opioid addiction 2 - amazon s3€¦ · opioid addiction 2.0 light university i welcome to light...
TRANSCRIPT

OpioidAddiction2.0
P.O.Box739•Forest,VA24551•1-800-526-8673•www.AACC.net

OpioidAddiction2.0
LightUniversity i
WelcometoLightUniversityandthe“OpioidAddiction2.0”programofstudy.Our prayer is that you will be blessed by your studies and increase your effectiveness inreaching out to others. We believe you will find this program to be academically sound,clinicallyexcellentandbiblically-based.Our faculty represents some of the best in their field – including professors, counselors andministers who provide students with current, practical instruction relevant to the needs oftoday’sgenerations.We have alsoworked hard to provide youwith a program that is convenient and flexible –givingyou theadvantageof “classroom instruction”onDVD-based lectures,peer interaction,andallowingyoutocompleteyourtraininginthecomfortofyourhomeoroffice.Thank you for your interest in this program of study. Our prayer is that you will grow inknowledge,discernment,andpeople-skillsthroughoutthiscourseofstudy.Sincerely,
RonHawkinsDean,LightUniversity
OpioidAddiction2.0
LightUniversity ii
TheAmericanAssociationofChristianCounselors
• Represents the largestorganizedmembership (nearly50,000)ofChristian counselorsandcaregiversintheworld,havingjustcelebratedits30thanniversaryin2016.
• Known for its top-tier publications (Christian Counseling Today, the Christian CounselingConnectionandChristianCoachingToday),professionalcredentialingopportunitiesofferedthroughtheInternationalBoardofChristianCare(IBCC),excellenceinChristiancounselingeducation, an arrayof broad-based conferences and live training events, radioprograms,regulatoryandadvocacyeffortsonbehalfofChristianprofessionals,apeer-reviewedEthicsCode, and collaborative partnerships such as Compassion International, the AACC hasbecomethefaceofChristiancounselingtoday.
• The AACC also helped launch the International Christian Coaching Association (ICCA) in
2011, and has developed a number of effective tools and training resources for LifeCoaches.
OurMission
The AACC is committed to assisting Christian counselors, the entire “community of care,”licensedprofessionals,pastors,and laychurchmemberswith littleorno formal training. It isourintentiontoequipclinical,pastoral,andlaycaregiverswithbiblicaltruthandpsychosocialinsights that minister to hurting persons and helps them move to personal wholeness,interpersonalcompetence,mentalstability,andspiritualmaturity.
OpioidAddiction2.0
LightUniversity iii
OurVision
TheAACC’svisionhastwocriticaldimensions:First,wedesiretoservetheworldwideChristianChurch by helping foster maturity in Christ. Secondly, we aim to serve, educate, and equip1,000,000 professional clinicians, pastoral counselors, and lay helpers throughout the nextdecade.WearecommittedtohelpingtheChurchequipGod’speopletoloveandcareforoneanother.We recognize Christian counseling as a unique form of Christian discipleship, assisting thechurch in its call to bring believers to maturity in the lifelong process of sanctification—ofgrowingtomaturityinChristandexperiencingabundantlife.Werecognizesomearegiftedtodosointhecontextofaclinical,professionaland/orpastoralmanner.Wealsobelieveselected laypeoplearecalledtocareforothersandthattheyneedtheappropriatetrainingandmentoringtodoso.WebelievetheroleofthehelpingministryintheChurchmustbesupportedbythreestrongcords:thepastor,thelayhelper,andtheclinicalprofessional.ItistothesethreerolesthattheAACCisdedicatedtoserve(Ephesians4:11-13).
OurCoreValues
InthenameofChrist,theAmericanAssociationofChristianCounselorsabidesbythefollowingvalues:
VALUE1:OURSOURCEWearecommittedtohonorJesusChristandglorifyGod,remainingflexibleandresponsivetotheHolySpiritinallthatHehascalledustobeanddo.VALUE2:OURSTRENGTHWearecommittedtobiblicaltruths,andtoclinicalexcellenceandunityinthedeliveryofallourresources,services,trainingandbenefits.VALUE3:OURSERVICEWeare committed toeffectivelyandcompetently serve the communityof careworldwide—bothourmembership and the churchat large—withexcellenceand timeliness, andbyover-deliveryonourpromises.VALUE4:OURSTAFFWearecommittedtovalueandinvestinourpeopleaspartnersinourmissiontohelpotherseffectivelyprovideChrist-centeredcounselingandsoulcareforhurtingpeople.VALUE5:OURSTEWARDSHIPWe are committed to profitably steward the resourcesGod gives to us in order to continueservingtheneedsofhurtingpeople.

OpioidAddiction2.0
LightUniversity iv
LightUniversity• Establishedin1999undertheleadershipofDr.TimClinton—hasnowseennearly250,000
students from around the world (including lay caregivers, pastors and chaplains, crisisresponders,lifecoaches,andlicensedmentalhealthpractitioners)enrollincoursesthataredelivered via multiple formats (live conference and webinar presentations, video-basedcertificationtraining,andastate-of-theartonlinedistanceteachingplatform).
• Thesepresentations,courses,andcertificateanddiplomaprograms,offeroneofthemostcomprehensive orientations to Christian counseling anywhere. The strength of LightUniversity is partially determined by its world-class faculty—over 150 of the leadingChristianeducators,authors,mentalhealthcliniciansandlifecoachingexpertsintheUnitedStates. This core groupof facultymembers represents a literal “Who’sWho” inChristiancounseling. No other university in the world has pulled together such a diverse andcomprehensivegroupofprofessionals.
• Educational and training materials cover over 40 relevant core areas in Christian—
counseling, lifecoaching,mediation,andcrisis response—equippingcompetentcaregiversand ministry leaders who are making a difference in their churches, communities, andorganizations.
OurMissionStatement
TotrainonemillionBiblicalCounselors,ChristianLifeCoaches,andChristianCrisisRespondersbyeducating,equipping,andservingtoday’sChristianleaders.
AcademicallySound•ClinicallyExcellent•DistinctivelyChristian

OpioidAddiction2.0
LightUniversity v
Video-basedCurriculum
• UtilizesDVDpresentations that incorporateover 150 of the leading Christian educators,authors,mentalhealthclinicians,andlifecoachingexpertsintheUnitedStates.
• Eachpresentationisapproximately50-60minutesinlengthandmostareaccompaniedbyacorrespondingtext(inoutlineformat)anda10-questionexaminationtomeasurelearningoutcomes.Therearenearly1,000uniquepresentationsthatareavailableandorganizedinvariouscourseofferings.
• Learning is self-directed and pacing is determined according to the individual time
parameters/scheduleofeachparticipant.• With the successful completion of each program course, participants receive an official
Certificate of Completion. In addition to the normal Certificate of Completion that eachparticipant receives, Regular and Advanced Diplomas in Biblical Counseling are alsoavailable.
Ø TheRegularDiploma isawardedbytakingCaringForPeopleGod’sWay,BreakingFreeandoneadditionalElectiveamongtheavailableCoreCourses.
Ø TheAdvancedDiplomaisawardedbytakingCaringForPeopleGod’sWay,BreakingFree,andanythreeElectivesamongtheavailableCoreCourses.
Credentialing
• LightUniversitycourses,programs,certificatesanddiplomasarerecognizedandendorsedbytheInternationalBoardofChristianCare(IBCC)anditsthreeaffiliateBoards:theBoardofChristianProfessional&PastoralCounselors(BCPPC);theBoardofChristianLifeCoaching(BCLC);andtheBoardofChristianCrisis&TraumaResponse(BCCTR).
• Credentialing is a separateprocess from certificate or diploma completion.However, theIBCC accepts Light University and Light University Online programs as meeting theacademic requirements for credentialing purposes. Graduates are eligible to apply forcredentialinginmostcases.
Ø Credentialinginvolvesanapplication,attestation,andpersonalreferences.
Ø CredentialrenewalsincludeContinuingEducationrequirements,re-attestation,andoccureitherannuallyorbienniallydependingonthespecificBoard.

OpioidAddiction2.0
LightUniversity vi
OnlineTesting
TheURLfortakingallquizzesforthiscourseis:http://www.lightuniversity.com/my-account/.
• TOLOGINTOYOURACCOUNT
Ø You should have received an email upon checkout that included your username,password,andalinktologintoyouraccountonline.
• MYDASHBOARDPAGE
Ø Once registered, youwill see theMyDVD Course Dashboard link by placing yourmousepointerovertheMyAccountmenuinthetopbarofthewebsite.Thispagewill includestudentPROFILE informationand theREGISTEREDCOURSES forwhichyouareregistered.TheLOG-OUTandMYDASHBOARDtabswillbeinthetoprightofeachscreen.Clickingonthe>nexttothecoursewilltakeyoutothecoursepagecontainingthequizzes.
• QUIZZES
Ø Simplyclickonthefirstquiztobegin.• PRINTCERTIFICATE
Afterallquizzesaresuccessfullycompleted,a“PrintYourCertificate”buttonwillappearnearthetopofthecoursepage.YouwillnowbeabletoprintoutaCertificateofCompletion.Yournameandthecourseinformationarepre-populated.ContinuingEducation The AACC is approved by the American Psychological Association (APA) to offer continuingeducationforpsychologists.TheAACCisaco-sponsorofthistrainingcurriculumandaNationalBoard of Certified Counselors (NBCC)ApprovedContinuing Education Provider (ACEPTM). TheAACC may award NBCC approved clock hours for events or programs that meet NBCCrequirements.TheAACCmaintainsresponsibilityforthecontentofthistrainingcurriculum.TheAACCalsoofferscontinuingeducationcreditforplaytherapiststhroughtheAssociationforPlayTherapy (APT Approved Provider #14-373), so long as the training element is specificallyapplicabletothepracticeofplaytherapy.It remains the responsibility of each individual to be aware of his/her state licensure andContinuing Education requirements. A letter certifying participation will be mailed to thoseindividuals who submit a Continuing Education request and have successfully completed allcourserequirements.

OpioidAddiction2.0
LightUniversity vii
Presentersfor
OpioidAddiction2.0
OpioidAddiction2.0
LightUniversity viii
PresenterBiographiesDavid Jenkins, Psy.D., is Professor of Counseling and Director of the M.A. in AddictionCounselingprogram in theDepartmentof Counselor Education and Family Studies at LibertyUniversity. He previously served as Clinical Director of the International Board of ChristianCounselors for the American Association of Christian Counselors and is currently on theExecutive Board of the Society for Christian Psychology.Withmore than 25 years of clinicalexperience,Dr.JenkinsspecializesintheintegrationofChristianfaithandclinicalpractice.Hehasworkedextensivelywithmood,anxiety,andaddictivedisordersinthecontextofindividual,marital,andfamilytherapy.Dr.Jenkinshasprovidededucation,consultation,supervision,andtrainingforavarietyofchurches,ministries,andprofessionals.Heisalsoanauthorandspeakeratconferences,seminars,andretreats.Michael Lyles,M.D. isagraduateof theUniversityofMichigan’ssix-yearpremedical-medicalprogram.Hecompletedhispsychiatric residencyandAPA/NIMHMinorityFellowshipatDukeUniversityMedicalCenter,wherehewastherecipientoftheNorthCarolinaNeuropsychiatricAssociationResidentoftheYearAward.Dr.LyleswasanAssistantProfessorofPsychiatryandAssociateDirectorofOutpatientServicesattheUniversityofKentuckyCollegeofMedicine.Hehasworkedintheprivatesectorinacommunitymentalhealthcenter,statepsychiatrichospitalandcounty,stateandfederalprisons. Inaddition,he isboardcertified inAdultPsychiatrybytheAmericanBoardofPsychiatryandNeurology.Hismajorareasofclinicalactivityaremooddisorders,anxietydisorders,andADHD.Dr.Lyleshaspublishedmorethan60articlesandvideopresentations and serves on the speaking and advisory boards for several pharmaceuticalcompanies.HeisanAACCExecutiveBoardmember.Linda Mintle, Ph.D., is the Chair of Behavioral Health at Liberty University’s College ofOsteopathicMedicine(LUCOM).ShereceivedherPh.D.inUrbanHealthandClinicalPsychologyfrom Old Dominion University, a master’s degree in Social Work, and Bachelor of Arts inPsychology and Communications, both from Western Michigan University. Dr. Mintle is aLicensedMarriageandFamilyTherapist,aLicensedClinicalSocialWorker,anationalspeaker,andbest-sellingauthorwith19booktitlescurrentlypublished,aswellasnumerousarticlesandtextbookchapters.SheisthehostofTheDr.LindaMintleradioshowonFaithRadio,anationalconferencespeaker,anationalbloggerforBeliefNet,andappearsregularlyasanationalnewsconsultantforvariousnetworksonissuesrelatedtomentalhealth.Eric Scalise, Ph.D., is the former Vice President for Professional Development with theAmericanAssociationofChristianCounselors,aswellasacurrentconsultantandtheirSeniorEditor.HeisalsothePresidentofLIVEnterprises&Consulting,LLC,andaLicensedProfessionalCounselor and LicensedMarriage&Family Therapistwithmore than37yearsof clinical andprofessionalexperienceinthementalhealthfield.Specialtyareasincludeprofessional/pastoralstress and burnout, combat trauma and PTSD, marriage and family issues, leadershipdevelopment, addictions, and lay counselor training. He is an author, a national andinternational conference speaker, and frequently consults with organizations, clinicians,ministryleaders,andchurchesonavarietyofissues.
OpioidAddiction2.0
LightUniversity ix
OpioidAddiction2.0TableofContents:
OPAD101:OpioidsandAddiction:AnAlarmingTsunami.......................................................1MichaelLyles,M.D.OPAD102:TheOpioidCrisis:AChristianCounselingResponse–PartI..................................12DavidJenkins,Psy.D.,andLindaMintle,Ph.D.OPAD103:TheOpioidCrisis:AChristianCounselingResponse–PartII.................................23DavidJenkins,Psy.D.,LindaMintle,Ph.D.,andEricScalise,Ph.D.

OpioidAddiction2.0
LightUniversity 1
OPAD101:
OpioidsandAddiction:AnAlarmingTsunami
MichaelLyles,M.D.

OpioidAddiction2.0
LightUniversity 2
Summary
Over thepast several years, theUnitedStateshasbeenoverwhelmedwitha growingopioid
crisisthathasnowreachedepidemicproportions.Nationalagenciesandtreatmentcentersare
activelysearchingforanswers.Dr.Lylesaddressesthescopeoftheproblem,examinessomeof
theunderlyingcauses,andlooksatthehumantoll,aswellasthedevastatingeffectsonnormal
brainfunctioning.
LearningObjectives
1. Participantswillexplorethecurrenttrendsofaddictions.
2. Participantswilldiscusshowsubstanceusedisordercametobesuchanepidemic.
3. Participantswillidentifyhowthebraininteractswithaddictivesubstances.

OpioidAddiction2.0
LightUniversity 3
I. TheScopeoftheProblem
A. SurgeonGeneral’sReport–2015Data
1. 27millionpeopleusedillicitdrugsormisusedprescriptionmedication
2. 20.8millionpeoplehadasubstanceusedisorder
3. 25%ofadults/adolescentsreportingbingedrinkingwithinthepastmonth
4. $420billiondollarsarespentannually
• Directhealthcarecosts
• Lostproductivity
• Criminaljusticesystem
• Exceedstheyearlycostsofdiabetes
B. SubstanceAbuseandMentalHealthSupportAdministration(SAMHSA)
1. 40%ofpeoplewithsubstanceabusedisordershaveaco-morbidmentalhealth
disorder.
2. Lessthan50%receivedtreatment.
C. SurgeonGeneralMurthy–November,2016
1. Thenumberofpatientswithsubstanceusedisordersis1.5timesgreaterthan
peoplewithallcancerscombined.
2. Morepeopleuseprescriptionopioidsthansmoketobacco.
OpioidAddiction2.0
LightUniversity 4
II. HowDidtheOpioidEpidemicOccur?
A. TheNatureoftheOpioidEpidemic
1. Twomillionpeoplehaveanopioidusedisorderinvolvingprescriptionopioids.
2. 20%havereceivedtreatment.
3. 600,000peoplehaveanopioidusedisorderinvolvingheroin.
4. Theannualdeathratefromprescriptionopioidshasremainedstablefrom2011–
2015buttheannualdeathratefromillicitopioidshastripled.
5. Adultpatientswithpsychiatricdisorderscompriseabout16%ofthepopulation,but
50%ofopioidprescriptionsareusedbythat16%.
B. Heroin
1. Heroinuseisata20yearhigh.
2. Heroinusehastripledfrom2003-2014.
3. Deathsfromheroinoverdosehavequintupled.
4. Sevendaysofheroinstudy:
• 18deaths
• 180overdoses
• 15babiesbornwithheroinrelatedmedicalproblems
• 23investigationsinitiatedintowell-beingofachild
• 210heroinusersinjail

OpioidAddiction2.0
LightUniversity 5
C. Why?
1. Increaseinprescriptionsgivenbydoctorsstarting1990s
2. Deceptivemarketingbypharmaceuticalcompanies
3. Professionalsocietiesslowtoadvocatefordrugabuse
4. From1991-2011,oxycodoneandhydrocodoneprescriptionswentfrom76millionto
219million.
5. Prescriptionofopioidspeakedin2010,anddeclinedthrough2015,butitisstill
threetimestherateof1999.
6. Highestratesareofopioidprescriptionarefoundincertainpopulations:
• Non-Hispanicwhites
• Highprevalenceofdiabetes/arthritis
• Highunemployment
• HighMedicaidenrollment
D. CoreSymptomsofSUD
1. Lossofcontrol
2. Preoccupationwiththedrug(mentalorbehavioral)
3. DSM-5

OpioidAddiction2.0
LightUniversity 6
III. SubstanceAbuseDisordersandtheBrain
A. BrainTerminology
1. Neurotransmitters
• Serotonin
• Dopamine
• Endorphins
• Norepinephrine
• GABA
2. Neurotransmittersarelikeakeyinalockthatopensthedoortotransmitamessage.

OpioidAddiction2.0
LightUniversity 7
B. ThePleasureRewardSystems
C. VTA,NucleusAccumbens:GenesisofPleasure
1. VentralTegmentalAreaistherootofdopamine.
2. PleasurableactivitiesstimulatetheVTAtomakedopamineinmildtomoderate
amountsthatthebraincanhandle.
3. Thedopamineisshippedtothenucleusaccumbens(viathemedialfascicular
bundle).
4. Dopaminecontrolspleasure,risesduringpleasurableactivity,andinteractswith
endorphins.
OpioidAddiction2.0
LightUniversity 8
D. NucleusAccumbens:TheJamesBrownCenter
1. Centerofpleasureandreward
2. SerotoninandGABAactas“brakes”tokeepthisfromspeedinguptoomuch.
3. Drugsofabusehighjackthesystemandspeedupthenucleusaccumbens.
4. Whenthenucleusaccumbensisover-stimulatedrepeatedly,itcreatesanew
normal.
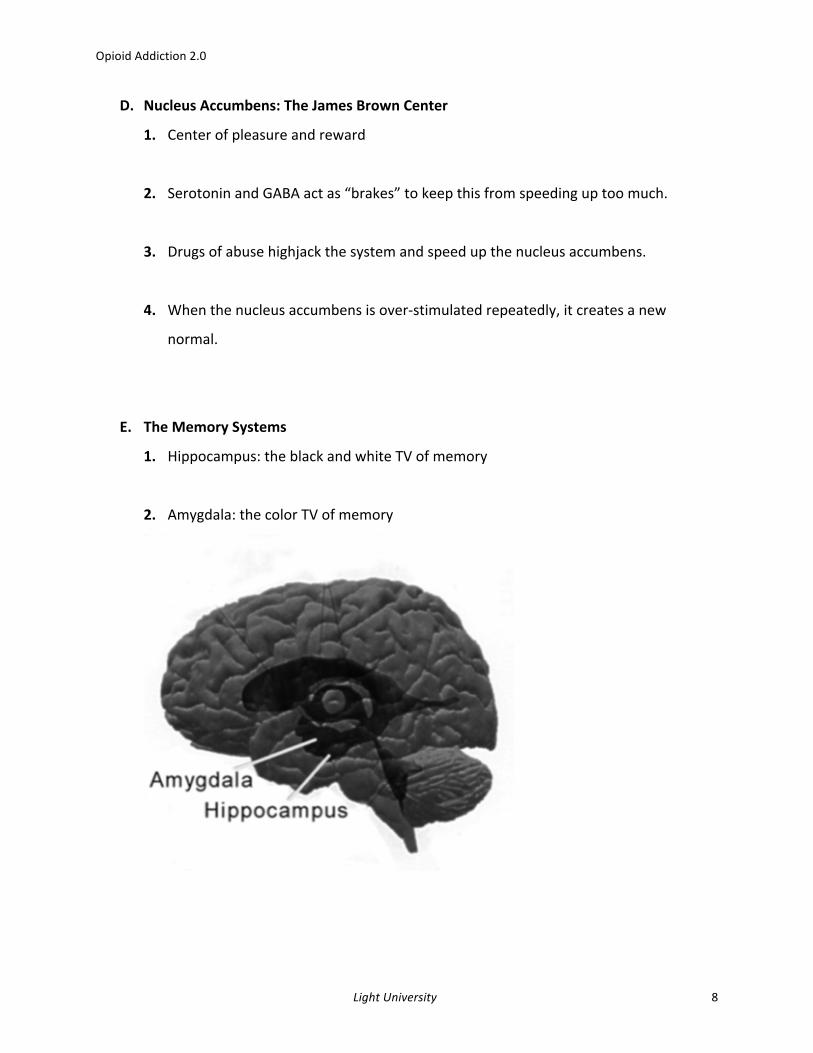
E. TheMemorySystems
1. Hippocampus:theblackandwhiteTVofmemory
2. Amygdala:thecolorTVofmemory

OpioidAddiction2.0
LightUniversity 9
F. ThePrefrontalCortex
1. Thesheriff/judgeofthebrain
2. Centerofexecutivefunctions
3. ConnectstotheVTAandthenucleusaccumbens
G. LocusCeruleus
1. Thesecurityalarm
2. Locatedinthebrainstem
3. Richinnorepinephrine
4. Responsibleforwithdrawal
H. DrugMediatedPleasure
1. Notallpeopleareaffectedthesamewaybymood-alteringdrugs.
2. Withrepeatedexposure,thesystemlosesitscalibrationandbeginstothinkthatthe
dopaminehighisnormal.
3. Thisresultsinanacquireddrive.
4. SerotoninandGABAareturnedoffandimpulsecontrolsarelost.
5. Where’smydopamine?

OpioidAddiction2.0
LightUniversity 10
I. DrugsofAbuseandtheRewardSystem
1. Thenucleusaccumbensisdirectlystimulatedbycocaine,amphetamines,opiates,
andmarijuana.
2. TheVTAisdirectlystimulatedbyalcohol,opiates,andnicotine.
3. Thelocusceruleusisstimulatedbynicotine,opiates,andalcohol.
4. Thehippocampusisaffectedbynicotine,marijuana,andalcohol.
IV. Conclusion
A. AProperUnderstandingofAddiction
1. Drugsofabusemimicnaturallyoccurringsubstancesinthebrain,hijackthesystem,
andchangethehardwiringofthebrain.
2. Wemustapproachaddictionandsubstanceabuseaschronichealthconditions,not
asacharacterflaw.
B. TheRealWorld
1. Peoplewithaddictivedisordersliveinshame,silence,andstigma.
2. Drugsaren’ttheonlythingstowhichpeoplegetaddicted.
OpioidAddiction2.0
LightUniversity 11
FurtherReading
U.S.SurgeonGeneral’sReporthttps://addiction.surgeongeneral.gov/CDCGuidelinesforPrescribingOpioidsforChronicPain:https://www.cdc.gov/drugoverdose/pdf/guidelines_factsheet-a.pdfNationalAcademiesofSciencesEngineeringandMedicineReporthttps://www.nap.edu/catalog/24781/pain-management-and-the-opioid-epidemic-balancing-societal-and-individualNationalInstituteonDrugAbuseMedicationAssistedTreatmentReporthttps://www.drugabuse.gov/publications/research-reports/medications-to-treat-opioid-addiction/overviewTheRoleofScienceinAddressingtheOpioidCrisishttp://www.nejm.org/doi/full/10.1056/NEJMsr1706626MartinsS,Sarvet,A.,etal.“ChangesinLifetimeHeroinUseandHeroinUseDisorder”Doi:10.1001/jamapsychiatry.2017.0113

OpioidAddiction2.0
LightUniversity 12
OPAD102:
TheOpioidCrisis:AChristianCounselingResponse–PartI
DavidJenkins,Psy.D.,andLindaMintle,Ph.D.

OpioidAddiction2.0
LightUniversity 13
Summary
Understanding the current opioid crisis is critical to developing an overall strategy for
comprehensiveoutreachandcare.Dr.JenkinsandDr.Mintlereviewemergingtrendsleadingto
addiction, the addiction process, the use of certain medications, and how opioid use has
impactedindividuals,families,churches,andentirecommunities.
LearningObjectives:
1. Participantswillbeabletorecognizethedifferenttypesoflicitandillicitopioids.
2. Participantswillexaminethehistoryofopioidabuseaswellascurrentstatisticsrelated
totheopioidepidemicinAmerica.
3. Participantswillanalyzetheneurologyofthebrainandhowitrelatestothestagesand
processofaddiction.

OpioidAddiction2.0
LightUniversity 14
I. TypesofOpioidMedications
A. LicitandIllicitOpioids
1. Codeine(onlyavailableingenericform)
2. Morphine(Astramorph,Avinza,Kadian,MSContin,Ora-MorphSR)
3. Hydrocodone(HysinglaER,ZohydroER)
4. Hydrocodone/acetaminophen(Lorcet,Lortab,Norco,Vicodin)
5. Oxycodone(OxyContin,Oxecta,Roxicodone)
6. Oxycodoneandacetaminophen(Percocet,Endocet,Roxicet)
7. Oxycodoneandnaloxone(TarginiqER)
8. Hydromorphone(Dilaudid,Exalgo)
9. Meperidine(Demerol)
10. Methadone(Dolophine,Methadose)
B. SyntheticOpioids
1. Fentanyl;Carfentanil
• Fentanylbyprescriptionisprimarilyusedforanesthesia,post-surgicalpain,and
managementofpaininopioid-tolerantpatients.

OpioidAddiction2.0
LightUniversity 15
2. NationalInstituteofDrugAbuse(2017)
• Fentanylis80xmorepotentthanmorphine
• Carfentanilis10,000xmorepotentthanmorphine
• Otheranaloguesalsomorepotent
• Illicitlymanufacturedversionsareresponsiblefortriplingsyntheticopioiddeaths
from2013(3,105)–2015(9,580).
II. CurrentStatistics
A. NumberofPrescriptions(Guy,etal.,2017)
1. Quadrupledfrom1999to2010,yetnoincreaseinreportedpain
• Opioidoverdosedeathsandtreatmentadmissionshaveparalleledthisincrease
• PrimaryCareProvidersaccountforhalfofthisincrease
2. Reasonsforincrease
• Treatmentofchronicnon-cancerpain…
• Whichincreasedtheaveragelengthoftimeopioidswereprescribed…
• Leadingtohigherdosagesandamountsperprescription
B. NumberofPrescriptions(CDC,2017)
1. 214,881,622opioidprescriptionsdispensedbyretailpharmaciesin2016fornearly
62millionpatients.
2. Averagenumberofopioidprescriptionswas3.5perpatientin2016.
3. Annualprescribingratesin2016:
• ≥30days’supplywas27.3per100persons
• <30days’supplywas39.2per100persons
OpioidAddiction2.0
LightUniversity 16
C. NumberofHospitalVisits(AHRQ,2016)
1. 64%increasebetween2005and2014inopioid-relatedinpatienthospitalizations
2. 99%increaseEmergencyDepartment(ED)visits
3. 90peopleperdaydiefromopioid-relatedoverdoses(2014rates)
4. Over130perdaybasedon2016rates(a45%increasein2years)
D. NumberofOverdoseDeaths
1. 2015:52,404overdosedeaths(63.1%opioid-related)
2. 2016:64,000overdosedeaths(74%opioid-related)
3. ASAM(2016)
• 4in5newheroinusersstartedoutmisusingprescriptionpainkillers.
• 94%ofrespondentsin2014surveyofpeopleintreatmentforopioidaddiction
chosetouseheroinbecauseprescriptionopioidswere“farmoreexpensiveand
hardertoobtain.”
E. NumberofPeoplewithOpioidUseDisorder(OUD)
1. NIDA(2017)
• Roughly21to29percentofpatientsprescribedopioidsforchronicpainmisuse
them(approx.15.2million)
• Between8-12percentdevelopanopioidusedisorder.(approx.6.2million)
• Anestimated4-6percentwhomisuseprescriptionopioidstransitiontoheroin
• About80percentofpeoplewhouseheroinfirstmisusedprescriptionopioids

OpioidAddiction2.0
LightUniversity 17
2. SAMHSA(2017)
• 2.1millionwithopioidusedisorder(OUD)
III. HowDidWeGetHere?
A. TheCurrentSituation
1. CDC:Guidelinesissuedforprescribingopioidsforchronicpain.
2. U.S.FoodandDrugAdministration:“Blackbox”warningonimmediaterelease
opioidpainkillers
3. PresidentTrumpdeclaredtheopioidcrisisanationalemergency.
B. TheHistoricalContext
1. DatesbacktotheAmericanCivilWar:Morphinedependentsoldier’s“Soldier’s
Disease”
2. 1970s:Percocet(oxycodone)andVicodin(acetaminophenandhydrocodone)onthe
market
3. WHOdeclaresinadequatetreatmentforpainapublichealthconcern
4. 1980:NewEnglandJournalofMedicine-“thedevelopmentofaddictionisrare”
5. 1995:AmericanPainSocietyintroducespainasthefifthvitalsignpromoting
assessmentandtreatmentofpain(painratings)
6. BigPharma:Aggressivelymarketingopioidsassafe;numbersofprescriptionssoar

OpioidAddiction2.0
LightUniversity 18
7. 2000:JointCommissionsupportingshort-termuseofopioidsaslowriskwith
materialssupportedbybigpharma
8. Mid2000s:Addictionspiralingoutofcontrol
C. WhyDoPeopleUseDrugs?
1. Multiplereasonstouserelatedtobothphysicalandemotionalpain
2. Abusebecomescompulsive.
3. Opioidsarenoteffectivetreatmentforchronicpain.
IV. UniqueAspectsofAddiction
A. TheStagesofChange
1. Precontemplation
2. Contemplation
3. Preparation
4. Action
5. Maintenance
6. Termination

OpioidAddiction2.0
LightUniversity 19
B. Learning
1. ClassicalConditioning
2. OperantConditioning
• PositiveReinforcement(e.g.,euphoria,extremerelaxation,etc.)
• NegativeReinforcement(e.g.,painrelief,anxietyreduction,etc.)
• EvidencethatthosewhobecomeaddictedexperienceCCandOCmoreintensely
C. TheProcessofAddiction
D. AspectsUniquetoOUD
1. Curiosityisnotmotivationforthosewithpain.
2. MostwhohaveOUDbeganwithnonmedicaluseofprescribedmedications(most
often,someoneelse’s).
OpioidAddiction2.0
LightUniversity 20
3. SocialUsemaygetby-passed.
4. Dependence(tolerance,withdrawal)but,formost,notAddiction(craving,lossof
control)
5. GuiltandShameevenmoreprominentformanyduetoillicituse,misuse,andopioid
usedisorder
6. HigherratesofModerateandSeverevs.Mildseverity
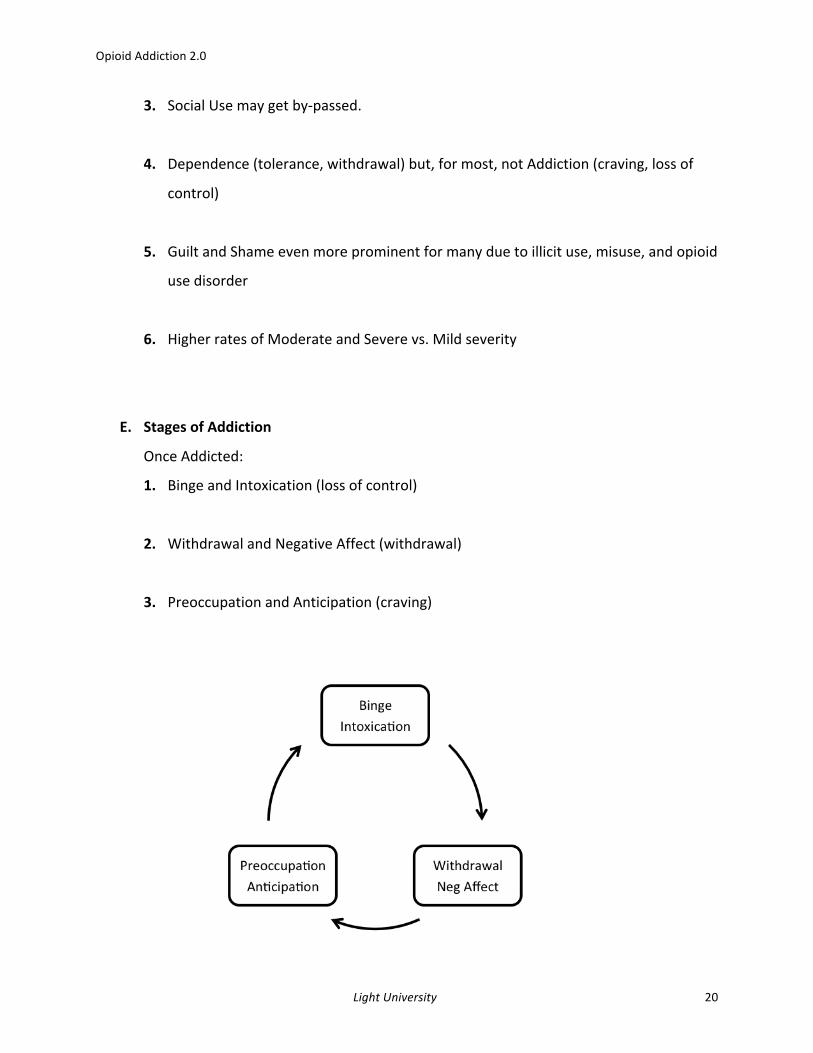
E. StagesofAddiction
OnceAddicted:
1. BingeandIntoxication(lossofcontrol)
2. WithdrawalandNegativeAffect(withdrawal)
3. PreoccupationandAnticipation(craving)
OpioidAddiction2.0
LightUniversity 21
F. NeurobiologyofAddiction
1. VentralTegmentalArea(VTA)
• Richindopaminergiccells
• Reward/salience;motivation
• Pleasure&Euphoria
• Projectionstolimbic&corticalareas
2. NucleusAccumbens(NAc)
• Pleasure,reinforcement,reinforcementlearning
• Prolongedexposurechanges“setpoints”inVTA,NAc,LC(arousal,vigilance)
• HypothalamicPituitaryAdrenal(HPA)Axis
• Stressresponsepathway
V. TheProperRoleofMedication
A. Acutevs.ChronicPain
1. Ingeneral,opioidsarenoteffectiveforchronicpain.
2. Foracutepain,thereisaplaceforopioidsasmedication.
B. TypesofPain
1. Nociceptivepain(tissuedamage)
2. Visceralpain(damagetothebody’sinternalorgans)
3. Somaticpain(stimulationofpainreceptors)

OpioidAddiction2.0
LightUniversity 22
4. Neuropathicpain(nerveinjurypain)
5. Peripheralneuropathicpain(damagetotheperipheralnerve)
C. Naloxone
1. BrandnameNarcan,mostlyinjected
2. Usedforthosewithhighriskofopioidoverdose
3. Usedtotreatanarcoticoverdoseinemergencysituations
4. Blockstheopioidsfor30-90minutestoreversetherespiratorydepressionthat
wouldleadtodeathfromoverdose
5. Onlyworksforwhenopioidsarepresentinthesystem

OpioidAddiction2.0
LightUniversity 23
OPAD103:
TheOpioidCrisis:AChristianCounselingResponse–PartII
DavidJenkins,Psy.D.,LindaMintle,Ph.D.,andEricScalise,Ph.D.
OpioidAddiction2.0
LightUniversity 24
Summary
In Part II, Dr. Jenkins and Dr. Mintle continue their discussion of opioid addiction and also
explorevarioustreatmentoptionsandproperprotocolsforpainmanagement, includingnon-
pharmacological strategies. A discussion on prevention, the role of faith, and the potential
influenceoftheChurchisalsooffered.
LearningObjectives
1. Participantswillexploretheroleofopioidsinmedicationandtreatmentsofpain.
2. Participantswilldiscussnon-pharmaceuticaltreatmentsforpain.
3. ParticipantswilldiscoverhowChristiancaregiversandthechurchcanworktogetherto
preventopioidabuseandpromoterecovery.

OpioidAddiction2.0
LightUniversity 25
I. TreatmentofOpioidUseDisorders
A. MedicationAssistedTreatment
1. Methadone:blockseuphoriceffects;reduceswithdrawalsymptoms
2. Buprenorphine:diminisheseffectsofdependency
3. Naltrexone:blockseuphoriceffects;reducescravings;binds&blocks(vs.activates)
opioidreceptors
B. Non-MedicationTypesofTreatment
1. Residential(inpatient)Treatments
2. GroupTherapy
3. IndividualPsychotherapy
• PainManagement
• TreatingCo-occurringDisorders
• AddressingDrugUseDisorder(s)
C. Modalities
1. CognitiveBehavioralTherapy(CBT)
2. MotivationalInterviewing(MI)
3. MotivationalEnhancementTherapy(MET)
4. Mindfulness-BasedStressReduction(MBSR)

OpioidAddiction2.0
LightUniversity 26
D. Non-PharmTreatmentsforChronicPain
1. Themoreattentionyougivetopain,themoreyouincreasepain
2. CBT:Thoughtsandemotionsturnupordownthevolumeofpain
3. Cognitiverestructuring(reframing):Dealwithnegativecognitionsandbeliefsabout
pain;expectationsforpain
4. Relaxationinterventions
• Guidedimagery
• Progressivemusclerelaxation
• Mindfulmeditation
• Musictherapy
• Hypnosis
• Biofeedback
• Copingskillstraining
• Physicalactivity
• Supportivetherapies
• Grouptherapies
• Stressmanagement
II. Q&AwiththePresenters
A. Addiction:IsitaDiseaseoraChoice?
1. Addictionbeginswithachoice.
2. Addictionisanacquireddisease.
3. Recoverybeginswithachoice.

OpioidAddiction2.0
LightUniversity 27
B. WhatAretheConsequencesofOpioidAbuse?
1. Constrictionoflifestyle
• Acheapsubstituteforjoyandpleasure
2. Physicalwithdrawalsymptoms
3. Shameandguilt
C. HasSocietyChangeditsViewsonOpioidUse?
1. Theuserprofilehaschanged
2. Asperceivedriskgoesdown,usegoesup,andasperceivedriskgoesup,usegoes
down.
D. WhatCantheChurchDo?
1. Preventionandrecoveryeffortsbythefaithcommunityareamongthemost
effectivesocietaltreatments.
2. Understandandseektochangetheculture.
• Thebestpreventionistoneverstart
3. Thechurchmuststarttalkingabouttheseissues.
4. Educateparents.
• Keepmedicationslockedup.

OpioidAddiction2.0
LightUniversity 28
5. Startsupportgroups.
6. Ministertothespiritualneedsofaddicts.
7. Pray!
8. Connectwithotherchurches.
E. HowDoYouIntervenewithaFriendorFamilyMember?
1. Revisittheoriginalconceptualizationsoftoughlove.
2. Beanexampleofwhatdeeppersonalchangelookslike.
3. Speakthetruthinlove.
F. TheFinalTakeaway
1. Addictionscanbeovercome.
2. Counselorsneedtositwithothersintheirshame.

OpioidAddiction2.0
LightUniversity 29
ResourcesAgency for Healthcare Research and Quality. (2016). Opioid-related hospitalizations up 64 percent nationwide
between 2005-2014; First state-by-state analysis showswide variations [Press release]. Retrieved fromhttp://www.ahrq.gov/news/newsroom/press-releases/opioid-related-hospitalizations.html.
AmericanPsychologicalAssociation.(2017).Overcomingopioidabuse:Howpsychologistshelppeoplewithopioiddependenceandaddiction[Factsheet].Retrievedfromhttp://www.apa.org/helpcenter/opioid-abuse.pdf.
AmericanSocietyofAddictionMedicine.(2016).Opioidaddiction:2016facts&figures[Factsheet].Retrievedfromhttps://www.asam.org/docs/default-source/advocacy/opioid-addiction-disease-facts-figures.pdf.
CentersforDiseaseControlandPrevention.(2017).Annualsurveillancereportofdrug-relatedrisksandoutcomes:United States, 2017. Retrieved from https://www.cdc.gov/drugoverdose/pdf/pubs/2017cdc-drug-surveillance-report.pdf
Guy,G.P,Zhang,K.,Bohm,M.K.,Losby,J.,Lewis,B.,Young,R.,...Dowell,D.(2017).Vitalsigns:Changesinopioidprescribing in the United States, 2006–2015.Morbidity andMortalityWeekly Report, 66(26), 697-704.Retrievedfromhttps://www.cdc.gov/mmwr/volumes/66/wr/pdfs/mm6626a4.pdf.
National Institute of Drug Abuse. (2017a). Opioid Crisis. Retrieved from https://www.drugabuse.gov/drugs-abuse/opioids/opioid-crisis.
NationalInstituteofDrugAbuse.(2017b).Researchontheuseandmisuseoffentanylandothersyntheticopioids.Retrievedfromhttps://www.drugabuse.gov/about-nida/legislative-activities/testimony-to-congress/2017/research-use-misuse-fentanyl-other-synthetic-opioids.
SubstanceAbuseMentalHealthServicesAdministration.(2017).KeysubstanceuseandmentalhealthindicatorsintheUnitedStates:Results fromthe2016NationalSurveyonDrugUseandHealth (HHSPublicationNo.SMA 17-5044, NSDUH Series H-52). Rockville,MD: Center for Behavioral Health Statistics and Quality,Substance Abuse and Mental Health Services Administration. Retrieved fromhttps://www.samhsa.gov/data/.

OpioidAddiction2.0
LightUniversity 30
Copyright2017LightUniversity
AllRightsReserved.
Nopartofthispublicationmaybereproducedinanyformwithouttheexpressedwritten
permissionofLightUniversityortheAmericanAssociationofChristianCounselors.
LightUniversity
POBox739
VA24551
MemberServices:1-800-526-8673