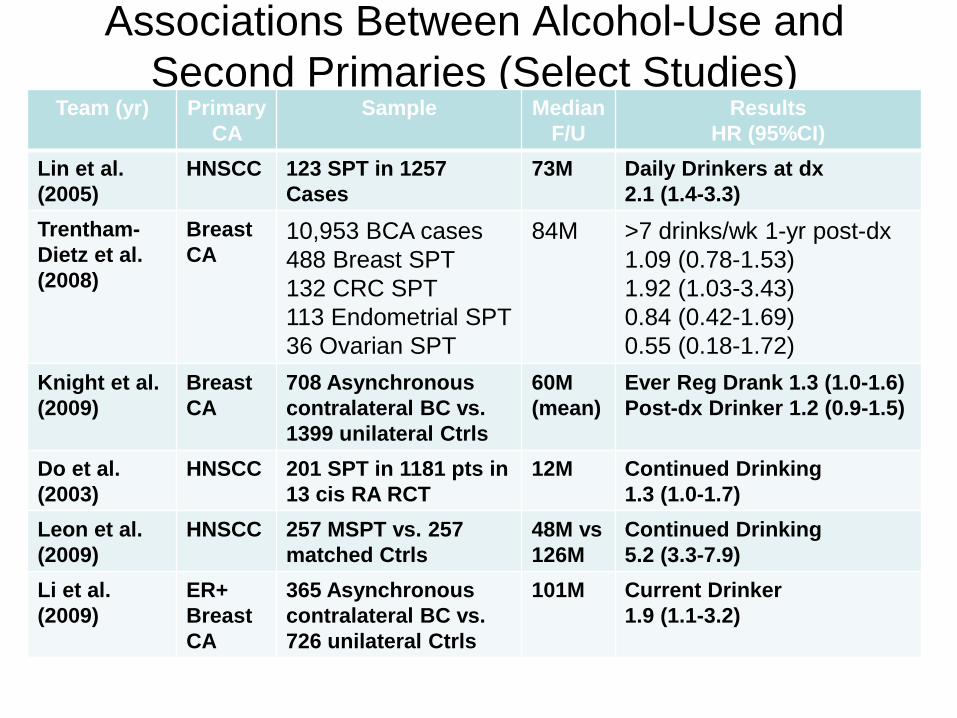
Associations Between Alcohol-Use and
Second Primaries (Select Studies) Team (yr) Primary
CA
Sample Median
F/U
Results
HR (95%CI)
Lin et al.
(2005)
HNSCC 123 SPT in 1257
Cases
73M Daily Drinkers at dx
2.1 (1.4-3.3)
Trentham-
Dietz et al.
(2008)
Breast
CA 10,953 BCA cases
488 Breast SPT
132 CRC SPT
113 Endometrial SPT
36 Ovarian SPT
84M >7 drinks/wk 1-yr post-dx
1.09 (0.78-1.53)
1.92 (1.03-3.43)
0.84 (0.42-1.69)
0.55 (0.18-1.72)
Knight et al.
(2009)
Breast
CA
708 Asynchronous
contralateral BC vs.
1399 unilateral Ctrls
60M
(mean)
Ever Reg Drank 1.3 (1.0-1.6)
Post-dx Drinker 1.2 (0.9-1.5)
Do et al.
(2003)
HNSCC 201 SPT in 1181 pts in
13 cis RA RCT
12M Continued Drinking
1.3 (1.0-1.7)
Leon et al.
(2009)
HNSCC 257 MSPT vs. 257
matched Ctrls
48M vs
126M
Continued Drinking
5.2 (3.3-7.9)
Li et al.
(2009)
ER+
Breast
CA
365 Asynchronous
contralateral BC vs.
726 unilateral Ctrls
101M Current Drinker
1.9 (1.1-3.2)
2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com
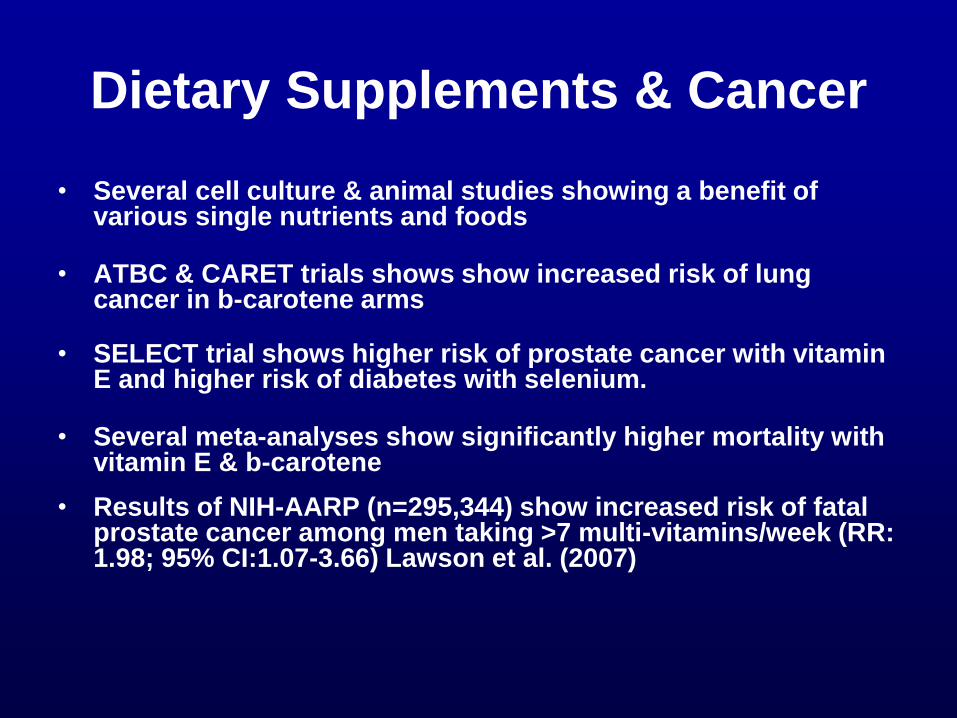
Dietary Supplements & Cancer
• Several cell culture & animal studies showing a benefit of various single nutrients and foods
• ATBC & CARET trials shows show increased risk of lung cancer in b-carotene arms
• SELECT trial shows higher risk of prostate cancer with vitamin E and higher risk of diabetes with selenium.
• Several meta-analyses show significantly higher mortality with vitamin E & b-carotene
• Results of NIH-AARP (n=295,344) show increased risk of fatal prostate cancer among men taking >7 multi-vitamins/week (RR: 1.98; 95% CI:1.07-3.66) Lawson et al. (2007)
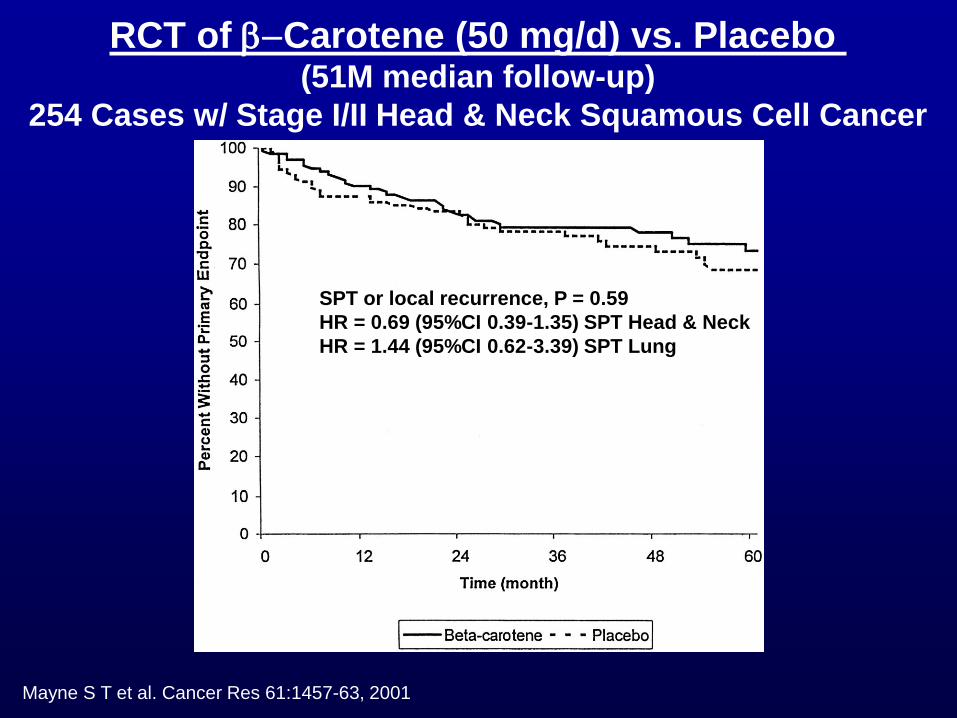
Mayne S T et al. Cancer Res 61:1457-63, 2001
RCT of b-Carotene (50 mg/d) vs. Placebo (51M median follow-up)
254 Cases w/ Stage I/II Head & Neck Squamous Cell Cancer
SPT or local recurrence, P = 0.59
HR = 0.69 (95%CI 0.39-1.35) SPT Head & Neck
HR = 1.44 (95%CI 0.62-3.39) SPT Lung

Bairati et al. JNCI ;97:481-8, 2005
Cancer-free survival (no recurrence & no SPT among participants randomly assigned to the
supplement arm (solid line) or to the placebo arm (dotted line)
Second Primary HR 2.88 (95%CI 1.56-5.31)
RCT of a- Tocopherol + b-Carotene vs. Placebo (52M median follow-up)
540 Cases w/ Stage I/II Head & Neck Squamous Cell Cancer

Bottom Line on Supplements
Rely on Food as a Source of Nutrients But , if considering supplements
-Have dietitian analyze diet for deficiency
- Check blood levels of nutrients
- Consider lowest dosage & most complex preparation
- If currently on supplements wean off slowly.
Calcium V.S.
Miracle
in a
Bottle

Synergy between Lifestyle Practices?
• Early stage breast cancer survivors in Multi-ethnic Cohort (n=670) Compared with inactive survivors consuming poor-quality diets, survivors engaging in any physical activity and consuming better-quality diets had an 89% reduced risk of death from any cause HR: 0.11 (0.04-0.36) and a 91% reduced risk of death from breast cancer HR: 0.09 (0.01- 0.89). (George et al. 2011)
• In 1490 early stage breast cancer survivors a combination of 5+ daily servings of F&V + accumulating 540+ MET-min/w associated with a doubling of survival HR: 0.56 (0.31 - 0.98) (Pierce et al. 2007)
• In 2193 post-menopausal breast cancer survivors from Iowa Woman’s Health Study those who were most adherent vs. least adherent (6-8 vs. 0-4) to AICR/WCRF guidelines had a 33% lower mortality rate (Inoue-Choi et al. 2013)
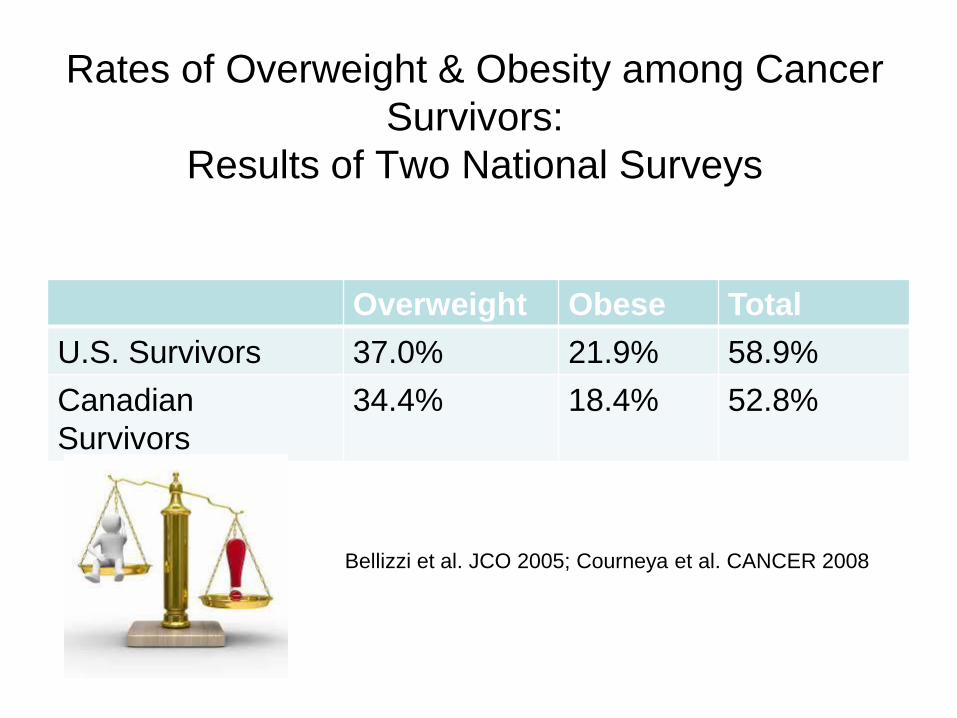
Rates of Overweight & Obesity among Cancer
Survivors:
Results of Two National Surveys
Overweight Obese Total
U.S. Survivors 37.0% 21.9% 58.9%
Canadian
Survivors
34.4% 18.4% 52.8%
Bellizzi et al. JCO 2005; Courneya et al. CANCER 2008

Blanchard et al, JCO 2008.
Many cancer survivors do not adhere to recommendations
(ACS Cancer Survivors II Study, n=9,105)
More Research is Needed
• Optimal timing
• Specific content, sequencing
and dose
• Impact on array of outcomes
• Mechanisms of action
• Factors that moderate effect
(cancer-type, tumor
characteristics, treatment, age,
co-morbidity, gender, etc.)
• Optimal delivery channel
(dissemination)
• Cost-effectiveness

Resources
• American Cancer Society: www.cancer.org
• Academy of Nutrition and Dietetics: www.eatright.org
• American Institute for Cancer Research: www.aicr.org
• Centers for Disease Control: www.cdc.gov/HealthyLiving
• National Center for Complementary & Alternative Medicine: http://nccam.nih.gov

http://aspo.org
March 15-17th
Birmingham, AL
Interactive Poster Sessions on Obesity and E-cigarettes
Preconference Workshop: Underserved Cancer Survivors