open access original research initiatives for improving
TRANSCRIPT
1Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Initiatives for improving delayed discharge from a hospital setting: a scoping review
Lauren Cadel ,1,2 Sara J T Guilcher ,2,3,4,5 Kristina Marie Kokorelias,3 Jason Sutherland,6 Jon Glasby,7 Tara Kiran,4,5,8,9 Kerry Kuluski1,4
To cite: Cadel L, Guilcher SJT, Kokorelias KM, et al. Initiatives for improving delayed discharge from a hospital setting: a scoping review. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
► Prepublication history and additional material for this paper is available online. To view these files, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjopen- 2020- 044291).
Received 31 August 2020Revised 18 January 2021Accepted 25 January 2021
For numbered affiliations see end of article.
Correspondence toLauren Cadel; lauren. cadel@ thp. ca
Original research
© Author(s) (or their employer(s)) 2021. Re- use permitted under CC BY- NC. No commercial re- use. See rights and permissions. Published by BMJ.
ABSTRACTObjective The overarching objective of the scoping review was to examine peer reviewed and grey literature for best practices that have been developed, implemented and/or evaluated for delayed discharge involving a hospital setting. Two specific objectives were to review what the delayed discharge initiatives entailed and identify gaps in the literature in order to inform future work.Design Scoping review.Methods Electronic databases and websites of government and healthcare organisations were searched for eligible articles. Articles were required to include an initiative that focused on delayed discharge, involve a hospital setting and be published between 1 January 2004 and 16 August 2019. Data were extracted using Microsoft Excel. Following extraction, a policy framework by Doern and Phidd was adapted to organise the included initiatives into categories: (1) information sharing; (2) tools and guidelines; (3) practice changes; (4) infrastructure and finance and (5) other.Results Sixty- six articles were included in this review. The majority of initiatives were categorised as practice change (n=36), followed by information sharing (n=19) and tools and guidelines (n=19). Numerous initiatives incorporated multiple categories. The majority of initiatives were implemented by multidisciplinary teams and resulted in improved outcomes such as reduced length of stay and discharge delays. However, the experiences of patients and families were rarely reported. Included initiatives also lacked important contextual information, which is essential for replicating best practices and scaling up.Conclusions This scoping review identified a number of initiatives that have been implemented to target delayed discharges. While the majority of initiatives resulted in positive outcomes, delayed discharges remain an international problem. There are significant gaps and limitations in evidence and thus, future work is warranted to develop solutions that have a sustainable impact.
INTRODUCTIONA delayed hospital discharge (known as alternate level of care (ALC) in Canada and delayed transfer of care in the UK) occurs when a patient is medically approved to be discharged, but remains in hospital for non- medical reasons (eg, waiting for a long- term care bed to become available or to transfer
home with services).1 While waiting for their next destination, patients’ level of care and activation often decrease or stop entirely. Delayed discharge can result in hospital patient flow issues (eg, emergency service backlogs, cancelled surgeries, delays in medically necessary care),2 increased health-care costs,3 an increased risk of functional decline,4 5 falls,6 hospital- related adverse events (eg, medication error, exposure to infectious disease),6 7 mortality,8 as well as poor patient and family experiences.9
Patients who experienced a delayed discharge in previous studies exhibited the following characteristics: female,10 older,10 11 physically or cognitively impaired.4 12–15 Patients have also shown to exhibit aggressive behaviours,16 use assistive devices17 and have psychiatric conditions,10 neurological disorders15 and/or multimor-bidity.17 In addition to these patient- level factors, there are a number of system- level factors that contribute to delayed discharges, including long wait lists for long- term care facilities,5 17–19 rehabilitation or other postacute care (eg, home care),11 12 20–23 the lack of culturally and religiously diverse long- term care facilities,15 limited or absent hospital services on weekends24 and organ-isational delays (eg, administrative delays, delayed assessments).24 25 There are also
Strengths and limitations of this study
► To our knowledge, this is the first scoping review to identify best practices for delayed discharges in-volving a hospital setting.
► The Preferred Reporting Items for Systematic Reviews and Meta- Analyses extension for Scoping Reviews Checklist was followed.
► A comprehensive search of peer reviewed and grey literature was conducted.
► A critical appraisal of the interventions was not performed.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

2 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
different pressures and priorities across sectors, with little incentive to work together as a system. For example, while hospitals may be focused on efficiency and throughput, community- based organisations may be focused on empowerment, longer- term quality of life outcomes and working at a pace that works for patients and families. The funding structure of hospitals and healthcare systems can also have an impact on overall patient flow, including discharge delays. Although there is wide variation in funding structures within and across countries, there is potential for funding to either incentivise or disincen-tivise timely hospital discharges.26–30
The combination of patient- level and system- level factors contributing to delayed discharges can also have a large financial impact on patients, families, healthcare providers and the healthcare system.3 A recent system-atic review reported that delayed discharges cost approx-imately £200–565 ($C320–$C900) per patient, per day.3 Further, it was estimated that the National Health Service (NHS) (England) spends £820 million ($C1.3 billion) every year on patients who have a discharge delay.31 Simi-larly, a recent report from Canada stated that three hospi-tals located in Ottawa, Ontario, spend approximately $C250 000 per day (combined) on patients occupying beds at a level of care they no longer require.32 In addi-tion to large costs for hospitals and healthcare systems, delayed hospital discharges can result in out- of- pocket costs for patients and families.33 Increased out- of- pocket costs, in addition to the other uncertainties associated with a delay, can heighten stress for patients and families, contribute to poor experiences and compromise quality of life.9
Overall, delayed hospital discharges are problematic internationally, highlighting a need to identify best prac-tices and current initiatives that are concentrating on solutions to this complex problem. To date, the majority of published literature on delayed discharge has focused on risk factors and characteristics of patients who experi-ence delayed discharge. There has been a limited focus on initiatives that address the delayed discharge problem. Therefore, the purpose of this scoping review was to examine peer reviewed and grey literature (literature published through non- traditional means) for initiatives that have been developed and/or evaluated for delayed discharge from a hospital setting, with the goal of iden-tifying best practices for reducing delayed discharge. A scoping review methodology was appropriate for addressing this goal, in order to identify the types of avail-able evidence on this topic, examine key characteristics relating to initiatives for delayed discharge and to identity knowledge gaps.34
METHODSThis review followed the scoping review methodology outlined by Levac et al,35 as well as the recently developed Preferred Reporting Items for Systematic Reviews and Meta- Analyses extension for Scoping Reviews (see online
supplemental table 1).36 A protocol for this scoping review was developed in consultation with a librarian at the University of Toronto, with continuous input from members of the research team.
Stage 1: identifying the research questionThe research question developed to lead this scoping review was: what is known in the literature about initia-tives (eg, strategies, programmes, interventions) that have been developed, implemented and/or evaluated for delayed discharge involving a hospital setting? The two main aims were: (1) to review what delayed discharge initiatives entail (eg, characteristics, outcomes) and (2) to identify gaps in the literature in order to inform future studies.
Stage 2: identifying relevant articlesThe search strategy was developed with a librarian at the University of Toronto and through consultations with an advisory group and collaborators who have experience in clinical practice or administration (see online supple-mental table 2 for Medline search strategy). Each search strategy was adapted for the specific database using appro-priate command line syntax and indexing. The following are examples of keywords searched using Boolean oper-ators, proximity operators, wild cards and truncations: ALC, delayed discharge, delayed transfer, bed blocking, strategy, model, intervention, programme, policy.
Electronic databases were searched for relevant articles. The following electronic databases were searched on 16 August 2019: MEDLINE (Ovid Interface), EMBASE (Ovid Interface), AMED (Ovid Interface), Cumulative Index to Nursing and Allied Health Literature (EBSCO Inter-face) and Cochrane Library. Grey literature was searched on the following databases and repositories: OpenGrey, Health Services Research Projects in Progress, UpToDate, Community Research and Development Information Services and TSpace, as well as on numerous national and international healthcare and government websites. We also reached out to key stakeholders, including members of our advisory group, to send us relevant reports and presentations.
Stage 3: study selectionFor inclusion, articles (peer- reviewed and grey literature) were required to meet the following criteria: (1) focused on delayed discharge, (2) included an initiative to address delayed discharge, (3) involved a hospital setting, (4) published between 1 January 2004 and 16 August 2019 and (5) peer- reviewed or grey literature. We focused our inclusion on initiatives involving a hospital setting because this is where the problem of delayed discharges surfaces. Articles were excluded if they met any one of the following criteria: (1) focused on changing the threshold/timing of discharge (early discharge), (2) books, book chapters, opinion pieces or editorials, (3) grey literature that did not sufficiently describe the initiative implemented (eg, implementation process, location, population, impact);
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

3Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
(4) protocols, trial papers or chart reviews or (5) confer-ence abstracts or articles without an accessible full text. Articles were excluded for criteria one (changing the threshold/timing of discharge) because the rationale for having an earlier discharge was often focused on other factors such as cost- savings by reducing length of stay, rather than specifically addressing a delayed discharge. Articles were excluded if they met criteria two (books, book chapters, opinion pieces or editorials) to elimi-nate articles with potential personal biases and summa-ries of peer- reviewed literature. Grey literature that did not provide sufficient details on the initiative (such as lacking a description of the components of the initiative) were excluded. Articles published more than 15 years ago, before 1 January 2004, were excluded to ensure the initiatives included in this scoping review were relevant to more current health service practices.
Articles identified from the database searches were imported into EndNote X9, a reference management software, where they were deduplicated following Bram-er’s method.37 The initial database searches identified 22 704 articles, which were reduced to 15 824 following deduplication (figure 1). The titles and abstracts of the articles were reviewed on Covidence, a software platform for systematic and scoping reviews.38 The research team (LC, KK, SJTG, KMK and JK) independently screened the titles and abstracts of 40 articles to test their agreement. The reviewers had a good per cent agreement (85%), so the remaining articles were divided among the team and screened by single reviewers (LC, KMK and JK). All disagreements were discussed in- person by the reviewers until a consensus was reached; minor revisions were made to the eligibility criteria to ensure clarity and consistency. Following title and abstract screening, articles were
reviewed at the full- text level. Thirty full- text articles were independently screened by the research team (LC, KK, SJTG, KMK, JK and MA) to test their interrater agree-ment. The remaining full- text articles (peer- reviewed and grey literature) were double screened by four reviewers (LC, KMK, JK and MA).
Stage 4: charting the dataThe data were charted by two reviewers (LC and KMK) using a data extraction form in Microsoft Excel. The form was developed and tested by the research team in a series of team meetings prior to the extraction of all data. We conducted spot checking of extracted data from 15% of the included articles to ensure complete-ness and accuracy of the extracted data. Any questions that arose during the charting process were discussed by the team. Charted data contained the following information: general information, study characteristics, population characteristics, initiative characteristics, characteristics of delayed discharge, study outcomes and conclusions.
Stage 5: collating, summarising and reporting resultsMicrosoft Excel was used to conduct a descriptive quanti-tative analysis of the included articles, as well as facilitate qualitative thematic analysis. The thematic analysis of the charted data was an inductive and iterative process, in which the team (LC, SJTG, KMK and KK) met in- person to discuss high level concepts and identified common themes across the included articles. When reviewing the extracted data, we found that the strategies appeared to cluster into core categories, which aligned with a concep-tual framework developed by Doern and Phidd.39 This framework classifies policy instruments/tools along a continuum (from those that are least coercive like infor-mation sharing to those that are more coercive like public ownership or, in our case, new infrastructure). We deduc-tively applied Doern and Phidd’s categories to classify our findings, with some minor adaptations. The five adapted categories were not mutually exclusive and included: (1) information sharing (live information sharing and docu-mented recommendations); (2) tools and guidelines; (3) practice changes; (4) infrastructure and finance and (5) other (see table 1 for category descriptions and exam-ples). The categories assisted with the organisation and presentation of the data.
Stage 6: consultationThe research team presented findings of the scoping review to key stakeholders (eg, hospital staff, patient and caregiver partners) through the planning process and analysis of results. These meetings were used to inform search terms, gather relevant documents, obtain feedback on the categorisation/organisation of initiatives, as well as identify knowledge gaps in order to develop targeted and actionable recommendations for future practice, policy and research.
Figure 1 PRISMA flow diagram of included articles. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta- Analyses.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

4 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Patient and public involvementAn advisory council (patient and caregiver partners), along with providers, managers and organisational leaders identified the lack of understanding about the state of evidence around best practices for delayed discharges, which informed the research question for this scoping review. The advisory council was involved with planning meetings where they provided feedback on the search terms and analysis. Results will be disseminated to the advisory council through presentations and a lay summary.
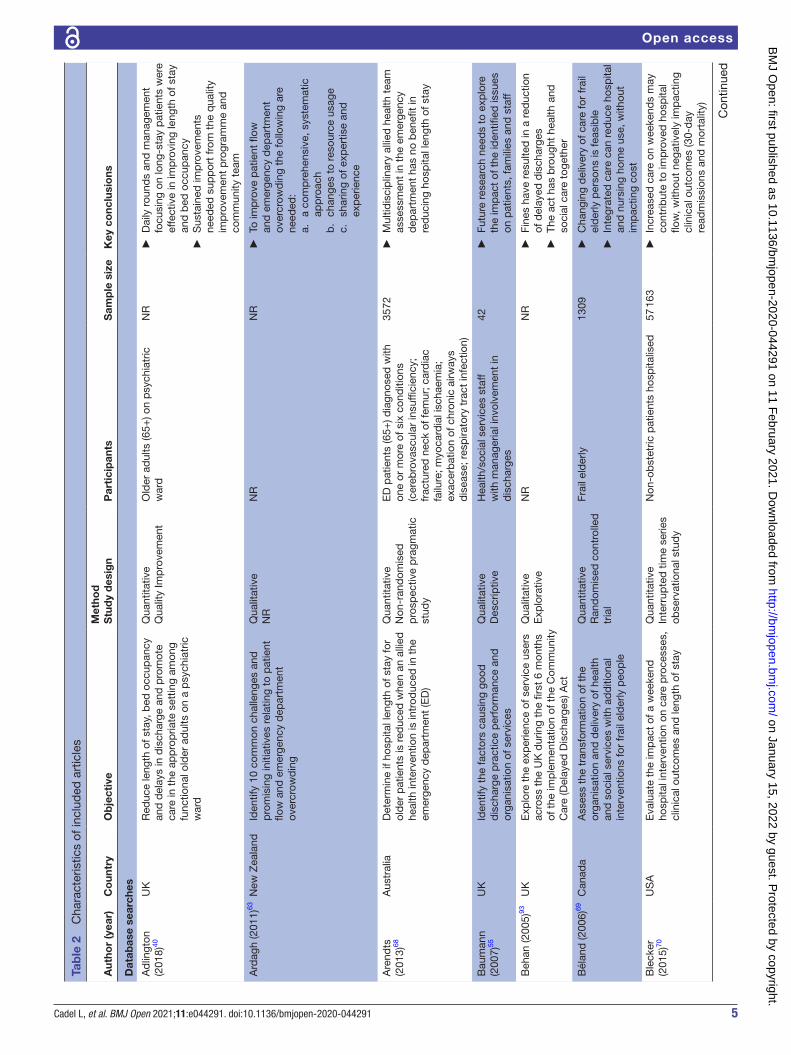
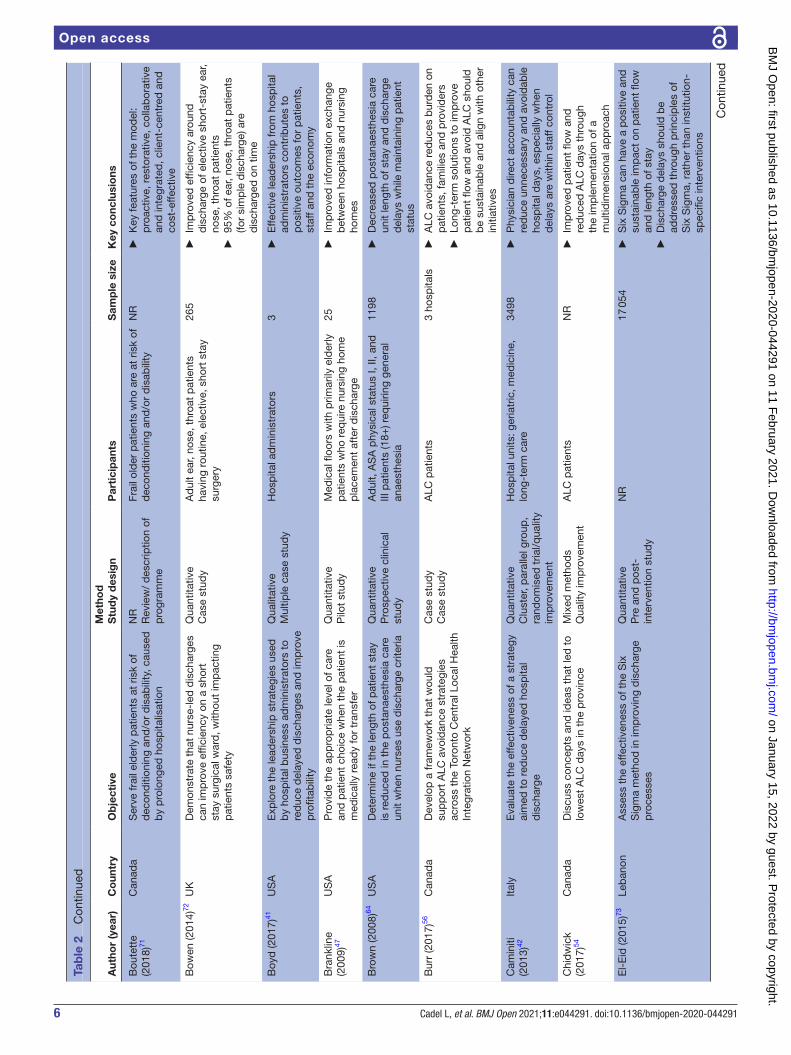
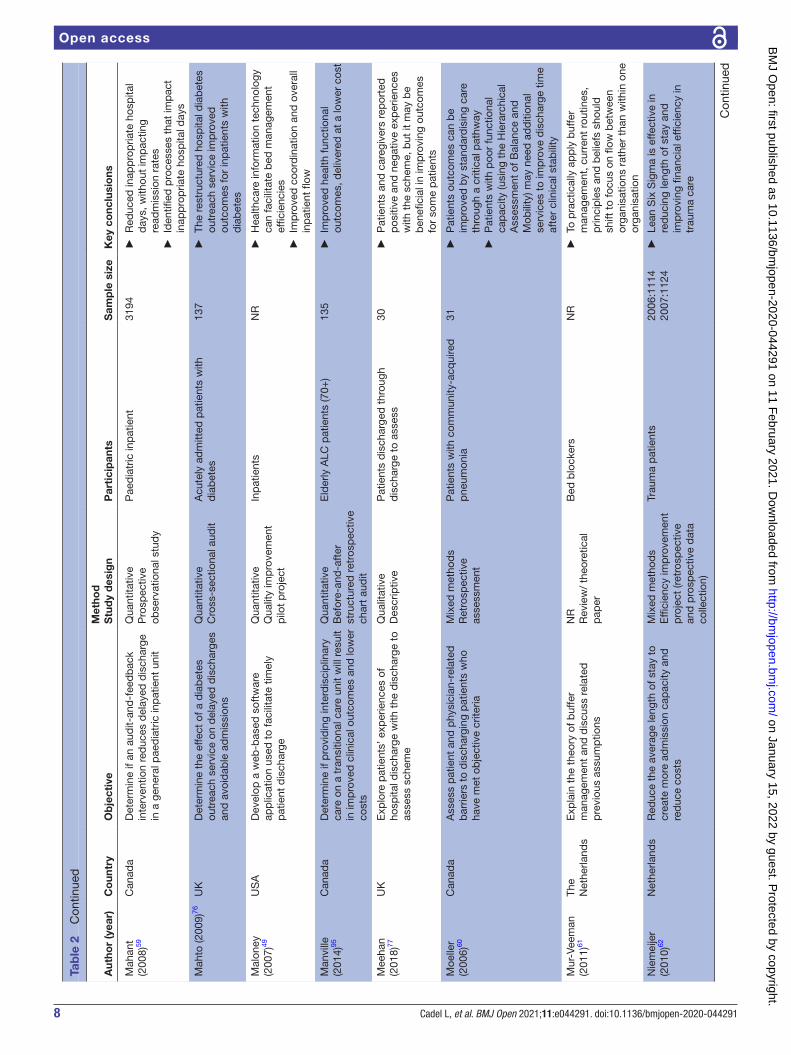
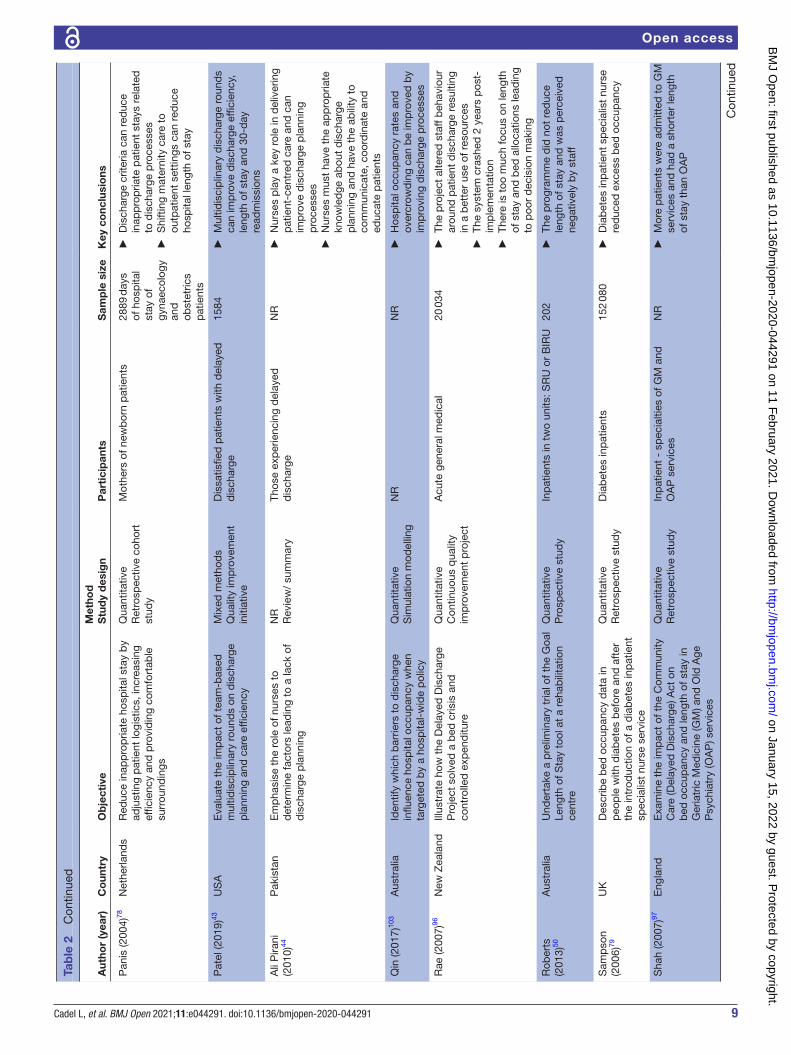
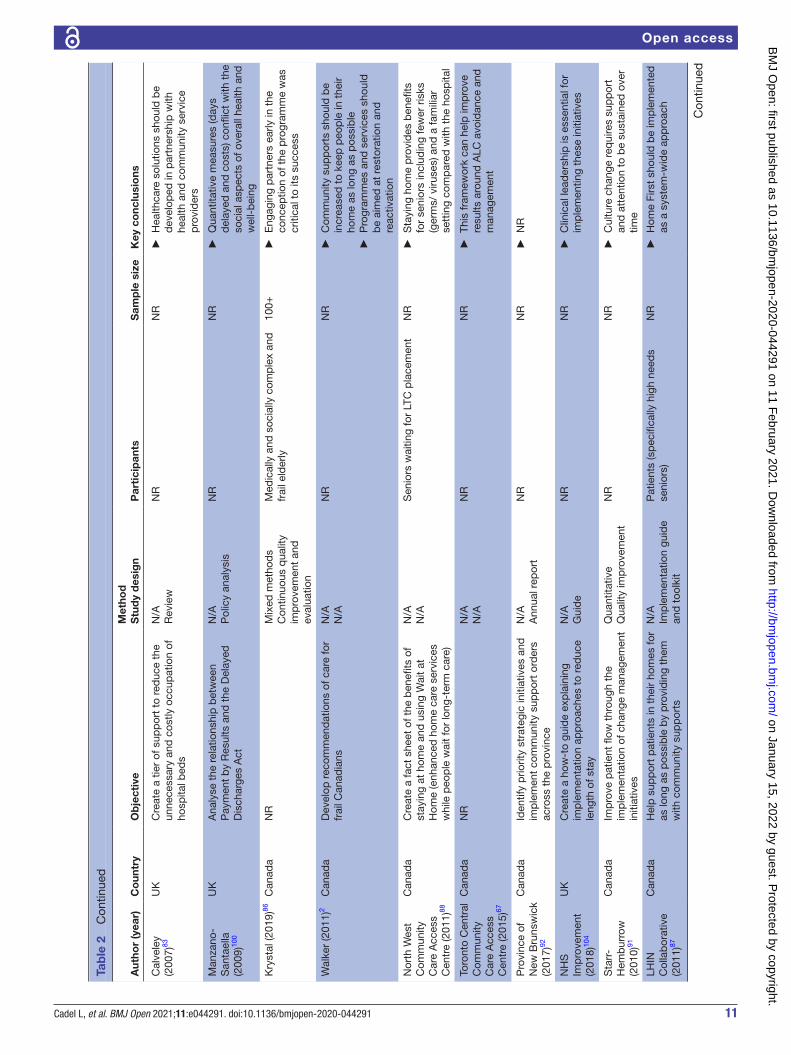
RESULTSStudy characteristicsThe database search identified 15 824 unique articles that were screened for eligibility; following title/abstract and full- text review, 66 articles were included in this scoping review, 49 articles from the database searches and 17 articles from the grey literature searches (figure 1). The majority of included articles were quantitative studies (n=34), with a few qualitative (n=5), mixed methods (n=6) or other designs (policy analyses, reviews, case studies and presentations; n=21). There was a large variety of study designs, with few randomised trials and prospective studies. Most initiatives were evaluated (n=42), with different types of evaluations such as process evaluations and outcome evaluations. The UK (n=21), USA (n=18) and Canada (n=17) were the most common countries where studies were conducted. Based on the year of publication, there was a fairly even distribution of peer- reviewed articles across the years of inclusion (from 2004 to 2019); however, the majority of grey literature was published in the last 10 years. Table 2 describes the char-acteristics of included articles.
The initiatives most commonly targeted adults and older adults; however, there were some initiatives targeting the paediatric population. Specific characteristics of the study population (ie, age, sex, gender, ethnicity/race, income level, education, marital status, household composition, employment status, comorbidities) were not reported in the majority of articles. Most peer- reviewed articles (n=31) defined a delayed discharge; however, there was a wide variety of definitions for these terms (see online supplemental table 3). The most common definition for delayed discharge was when a patient was identified as medically ready for discharge, but remained in hospital. Table 3 describes the initiative characteristics.
Based on Doern and Phidd’s adapted framework,39 we categorised the included initiatives as: information sharing (n=19); tools and guidelines (n=19); practice changes (n=36); infrastructure and finance (n=10); or other (n=3), which are described in detail below (see figure 2). Numerous articles used a combination of cate-gories in their initiatives (eg, information sharing and practice change).
Information sharingThe information sharing category included initiatives that promoted communication, leadership from senior staff and information exchange within or across organi-sations.2 40–55 The majority of information sharing initia-tives included team meetings and huddles to facilitate communication through in- person interactions between staff, and less often between staff and patients/fami-lies.40 41 43 44 46 Information sharing was promoted between multidisciplinary teams and patients to improve length of stay and continuity of care. For example, Adlington et al implemented Plan Do Study Act cycles during weekly quality improvement meetings, in which driver diagrams
Table 1 Categories, descriptions and examples of initiative categorisation
Category name Description Examples
Information SharingA—live sharingB—recommended initiatives— calls to action
► A—information sharing through in- person or technology- based communication (synchronous communication)
► B—information sharing through documents which share suggestions, recommendations or for information purposes (motivation)
► A—rounding, team meetings, one- on- on communication
► B—examples: suggested strategies (or ‘calls to action’) which ranged from recommending investments in new long- term care beds, increasing funding for behavioural supports, audits and reports, encouraging team building
Tools and guidelines ► Tangible/concrete guides to inform practice ► Implemented tool/guidance document that is being used in the healthcare system
► Toolkits, guidelines, escalation processes, frameworks
Practice changes ► A change in how care is delivered ► Nurse- led discharges, roles of providers and/or composition of team are organised differently
Infrastructure and finance ► Tangible structural or financial changes ► Financial penalties/incentives, building more hospital, rehabilitation or long- term care beds
Other initiatives ► Different initiative that does not fit into any of the above categories
► Statistical models (predictive modelling)
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
5Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Tab
le 2
C
hara
cter
istic
s of
incl
uded
art
icle
s
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Dat
abas
e se
arch
es
Ad
lingt
on
(201
8)40
UK
Red
uce
leng
th o
f sta
y, b
ed o
ccup
ancy
an
d d
elay
s in
dis
char
ge a
nd p
rom
ote
care
in t
he a
pp
rop
riate
set
ting
amon
g fu
nctio
nal o
lder
ad
ults
on
a p
sych
iatr
ic
war
d
Qua
ntita
tive
Qua
lity
Imp
rove
men
tO
lder
ad
ults
(65+
) on
psy
chia
tric
w
ard
NR
►
Dai
ly r
ound
s an
d m
anag
emen
t fo
cusi
ng o
n lo
ng- s
tay
pat
ient
s w
ere
effe
ctiv
e in
imp
rovi
ng le
ngth
of s
tay
and
bed
occ
upan
cy
►S
usta
ined
imp
rove
men
ts
need
ed s
upp
ort
from
the
qua
lity
imp
rove
men
t p
rogr
amm
e an
d
com
mun
ity t
eam
Ard
agh
(201
1)63
New
Zea
land
Iden
tify
10 c
omm
on c
halle
nges
and
p
rom
isin
g in
itiat
ives
rel
atin
g to
pat
ient
flo
w a
nd e
mer
genc
y d
epar
tmen
t ov
ercr
owd
ing
Qua
litat
ive
NR
NR
NR
►
To im
pro
ve p
atie
nt fl
ow
and
em
erge
ncy
dep
artm
ent
over
crow
din
g th
e fo
llow
ing
are
need
ed:
a.
a co
mp
rehe
nsiv
e, s
yste
mat
ic
app
roac
hb
. ch
ange
s to
res
ourc
e us
age
c.
shar
ing
of e
xper
tise
and
ex
per
ienc
e
Are
ndts
(2
013)
68A
ustr
alia
Det
erm
ine
if ho
spita
l len
gth
of s
tay
for
old
er p
atie
nts
is r
educ
ed w
hen
an a
llied
he
alth
inte
rven
tion
is in
trod
uced
in t
he
emer
genc
y d
epar
tmen
t (E
D)
Qua
ntita
tive
Non
- ran
dom
ised
p
rosp
ectiv
e p
ragm
atic
st
udy
ED
pat
ient
s (6
5+) d
iagn
osed
with
on
e or
mor
e of
six
con
diti
ons
(cer
ebro
vasc
ular
insu
ffici
ency
; fr
actu
red
nec
k of
fem
ur; c
ard
iac
failu
re; m
yoca
rdia
l isc
haem
ia;
exac
erb
atio
n of
chr
onic
airw
ays
dis
ease
; res
pira
tory
tra
ct in
fect
ion)
3572
►
Mul
tidis
cip
linar
y al
lied
hea
lth t
eam
as
sess
men
t in
the
em
erge
ncy
dep
artm
ent
has
no b
enefi
t in
re
duc
ing
hosp
ital l
engt
h of
sta
y
Bau
man
n (2
007)
55U
KId
entif
y th
e fa
ctor
s ca
usin
g go
od
dis
char
ge p
ract
ice
per
form
ance
and
or
gani
satio
n of
ser
vice
s
Qua
litat
ive
Des
crip
tive
Hea
lth/s
ocia
l ser
vice
s st
aff
with
man
ager
ial i
nvol
vem
ent
in
dis
char
ges
42
►Fu
ture
res
earc
h ne
eds
to e
xplo
re
the
imp
act
of t
he id
entifi
ed is
sues
on
pat
ient
s, fa
mili
es a
nd s
taff
Beh
an (2
005)
93U
KE
xplo
re t
he e
xper
ienc
e of
ser
vice
use
rs
acro
ss t
he U
K d
urin
g th
e fir
st 6
mon
ths
of t
he im
ple
men
tatio
n of
the
Com
mun
ity
Car
e (D
elay
ed D
isch
arge
s) A
ct
Qua
litat
ive
Exp
lora
tive
NR
NR
►
Fine
s ha
ve r
esul
ted
in a
red
uctio
n of
del
ayed
dis
char
ges
►
The
act
has
bro
ught
hea
lth a
nd
soci
al c
are
toge
ther
Bél
and
(200
6)69
Can
ada
Ass
ess
the
tran
sfor
mat
ion
of t
he
orga
nisa
tion
and
del
iver
y of
hea
lth
and
soc
ial s
ervi
ces
with
ad
diti
onal
in
terv
entio
ns fo
r fr
ail e
lder
ly p
eop
le
Qua
ntita
tive
Ran
dom
ised
con
trol
led
tr
ial
Frai
l eld
erly
1309
►
Cha
ngin
g d
eliv
ery
of c
are
for
frai
l el
der
ly p
erso
ns is
feas
ible
►
Inte
grat
ed c
are
can
red
uce
hosp
ital
and
nur
sing
hom
e us
e, w
ithou
t im
pac
ting
cost
Ble
cker
(2
015)
70U
SA
Eva
luat
e th
e im
pac
t of
a w
eeke
nd
hosp
ital i
nter
vent
ion
on c
are
pro
cess
es,
clin
ical
out
com
es a
nd le
ngth
of s
tay
Qua
ntita
tive
Inte
rrup
ted
tim
e se
ries
obse
rvat
iona
l stu
dy
Non
- ob
stet
ric p
atie
nts
hosp
italis
ed57
163
►
Incr
ease
d c
are
on w
eeke
nds
may
co
ntrib
ute
to im
pro
ved
hos
pita
l flo
w, w
ithou
t ne
gativ
ely
imp
actin
g cl
inic
al o
utco
mes
(30-
day
r e
adm
issi
ons
and
mor
talit
y)
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
6 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Bou
tett
e (2
018)
71C
anad
aS
erve
frai
l eld
erly
pat
ient
s at
ris
k of
d
econ
diti
onin
g an
d/o
r d
isab
ility
, cau
sed
b
y p
rolo
nged
hos
pita
lisat
ion
NR
Rev
iew
/ d
escr
iptio
n of
p
rogr
amm
e
Frai
l old
er p
atie
nts
who
are
at
risk
of
dec
ond
ition
ing
and
/or
dis
abili
tyN
R
►K
ey fe
atur
es o
f the
mod
el:
pro
activ
e, r
esto
rativ
e, c
olla
bor
ativ
e an
d in
tegr
ated
, clie
nt- c
entr
ed a
nd
cost
- effe
ctiv
e
Bow
en (2
014)
72U
KD
emon
stra
te t
hat
nurs
e- le
d d
isch
arge
s ca
n im
pro
ve e
ffici
ency
on
a sh
ort
stay
sur
gica
l war
d, w
ithou
t im
pac
ting
pat
ient
s sa
fety
Qua
ntita
tive
Cas
e st
udy
Ad
ult
ear,
nose
, thr
oat
pat
ient
s ha
ving
rou
tine,
ele
ctiv
e, s
hort
sta
y su
rger
y
265
►
Imp
rove
d e
ffici
ency
aro
und
d
isch
arge
of e
lect
ive
shor
t- st
ay e
ar,
nose
, thr
oat
pat
ient
s
►95
% o
f ear
, nos
e, t
hroa
t p
atie
nts
(for
sim
ple
dis
char
ge) a
re
dis
char
ged
on
time
Boy
d (2
017)
41U
SA
Exp
lore
the
lead
ersh
ip s
trat
egie
s us
ed
by
hosp
ital b
usin
ess
adm
inis
trat
ors
to
red
uce
del
ayed
dis
char
ges
and
imp
rove
p
rofit
abili
ty
Qua
litat
ive
Mul
tiple
cas
e st
udy
Hos
pita
l ad
min
istr
ator
s3
►
Effe
ctiv
e le
ader
ship
from
hos
pita
l ad
min
istr
ator
s co
ntrib
utes
to
pos
itive
out
com
es fo
r p
atie
nts,
st
aff a
nd t
he e
cono
my
Bra
nklin
e (2
009)
47U
SA
Pro
vid
e th
e ap
pro
pria
te le
vel o
f car
e an
d p
atie
nt c
hoic
e w
hen
the
pat
ient
is
med
ical
ly r
ead
y fo
r tr
ansf
er
Qua
ntita
tive
Pilo
t st
udy
Med
ical
floo
rs w
ith p
rimar
ily e
lder
ly
pat
ient
s w
ho r
equi
re n
ursi
ng h
ome
pla
cem
ent
afte
r d
isch
arge
25
►Im
pro
ved
info
rmat
ion
exch
ange
b
etw
een
hosp
itals
and
nur
sing
ho
mes
Bro
wn
(200
8)64
US
AD
eter
min
e if
the
leng
th o
f pat
ient
sta
y is
red
uced
in t
he p
osta
naes
thes
ia c
are
unit
whe
n nu
rses
use
dis
char
ge c
riter
ia
Qua
ntita
tive
Pro
spec
tive
clin
ical
st
udy
Ad
ult,
AS
A p
hysi
cal s
tatu
s I,
II, a
nd
III p
atie
nts
(18+
) req
uirin
g ge
nera
l an
aest
hesi
a
1198
►
Dec
reas
ed p
osta
naes
thes
ia c
are
unit
leng
th o
f sta
y an
d d
isch
arge
d
elay
s w
hile
mai
ntai
ning
pat
ient
st
atus
Bur
r (2
017)
56C
anad
aD
evel
op a
fram
ewor
k th
at w
ould
su
pp
ort
ALC
avo
idan
ce s
trat
egie
s ac
ross
the
Tor
onto
Cen
tral
Loc
al H
ealth
In
tegr
atio
n N
etw
ork
Cas
e st
udy
Cas
e st
udy
ALC
pat
ient
s3
hosp
itals
►
ALC
avo
idan
ce r
educ
es b
urd
en o
n p
atie
nts,
fam
ilies
and
pro
vid
ers
►
Long
- ter
m s
olut
ions
to
imp
rove
p
atie
nt fl
ow a
nd a
void
ALC
sho
uld
b
e su
stai
nab
le a
nd a
lign
with
oth
er
initi
ativ
es
Cam
initi
(2
013)
42Ita
lyE
valu
ate
the
effe
ctiv
enes
s of
a s
trat
egy
aim
ed t
o re
duc
e d
elay
ed h
osp
ital
dis
char
ge
Qua
ntita
tive
Clu
ster
, par
alle
l gro
up,
rand
omis
ed t
rial/q
ualit
y im
pro
vem
ent
Hos
pita
l uni
ts: g
eria
tric
, med
icin
e,
long
- ter
m c
are
3498
►
Phy
sici
an d
irect
acc
ount
abili
ty c
an
red
uce
unne
cess
ary
and
avo
idab
le
hosp
ital d
ays,
esp
ecia
lly w
hen
del
ays
are
with
in s
taff
cont
rol
Chi
dw
ick
(201
7)54
Can
ada
Dis
cuss
con
cep
ts a
nd id
eas
that
led
to
low
est
ALC
day
s in
the
pro
vinc
eM
ixed
met
hod
sQ
ualit
y im
pro
vem
ent
ALC
pat
ient
sN
R
►Im
pro
ved
pat
ient
flow
and
re
duc
ed A
LC d
ays
thro
ugh
the
imp
lem
enta
tion
of a
m
ultid
imen
sion
al a
pp
roac
h
El-
Eid
(201
5)73
Leb
anon
Ass
ess
the
effe
ctiv
enes
s of
the
Six
S
igm
a m
etho
d in
imp
rovi
ng d
isch
arge
p
roce
sses
Qua
ntita
tive
Pre
and
pos
t-
inte
rven
tion
stud
y
NR
17 0
54
►S
ix S
igm
a ca
n ha
ve a
pos
itive
and
su
stai
nab
le im
pac
t on
pat
ient
flow
an
d le
ngth
of s
tay
►
Dis
char
ge d
elay
s sh
ould
be
add
ress
ed t
hrou
gh p
rinci
ple
s of
S
ix S
igm
a, r
athe
r th
an in
stitu
tion-
sp
ecifi
c in
terv
entio
ns
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

7Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Gau
ghan
(2
015)
101
Eng
land
Inve
stig
ate
the
red
uctio
n in
hos
pita
l b
ed- b
lock
ing
due
to
a gr
eate
r su
pp
ly o
f nu
rsin
g ho
me
bed
s or
red
uced
cos
ts
Qua
ntita
tive
Sta
tistic
al m
odel
ling
- E
mp
irica
l ana
lysi
s
Pat
ient
s w
aitin
g fo
r ho
spita
l d
isch
arge
NR
►
Imp
rove
d c
oord
inat
ion
bet
wee
n he
alth
and
long
- ter
m c
are
is
esse
ntia
l for
ad
dre
ssin
g d
elay
ed
dis
char
ges
Gra
ham
(2
012)
74U
KE
valu
ate
the
effe
ct o
f the
lap
aros
cop
ic
nurs
e sp
ecia
list
on p
atie
nt d
isch
arge
Qua
ntita
tive
Ret
rosp
ectiv
e co
mp
aris
on
Lap
aros
cop
ic c
hole
cyst
ecto
my
and
la
par
osco
pic
ingu
inal
her
nia
rep
air
pat
ient
s
128
►
Nur
se- l
ed d
isch
arge
may
incr
ease
d
isch
arge
pos
tlap
aros
cop
ic s
urge
ry
with
out
imp
actin
g p
atie
nt c
are
Gut
man
is
(201
6)65
Can
ada
Out
line
chan
ge s
trat
egie
s an
d t
heir
imp
act
heal
th s
yste
m t
rans
form
atio
n an
d t
hose
livi
ng w
ith r
esp
onsi
ve
beh
avio
urs
and
the
ir fa
mily
mem
ber
s
Mix
ed m
etho
ds
Qua
lity
imp
rove
men
tIn
div
idua
ls w
ith r
esp
onsi
ve
beh
avio
urs
NR
►
Imp
rove
d c
oord
inat
ion
and
co
mm
unic
atio
n ac
ross
sec
tors
►
Pro
vid
ed h
ealth
care
pro
vid
ers
with
le
arni
ng o
pp
ortu
nitie
s
Hen
woo
d
(200
6)48
UK
Exa
min
e th
e p
artn
ersh
ip b
etw
een
heal
th
and
soc
ial c
are
by
exp
lorin
g is
sues
with
ho
spita
l dis
char
ges
Cas
e st
udy
Cas
e st
udy
Inp
atie
nts
NR
►
Ad
dre
ssin
g an
d im
pro
ving
del
ayed
d
isch
arge
s re
qui
res
par
tner
ship
s b
etw
een
heal
th a
nd s
ocia
l car
e an
d
a w
hole
sys
tem
s- b
ased
ap
pro
ach
Hol
land
(2
016)
57U
SA
Rep
ort
the
dev
elop
men
t an
d e
valu
atio
n of
a d
isch
arge
del
ay t
rack
ing
and
re
por
ting
mec
hani
sm
Qua
ntita
tive
Pra
ctic
e im
pro
vem
ent
pro
ject
Inp
atie
nts
NR
►
Dis
char
ge d
elay
s ca
n b
e re
duc
ed
if sy
stem
and
pro
cess
bre
akd
owns
ar
e id
entifi
ed a
nd a
dd
ress
ed
Kat
salia
ki
(200
5)10
2U
KD
escr
ibe
a p
roje
ct in
vest
igat
ing
pot
entia
l car
e p
athw
ays
for
eld
erly
p
eop
le a
fter
dis
char
ge fr
om h
osp
ital
Qua
ntita
tive
Dis
cret
e- ev
ent
sim
ulat
ion,
sim
ulat
ion
mod
el
Inp
atie
nts
NR
►
Sim
ulat
ion
is a
sui
tab
le
met
hod
olog
y fo
r re
cord
ing
and
ev
alua
ting
the
new
pos
tacu
te
pac
kage
s
Lees
- Deu
tsch
(2
019)
66U
KId
entif
y co
re c
hara
cter
istic
s of
pat
ient
d
isch
arge
crit
eria
, rec
ord
ed in
clin
ical
m
anag
emen
t p
lans
or
case
not
es
Qua
ntita
tive
Sys
tem
atic
ob
serv
atio
nal
retr
osp
ectiv
e re
view
Pat
ient
s d
isch
arge
d fr
om t
he a
cute
m
edic
ine
unit
and
sho
rt- s
tay
units
50
►C
riter
ia- l
ed d
isch
arge
may
be
suita
ble
for
sele
ct p
atie
nts
in
imp
rovi
ng t
imel
ines
s of
dis
char
ge
Levi
n (2
019)
94S
cotla
ndE
xam
ine
the
imp
act
of In
term
edia
te
Car
e an
d t
he 7
2- ho
ur t
arge
t on
del
ayed
ho
spita
l dis
char
ge
Qua
ntita
tive
Con
trol
led
inte
rrup
ted
tim
e se
ries
des
ign
Pat
ient
s ag
ed 7
5+10
7 02
2
►Im
med
iate
imp
act
on d
ays
del
ayed
, but
incr
easi
ng r
ates
day
s d
elay
ed o
ver
time
sugg
ests
tha
t In
term
edia
te C
are
serv
ices
may
ne
ed t
o b
e ad
apte
d
Lian
(200
8)58
Sin
gap
ore
Dev
elop
met
hod
s to
red
uce
the
hosp
ital
leng
th o
f sta
y fo
r p
rem
atur
e in
fant
s b
y 30
%, w
ithin
6 m
onth
s
Qua
ntita
tive
Ret
rosp
ectiv
e re
view
Pre
mat
ure
infa
nts
78
►D
isch
arge
pla
nnin
g sh
ould
beg
in
on h
osp
ital a
dm
issi
on
►N
urse
s sh
ould
coa
ch p
aren
ts t
o p
rep
are
them
to
care
for
thei
r in
fant
at
hom
e
Mae
ssen
(2
008)
75N
ethe
rland
sA
sses
s th
e ef
fect
of e
nhan
ced
rec
over
y af
ter
surg
ery
pro
gram
me
on d
isch
arge
d
elay
s
Qua
ntita
tive
Ret
rosp
ectiv
e/
pro
spec
tive
stud
y
Pat
ient
s un
der
goin
g el
ectiv
e co
lore
ctal
res
ectio
n17
3
►A
dd
ition
al r
ecov
ery
stat
istic
s sh
ould
be
add
ed a
s ou
tcom
es o
f th
e E
RA
S p
rogr
amm
e
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
8 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Mah
ant
(200
8)59
Can
ada
Det
erm
ine
if an
aud
it- an
d- f
eed
bac
k in
terv
entio
n re
duc
es d
elay
ed d
isch
arge
in
a g
ener
al p
aed
iatr
ic in
pat
ient
uni
t
Qua
ntita
tive
Pro
spec
tive
obse
rvat
iona
l stu
dy
Pae
dia
tric
inp
atie
nt31
94
►R
educ
ed in
app
rop
riate
hos
pita
l d
ays,
with
out
imp
actin
g re
adm
issi
on r
ates
►
Iden
tified
pro
cess
es t
hat
imp
act
inap
pro
pria
te h
osp
ital d
ays
Mah
to (2
009)
76U
KD
eter
min
e th
e ef
fect
of a
dia
bet
es
outr
each
ser
vice
on
del
ayed
dis
char
ges
and
avo
idab
le a
dm
issi
ons
Qua
ntita
tive
Cro
ss- s
ectio
nal a
udit
Acu
tely
ad
mitt
ed p
atie
nts
with
d
iab
etes
137
►
The
rest
ruct
ured
hos
pita
l dia
bet
es
outr
each
ser
vice
imp
rove
d
outc
omes
for
inp
atie
nts
with
d
iab
etes
Mal
oney
(2
007)
49U
SA
Dev
elop
a w
eb- b
ased
sof
twar
e ap
plic
atio
n us
ed t
o fa
cilit
ate
timel
y p
atie
nt d
isch
arge
Qua
ntita
tive
Qua
lity
imp
rove
men
t p
ilot
pro
ject
Inp
atie
nts
NR
►
Hea
lthca
re in
form
atio
n te
chno
logy
ca
n fa
cilit
ate
bed
man
agem
ent
effic
ienc
ies
►
Imp
rove
d c
oord
inat
ion
and
ove
rall
inp
atie
nt fl
ow
Man
ville
(2
014)
95C
anad
aD
eter
min
e if
pro
vid
ing
inte
rdis
cip
linar
y ca
re o
n a
tran
sitio
nal c
are
unit
will
res
ult
in im
pro
ved
clin
ical
out
com
es a
nd lo
wer
co
sts
Qua
ntita
tive
Bef
ore-
and
- aft
er
stru
ctur
ed r
etro
spec
tive
char
t au
dit
Eld
erly
ALC
pat
ient
s (7
0+)
135
►
Imp
rove
d h
ealth
func
tiona
l ou
tcom
es, d
eliv
ered
at
a lo
wer
cos
t
Mee
han
(201
8)77
UK
Exp
lore
pat
ient
s’ e
xper
ienc
es o
f ho
spita
l dis
char
ge w
ith t
he d
isch
arge
to
asse
ss s
chem
e
Qua
litat
ive
Des
crip
tive
Pat
ient
s d
isch
arge
d t
hrou
gh
dis
char
ge t
o as
sess
30
►P
atie
nts
and
car
egiv
ers
rep
orte
d
pos
itive
and
neg
ativ
e ex
per
ienc
es
with
the
sch
eme,
but
it m
ay b
e b
enefi
cial
in im
pro
ving
out
com
es
for
som
e p
atie
nts
Moe
ller
(200
6)60
Can
ada
Ass
ess
pat
ient
and
phy
sici
an- r
elat
ed
bar
riers
to
dis
char
ging
pat
ient
s w
ho
have
met
ob
ject
ive
crite
ria
Mix
ed m
etho
ds
Ret
rosp
ectiv
e as
sess
men
t
Pat
ient
s w
ith c
omm
unity
- acq
uire
d
pne
umon
ia31
►
Pat
ient
s ou
tcom
es c
an b
e im
pro
ved
by
stan
dar
dis
ing
care
th
roug
h a
criti
cal p
athw
ay
►P
atie
nts
with
poo
r fu
nctio
nal
cap
acity
(usi
ng t
he H
iera
rchi
cal
Ass
essm
ent
of B
alan
ce a
nd
Mob
ility
) may
nee
d a
dd
ition
al
serv
ices
to
imp
rove
dis
char
ge t
ime
afte
r cl
inic
al s
tab
ility
Mur
- Vee
man
(2
011)
61Th
e N
ethe
rland
sE
xpla
in t
he t
heor
y of
buf
fer
man
agem
ent
and
dis
cuss
rel
ated
p
revi
ous
assu
mp
tions
NR
Rev
iew
/ th
eore
tical
p
aper
Bed
blo
cker
sN
R
►To
pra
ctic
ally
ap
ply
buf
fer
man
agem
ent,
cur
rent
rou
tines
, p
rinci
ple
s an
d b
elie
fs s
houl
d
shift
to
focu
s on
flow
bet
wee
n or
gani
satio
ns r
athe
r th
an w
ithin
one
or
gani
satio
n
Nie
mei
jer
(201
0)62
Net
herla
nds
Red
uce
the
aver
age
leng
th o
f sta
y to
cr
eate
mor
e ad
mis
sion
cap
acity
and
re
duc
e co
sts
Mix
ed m
etho
ds
Effi
cien
cy im
pro
vem
ent
pro
ject
(ret
rosp
ectiv
e an
d p
rosp
ectiv
e d
ata
colle
ctio
n)
Trau
ma
pat
ient
s20
06:1
114
2007
:112
4
►Le
an S
ix S
igm
a is
effe
ctiv
e in
re
duc
ing
leng
th o
f sta
y an
d
imp
rovi
ng fi
nanc
ial e
ffici
ency
in
trau
ma
care
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
9Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Pan
is (2
004)
78N
ethe
rland
sR
educ
e in
app
rop
riate
hos
pita
l sta
y b
y ad
just
ing
pat
ient
logi
stic
s, in
crea
sing
ef
ficie
ncy
and
pro
vid
ing
com
fort
able
su
rrou
ndin
gs
Qua
ntita
tive
Ret
rosp
ectiv
e co
hort
st
udy
Mot
hers
of n
ewb
orn
pat
ient
s28
89 d
ays
of h
osp
ital
stay
of
gyna
ecol
ogy
and
ob
stet
rics
pat
ient
s
►
Dis
char
ge c
riter
ia c
an r
educ
e in
app
rop
riate
pat
ient
sta
ys r
elat
ed
to d
isch
arge
pro
cess
es
►S
hift
ing
mat
erni
ty c
are
to
outp
atie
nt s
ettin
gs c
an r
educ
e ho
spita
l len
gth
of s
tay
Pat
el (2
019)
43U
SA
Eva
luat
e th
e im
pac
t of
tea
m- b
ased
m
ultid
isci
plin
ary
roun
ds
on d
isch
arge
p
lann
ing
and
car
e ef
ficie
ncy
Mix
ed m
etho
ds
Qua
lity
imp
rove
men
t in
itiat
ive
Dis
satis
fied
pat
ient
s w
ith d
elay
ed
dis
char
ge15
84
►M
ultid
isci
plin
ary
dis
char
ge r
ound
s ca
n im
pro
ve d
isch
arge
effi
cien
cy,
leng
th o
f sta
y an
d 3
0- d
ay
read
mis
sion
s
Ali
Pira
ni
(201
0)44
Pak
ista
nE
mp
hasi
se t
he r
ole
of n
urse
s to
d
eter
min
e fa
ctor
s le
adin
g to
a la
ck o
f d
isch
arge
pla
nnin
g
NR
Rev
iew
/ su
mm
ary
Thos
e ex
per
ienc
ing
del
ayed
d
isch
arge
NR
►
Nur
ses
pla
y a
key
role
in d
eliv
erin
g p
atie
nt- c
entr
ed c
are
and
can
im
pro
ve d
isch
arge
pla
nnin
g p
roce
sses
►
Nur
ses
mus
t ha
ve t
he a
pp
r op
riate
kn
owle
dge
ab
out
dis
char
ge
pla
nnin
g an
d h
ave
the
abili
ty t
o co
mm
unic
ate,
coo
rdin
ate
and
ed
ucat
e p
atie
nts
Qin
(201
7)10
3A
ustr
alia
Iden
tify
whi
ch b
arrie
rs t
o d
isch
arge
in
fluen
ce h
osp
ital o
ccup
ancy
whe
n ta
rget
ed b
y a
hosp
ital-
wid
e p
olic
y
Qua
ntita
tive
Sim
ulat
ion
mod
ellin
gN
RN
R
►H
osp
ital o
ccup
ancy
rat
es a
nd
over
crow
din
g ca
n b
e im
pro
ved
by
imp
rovi
ng d
isch
arge
pro
cess
es
Rae
(200
7)96
New
Zea
land
Illus
trat
e ho
w t
he D
elay
ed D
isch
arge
P
roje
ct s
olve
d a
bed
cris
is a
nd
cont
rolle
d e
xpen
ditu
re
Qua
ntita
tive
Con
tinuo
us q
ualit
y im
pro
vem
ent
pro
ject
Acu
te g
ener
al m
edic
al20
034
►
The
pro
ject
alte
red
sta
ff b
ehav
iour
ar
ound
pat
ient
dis
char
ge r
esul
ting
in a
bet
ter
use
of r
esou
rces
►
The
syst
em c
rash
ed 2
yea
rs p
ost-
im
ple
men
tatio
n
►Th
ere
is t
oo m
uch
focu
s on
leng
th
of s
tay
and
bed
allo
catio
ns le
adin
g to
poo
r d
ecis
ion
mak
ing
Rob
erts
(2
013)
50A
ustr
alia
Und
erta
ke a
pre
limin
ary
tria
l of t
he G
oal
Leng
th o
f Sta
y to
ol a
t a
reha
bili
tatio
n ce
ntre
Qua
ntita
tive
Pro
spec
tive
stud
yIn
pat
ient
s in
tw
o un
its: S
RU
or
BIR
U20
2
►Th
e p
rogr
amm
e d
id n
ot r
educ
e le
ngth
of s
tay
and
was
per
ceiv
ed
nega
tivel
y b
y st
aff
Sam
pso
n (2
006)
79U
KD
escr
ibe
bed
occ
upan
cy d
ata
in
peo
ple
with
dia
bet
es b
efor
e an
d a
fter
th
e in
trod
uctio
n of
a d
iab
etes
inp
atie
nt
spec
ialis
t nu
rse
serv
ice
Qua
ntita
tive
Ret
rosp
ectiv
e st
udy
Dia
bet
es in
pat
ient
s15
2 08
0
►D
iab
etes
inp
atie
nt s
pec
ialis
t nu
rse
red
uced
exc
ess
bed
occ
upan
cy
Sha
h (2
007)
97E
ngla
ndE
xam
ine
the
imp
act
of t
he C
omm
unity
C
are
(Del
ayed
Dis
char
ge) A
ct o
n b
ed o
ccup
ancy
and
leng
th o
f sta
y in
G
eria
tric
Med
icin
e (G
M) a
nd O
ld A
ge
Psy
chia
try
(OA
P) s
ervi
ces
Qua
ntita
tive
Ret
rosp
ectiv
e st
udy
Inp
atie
nt -
sp
ecia
lties
of G
M a
nd
OA
P s
ervi
ces
NR
►
Mor
e p
atie
nts
wer
e ad
mitt
ed t
o G
M
serv
ices
and
had
a s
hort
er le
ngth
of
sta
y th
an O
AP
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

10 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Sob
otka
(2
017)
51U
SA
Des
crib
e a
hosp
ital-
to- h
ome
tran
sitio
nal
care
mod
elC
ase
stud
yIll
ustr
ativ
e ca
se d
esig
n/
revi
ew
Pae
dia
tric
inp
atie
nt1
►
Tran
sitio
nal c
are
pro
gram
mes
ca
n im
pro
ve c
are
for
vuln
erab
le
pop
ulat
ions
by
red
ucin
g he
alth
and
d
evel
opm
enta
l diff
eren
ces
Sta
rr-
Hem
bur
row
(2
011)
80
Can
ada
Min
imis
e th
e nu
mb
er o
f pos
t- ac
ute
pat
ient
s tr
ansi
tioni
ng fr
om h
osp
ital
to lo
ng- t
erm
car
e an
d d
evel
op a
n in
tegr
ated
pla
n fo
r ap
pro
pria
te c
are
and
p
lace
men
t
Qua
ntita
tive
Qua
lity
imp
rove
men
tA
LC p
atie
nts
NR
►
Inte
r an
d in
tra-
pro
fess
iona
l co
llab
orat
ion
is im
por
tant
to
stan
dar
dis
e d
isch
arge
pro
cess
es,
bui
ld t
rust
and
res
pec
t an
d im
pro
ve
coor
din
atio
n of
car
e
Sut
herla
nd
(201
3)45
Can
ada
Des
crib
e st
ruct
ural
cha
lleng
es t
o re
duc
e th
e im
pac
t of
ALC
pat
ient
s an
d
to p
rop
ose
pol
icy
alte
rnat
ives
tha
t co
uld
re
duc
e oc
cup
ancy
NR
Dis
cuss
ion
and
deb
ate
artic
le
ALC
pat
ient
sN
R
►A
col
lab
orat
ive
app
roac
h co
mb
inin
g th
e th
ree
stra
tegi
es
shou
ld b
e co
nsid
ered
to
add
ress
A
LC
Tab
er (2
013)
81U
SA
Test
a p
rogr
amm
e to
imp
rove
leng
th
of s
tay,
del
ayed
dis
char
ges
and
ear
ly
read
mis
sion
s fo
r ki
dne
y tr
ansp
lant
re
cip
ient
s
Qua
ntita
tive
Ob
serv
atio
nal s
tud
yA
dul
t ki
dne
y tr
ansp
lant
rec
ipie
nts
476
►
Imp
rovi
ng m
edic
atio
n sa
fety
pos
t ki
dne
y tr
ansp
lant
can
imp
rove
cl
inic
al o
utco
mes
(acu
te r
ejec
tion
and
infe
ctio
n ra
tes,
rea
dm
issi
on
rate
s)
Ud
ayai
(201
2)82
Ind
iaR
educ
e p
atie
nt d
isch
arge
tim
e th
roug
h a
Six
Sig
ma
pro
ject
Qua
ntita
tive
Tim
e m
otio
n st
udy
Cas
h p
atie
nts
NR
►
Imp
rovi
ng d
isch
arge
tim
e al
low
ed
for
mor
e p
atie
nts
to b
e m
anag
ed,
imp
rovi
ng r
even
ue
►Le
ader
ship
sup
por
t an
d e
mp
loye
e p
artic
ipat
ion
wer
e es
sent
ial f
or
succ
ess
Will
iam
s (2
010)
52A
ustr
alia
Exa
min
e th
e im
pac
t of
a c
ritic
al c
are
outr
each
ser
vice
on
freq
uenc
y of
d
isch
arge
del
ay fr
om t
he in
tens
ive
care
un
it
Qua
ntita
tive
Pro
spec
tive
coho
rt
stud
y
Pat
ient
s d
isch
arge
d fr
om t
he IC
U11
23
►Th
e cr
itica
l car
e ou
trea
ch r
ole
did
no
t d
ecre
ase
del
ayed
dis
char
ges
►
Red
ucin
g d
elay
s r e
qui
res
a co
llab
orat
ive
app
roac
h fo
cusi
ng o
n ho
spita
l flow
, rat
her
than
just
the
d
isch
arge
pro
cess
Youn
is (2
011)
53U
KC
omp
are
the
effe
ct o
f an
enha
nced
re
cove
ry p
rogr
amm
e w
ith p
reop
erat
ive
stom
a ed
ucat
ion
on t
he n
umb
er o
f p
atie
nts
with
pro
long
ed h
osp
ital s
tay
Qua
ntita
tive
Pro
spec
tive
stud
yP
atie
nts
und
ergo
ing
ante
rior
rese
ctio
n w
ith t
he fo
rmat
ion
of a
lo
op il
eost
omy
120
►
Pre
- op
erat
ivel
y in
tegr
atin
g st
oma
man
agem
ent
educ
atio
n in
to a
n en
hanc
ed r
ecov
ery
pro
gram
me
can
red
uce
del
ayed
dis
char
ges
Gre
y lit
erat
ure
Ano
nym
ous
(200
8)99
US
AC
reat
e an
exp
edite
d d
isch
arge
fund
to
pay
for
good
s an
d s
ervi
ces
inhi
biti
ng a
p
atie
nt’s
dis
char
ge (m
edic
al e
qui
pm
ent,
m
edic
atio
n an
d t
rans
por
tatio
n)
N/A
New
s ar
ticle
Uni
nsur
ed p
atie
nts
NR
►
Pat
ient
s ca
n b
e sa
fely
dis
char
ged
th
roug
h su
pp
ort
from
the
dis
char
ge
fund
Ano
nym
ous
(201
0)46
US
AIm
pro
ve p
atie
nt fl
ow t
hrou
gh in
itiat
ives
th
at d
ecre
ase
leng
th o
f sta
y an
d
incr
ease
cap
acity
N/A
New
s ar
ticle
NR
NR
►
NR
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
11Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Cal
vele
y (2
007)
83U
KC
reat
e a
tier
of s
upp
ort
to r
educ
e th
e un
nece
ssar
y an
d c
ostly
occ
upat
ion
of
hosp
ital b
eds
N/A
Rev
iew
NR
NR
►
Hea
lthca
re s
olut
ions
sho
uld
be
dev
elop
ed in
par
tner
ship
with
he
alth
and
com
mun
ity s
ervi
ce
pro
vid
ers
Man
zano
- S
anta
ella
(2
009)
100
UK
Ana
lyse
the
rel
atio
nshi
p b
etw
een
Pay
men
t b
y R
esul
ts a
nd t
he D
elay
ed
Dis
char
ges
Act
N/A
Pol
icy
anal
ysis
NR
NR
►
Qua
ntita
tive
mea
sure
s (d
ays
del
ayed
and
cos
ts) c
onfli
ct w
ith t
he
soci
al a
spec
ts o
f ove
rall
heal
th a
nd
wel
l- b
eing
Kry
stal
(201
9)86
Can
ada
NR
Mix
ed m
etho
ds
Con
tinuo
us q
ualit
y im
pro
vem
ent
and
ev
alua
tion
Med
ical
ly a
nd s
ocia
lly c
omp
lex
and
fr
ail e
lder
ly10
0+
►E
ngag
ing
par
tner
s ea
rly in
the
co
ncep
tion
of t
he p
rogr
amm
e w
as
criti
cal t
o its
suc
cess
Wal
ker
(201
1)2
Can
ada
Dev
elop
rec
omm
end
atio
ns o
f car
e fo
r fr
ail C
anad
ians
N/A
N/A
NR
NR
►
Com
mun
ity s
upp
orts
sho
uld
be
incr
ease
d t
o ke
ep p
eop
le in
the
ir ho
me
as lo
ng a
s p
ossi
ble
►
Pro
gram
mes
and
ser
vice
s sh
ould
b
e ai
med
at
rest
orat
ion
and
re
activ
atio
n
Nor
th W
est
Com
mun
ity
Car
e A
cces
s C
entr
e (2
011)
88
Can
ada
Cre
ate
a fa
ct s
heet
of t
he b
enefi
ts o
f st
ayin
g at
hom
e an
d u
sing
Wai
t at
H
ome
(enh
ance
d h
ome
care
ser
vice
s w
hile
peo
ple
wai
t fo
r lo
ng- t
erm
car
e)
N/A
N/A
Sen
iors
wai
ting
for
LTC
pla
cem
ent
NR
►
Sta
ying
hom
e p
rovi
des
ben
efits
fo
r se
nior
s in
clud
ing
few
er r
isks
(g
erm
s/ v
iruse
s) a
nd a
fam
iliar
se
ttin
g co
mp
ared
with
the
hos
pita
l
Toro
nto
Cen
tral
C
omm
unity
C
are
Acc
ess
Cen
tre
(201
5)67
Can
ada
NR
N/A
N/A
NR
NR
►
This
fram
ewor
k ca
n he
lp im
pro
ve
resu
lts a
roun
d A
LC a
void
ance
and
m
anag
emen
t
Pro
vinc
e of
N
ew B
runs
wic
k (2
017)
92
Can
ada
Iden
tify
prio
rity
stra
tegi
c in
itiat
ives
and
im
ple
men
t co
mm
unity
sup
por
t or
der
s ac
ross
the
pro
vinc
e
N/A
Ann
ual r
epor
tN
RN
R
►N
R
NH
S
Imp
rove
men
t (2
018)
104
UK
Cre
ate
a ho
w- t
o gu
ide
exp
lain
ing
imp
lem
enta
tion
app
roac
hes
to r
educ
e le
ngth
of s
tay
N/A
Gui
de
NR
NR
►
Clin
ical
lead
ersh
ip is
ess
entia
l for
im
ple
men
ting
thes
e in
itiat
ives
Sta
rr-
Hem
bur
row
(2
010)
91
Can
ada
Imp
rove
pat
ient
flow
thr
ough
the
im
ple
men
tatio
n of
cha
nge
man
agem
ent
initi
ativ
es
Qua
ntita
tive
Qua
lity
imp
rove
men
tN
RN
R
►C
ultu
re c
hang
e re
qui
res
sup
por
t an
d a
tten
tion
to b
e su
stai
ned
ove
r tim
e
LHIN
C
olla
bor
ativ
e (2
011)
87
Can
ada
Hel
p s
upp
ort
pat
ient
s in
the
ir ho
mes
for
as lo
ng a
s p
ossi
ble
by
pro
vid
ing
them
w
ith c
omm
unity
sup
por
ts
N/A
Imp
lem
enta
tion
guid
e an
d t
oolk
it
Pat
ient
s (s
pec
ifica
lly h
igh
need
s se
nior
s)N
R
►H
ome
Firs
t sh
ould
be
imp
lem
ente
d
as a
sys
tem
- wid
e ap
pro
ach
Tab
le 2
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
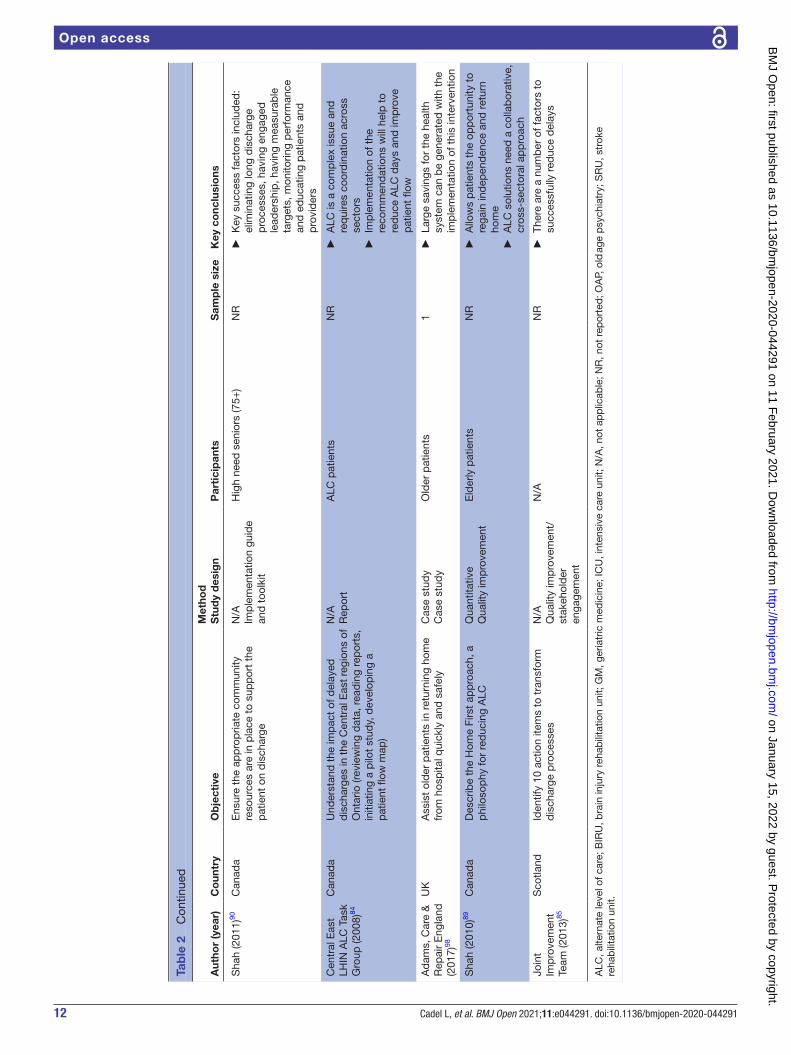
12 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
(yea
r)C
oun
try
Ob
ject
ive
Met
hod
Stu
dy
des
ign
Par
tici
pan
tsS
amp
le s
ize
Key
co
nclu
sio
ns
Sha
h (2
011)
90C
anad
aE
nsur
e th
e ap
pro
pria
te c
omm
unity
re
sour
ces
are
in p
lace
to
sup
por
t th
e p
atie
nt o
n d
isch
arge
N/A
Imp
lem
enta
tion
guid
e an
d t
oolk
it
Hig
h ne
ed s
enio
rs (7
5+)
NR
►
Key
suc
cess
fact
ors
incl
uded
: el
imin
atin
g lo
ng d
isch
arge
p
roce
sses
, hav
ing
enga
ged
le
ader
ship
, hav
ing
mea
sura
ble
ta
rget
s, m
onito
ring
per
form
ance
an
d e
duc
atin
g p
atie
nts
and
p
rovi
der
s
Cen
tral
Eas
t LH
IN A
LC T
ask
Gro
up (2
008)
84
Can
ada
Und
erst
and
the
imp
act
of d
elay
ed
dis
char
ges
in t
he C
entr
al E
ast
regi
ons
of
Ont
ario
(rev
iew
ing
dat
a, r
ead
ing
rep
orts
, in
itiat
ing
a p
ilot
stud
y, d
evel
opin
g a
pat
ient
flow
map
)
N/A
Rep
ort
ALC
pat
ient
sN
R
►A
LC is
a c
omp
lex
issu
e an
d
req
uire
s co
ord
inat
ion
acro
ss
sect
ors
►
Imp
lem
enta
tion
of t
he
reco
mm
end
atio
ns w
ill h
elp
to
red
uce
ALC
day
s an
d im
pro
ve
pat
ient
flow
Ad
ams,
Car
e &
R
epai
r E
ngla
nd
(201
7)98
UK
Ass
ist
old
er p
atie
nts
in r
etur
ning
hom
e fr
om h
osp
ital q
uick
ly a
nd s
afel
yC
ase
stud
yC
ase
stud
yO
lder
pat
ient
s1
►
Larg
e sa
ving
s fo
r th
e he
alth
sy
stem
can
be
gene
rate
d w
ith t
he
imp
lem
enta
tion
of t
his
inte
rven
tion
Sha
h (2
010)
89C
anad
aD
escr
ibe
the
Hom
e Fi
rst
app
roac
h, a
p
hilo
sop
hy fo
r re
duc
ing
ALC
Qua
ntita
tive
Qua
lity
imp
rove
men
tE
lder
ly p
atie
nts
NR
►
Allo
ws
pat
ient
s th
e op
por
tuni
ty t
o re
gain
ind
epen
den
ce a
nd r
etur
n ho
me
►
ALC
sol
utio
ns n
eed
a c
olla
bor
ativ
e,
cros
s- se
ctor
al a
pp
roac
h
Join
t Im
pro
vem
ent
Team
(201
3)85
Sco
tland
Iden
tify
10 a
ctio
n ite
ms
to t
rans
form
d
isch
arge
pro
cess
esN
/AQ
ualit
y im
pro
vem
ent/
st
akeh
old
er
enga
gem
ent
N/A
NR
►
Ther
e ar
e a
num
ber
of f
acto
rs t
o su
cces
sful
ly r
educ
e d
elay
s
ALC
, alte
rnat
e le
vel o
f car
e; B
IRU
, bra
in in
jury
reh
abili
tatio
n un
it; G
M, g
eria
tric
med
icin
e; IC
U, i
nten
sive
car
e un
it; N
/A, n
ot a
pp
licab
le; N
R, n
ot r
epor
ted
; OA
P, o
ld a
ge p
sych
iatr
y; S
RU
, str
oke
reha
bili
tatio
n un
it.
Tab
le 2
C
ontin
ued
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

13Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Tab
le 3
In
itiat
ive
char
acte
ristic
s
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Dat
abas
e S
earc
hes
Ad
lingt
on40
Qua
lity
imp
rove
men
t p
rogr
amm
e
►W
eekl
y q
ualit
y im
pro
vem
ent
mee
tings
with
d
river
dia
gram
s to
imp
lem
ent
Pla
n D
o S
tud
y A
ct c
ycle
s
Old
er a
dul
ts (>
65) o
n p
sych
iatr
ic w
ard
Hos
pita
lM
ile E
nd H
osp
ital
(Lea
den
hall
War
d),
26 b
eds
Info
rmat
ion
shar
ing
live
►
Leng
th o
f sta
y w
as r
educ
ed fr
om a
n av
erag
e of
47
day
s to
30
day
s
►B
ed o
ccup
ancy
was
red
uced
from
77%
to
54%
Ard
agh63
10 p
rom
isin
g in
itiat
ives
►
Sp
ecia
l bed
s, h
osp
ital o
per
atio
ns p
lann
ing,
d
isch
arge
pla
nnin
g, a
cces
s to
imag
ing,
re
spon
sive
acu
te s
econ
dar
y se
rvic
es,
pat
hway
s fo
r ac
ute
pat
ient
s, a
cute
dem
and
m
itiga
tion,
enh
ance
d E
D la
yout
, enh
ance
d E
D
seni
or s
taffi
ng, e
ngag
emen
t of
sta
ff
NR
Hos
pita
lsTo
ols
and
gu
idel
ines
Pra
ctic
e ch
ange
s
►
Iden
tified
top
10
chal
leng
es a
nd 1
0 p
rom
isin
g in
itiat
ives
rel
ated
to
pat
ient
flow
and
em
erge
ncy
dep
artm
ent
over
crow
din
g
Are
ndts
68A
llied
hea
lth a
sses
smen
t
►A
com
pr e
hens
ive
asse
ssm
ent
of p
atie
nts
by
an a
llied
hea
lth t
eam
with
in h
ours
of
pre
sent
atio
n to
the
hos
pita
l thr
ough
the
em
erge
ncy
dep
artm
ent
Pat
ient
s (>
65)
dia
gnos
ed w
ith
one
or m
ore
of
six
pre
det
erm
ined
co
nditi
ons
Hos
pita
lsTw
o A
ustr
alia
n te
rtia
ry
hosp
itals
Pra
ctic
e ch
ange
s
►N
o b
enefi
t in
red
ucin
g ho
spita
l len
gth
of s
tay
Bau
man
n55N
/A ►
Qua
litat
ive
stud
y to
iden
tify
fact
ors
asso
ciat
ed
with
low
rat
es o
f del
ayed
dis
char
ges
Hea
lth/
soci
al
serv
ices
sta
ff w
ith m
anag
eria
l in
volv
emen
t in
d
isch
arge
s
Hos
pita
ls (6
site
s)4
sout
hern
site
s, 2
nor
ther
n si
tes
Initi
ativ
es
des
crib
ed t
ouch
on
all
cate
gorie
s
►
6 hi
gh- p
erfo
rmin
g ho
spita
l site
s id
entifi
ed
issu
es im
pac
ting
del
ayed
dis
char
ges
(cap
acity
, int
erna
l hos
pita
l effi
cien
cies
and
in
tera
genc
y ef
ficie
ncie
s)
►R
esou
rces
and
tea
ms
to p
reve
nt a
void
able
ad
mis
sion
s
►D
isch
arge
tea
ms
to s
upp
ort
nurs
es'
dis
char
ge p
lann
ing,
►
Sys
tem
s fo
r m
onito
ring
and
com
mun
icat
ing
pat
ient
s' p
rogr
ess,
►
Pat
ient
cho
ice
pro
toco
ls
►E
nsur
e av
aila
bili
ty o
f res
pon
sive
tr
ansp
orta
tion
and
dis
char
ge lo
unge
s
Beh
an93
Com
mun
ity C
are
(Del
ayed
Dis
char
ge) A
ct 2
003
►
Loca
l aut
horit
ies
are
finan
cial
ly r
esp
onsi
ble
(p
aym
ents
) to
acut
e ho
spita
l whe
n p
atie
nts
rem
ain
in h
osp
ital b
ecau
se c
omm
unity
car
e ar
rang
emen
ts h
ave
not
bee
n m
ade
NR
7 ar
eas
acro
ss t
he U
KIn
fras
truc
ture
and
fin
ance
►
Nat
iona
l dec
reas
e in
del
ayed
dis
char
ges
bet
wee
n 20
03 a
nd 2
004
Bél
and
69In
tegr
ated
car
e
►C
omm
unity
- bas
ed m
ultid
isci
plin
ary
team
s w
ho
pr o
vid
e in
tegr
ated
car
e an
d c
oord
inat
e he
alth
an
d s
ocia
l ser
vice
Frai
l eld
erly
Com
mun
ity s
ervi
ce c
entr
es/
orga
nisa
tions
Pra
ctic
e ch
ange
s
►S
igni
fican
t (5
0%) r
educ
tion
in t
he n
umb
er
of p
atie
nts
in t
he in
tegr
ated
car
e gr
oup
tha
t b
ecam
e A
LC
►N
o si
gnifi
cant
diff
eren
ces
in u
tilis
atio
n or
co
sts
bet
wee
n gr
oup
s
►In
crea
sed
car
egiv
er s
atis
fact
ion
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
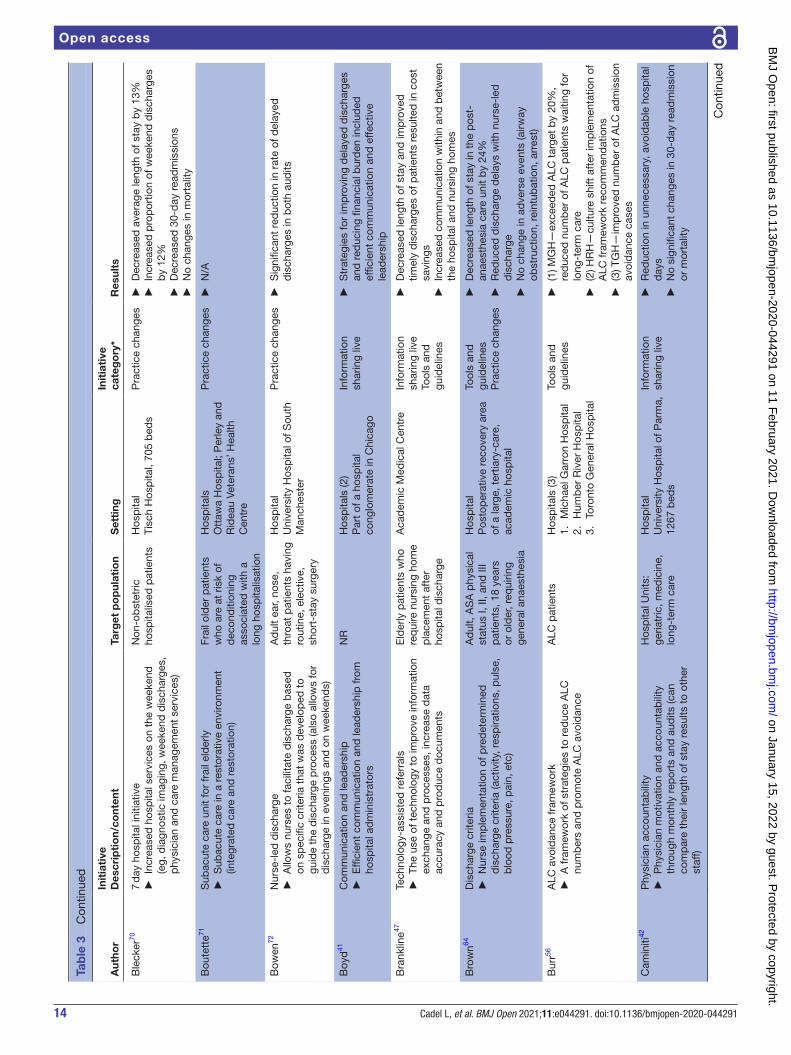
14 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Ble
cker
707
day
hos
pita
l ini
tiativ
e
►In
crea
sed
hos
pita
l ser
vice
s on
the
wee
kend
(e
g, d
iagn
ostic
imag
ing,
wee
kend
dis
char
ges,
p
hysi
cian
and
car
e m
anag
emen
t se
rvic
es)
Non
- ob
stet
ric
hosp
italis
ed p
atie
nts
Hos
pita
lTi
sch
Hos
pita
l, 70
5 b
eds
Pra
ctic
e ch
ange
s
►D
ecre
ased
ave
rage
leng
th o
f sta
y b
y 13
%
►In
crea
sed
pro
por
tion
of w
eeke
nd d
isch
arge
s b
y 12
%
►D
ecre
ased
30-
day
rea
dm
issi
ons
►
No
chan
ges
in m
orta
lity
Bou
tett
e71S
ubac
ute
care
uni
t fo
r fr
ail e
lder
ly
►S
ubac
ute
car e
in a
res
tora
tive
envi
ronm
ent
(inte
grat
ed c
are
and
res
tora
tion)
Frai
l old
er p
atie
nts
who
are
at
risk
of
dec
ond
ition
ing
asso
ciat
ed w
ith a
lo
ng h
osp
italis
atio
n
Hos
pita
lsO
ttaw
a H
osp
ital;
Per
ley
and
R
idea
u Ve
tera
ns’ H
ealth
C
entr
e
Pra
ctic
e ch
ange
s
►N
/A
Bow
en72
Nur
se- l
ed d
isch
arge
►
Allo
ws
nurs
es t
o fa
cilit
ate
dis
char
ge b
ased
on
sp
ecifi
c cr
iteria
tha
t w
as d
evel
oped
to
guid
e th
e d
isch
arge
pro
cess
(als
o al
low
s fo
r d
isch
arge
in e
veni
ngs
and
on
wee
kend
s)
Ad
ult
ear,
nose
, th
roat
pat
ient
s ha
ving
ro
utin
e, e
lect
ive,
sh
ort-
stay
sur
gery
Hos
pita
lU
nive
rsity
Hos
pita
l of S
outh
M
anch
este
r
Pra
ctic
e ch
ange
s
►S
igni
fican
t re
duc
tion
in r
ate
of d
elay
ed
dis
char
ges
in b
oth
aud
its
Boy
d41
Com
mun
icat
ion
and
lead
ersh
ip
►E
ffici
ent
com
mun
icat
ion
and
lead
ersh
ip fr
om
hosp
ital a
dm
inis
trat
ors
NR
Hos
pita
ls (2
)P
art
of a
hos
pita
l co
nglo
mer
ate
in C
hica
go
Info
rmat
ion
shar
ing
live
►
Str
ateg
ies
for
imp
rovi
ng d
elay
ed d
isch
arge
s an
d r
educ
ing
finan
cial
bur
den
incl
uded
ef
ficie
nt c
omm
unic
atio
n an
d e
ffect
ive
lead
ersh
ip
Bra
nklin
e47Te
chno
logy
- ass
iste
d r
efer
rals
►
The
use
of t
echn
olog
y to
imp
r ove
info
rmat
ion
exch
ange
and
pro
cess
es, i
ncre
ase
dat
a ac
cura
cy a
nd p
rod
uce
doc
umen
ts
Eld
erly
pat
ient
s w
ho
req
uire
nur
sing
hom
e p
lace
men
t af
ter
hosp
ital d
isch
arge
Aca
dem
ic M
edic
al C
entr
eIn
form
atio
n sh
arin
g liv
eTo
ols
and
gu
idel
ines
►
Dec
reas
ed le
ngth
of s
tay
and
imp
rove
d
timel
y d
isch
arge
s of
pat
ient
s re
sulte
d in
cos
t sa
ving
s
►In
crea
sed
com
mun
icat
ion
with
in a
nd b
etw
een
the
hosp
ital a
nd n
ursi
ng h
omes
Bro
wn64
Dis
char
ge c
riter
ia
►N
urse
imp
lem
enta
tion
of p
red
eter
min
ed
dis
char
ge c
riter
ia (a
ctiv
ity, r
esp
iratio
ns, p
ulse
, b
lood
pre
ssur
e, p
ain,
etc
)
Ad
ult,
AS
A p
hysi
cal
stat
us I,
II, a
nd II
I p
atie
nts,
18
year
s or
old
er, r
equi
ring
gene
ral a
naes
thes
ia
Hos
pita
lP
osto
per
ativ
e re
cove
ry a
rea
of a
larg
e, t
ertia
ry- c
are,
ac
adem
ic h
osp
ital
Tool
s an
d
guid
elin
esP
ract
ice
chan
ges
►
Dec
reas
ed le
ngth
of s
tay
in t
he p
ost-
an
aest
hesi
a ca
re u
nit
by
24%
►
Red
uced
dis
char
ge d
elay
s w
ith n
urse
- led
d
isch
arge
►
No
chan
ge in
ad
vers
e ev
ents
(airw
ay
obst
ruct
ion,
rei
ntub
atio
n, a
rres
t)
Bur
r56A
LC a
void
ance
fram
ewor
k
►A
fram
ewor
k of
str
ateg
ies
to r
educ
e A
LC
num
ber
s an
d p
rom
ote
ALC
avo
idan
ce
ALC
pat
ient
sH
osp
itals
(3)
1.
Mic
hael
Gar
ron
Hos
pita
l2.
H
umb
er R
iver
Hos
pita
l3.
To
ront
o G
ener
al H
osp
ital
Tool
s an
d
guid
elin
es
►(1
) MG
H—
exce
eded
ALC
tar
get
by
20%
, re
duc
ed n
umb
er o
f ALC
pat
ient
s w
aitin
g fo
r lo
ng- t
erm
car
e
►(2
) HR
H—
cultu
re s
hift
aft
er im
ple
men
tatio
n of
A
LC fr
amew
ork
reco
mm
end
atio
ns
►(3
) TG
H—
imp
rove
d n
umb
er o
f ALC
ad
mis
sion
av
oid
ance
cas
es
Cam
initi
42P
hysi
cian
acc
ount
abili
ty
►P
hysi
cian
mot
ivat
ion
and
acc
ount
abili
ty
thr o
ugh
mon
thly
rep
orts
and
aud
its (c
an
com
par
e th
eir
leng
th o
f sta
y re
sults
to
othe
r st
aff)
Hos
pita
l Uni
ts:
geria
tric
, med
icin
e,
long
- ter
m c
are
Hos
pita
lU
nive
rsity
Hos
pita
l of P
arm
a,
1267
bed
s
Info
rmat
ion
shar
ing
live
►
Red
uctio
n in
unn
eces
sary
, avo
idab
le h
osp
ital
day
s
►N
o si
gnifi
cant
cha
nges
in 3
0- d
ay r
ead
mis
sion
or
mor
talit
y
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
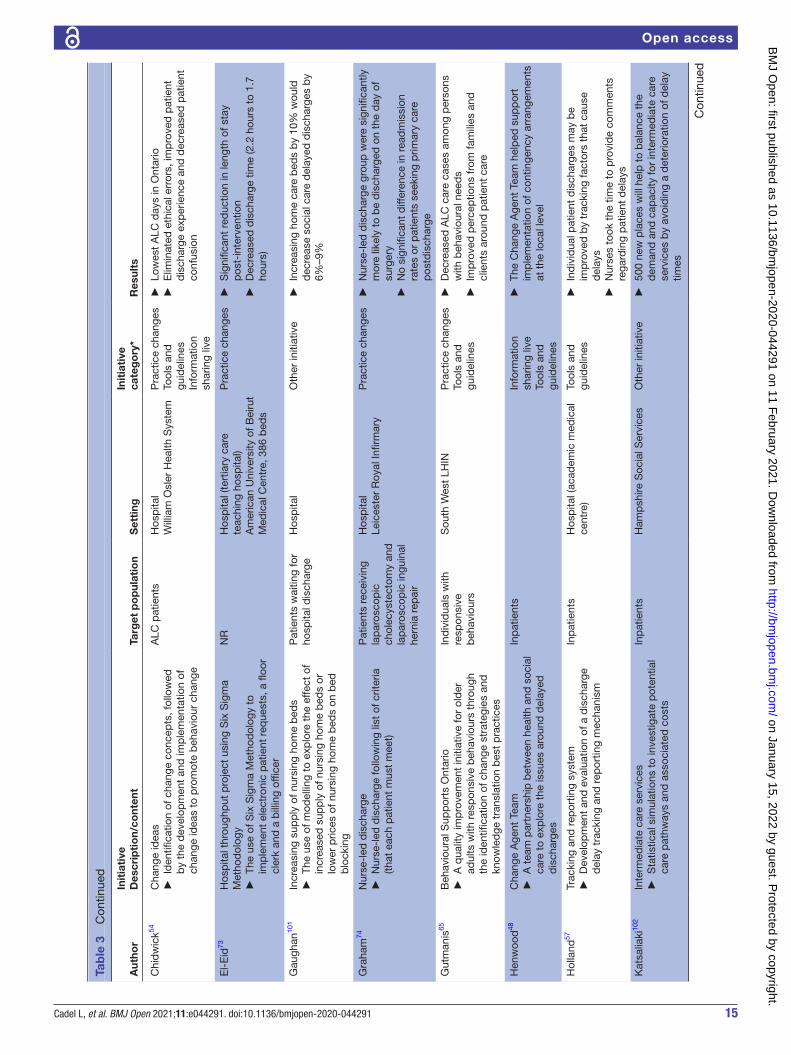
15Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Chi
dw
ick54
Cha
nge
idea
s
►Id
entifi
catio
n of
cha
nge
conc
epts
, fol
low
ed
by
the
dev
elop
men
t an
d im
ple
men
tatio
n of
ch
ange
idea
s to
pro
mot
e b
ehav
iour
cha
nge
ALC
pat
ient
sH
osp
ital
Will
iam
Osl
er H
ealth
Sys
tem
Pra
ctic
e ch
ange
sTo
ols
and
gu
idel
ines
Info
rmat
ion
shar
ing
live
►
Low
est
ALC
day
s in
Ont
ario
►
Elim
inat
ed e
thic
al e
rror
s, im
pro
ved
pat
ient
d
isch
arge
exp
erie
nce
and
dec
reas
ed p
atie
nt
conf
usio
n
El-
Eid
73H
osp
ital t
hrou
ghp
ut p
roje
ct u
sing
Six
Sig
ma
Met
hod
olog
y
►Th
e us
e of
Six
Sig
ma
Met
hod
olog
y to
im
ple
men
t el
ectr
onic
pat
ient
req
uest
s, a
floo
r cl
erk
and
a b
illin
g of
ficer
NR
Hos
pita
l (te
rtia
ry c
are
teac
hing
hos
pita
l)A
mer
ican
Uni
vers
ity o
f Bei
rut
Med
ical
Cen
tre,
386
bed
s
Pra
ctic
e ch
ange
s
►S
igni
fican
t re
duc
tion
in le
ngth
of s
tay
pos
t- in
terv
entio
n
►D
ecre
ased
dis
char
ge t
ime
(2.2
hou
rs t
o 1.
7 ho
urs)
Gau
ghan
101
Incr
easi
ng s
upp
ly o
f nur
sing
hom
e b
eds
►
The
use
of m
odel
ling
to e
xplo
re t
he e
ffect
of
incr
ease
d s
upp
ly o
f nur
sing
hom
e b
eds
or
low
er p
rices
of n
ursi
ng h
ome
bed
s on
bed
b
lock
ing
Pat
ient
s w
aitin
g fo
r ho
spita
l dis
char
geH
osp
ital
Oth
er in
itiat
ive
►
Incr
easi
ng h
ome
care
bed
s b
y 10
% w
ould
d
ecre
ase
soci
al c
are
del
ayed
dis
char
ges
by
6%–9
%
Gra
ham
74N
urse
- led
dis
char
ge
►N
urse
- led
dis
char
ge fo
llow
ing
list
of c
riter
ia
(that
eac
h p
atie
nt m
ust
mee
t)
Pat
ient
s re
ceiv
ing
lap
aros
cop
ic
chol
ecys
tect
omy
and
la
par
osco
pic
ingu
inal
he
rnia
rep
air
Hos
pita
lLe
ices
ter
Roy
al In
firm
ary
Pra
ctic
e ch
ange
s
►N
urse
- led
dis
char
ge g
roup
wer
e si
gnifi
cant
ly
mor
e lik
ely
to b
e d
isch
arge
d o
n th
e d
ay o
f su
rger
y
►N
o si
gnifi
cant
diff
eren
ce in
rea
dm
issi
on
rate
s or
pat
ient
s se
ekin
g p
rimar
y ca
re
pos
tdis
char
ge
Gut
man
is65
Beh
avio
ural
Sup
por
ts O
ntar
io
►A
qua
lity
imp
rove
men
t in
itiat
ive
for
old
er
adul
ts w
ith r
esp
onsi
ve b
ehav
iour
s th
roug
h th
e id
entifi
catio
n of
cha
nge
stra
tegi
es a
nd
know
led
ge t
rans
latio
n b
est
pra
ctic
es
Ind
ivid
uals
with
re
spon
sive
b
ehav
iour
s
Sou
th W
est
LHIN
Pra
ctic
e ch
ange
sTo
ols
and
gu
idel
ines
►
Dec
reas
ed A
LC c
are
case
s am
ong
per
sons
w
ith b
ehav
iour
al n
eed
s
►Im
pro
ved
per
cep
tions
from
fam
ilies
and
cl
ient
s ar
ound
pat
ient
car
e
Hen
woo
d48
Cha
nge
Age
nt T
eam
►
A t
eam
par
tner
ship
bet
wee
n he
alth
and
soc
ial
care
to
exp
lore
the
issu
es a
roun
d d
elay
ed
dis
char
ges
Inp
atie
nts
Info
rmat
ion
shar
ing
live
Tool
s an
d
guid
elin
es
►
The
Cha
nge
Age
nt T
eam
hel
ped
sup
por
t im
ple
men
tatio
n of
con
tinge
ncy
arra
ngem
ents
at
the
loca
l lev
el
Hol
land
57Tr
acki
ng a
nd r
epor
ting
syst
em
►D
evel
opm
ent
and
eva
luat
ion
of a
dis
char
ge
del
ay t
rack
ing
and
rep
ortin
g m
echa
nism
Inp
atie
nts
Hos
pita
l (ac
adem
ic m
edic
al
cent
re)
Tool
s an
d
guid
elin
es
►In
div
idua
l pat
ient
dis
char
ges
may
be
imp
rove
d b
y tr
acki
ng fa
ctor
s th
at c
ause
d
elay
s
►N
urse
s to
ok t
he t
ime
to p
rovi
de
com
men
ts
rega
rdin
g p
atie
nt d
elay
s
Kat
salia
ki10
2In
term
edia
te c
are
serv
ices
►
Sta
tistic
al s
imul
atio
ns t
o in
vest
igat
e p
oten
tial
care
pat
hway
s an
d a
ssoc
iate
d c
osts
Inp
atie
nts
Ham
psh
ire S
ocia
l Ser
vice
sO
ther
initi
ativ
e
►50
0 ne
w p
lace
s w
ill h
elp
to
bal
ance
the
d
eman
d a
nd c
apac
ity fo
r in
term
edia
te c
are
serv
ices
by
avoi
din
g a
det
erio
ratio
n of
del
ay
times
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

16 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Lees
- Deu
tsch
66C
riter
ia le
d d
isch
arge
- S
elec
tion
of P
atie
nts
for
Effi
cien
t an
d E
ffect
ive
Dis
char
ge
►P
atie
nt d
isch
arge
is g
uid
ed b
y a
set
of c
linic
al
crite
ria; o
nce
the
pat
ient
mee
ts t
he c
riter
ia, a
m
emb
er o
f the
tea
m c
an fa
cilit
ate
dis
char
ge
Pat
ient
s d
isch
arge
d
from
the
AM
U a
nd
bot
h sh
ort-
stay
war
ds
Hos
pita
l (ac
ute
med
icin
e se
rvic
e w
ith fo
ur c
linic
al
area
s)
Tool
s an
d
guid
elin
esP
ract
ice
chan
ges
►
27 p
atie
nts
wer
e su
itab
le fo
r cr
iteria
led
d
isch
arge
, 23
wer
e no
t
►M
ean
wai
t tim
e fo
r th
e 27
sui
tab
le p
atie
nts
prio
r to
dis
char
ge w
as 4
hou
rs a
nd 5
1 m
in
►D
isch
arge
del
ays
wer
e of
ten
caus
ed b
y sy
stem
del
ays
Levi
n94S
tep
- up
inte
rmed
iate
car
e un
its
►A
brid
ging
ser
vice
bet
wee
n ho
spita
l and
hom
e fo
r in
div
idua
ls r
ead
y fo
r d
isch
arge
from
acu
te
care
; allo
ws
for
reco
very
and
reg
aini
ng o
f in
dep
end
ence
Age
d 7
5+H
osp
ital
Infr
astr
uctu
re a
nd
finan
ce
►R
educ
ed b
ed d
ays
del
ayed
►
Rat
e of
day
s d
elay
ed in
crea
sed
ove
r tim
e
Lian
58N
ew d
isch
arge
gui
del
ines
for
pre
mat
ure
bab
ies
►
Dev
elop
men
t of
new
dis
char
ge g
uid
elin
es fo
r p
rem
atur
e ne
onat
es
Pre
mat
ure
infa
nts
Hos
pita
lS
inga
por
e G
ener
al H
osp
ital
Tool
s an
d
guid
elin
es
►R
educ
ed m
edia
n d
urat
ion
of h
osp
italis
atio
n fr
om 5
8.2
day
s to
34.
9 d
ays
►
Cos
t sa
ving
s of
$61
74/in
fant
Mae
ssen
75E
nhan
ced
rec
over
y af
ter
surg
ery
►
Red
uctio
n in
the
pos
top
erat
ive
r eco
very
per
iod
to
red
uce
over
all h
osp
ital l
engt
h of
sta
y
Pat
ient
s un
der
goin
g el
ectiv
e co
lore
ctal
re
sect
ion
Hos
pita
lP
ract
ice
chan
ges
►
No
sign
ifica
nt d
iffer
ence
in p
rop
ortio
n of
p
atie
nts
with
a d
isch
arge
del
ay p
ost-
ER
AS
p
r ogr
amm
e
►A
pp
roxi
mat
ely
90%
of p
atie
nts
pre
and
p
ost-
ER
AS
wer
e no
t d
isch
arge
d o
n th
e d
ay
dis
char
ge c
riter
ia/
func
tiona
l rec
over
y w
ere
met
Mah
ant
(200
8)59
Med
ical
Car
e A
pp
rop
riate
ness
Pro
toco
- aud
it an
d
feed
bac
k
►A
too
l tha
t p
rovi
des
info
rmat
ion
on h
osp
ital
bed
use
(qua
lified
and
non
qua
lified
hos
pita
l d
ays)
Pae
dia
tric
inp
atie
nts
Hos
pita
lH
osp
ital f
or S
ick
Chi
ldre
nTo
ols
and
gu
idel
ines
►
Sig
nific
antly
low
er r
isk
of in
app
rop
riate
ho
spita
l day
s
►D
urin
g th
e in
terv
entio
n, 3
3% o
f bed
day
s w
ere
nonq
ualifi
ed, c
omp
ared
with
47%
pre
- in
terv
entio
n
►N
o ch
ange
in 4
8- ho
ur r
ead
mis
sion
rat
e
Mah
to 76
Hos
pita
l dia
bet
es o
utre
ach
serv
ice
►
A s
ervi
ce t
o p
reve
nt a
dm
issi
on t
hrou
gh a
nu
mb
er o
f str
ateg
ies
(imp
rove
d a
cces
s to
se
rvic
es, m
anag
emen
t of
med
ical
pro
ble
ms,
ea
rly d
isch
arge
pla
nnin
g, o
rgan
isat
ion
of
follo
w- u
p c
are)
Acu
tely
ad
mitt
ed
pat
ient
s w
ith d
iab
etes
Hos
pita
lN
ew C
ross
Hos
pita
l, 70
0 b
eds
Pra
ctic
e ch
ange
s
►R
educ
tion
in b
ed o
ccup
ancy
, ina
pp
rop
riate
ad
mis
sion
s, d
elay
ed d
isch
arge
s an
d e
ffect
ive
dis
char
ge p
lann
ing
Mal
oney
49P
atie
nt t
rack
er
►A
web
- bas
ed a
pp
licat
ion
to fa
cilit
ate
the
dis
char
ge p
roce
ss b
y en
hanc
ing
com
mun
icat
ion
bet
wee
n d
isci
plin
es
Inp
atie
nts
Hos
pita
lP
rimar
y C
hild
ren’
s M
edic
al
Cen
tre
Tool
s an
d
guid
elin
esIn
form
atio
n sh
arin
g liv
e
►
Dec
reas
ed n
umb
er o
f can
celle
d s
urge
ries,
m
edia
n em
erge
ncy
dep
artm
ent
leng
th o
f sta
y an
d a
vera
ge n
umb
er o
f inp
atie
nt a
dm
issi
ons
Man
ville
95Tr
ansi
tiona
l car
e un
it
►A
reh
abili
tatio
n- st
yle
unit
with
enh
ance
d
nurs
ing
and
reh
abili
tatio
n se
rvic
es fo
r el
der
ly
pat
ient
s
Eld
erly
ALC
pat
ient
s (7
0+)
Hos
pita
lS
t Jo
sep
h’s
Hos
pita
l, 22
- bed
tr
ansi
tiona
l car
e un
it
Infr
astr
uctu
re a
nd
finan
ce
►Im
pro
ved
hea
lth o
utco
mes
and
dis
char
ge
dis
pos
ition
, dec
reas
ed le
ngth
of s
tay
and
co
sts
per
pat
ient
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
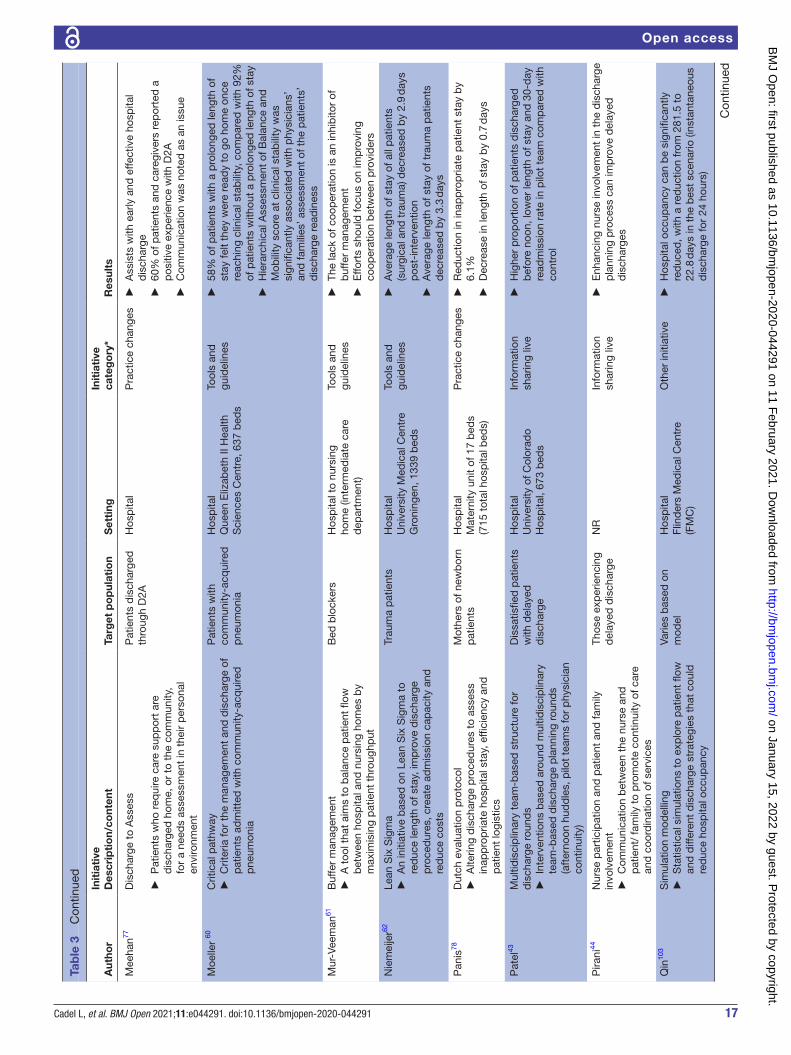
17Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Mee
han77
Dis
char
ge t
o A
sses
s
►
Pat
ient
s w
ho r
equi
re c
are
sup
por
t ar
e d
isch
arge
d h
ome,
or
to t
he c
omm
unity
, fo
r a
need
s as
sess
men
t in
the
ir p
erso
nal
envi
ronm
ent
Pat
ient
s d
isch
arge
d
thro
ugh
D2A
Hos
pita
lP
ract
ice
chan
ges
►
Ass
ists
with
ear
ly a
nd e
ffect
ive
hosp
ital
dis
char
ge
►60
% o
f pat
ient
s an
d c
areg
iver
s re
por
ted
a
pos
itive
exp
erie
nce
with
D2A
►
Com
mun
icat
ion
was
not
ed a
s an
issu
e
Moe
ller
60C
ritic
al p
athw
ay
►C
riter
ia fo
r th
e m
anag
emen
t an
d d
isch
arge
of
pat
ient
s ad
mitt
ed w
ith c
omm
unity
- acq
uire
d
pne
umon
ia
Pat
ient
s w
ith
com
mun
ity- a
cqui
red
p
neum
onia
Hos
pita
lQ
ueen
Eliz
abet
h II
Hea
lth
Sci
ence
s C
entr
e, 6
37 b
eds
Tool
s an
d
guid
elin
es
►58
% o
f pat
ient
s w
ith a
pro
long
ed le
ngth
of
stay
felt
they
wer
e re
ady
to g
o ho
me
once
re
achi
ng c
linic
al s
tab
ility
, com
par
ed w
ith 9
2%
of p
atie
nts
with
out
a p
rolo
nged
leng
th o
f sta
y
►H
iera
rchi
cal A
sses
smen
t of
Bal
ance
and
M
obili
ty s
core
at
clin
ical
sta
bili
ty w
as
sign
ifica
ntly
ass
ocia
ted
with
phy
sici
ans’
an
d fa
mili
es’ a
sses
smen
t of
the
pat
ient
s’
dis
char
ge r
ead
ines
s
Mur
- Vee
man
61B
uffe
r m
anag
emen
t
►A
too
l tha
t ai
ms
to b
alan
ce p
atie
nt fl
ow
bet
wee
n ho
spita
l and
nur
sing
hom
es b
y m
axim
isin
g p
atie
nt t
hrou
ghp
ut
Bed
blo
cker
sH
osp
ital t
o nu
rsin
g ho
me
(inte
rmed
iate
car
e d
epar
tmen
t)
Tool
s an
d
guid
elin
es
►Th
e la
ck o
f coo
per
atio
n is
an
inhi
bito
r of
b
uffe
r m
anag
emen
t
►E
ffort
s sh
ould
focu
s on
imp
rovi
ng
coop
erat
ion
bet
wee
n p
rovi
der
s
Nie
mei
jer62
Lean
Six
Sig
ma
►
An
initi
ativ
e b
ased
on
Lean
Six
Sig
ma
to
red
uce
leng
th o
f sta
y, im
pro
ve d
isch
arge
p
roce
dur
es, c
reat
e ad
mis
sion
cap
acity
and
re
duc
e co
sts
Trau
ma
pat
ient
sH
osp
ital
Uni
vers
ity M
edic
al C
entr
e G
roni
ngen
, 133
9 b
eds
Tool
s an
d
guid
elin
es
►A
vera
ge le
ngth
of s
tay
of a
ll p
atie
nts
(sur
gica
l and
tra
uma)
dec
reas
ed b
y 2.
9 d
ays
pos
t- in
terv
entio
n
►A
vera
ge le
ngth
of s
tay
of t
raum
a p
atie
nts
dec
reas
ed b
y 3.
3 d
ays
Pan
is78
Dut
ch e
valu
atio
n p
roto
col
►
Alte
ring
dis
char
ge p
roce
dur
es t
o as
sess
in
app
rop
riate
hos
pita
l sta
y, e
ffici
ency
and
p
atie
nt lo
gist
ics
Mot
hers
of n
ewb
orn
pat
ient
sH
osp
ital
Mat
erni
ty u
nit
of 1
7 b
eds
(715
tot
al h
osp
ital b
eds)
Pra
ctic
e ch
ange
s
►R
educ
tion
in in
app
rop
riate
pat
ient
sta
y b
y 6.
1%
►D
ecr e
ase
in le
ngth
of s
tay
by
0.7
day
s
Pat
el43
Mul
tidis
cip
linar
y te
am- b
ased
str
uctu
re fo
r d
isch
arge
rou
nds
►
Inte
rven
tions
bas
ed a
r oun
d m
ultid
isci
plin
ary
team
- bas
ed d
isch
arge
pla
nnin
g ro
und
s (a
fter
noon
hud
dle
s, p
ilot
team
s fo
r p
hysi
cian
co
ntin
uity
)
Dis
satis
fied
pat
ient
s w
ith d
elay
ed
dis
char
ge
Hos
pita
lU
nive
rsity
of C
olor
ado
Hos
pita
l, 67
3 b
eds
Info
rmat
ion
shar
ing
live
►
Hig
her
pro
por
tion
of p
atie
nts
dis
char
ged
b
efor
e no
on, l
ower
leng
th o
f sta
y an
d 3
0- d
ay
r ead
mis
sion
rat
e in
pilo
t te
am c
omp
ared
with
co
ntro
l
Pira
ni44
Nur
se p
artic
ipat
ion
and
pat
ient
and
fam
ily
invo
lvem
ent
►
Com
mun
icat
ion
bet
wee
n th
e nu
rse
and
p
atie
nt/
fam
ily t
o p
rom
ote
cont
inui
ty o
f car
e an
d c
oord
inat
ion
of s
ervi
ces
Thos
e ex
per
ienc
ing
del
ayed
dis
char
geN
RIn
form
atio
n sh
arin
g liv
e
►E
nhan
cing
nur
se in
volv
emen
t in
the
dis
char
ge
pla
nnin
g p
roce
ss c
an im
pro
ve d
elay
ed
dis
char
ges
Qin
103
Sim
ulat
ion
mod
ellin
g
►S
tatis
tical
sim
ulat
ions
to
exp
lore
pat
ient
flow
an
d d
iffer
ent
dis
char
ge s
trat
egie
s th
at c
ould
re
duc
e ho
spita
l occ
upan
cy
Varie
s b
ased
on
mod
elH
osp
ital
Flin
der
s M
edic
al C
entr
e (F
MC
)
Oth
er in
itiat
ive
►
Hos
pita
l occ
upan
cy c
an b
e si
gnifi
cant
ly
red
uced
, with
a r
educ
tion
from
281
.5 t
o 22
.8 d
ays
in t
he b
est
scen
ario
(ins
tant
aneo
us
dis
char
ge fo
r 24
hou
rs)
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

18 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Rae
96D
elay
ed d
isch
arge
pro
ject
►
Loca
l aut
horit
ies
are
finan
cial
ly r
esp
onsi
ble
(p
aym
ents
) to
acut
e ho
spita
l whe
n p
atie
nts
rem
ain
in h
osp
ital b
ecau
se c
omm
unity
car
e ar
rang
emen
ts h
ave
not
bee
n m
ade
Acu
te g
ener
al
med
ical
pat
ient
sH
osp
ital
Dun
edin
hos
pita
lIn
fras
truc
ture
and
fin
ance
►
Mea
n le
ngth
of s
tay
dec
reas
ed b
y 2.
6 d
ays
(from
6.5
to
3.9
day
s)
►D
ecre
ased
cos
ts o
f ser
vice
del
iver
y b
y $2
.4 m
illio
n
►B
ed n
umb
ers
dec
reas
ed b
y 24
(fro
m 5
6 to
32
)
►N
o ch
ange
in r
ead
mis
sion
rat
es
Rob
erts
50R
oyal
Reh
abili
tatio
n C
entr
e, S
ydne
y, g
oal l
engt
h of
sta
y to
ol
►A
too
l tha
t re
por
ts t
he le
ngth
of s
tay
ben
chm
ark
figur
es o
n an
ind
ivid
ual p
atie
nt
bas
is
Inp
atie
nts
in t
wo
units
: SR
U (s
trok
e re
hab
ilita
tion
unit)
or
BIR
U (B
rain
Inju
ry
Reh
abili
tatio
n U
nit
Hos
pita
lH
amp
stea
d R
ehab
ilita
tion
Cen
tre,
128
bed
s
Tool
s an
d
guid
elin
esIn
form
atio
n sh
arin
g liv
e
►
Tota
l dis
char
ge d
elay
s fr
om t
he 2
uni
ts
tota
led
631
1 d
ays
►
Leng
th o
f sta
y w
as n
ot d
ecre
ased
►
Neg
ativ
e p
erce
ptio
ns o
f the
pro
gram
me
from
st
aff
Sam
pso
n79D
iab
etes
inp
atie
nt s
pec
ialis
t nu
rse
►
Dia
bet
es m
anag
emen
t, b
ased
on
stru
ctur
ed
grou
p e
duc
atio
n, fo
r al
l dia
bet
es in
pat
ient
s
Dia
bet
es in
pat
ient
sH
osp
ital
Nor
folk
and
Nor
wic
h U
nive
rsity
Hos
pita
l NH
S
Trus
t, 9
89 b
eds
Pra
ctic
e ch
ange
s
►D
ecre
ased
mea
n ex
cess
bed
day
s b
y 0.
7 d
ays
(from
1.9
to
1.2)
Sha
h97C
omm
unity
Car
e (D
elay
ed D
isch
arge
) Act
200
3
►Lo
cal a
utho
ritie
s ar
e fin
anci
ally
res
pon
sib
le
(pay
men
ts) t
o ac
ute
hosp
ital w
hen
pat
ient
s re
mai
n in
hos
pita
l bec
ause
com
mun
ity c
are
arra
ngem
ents
hav
e no
t b
een
mad
e
Inp
atie
nt -
sp
ecia
lties
of
Ger
iatr
ic M
edic
ine
(GM
) and
Old
Age
P
sych
iatr
y (O
AP
) se
rvic
es
Hos
pita
lsIn
fras
truc
ture
and
fin
ance
GM
:
►D
ecre
ased
med
ian
and
mea
n le
ngth
of s
tay
►
Incr
ease
d n
umb
er o
f fini
shed
ep
isod
es
(inp
atie
nt d
isch
arge
s)
►N
o re
latio
nshi
p w
ith n
umb
er o
f bed
day
sO
AP
:
►In
crea
sed
med
ian
and
mea
n le
ngth
of s
tay
►
Dec
reas
ed n
umb
er o
f fini
shed
ep
isod
es
(inp
atie
nt d
isch
arge
s)
►In
crea
sed
num
ber
of b
ed d
ays
Sob
otka
51H
osp
ital-
to- h
ome
tran
sitio
nal c
are
pro
gram
me
at
AH
K
►
A p
rogr
amm
e to
sup
por
t an
d e
duc
ate
fam
ilies
on
pro
vid
ing
care
for
med
ical
ly s
tab
le c
hild
ren
at h
ome
Pae
dia
tric
inp
atie
ntTr
ansi
tiona
l and
Res
pite
C
entr
eA
lmos
t H
ome
Kid
s
Pra
ctic
e ch
ange
sIn
form
atio
n sh
arin
g liv
e
►
2 m
onth
s fo
llow
ing
sup
por
t at
AH
K, t
he
pat
ient
tra
nsiti
oned
hom
e to
be
care
d fo
r b
y hi
s m
othe
r an
d h
ome
care
tea
m
Sta
rr-
Hem
bur
r ow
80H
ome
Firs
t
►A
pr o
gram
me
des
igne
d t
o he
lp k
eep
pat
ient
s in
the
ir ho
mes
(with
com
mun
ity s
upp
orts
) for
as
long
as
pos
sib
le; f
ocus
ing
on p
rovi
din
g ac
cess
to
need
ed s
ervi
ces
ALC
pat
ient
sH
osp
itals
Pra
ctic
e ch
ange
s
►R
ate
of A
LC p
atie
nts
dec
reas
ed b
y at
leas
t 50
% a
cros
s th
e re
gion
of s
tud
y
Sut
herla
nd45
Bui
ld m
ore;
Inte
grat
ed c
are;
and
Fin
anci
al
ince
ntiv
es
►Th
ree
stra
tegi
es t
o im
pro
ve A
LC im
pac
t on
ho
spita
ls (b
uild
mor
e b
eds,
inte
grat
ed c
are,
fin
anci
al in
cent
ives
for
pos
t- ac
ute
pro
vid
ers)
ALC
pat
ient
sH
osp
itals
Info
rmat
ion
shar
ing
reco
mm
end
atio
n d
ocum
ent
►
N/A
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
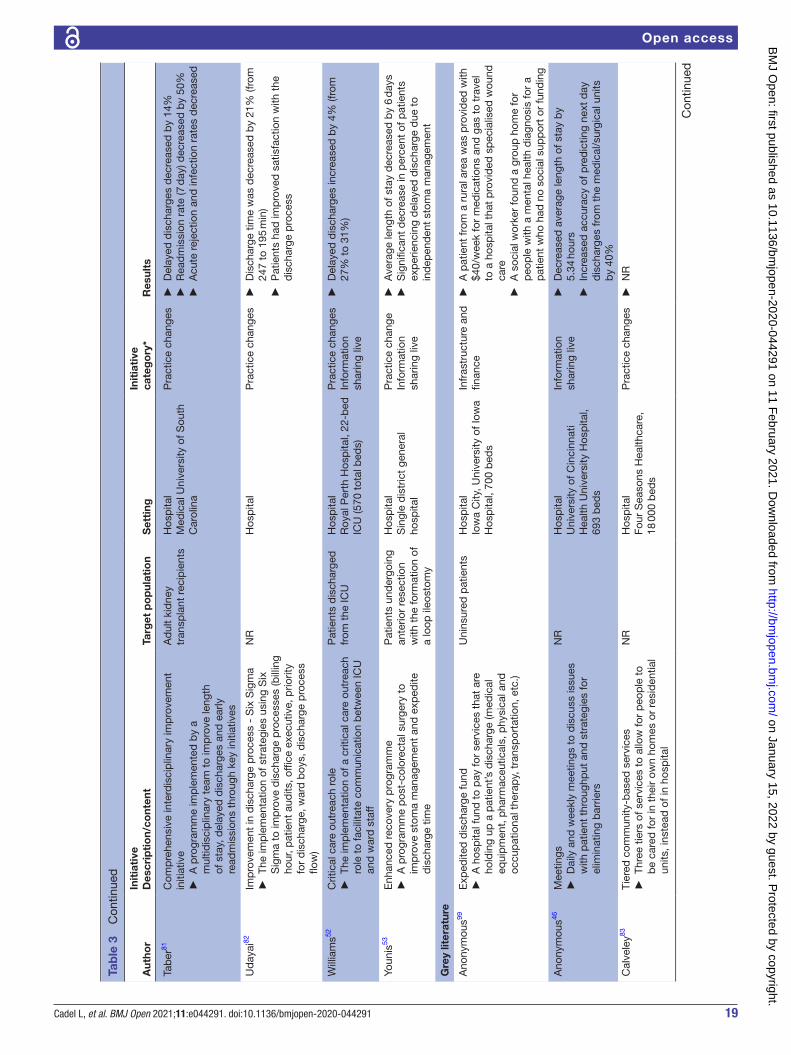
19Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Tab
er81
Com
pre
hens
ive
inte
rdis
cip
linar
y im
pro
vem
ent
initi
ativ
e
►A
pro
gram
me
imp
lem
ente
d b
y a
mul
tidis
cip
linar
y te
am t
o im
pro
ve le
ngth
of
sta
y, d
elay
ed d
isch
arge
s an
d e
arly
re
adm
issi
ons
thro
ugh
key
initi
ativ
es
Ad
ult
kid
ney
tran
spla
nt r
ecip
ient
sH
osp
ital
Med
ical
Uni
vers
ity o
f Sou
th
Car
olin
a
Pra
ctic
e ch
ange
s
►D
elay
ed d
isch
arge
s d
ecre
ased
by
14%
►
Rea
dm
issi
on r
ate
(7 d
ay) d
ecre
ased
by
50%
►
Acu
te r
ejec
tion
and
infe
ctio
n ra
tes
dec
reas
ed
Ud
ayai
82Im
pro
vem
ent
in d
isch
arge
pro
cess
- S
ix S
igm
a
►Th
e im
ple
men
tatio
n of
str
ateg
ies
usin
g S
ix
Sig
ma
to im
pro
ve d
isch
arge
pro
cess
es (b
illin
g ho
ur, p
atie
nt a
udits
, offi
ce e
xecu
tive,
prio
rity
for
dis
char
ge, w
ard
boy
s, d
isch
arge
pro
cess
flo
w)
NR
Hos
pita
lP
ract
ice
chan
ges
►
Dis
char
ge t
ime
was
dec
reas
ed b
y 21
% (f
rom
24
7 to
195
min
)
►P
atie
nts
had
imp
rove
d s
atis
fact
ion
with
the
d
isch
arge
pro
cess
Will
iam
s52C
ritic
al c
are
outr
each
rol
e
►Th
e im
ple
men
tatio
n of
a c
ritic
al c
are
outr
each
ro
le t
o fa
cilit
ate
com
mun
icat
ion
bet
wee
n IC
U
and
war
d s
taff
Pat
ient
s d
isch
arge
d
from
the
ICU
Hos
pita
lR
oyal
Per
th H
osp
ital,
22- b
ed
ICU
(570
tot
al b
eds)
Pra
ctic
e ch
ange
sIn
form
atio
n sh
arin
g liv
e
►
Del
ayed
dis
char
ges
incr
ease
d b
y 4%
(fro
m
27%
to
31%
)
Youn
is53
Enh
ance
d r
ecov
ery
pro
gram
me
►
A p
rogr
amm
e p
ost-
colo
rect
al s
urge
ry t
o im
pro
ve s
tom
a m
anag
emen
t an
d e
xped
ite
dis
char
ge t
ime
Pat
ient
s un
der
goin
g an
terio
r re
sect
ion
with
the
form
atio
n of
a
loop
ileo
stom
y
Hos
pita
lS
ingl
e d
istr
ict
gene
ral
hosp
ital
Pra
ctic
e ch
ange
Info
rmat
ion
shar
ing
live
►
Ave
rage
leng
th o
f sta
y d
ecre
ased
by
6 d
ays
►
Sig
nific
ant
dec
reas
e in
per
cent
of p
atie
nts
exp
erie
ncin
g d
elay
ed d
isch
arge
due
to
ind
epen
den
t st
oma
man
agem
ent
Gre
y lit
erat
ure
Ano
nym
ous99
Exp
edite
d d
isch
arge
fund
►
A h
osp
ital f
und
to
pay
for
serv
ices
tha
t ar
e ho
ldin
g up
a p
atie
nt’s
dis
char
ge (m
edic
al
equi
pm
ent,
pha
rmac
eutic
als,
phy
sica
l and
oc
cup
atio
nal t
hera
py,
tra
nsp
orta
tion,
etc
.)
Uni
nsur
ed p
atie
nts
Hos
pita
lIo
wa
City
, Uni
vers
ity o
f Iow
a H
osp
ital,
700
bed
s
Infr
astr
uctu
re a
nd
finan
ce
►A
pat
ient
from
a r
ural
are
a w
as p
rovi
ded
with
$4
0/w
eek
for
med
icat
ions
and
gas
to
trav
el
to a
hos
pita
l tha
t p
rovi
ded
sp
ecia
lised
wou
nd
care
►
A s
ocia
l wor
ker
foun
d a
gro
up h
ome
for
peo
ple
with
a m
enta
l hea
lth d
iagn
osis
for
a p
atie
nt w
ho h
ad n
o so
cial
sup
por
t or
fund
ing
Ano
nym
ous46
Mee
tings
►
Dai
ly a
nd w
eekl
y m
eetin
gs t
o d
iscu
ss is
sues
w
ith p
atie
nt t
hrou
ghp
ut a
nd s
trat
egie
s fo
r el
imin
atin
g b
arrie
rs
NR
Hos
pita
lU
nive
rsity
of C
inci
nnat
i H
ealth
Uni
vers
ity H
osp
ital,
693
bed
s
Info
rmat
ion
shar
ing
live
►
Dec
reas
ed a
vera
ge le
ngth
of s
tay
by
5.34
hou
rs
►In
crea
sed
acc
urac
y of
pre
dic
ting
next
day
d
isch
arge
s fr
om t
he m
edic
al/s
urgi
cal u
nits
b
y 40
%
Cal
vele
y83Ti
ered
com
mun
ity- b
ased
ser
vice
s
►Th
ree
tiers
of s
ervi
ces
to a
llow
for
peo
ple
to
be
care
d fo
r in
the
ir ow
n ho
mes
or
resi
den
tial
units
, ins
tead
of i
n ho
spita
l
NR
Hos
pita
lFo
ur S
easo
ns H
ealth
care
, 18
000
bed
s
Pra
ctic
e ch
ange
s
►N
R
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
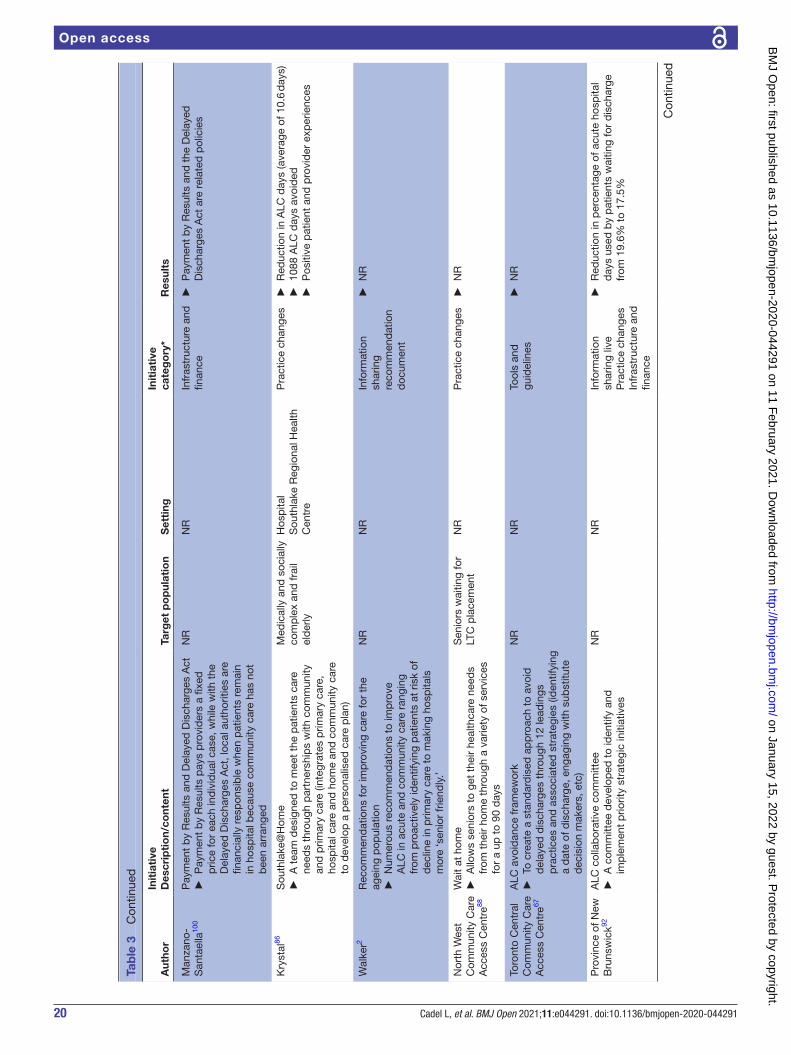
20 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
Man
zano
- S
anta
ella
100
Pay
men
t b
y R
esul
ts a
nd D
elay
ed D
isch
arge
s A
ct
►P
aym
ent
by
Res
ults
pay
s p
r ovi
der
s a
fixed
p
rice
for
each
ind
ivid
ual c
ase,
whi
le w
ith t
he
Del
ayed
Dis
char
ges
Act
, loc
al a
utho
ritie
s ar
e fin
anci
ally
res
pon
sib
le w
hen
pat
ient
s re
mai
n in
hos
pita
l bec
ause
com
mun
ity c
are
has
not
bee
n ar
rang
ed
NR
NR
Infr
astr
uctu
re a
nd
finan
ce
►P
aym
ent
by
Res
ults
and
the
Del
ayed
D
isch
arge
s A
ct a
re r
elat
ed p
olic
ies
Kry
stal
86S
outh
lake
@H
ome
►
A t
eam
des
igne
d t
o m
eet
the
pat
ient
s ca
r e
need
s th
roug
h p
artn
ersh
ips
with
com
mun
ity
and
prim
ary
care
(int
egra
tes
prim
ary
care
, ho
spita
l car
e an
d h
ome
and
com
mun
ity c
are
to d
evel
op a
per
sona
lised
car
e p
lan)
Med
ical
ly a
nd s
ocia
lly
com
ple
x an
d fr
ail
eld
erly
Hos
pita
lS
outh
lake
Reg
iona
l Hea
lth
Cen
tre
Pra
ctic
e ch
ange
s
►R
educ
tion
in A
LC d
ays
(ave
rage
of 1
0.6
day
s)
►10
88 A
LC d
ays
avoi
ded
►
Pos
itive
pat
ient
and
pro
vid
er e
xper
ienc
es
Wal
ker2
Rec
omm
end
atio
ns fo
r im
pro
ving
car
e fo
r th
e ag
eing
pop
ulat
ion
►
Num
erou
s re
com
men
dat
ions
to
imp
rove
A
LC in
acu
te a
nd c
omm
unity
car
e ra
ngin
g fr
om p
roac
tivel
y id
entif
ying
pat
ient
s at
ris
k of
d
eclin
e in
prim
ary
care
to
mak
ing
hosp
itals
m
ore
‘sen
ior
frie
ndly
.’
NR
NR
Info
rmat
ion
shar
ing
reco
mm
end
atio
n d
ocum
ent
►
NR
Nor
th W
est
Com
mun
ity C
are
Acc
ess
Cen
tre88
Wai
t at
hom
e
►A
llow
s se
nior
s to
get
the
ir he
alth
care
nee
ds
from
the
ir ho
me
thro
ugh
a va
riety
of s
ervi
ces
for
a up
to
90 d
ays
Sen
iors
wai
ting
for
LTC
pla
cem
ent
NR
Pra
ctic
e ch
ange
s
►N
R
Toro
nto
Cen
tral
C
omm
unity
Car
e A
cces
s C
entr
e67
ALC
avo
idan
ce fr
amew
ork
►
To c
reat
e a
stan
dar
dis
ed a
pp
roac
h to
avo
id
del
ayed
dis
char
ges
thro
ugh
12 le
adin
gs
pra
ctic
es a
nd a
ssoc
iate
d s
trat
egie
s (id
entif
ying
a
dat
e of
dis
char
ge, e
ngag
ing
with
sub
stitu
te
dec
isio
n m
aker
s, e
tc)
NR
NR
Tool
s an
d
guid
elin
es
►N
R
Pro
vinc
e of
New
B
runs
wic
k92A
LC c
olla
bor
ativ
e co
mm
ittee
►
A c
omm
ittee
dev
elop
ed t
o id
entif
y an
d
imp
lem
ent
prio
rity
stra
tegi
c in
itiat
ives
NR
NR
Info
rmat
ion
shar
ing
live
Pra
ctic
e ch
ange
sIn
fras
truc
ture
and
fin
ance
►
Red
uctio
n in
per
cent
age
of a
cute
hos
pita
l d
ays
used
by
pat
ient
s w
aitin
g fo
r d
isch
arge
fr
om 1
9.6%
to
17.5
%
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

21Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Aut
hor
Init
iati
veD
escr
ipti
on/
cont
ent
Targ
et p
op
ulat
ion
Set
ting
Init
iati
ve
cate
go
ry*
Res
ults
NH
S
Imp
rove
men
t104
SA
FER
pat
ient
flow
bun
dle
►
A t
ool t
o re
duc
e d
elay
s fo
r p
atie
nts
on
inp
atie
nt w
ard
s
NR
NR
Info
rmat
ion
shar
ing
reco
mm
end
atio
n d
ocum
ent
►
Mos
t ef
fect
ive
whe
n us
ed w
ith R
ed2G
reen
d
ays
►
Sup
por
ts d
ecis
ion
mak
ing
by
allo
win
g st
aff t
o vi
sual
ise
pla
ns
Red
2Gre
en d
ays
►
A t
ool t
o re
duc
e un
nece
ssar
y w
aitin
g b
y p
atie
nts
NR
NR
►
A b
oard
(ele
ctro
nic
or w
hite
) sho
uld
act
as
a fo
cal p
oint
for
roun
ds
Long
- sta
y p
atie
nt r
evie
ws
►
Wee
kly
revi
ews
of lo
ng- s
tay
pat
ient
s (>
20 d
ays)
, to
help
ad
dre
ss o
bst
acle
s th
at a
re
del
ayin
g d
isch
arge
NR
NR
►
Wee
kly
long
- sta
y p
atie
nt r
evie
ws
can
red
uce
the
num
ber
of i
npat
ient
s w
ith a
leng
th o
f sta
y >
20 d
ays
by
up t
o 50
%
Mul
tiage
ncy
Dis
char
ge E
vent
►
Rev
iew
of i
ndiv
idua
l pat
ient
jour
neys
by
brin
ging
tog
ethe
r se
nior
sta
ff fr
om h
ealth
and
so
cial
car
e
NR
NR
►
Gre
ates
t im
pac
t on
pat
ient
s w
ith a
leng
th o
f st
ay >
6 d
ays
Cen
tral
Eas
t LH
IN A
LC T
ask
Gro
up84
Hom
e Fi
rst
►
A p
rogr
amm
e d
esig
ned
to
help
kee
p p
atie
nts
in t
heir
hom
es (w
ith c
omm
unity
sup
por
ts) f
or
as lo
ng a
s p
ossi
ble
by
conn
ectin
g p
atie
nts
to
thei
r ne
eded
res
ourc
es
NR
Hos
pita
lH
alto
n H
ealth
Ser
vice
s, 4
59
bed
s
Pra
ctic
e ch
ange
s
►P
erce
nt o
f ALC
(acu
te) r
educ
ed fr
om 2
2%–
28%
to
4%–6
%
Ad
ams,
Car
e an
d R
epai
r E
ngla
nd98
Hom
e Fi
rst
►
A p
rogr
amm
e d
esig
ned
to
help
kee
p h
igh
need
s se
nior
s in
the
ir ho
mes
(with
com
mun
ity
sup
por
ts) f
or a
s lo
ng a
s p
ossi
ble
and
invo
lve
the
fam
ily in
car
e
Pat
ient
s (s
pec
ifica
lly
high
nee
ds
seni
ors)
NR
Pra
ctic
e ch
ange
s
►N
R
Sha
h89H
ome
Firs
t
►A
pro
gram
me
des
igne
d t
o he
lp k
eep
pat
ient
s in
the
ir ho
mes
(with
enh
ance
d h
ome
care
su
pp
orts
) as
they
wai
t fo
r lo
ng- t
erm
car
e
Hig
h ne
ed s
enio
rs
(75+
)Tr
illiu
m H
ealth
Par
tner
s,
vario
us c
omm
unity
and
long
- te
rm c
are
orga
nisa
tions
Pra
ctic
e ch
ange
s
►2-
fold
red
uctio
n in
mon
thly
ave
rage
of A
LC
pat
ient
s
►30
.5%
red
uctio
n in
num
ber
of A
LC t
o LT
C
hosp
ital r
efer
rals
Join
t Im
pro
vem
ent
Team
85
►
NR
ALC
pat
ient
s9
com
mun
ity h
osp
ital
corp
orat
ions
, 14
hosp
ital
site
s an
d a
men
tal h
ealth
ce
ntre
in o
ne O
ntar
io r
egio
n16
42 b
eds
acro
ss t
he
faci
litie
s
Pra
ctic
e ch
ange
s
►E
xpec
ted
to
red
uced
ALC
day
s b
y 30
% o
ver
the
next
3 y
ears
Ad
ams,
Car
e an
d R
epai
r E
ngla
nd98
Wes
t of
Eng
land
car
e an
d r
epai
r
►E
nab
les
old
er p
atie
nts
to r
etur
n ho
me
from
ho
spita
l qui
ckly
and
saf
ely
by
orga
nisi
ng a
nd
rep
airin
g ho
me
(cle
anin
g, c
lear
ing
clut
ter,
smal
l ad
apta
tions
)
Old
er p
atie
nts
Wes
t of
Eng
land
Car
e an
d
Rep
air
Infr
astr
uctu
re a
nd
finan
ce
►S
ubst
antia
l cos
t sa
ving
s in
hos
pita
l bed
day
s,
hous
ing
inte
rven
tions
and
hos
pita
l sta
ff tim
e
Tab
le 3
C
ontin
ued
Con
tinue
d
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
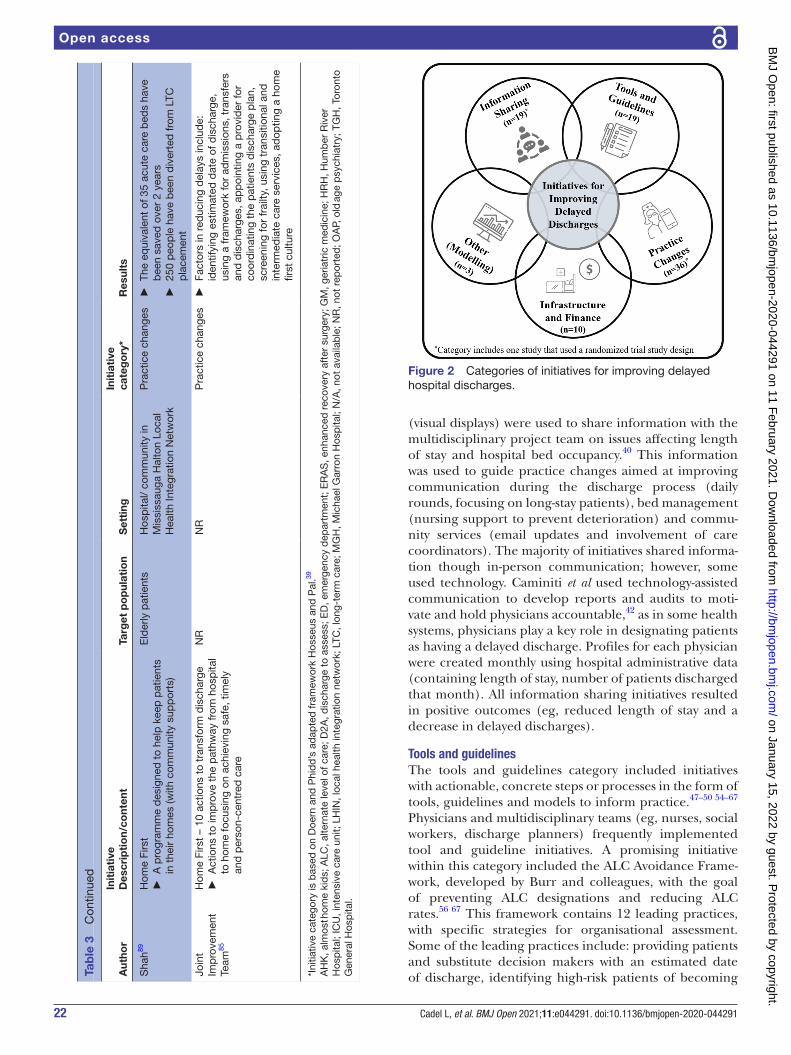
22 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
(visual displays) were used to share information with the multidisciplinary project team on issues affecting length of stay and hospital bed occupancy.40 This information was used to guide practice changes aimed at improving communication during the discharge process (daily rounds, focusing on long- stay patients), bed management (nursing support to prevent deterioration) and commu-nity services (email updates and involvement of care coordinators). The majority of initiatives shared informa-tion though in- person communication; however, some used technology. Caminiti et al used technology- assisted communication to develop reports and audits to moti-vate and hold physicians accountable,42 as in some health systems, physicians play a key role in designating patients as having a delayed discharge. Profiles for each physician were created monthly using hospital administrative data (containing length of stay, number of patients discharged that month). All information sharing initiatives resulted in positive outcomes (eg, reduced length of stay and a decrease in delayed discharges).
Tools and guidelinesThe tools and guidelines category included initiatives with actionable, concrete steps or processes in the form of tools, guidelines and models to inform practice.47–50 54–67 Physicians and multidisciplinary teams (eg, nurses, social workers, discharge planners) frequently implemented tool and guideline initiatives. A promising initiative within this category included the ALC Avoidance Frame-work, developed by Burr and colleagues, with the goal of preventing ALC designations and reducing ALC rates.56 67 This framework contains 12 leading practices, with specific strategies for organisational assessment. Some of the leading practices include: providing patients and substitute decision makers with an estimated date of discharge, identifying high- risk patients of becoming A
utho
rIn
itia
tive
Des
crip
tio
n/co
nten
tTa
rget
po
pul
atio
nS
etti
ngIn
itia
tive
ca
teg
ory
*R
esul
ts
Sha
h89H
ome
Firs
t
►A
pro
gram
me
des
igne
d t
o he
lp k
eep
pat
ient
s in
the
ir ho
mes
(with
com
mun
ity s
upp
orts
)
Eld
erly
pat
ient
sH
osp
ital/
com
mun
ity in
M
issi
ssau
ga H
alto
n Lo
cal
Hea
lth In
tegr
atio
n N
etw
ork
Pra
ctic
e ch
ange
s
►Th
e eq
uiva
lent
of 3
5 ac
ute
care
bed
s ha
ve
bee
n sa
ved
ove
r 2
year
s
►25
0 p
eop
le h
ave
bee
n d
iver
ted
from
LTC
p
lace
men
t
Join
t Im
pro
vem
ent
Team
85
Hom
e Fi
rst
– 10
act
ions
to
tran
sfor
m d
isch
arge
►
Act
ions
to
imp
r ove
the
pat
hway
from
hos
pita
l to
hom
e fo
cusi
ng o
n ac
hiev
ing
safe
, tim
ely
and
per
son-
cent
r ed
car
e
NR
NR
Pra
ctic
e ch
ange
s
►Fa
ctor
s in
red
ucin
g d
elay
s in
clud
e:
iden
tifyi
ng e
stim
ated
dat
e of
dis
char
ge,
usin
g a
fram
ewor
k fo
r ad
mis
sion
s, t
rans
fers
an
d d
isch
arge
s, a
pp
oint
ing
a p
rovi
der
for
coor
din
atin
g th
e p
atie
nts
dis
char
ge p
lan,
sc
reen
ing
for
frai
lty, u
sing
tra
nsiti
onal
and
in
term
edia
te c
are
serv
ices
, ad
optin
g a
hom
e fir
st c
ultu
re
*Ini
tiativ
e ca
tego
ry is
bas
ed o
n D
oern
and
Phi
dd
’s a
dap
ted
fram
ewor
k H
osse
us a
nd P
al.39
AH
K, a
lmos
t hom
e ki
ds;
ALC
, alte
rnat
e le
vel o
f car
e; D
2A, d
isch
arge
to
asse
ss; E
D, e
mer
genc
y d
epar
tmen
t; E
RA
S, e
nhan
ced
rec
over
y af
ter
surg
ery;
GM
, ger
iatr
ic m
edic
ine;
HR
H, H
umb
er R
iver
H
osp
ital;
ICU
, int
ensi
ve c
are
unit;
LH
IN, l
ocal
hea
lth in
tegr
atio
n ne
twor
k; L
TC, l
ong-
term
car
e; M
GH
, Mic
hael
Gar
ron
Hos
pita
l; N
/A, n
ot a
vaila
ble
; NR
, not
rep
orte
d; O
AP,
old
age
psy
chia
try;
TG
H, T
oron
to
Gen
eral
Hos
pita
l.
Tab
le 3
C
ontin
ued
Figure 2 Categories of initiatives for improving delayed hospital discharges.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

23Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
ALC and implementing escalation processes for the management of ALC challenges. Additional initiatives focused on improving patient flow through criteria- led discharges (discharging patients once a predetermined set of criteria had been met) and critical pathways/discharge guidelines.
The majority of initiatives categorised as tools and guidelines had positive results,47–49 54–60 62 64–66 which included a reduction in hospital days and length of stay. However, one initiative, the Goal Length of Stay Tool, did not have positive outcomes on length of stay.50 This initia-tive incorporated information sharing into a computer- based programme to identify patients whose length of stay exceeded their benchmark figure. It had no change on length of stay and was perceived negatively by staff because they did not believe the benchmark figure was an accurate representation of a patient’s current functional status and readiness for discharge.
Practice changesThis category included initiatives that altered how usual care was delivered.51–55 63–66 68–92 Common practice change initiatives included hospital- based, nurse- led discharges and cross- sectoral transitional programmes (eg, Home First, Discharge to Assess, Hospital to Home). Most were implemented by nurses and multidisciplinary teams. Nurse- led and criteria- led discharges often involved a predetermined list of criteria (clinical parameters) that a patient was required to meet in order to be discharged from hospital by a member of the discharge team. For example, Graham et al conducted a retrospective study (N=128) to compare nurse- led and doctor- led discharge (standard discharge pathway) postlaparoscopic surgery.74 For nurse- led discharge, the patient had to meet 13 pre- established criteria (stable vital signs and comparable to baseline on admission; achieved optimal mobility; minimal nausea, vomiting and dizziness; adequate pain control; received written and verbal instructions about postoperative care, etc). When compared with the doctor- led discharge group (n=64), patients in the nurse- led group (n=64) were significantly more likely to be discharged on the day of surgery. Incomparing reasons for the success of the nurse- led model, the authors did not tieit to patient factors but rather the ready availability of the nurse specialistwho was able to implement the clearly outlined discharge criteria (specific fornurse- led discharge) much more quickly than the doctor- led group (who did not use suchcriteria).
Another unique example of a practice change initiative was the 7- day Hospital Initiative implemented by Blecker et al.70 The purpose of this observational study was to eval-uate the impact of increasing weekend staff (hospitalists, care managers, social workers) and services on length of stay, percent of patients discharged on weekends, 30- day readmission rate and in- hospital mortality rate. This multifaceted intervention resulted in a decreased average length of stay, an increased proportion of
weekend discharges and no impact on readmission rates or mortality.
The majority of initiatives categorised as a practice change resulted in positive outcomes on length of stay and rate of discharge delays. However, there were several initia-tives that were perceived negatively by patients,77 or had no change68 75 or a negative impact52 on study outcomes (increase in delayed discharges). Meehan et al explored patient experiences with a programme (Discharge to Assess) that discharged patients who were clinically ready but still required support, in order for their needs to be assessed in their own environment (ie, at home).77 Nega-tive experiences were described by participants (patients and caregivers) who indicated feeling ignored, had poor communication with their healthcare providers and were not involved in the decision- making process. Negative outcomes were also identified in Williams et al prospective cohort study.52 This study evaluated the impact of a crit-ical care outreach role on delays in discharge and iden-tified that discharge delays from the intensive care unit increased over the study period with the implementation of this role. The authors emphasised the importance of a multifaceted and collaborative approach (involving multiple stakeholders/ team members), focusing on patient flow throughout the hospital in order to address the numerous factors impacting delays.
Infrastructure and financeThe infrastructure and finance category included initia-tives that involved tangible structural or financial changes (eg, building more long- term care beds to facilitate the transition of patients out of hospital, financial penalties for remaining in hospital after being medically ready for discharge).55 92–100 The Community Care (Delayed Discharges) Act in the UK was an initiative identified in multiple articles.93 96 97 100 This initiative required local authorities to make payments to acute hospitals when patients could not be discharged because appropriate community care arrangements had not been made. Although this measure was not necessarily enforced, it created incentive for the hospital and community to work together more collaboratively. Additionally, transitional care units94 95 and discharge funds98 99 were common initiatives implemented to address delayed discharges among elderly patients. Transitional care units focused on rehabilitation to promote recovery and the regaining of independence, while discharge funds paid for services that were preventing the patient from being discharged or returning home (eg, medical equipment, medications, transportation, home repairs). All initiatives categorised as infrastructure and finance had positive results on study outcomes, including reductions in discharge delays, length of stay and cost.93–98
Other initiativesThe other initiatives category included statistical and predictive modelling of initiatives to improve delayed discharges.101–103 These models explored the impact of
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

24 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
increasing the supply of nursing home beds,101 potential care pathways for the elderly and reimbursement costs102 and discharge strategies to reduce hospital occupancy.103 Gaughan et al's modelling and empirical analysis iden-tified that increasing the supply of long- term care beds can decrease delayed discharges caused by a lack of social care.101 Their models further emphasised the importance of communication between hospitals and the long- term care sector to reduce social care delayed discharges. Simi-larly, Katsaliaki et al used discrete- event simulations to determine care pathways and associated costs, in which they identified that adding new beds in hospital or inter-mediate care could reduce delay times.102
Recommended initiatives: calls to actionSeveral articles were not evaluations but reports or reviews consisting of recommended initiatives to address delayed hospital discharges, which often combined a number of the categories illustrated above.2 45 92 104 Sutherland and Crump outlined three key solutions for improving delayed discharges in Canada: building more acute and postacute care beds, increasing integrated care and creating finan-cial incentives to improve the quality, quantity and effec-tiveness of healthcare.45 The authors discussed challenges and limitations to implementing each of these options and emphasised that a potential solution to addressing delayed discharges was to combine the three strategies. Another Canadian report developed recommendations for providing care to the ageing population and those experiencing a delayed discharge.2 Walker outlined recommendations for improving primary care, the care continuum and senior friendly acute care, responding to special needs populations (eg, persons with mental health concerns, addiction and neurological conditions, on dial-ysis or ventilators), and implementing an ‘Assess and Restore’ model (a programme to help patients maintain or regain functional independence, transition to home and remain in the community for as long as possible).
The NHS improvement (UK) also released a guide in 2019 on reducing long hospital stays.104 This guide contained several recommendations for tackling delayed discharges including: a patient flow bundle (a tool to reduce delays for patients on inpatient wards), Red2Green Days (a visual tool to reduce unnecessary waiting by patients by supporting the rounding process), long- stay patient reviews (weekly reviews of long- stay patients (>20 days), to help tackle obstacles that are delaying discharge) and multiagency discharge events (review of individual patient journeys by bringing together senior staff from the local health and social care system).
DISCUSSIONThe purpose of this scoping review was to identify best practices for reducing delayed discharges, examine the characteristics of identified initiatives and develop recom-mendations for future work. Based on the 66 included articles, our findings showed that: (1) initiatives are
focused on quantitative outcomes, with limited assess-ment of the impact on patient, caregiver and provider experiences; (2) the sustainability of initiatives overtime is not measured (3) there is a lack of important contex-tual information reported (eg, population characteris-tics, setting, implementation processes) and (4) there are inconsistencies in how delayed discharges are defined.
This review highlighted where the majority of efforts around addressing delayed discharges have been placed. Practice change was the most common categorisation of initiatives (n=36), followed by information sharing (n=19) and infrastructure and finance (n=19). All initiatives cate-gorised as information sharing and infrastructure and finance reported positive outcomes. Despite reporting positive outcomes, many information sharing initiatives promoted communication between staff, with a limited number targeting communication with patients and families. Additionally, there were more initiatives imple-mented in a single sector (eg, in hospital) in comparison to cross- sectoral initiatives (eg, hospital and home care).
Length of stay was the most common outcome measured in this scoping review, with a limited number of articles exploring patient, caregiver and provider experiences. For example, could it be considered a success if an initia-tive does not result in a reduced length of stay, but allows patients to obtain broader goals related to their care (ie, being able to return home) or enhance their care expe-rience? Qualitative methods, including the capturing of patient, caregiver and provider experiences, would allow for a deeper exploration and understanding of success from the perspectives of different stakeholders involved in the initiative.105–107 Experiential evidence on whether an intervention is working is required. As noted in our review, a tool developed to better understand delayed discharge was deemed irrelevant by care providers who felt that the tool captured the wrong information.50 There-fore, capturing providers’ experiences and perspectives are essential in understanding effectiveness of strategies as well as uptake. Most articles included in this scoping review used a quantitative study design, with limited arti-cles using mixed methods or qualitative approaches; thus highlighting a key focus for future research.
The majority of initiatives had an intervention or follow- up period of 1 year, but this ranged from 4 months to 3 years. Based on the limited number initiatives with a follow- up period of longer than 1 year (n=8), there is a need for more formal evaluations with longer follow- up periods to measure the sustainability of initiatives over time. For example, Shelton et al’s Integrated Sustain-ability Framework consists of five categories of factors associated with the sustainability of interventions across different contexts and settings: outer context (eg, poli-cies, leadership, funding), inner context (eg, culture, mission, funding), intervention characteristics (eg, cost, adaptability, benefit), processes (eg, partnership, training/support, planning, capacity building) and implementer and population characteristics (eg, imple-mentation skills/expertise, attitudes/motivation).108
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

25Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
Shelton et al recommended prospective, multi- level and mixed methods study designs for studying the impact and sustainability of interventions. Overall, the initiatives included in this scoping review had positive short- term impacts, but it is unclear if these outcomes are main-tained over time. This emphasises the need to design and implement interventions with sustainability in mind.
The majority of categories of initiatives resulted in posi-tive outcomes; however, initiatives classified as practice change had the most mixed outcomes (positive, negative and no change). Practice changes often require a greater number of resources and are more complex to implement than static solutions (ie, hosting daily rounds, developing a framework, etc). A recent systematic review (2018) conducted by Geerligs et al identified implementation barriers and facilitators of patient- focused, in- hospital interventions,109 highlighting the complex interplay of factors that can impact implementation. Three domains, with the potential to impact the implementation process, were identified: system (environmental context, culture, communication processes and external requirements), staff (commitment and attitudes, understanding and awareness, role identity and skills, ability and confidence) and intervention (ease of integration, face validity, safety and legality and supportive components). Thus, it is important for interventions to be nimble and adaptable to support the changing need of patients, caregivers, providers, organisations and policy contexts over time.
It was also unclear if some initiatives moved prob-lems from one sector to another. For example, adding more intermediate care beds may alleviate pressures in acute care in the short- term but eventually also be at full capacity if community resources are not available. The 7- day hospital discharge initiative highlighted in this review, improved hospital throughput but had no impact on re- admissions,70 suggesting that thinking beyond one sector is required. It is encouraging that most practice change initiatives resulted in improved outcomes, but more clarity is needed to understand what the trade- offs were, as well as how to scale- up the successful initiatives.
Health systems also need to consider their broader goals around delayed hospital discharge—should it only be about reducing delays or should we place an equal focus on optimising patient and caregiver experiences and outcomes? The health system context, including the funding environment, will ultimately shape what inter-ventions get implemented and how they are sustained over time. Some interventions may be considered low value in some countries and contexts and high value in others. Additionally, certain initiatives may be more effective in different environments, as variations in the number of hospital and long- term care beds per capita, infrastructure financing and degree of integration across sectors may impact the outcomes of an initiative. Future research needs to better understand why some strategies may thrive in some environments and not others.
Another key finding identified in the scoping review was the lack of information and details on the implementation
strategy (how strategies were implemented, over what time period, how implementation challenges were dealt with), setting (where was it implemented) and popu-lation characteristics (who was it implemented for). The implementation of initiatives can be impacted by differences in healthcare system structure and funding. Further, this contextual information is essential for both understanding outcomes, scaling- up and sustainability of interventions because it is not only important to know if the intervention was effective, but also for whom and in what context it was effective.110 111
Finally, this review highlighted a lack of consistency in how delayed discharge was defined, both within and across countries. While there was one definition that was used more frequently (a patient was identified as medi-cally ready/fit for discharge, but remained in hospital), there can be different interpretations of when a patient is considered ‘medically fit’ and who makes this deci-sion. Inconsistent definitions can lead to variations in the reported rates of delayed discharge, which can further impact the perceived applicability and effectiveness of an intervention. Our finding was echoed in a narrative review conducted by Glasby et al, who further explained the challenges differing definitions create when attempting to compare findings.112 In order to mitigate these chal-lenges, it is critical to be more consistent around how delayed discharges are defined.
Future workFrom this review, we have identified areas for future research. First, patient, family and provider needs and experiences should be explored during the development and implementation of initiatives aimed at improving delayed discharges. Patient and family engagement is both important and recommended by healthcare and govern-ment organisations; however, they are often excluded in the development and write- up of best practice guide-lines.113 Second, evaluation studies that track outcomes over a longer period of time should be conducted to study the sustainability of initiatives over time, how they are adapted (developmental evaluations), as well as their impact on other sectors (eg, primary and commu-nity care). Third, initiatives should be implemented and integrated across sectors (hospital, primary care and home and community care) to help get at the root of the problem and ensure the implementation of an initiative in one setting does not simply shift the problem to another. Fourth, a review should be conducted to assess the state of knowledge around initiatives that are more upstream in nature (eg, hospital admission avoidance, emergency department diversion and delivery models that proactively address the health and social care needs of individuals in community settings). Finally, there is an opportunity for future research to consider a realist review of the liter-ature on delayed hospital discharge to understand the context, mechanisms of impact, outcomes and theories of change, given that addressing a delayed discharge is a complex problem. As a first step, we sought to include
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

26 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
interventions that included hospitals, and this revealed a single sector and reactive approach to addressing delayed discharge.
LimitationsThere are a few limitations of this review that should be noted. It is possible that some relevant articles were missed because the search was limited from 1 January 2004 and 16 August 2019 and conducted in English. Our search strategy was comprehensive and we conducted an in- depth search of grey literature to minimise the poten-tial of missed articles. While we did not limit the inclusion of articles to the English language, our search strategy was in English, so there is a possibility that articles published in different languages were not identified. We excluded studies that changed the threshold/timing of discharge (early discharge), as they often focused on cost- savings. We acknowledge that some of these initiatives may have transferable lessons to address discharge delays, and thus, note their exclusion as a potential limitation of this review. Although it is not a requirement for scoping reviews,36 the interventions in this review were not criti-cally appraised, and thus, we cannot make recommenda-tions on which interventions should be scaled up. Given concerns with regression toward the mean, especially for quality improvement projects, any positive results need to be interpreted with caution. Health systems are complex, evolving environments, where various iterations of strat-egies are regularly implemented, but not necessarily formally reported or published. Future work by our team will include a process evaluation on how strategies are actually implemented in different health system contexts, as well as why they work or do not work.
Ethical considerationsThere are a few ethical concerns associated with scoping reviews to be noted. These concerns include authorship, transparency and plagiarism. All authors met the Inter-national Committee of Medical Journal Editors’ recom-mended criteria for authorship and author order was based on overall contribution to the review. We clearly outlined our methods at each stage of the scoping review to ensure transparency and replicability. We also acknowl-edged individuals who contributed to the review, but who did not warrant authorship. Lastly, when reporting the results of individual studies, we wrote them in our own words and cited appropriately to avoid plagiarism.
CONCLUSIONSThis scoping review identified a variety of initiatives addressing delayed discharges across five categories: infor-mation sharing, tools and guidelines, practice changes, infrastructure and finance and other. The majority of initiatives were focused on practice changes and many incorporated more than one category. Initiatives were often implemented in a single sector, rather than across sectors. It appears that many strategies implemented in
hospitals including communication huddles, nurse- led discharges, home first programmes and building more infrastructure had positive short- term impacts. Many initiatives that led to positive outcomes were implemented by a multidisciplinary team and included a number of components (eg, monthly reports and education). The success of these initiatives is based on a service- led defini-tion of success (effective use of hospital resources), rather than success from the patient and family perspective. This highlights the need to shift to a more patient- centred approach that focuses on improving outcomes and expe-riences, rather than system and hospital outcomes (ie, length of stay and hospital occupancy) alone. Despite the number of unique initiatives aimed at addressing delayed discharges, current strategies may not be getting at the root of the problem (initiatives/intervention prior to hospital admission) and there is a need for solutions to this problem that have a long- term and sustainable impact.
Author affiliations1Institute for Better Health, Trillium Health Partners, Mississauga, Ontario, Canada2Leslie Dan Faculty of Pharmacy, University of Toronto, Toronto, Ontario, Canada3Rehabiliation Sciences Institute, University of Toronto, Toronto, Ontario, Canada4Institute of Health Policy, Management and Evaluation, Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada5Quality Division, Ontario Health, Toronto, Ontario, Canada6Centre for Health Services and Policy Research, School of Population and Public Health, University of British Columbia, Vancouver, British Columbia, Canada7School of Social Policy, University of Birmingham, Edgbaston, Birmingham, UK8Department of Family and Community Medicine, University of Toronto, Toronto, Ontario, Canada9MAP Centre for Urban Health Solutions, St. Michael’s Hospital, Toronto, Ontario, Canada
Twitter Kristina Marie Kokorelias @kmkokorelias
Acknowledgements The authors would like to thank the University of Toronto librarian for their contribution to the search strategy, as well as Juliane Koropeski (JK) and Maliha Asif (MA) for their help screening articles. We would like to thank the involvement of our stakeholders who provided feedback on our search terms and sent us grey literature. Lastly, we would like to thank our Alternate Level of Care Advisory Council and Ida McLaughlin (chair of council) for their continual support and feedback on this programme of work.
Contributors KK, SJTG, JS, JG and TK were responsible for the conception and design of the study, as well as acquisition of funding for the study. LC, SJTG, KMK and KK led the screening of articles and the analysis and interpretation of data, but all authors contributed to the analysis and interpretation. Drafts of the manuscript were reviewed and revised by all authors. All of the authors read and approved the final manuscript.
Funding This work was supported by the Canadian Institutes of Health Research- Transitions in Care Strategic Funding Initiative on Best and Wise Practices (Grant #163064). KK holds the Dr Mathias Gysler Research Chair in Patient and Family Centred Care. SJTG and TK are funded by the Canadian Institutes of Health Research Embedded Scientist Salary Award on Transitions in Care working with Ontario Health (Quality); the award also supported staff to assist with screening.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
27Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iDsLauren Cadel http:// orcid. org/ 0000- 0001- 6925- 8163Sara J T Guilcher http:// orcid. org/ 0000- 0002- 9552- 9139
REFERENCES 1 Bate A. Delayed transfers of care in the NHS, 2017: 1–20. 2 Walker D. Caring for our aging population and addressing alternate
level of care: report submitted to the Minister of health and long- term care. Canada, 2011.
3 Rojas- García A, Turner S, Pizzo E, et al. Impact and experiences of delayed discharge: a mixed- studies systematic review. Health Expect 2018;21:41–56.
4 Barnable A, Welsh D, Lundrigan E, et al. Analysis of the influencing factors associated with being designated alternate level of care. Home Health Care Manag Pract 2015;27:3–12.
5 McCloskey R, Jarrett P, Stewart C, et al. Alternate level of care patients in hospitals: what does dementia have to do with this? Can Geriatr J 2014;17:88–94.
6 Walker H, Langton D, Thomson L. 'New to forensic'; implementing a problem- based introductory educational programme for forensic practitioners in Scotland. J Psychiatr Ment Health Nurs 2011;18:934–42.
7 Jasinarachchi KH, Ibrahim IR, Keegan BC, et al. Delayed transfer of care from NHS secondary care to primary care in England: its determinants, effect on hospital bed days, prevalence of acute medical conditions and deaths during delay, in older adults aged 65 years and over. BMC Geriatr 2009;9:4.
8 Rosman M, Rachminov O, Segal O, et al. Prolonged patients' in- hospital waiting period after discharge eligibility is associated with increased risk of infection, morbidity and mortality: a retrospective cohort analysis. BMC Health Serv Res 2015;15:246–46.
9 Everall AC, Guilcher SJT, Cadel L, et al. Patient and caregiver experience with delayed discharge from a hospital setting: a scoping review. Health Expect 2019;22:863–73.
10 Amy C, Zagorski B, Chan V, et al. Acute care alternate- level- of- care days due to delayed discharge for traumatic and non- traumatic brain injuries. Healthc Policy 2012;7:41–55.
11 Hwabejire JO, Kaafarani HMA, Imam AM, et al. Excessively long Hospital stays after trauma are not related to the severity of illness: let's aim to the right target! JAMA Surg 2013;148:956–61.
12 Challis D, Hughes J, Xie C, et al. An examination of factors influencing delayed discharge of older people from hospital. Int J Geriatr Psychiatry 2014;29:160–8.
13 Costa AP, Hirdes JP. Clinical characteristics and service needs of Alternate- Level- of- Care patients waiting for long- term care in Ontario hospitals. Healthc Policy 2010;6:32–46.
14 Costa AP, Poss JW, Peirce T, et al. Acute care inpatients with long- term delayed- discharge: evidence from a Canadian health region. BMC Health Serv Res 2012;12:172.
15 Kozyrskyi A, De Coster C, St John P. Long stay patients in Winnipeg acute care hospitals. Healthc Manage Forum 2002;Suppl:15–20.
16 Lorenzo RD, Formicola V, Carra E, et al. Risk factors for long- stay in an Italian acute psychiatric ward: a 7- year retrospective analysis. J Nurs Educ Pract 2013;4:p68.
17 Rogers A, Clark EH, Rittenhouse K, et al. Breaking down the barriers! factors contributing to barrier days in a mature trauma center. J Trauma Acute Care Surg 2014;76:191–5.
18 Mitchell F, Gilmour M, McLaren G. Hospital discharge: a descriptive study of the patient journey for frail older people with complex needs. J Integr Care 2010;18:30–6.
19 Tan WS, Chong WF, Chua KSG, et al. Factors associated with delayed discharges after inpatient stroke rehabilitation in Singapore. Ann Acad Med Singap 2010;39:435–41.
20 Landeiro F, Leal J, Gray AM. The impact of social isolation on delayed Hospital discharges of older hip fracture patients and associated costs. Osteoporos Int 2016;27:737–45.
21 Poulos CJ, Magee C, Bashford G, et al. Determining level of care appropriateness in the patient journey from acute care to rehabilitation. BMC Health Serv Res 2011;11:291–91.
22 Zeitz KM, Carter L, Robinson C. The ebbs and flows of changing acute bed capacity delays. Aust Health Rev 2013;37:66–9.
23 Anderson ME, Glasheen JJ, Anoff D, et al. Understanding predictors of prolonged hospitalizations among general medicine patients: a guide and preliminary analysis. J Hosp Med 2015;10:623–6.
24 Hendy P, Patel JH, Kordbacheh T, et al. In- depth analysis of delays to patient discharge: a metropolitan teaching hospital experience. Clin Med 2012;12:320–3.
25 Salonga- Reyes A, Scott IA. Stranded: causes and effects of discharge delays involving non- acute in- patients requiring maintenance care in a tertiary hospital general medicine service. Aust Health Review 2017;41:54–62.
26 Sutherland JM, Repin N, Crump RT. Paying for hospital services: a hard look at the options. Toronto, Canada: CD Howe Institute, 2013: 1–32.
27 Sutherland J. Hospital payment policy in Canada: options for the future. Canadian Health Services Research Foundation, 2011.
28 Ontario Ministry of Health and Long- Term Care. Quality- based procedures indicators: an implementation guidance document. Ontario, Canada, 2014: 1–38.
29 David G, Polsky D. Economics of Home Health Services. In: Culyer AJ, ed. Encyclopedia of health economics. San Diego: Elsevier, 2014: 477–83.
30 Treasury HM. Spring budget 2017. United Kingdom, 2017. 31 Knowles G, Burke MR, Carr M. Independent expert review of
delayed discharges: Department of health, 2018. 32 Fagan L. 'Bed blockers' costing Ottawa hospitals millions. Glut of
patients awaiting more appropriate care a 'crisis,' health workers say. Ottawa: CBC News, 2019.
33 McCloskey R, Jarrett P, Stewart C. The untold story of being designated an alternate level of care patient. Healthc Policy 2015;11:76–89.
34 Munn Z, Peters MDJ, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 2018;18:143.
35 Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;5:69.
36 Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA- ScR): checklist and explanation. Ann Intern Med 2018;169:467–73.
37 Bramer WM, Giustini D, de Jonge GB, et al. De- duplication of database search results for systematic reviews in endnote. J Med Libr Assoc 2016;104:240–3.
38 Babineau J. Product review: Covidence (systematic review software). J Can Health Libr Assoc 2014;35:68–71.
39 Doern GB, Phidd RW. Canadian public policy: ideas, stucture and process. 2nd. Toronto, Canada: Nelson Canada, 1992.
40 Adlington K, Brown J, Ralph L, et al. Better care: reducing length of stay and bed occupancy on an older adult psychiatric ward. BMJ Open Qual 2018;7:e000149.
41 Boyd SS. Hospital administrators' strategies for reducing delayed Hospital discharges and improving profitability. Walden Dissertations and Doctoral Studies 2017:1.
42 Caminiti C, Meschi T, Braglia L, et al. Reducing unnecessary Hospital days to improve quality of care through physician accountability: a cluster randomised trial. BMC Health Serv Res 2013;13:14.
43 Patel H, Yirdaw E, Yu A, et al. Improving early discharge using a team- based structure for discharge multidisciplinary rounds. Prof Case Manag 2019;24:83–9.
44 Ali Pirani SS. Prevention of delay in the patient discharge process: an emphasis on nurses' role. J Nurses Staff Dev 2010;26:E1–5.
45 Sutherland J, Crump R. Alternative Level of Care: Canada’s Hospital Beds, the Evidence and Options. Hcpol 2013;9:26–34.
46 Anonymous. Patient flow initiatives decrease LOS, up capacity. Hosp Case Manag 2010;18:117–24.
47 Brankline AL, Coyle CM, Jencks KA, et al. Practical innovations: technology- assisted referrals. Soc Work Health Care 2009;48:768–76.
48 Henwood M. Effective partnership working: a case study of hospital discharge. Health Soc Care Community 2006;14:400–7.
49 Maloney CG, Wolfe D, Gesteland PH, et al. A tool for improving patient discharge process and hospital communication practices: the "Patient Tracker". AMIA Annu Symp Proc 2007:493–7.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from
28 Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
50 Roberts K, Stiller K, Harling R, et al. Impacts and perceptions of a computer- based length of stay benchmarking program. Int J Ther Rehabil 2013;20:237–45.
51 Sobotka SA, Agrawal RK, Msall ME. Prolonged hospital discharge for children with technology dependency: a source of health care disparities. Pediatr Ann 2017;46:e365–70.
52 Williams TA, Leslie GD, Brearley L, et al. Discharge delay, room for improvement? Aust Crit Care 2010;23:141–9.
53 Younis J, Salerno G, Fanto D, et al. Focused preoperative patient stoma education, prior to ileostomy formation after anterior resection, contributes to a reduction in delayed discharge within the enhanced recovery programme. Int J Colorectal Dis 2012;27:1–5.
54 Chidwick P, Oliver J, Ball D, et al. Six change ideas that significantly minimize alternate level of care (alc) days in acute care hospitals. Healthc Q 2017;20:37–43.
55 Baumann M, Evans S, Perkins M, et al. Organisation and features of hospital, intermediate care and social services in English sites with low rates of delayed discharge. Health Soc Care Community 2007;15:295–305.
56 Burr E, Dickau S. Leading practices in alternate levels of care (alc) avoidance: a standardized approach. Hcq 2017;20:44–7.
57 Holland DE, Pacyna JE, Gillard KL. Tracking discharge delays: critical first step toward mitigating process Breakdowns and Inefficiencies. J Nurs Care Qual 2016;31:17–23.
58 Lian YC, Ying SHK, Peng CC, et al. Early discharge study for premature infants: Singapore General Hospital. Perm J 2008;12:15–18.
59 Mahant S, Peterson R, Campbell M, et al. Reducing inappropriate hospital use on a general pediatric inpatient unit. Pediatrics 2008;121:e1068–73.
60 Moeller JJ, Ma M, Hernandez P, et al. Discharge delay in patients with community- acquired pneumonia managed on a critical pathway. Can J Infect Dis Med Microbiol 2006;17:109–13.
61 Mur- Veeman I, Govers M. Buffer management to solve bed- blocking in the Netherlands 2000-2010. Cooperation from an integrated care chain perspective as a key success factor for managing patient flows. Int J Integr Care 2011;11:e080.
62 Niemeijer GC, Trip A, Ahaus KTB, et al. Quality in trauma care: improving the discharge procedure of patients by means of lean six sigma. J Trauma 2010;69:614–9.
63 Ardagh MW, Tonkin G, Possenniskie C. Improving acute patient flow and resolving emergency department overcrowding in New Zealand hospitals--the major challenges and the promising initiatives. N Z Med J 2011;124:64–73.
64 Brown I, Jellish WS, Kleinman B, et al. Use of postanesthesia discharge criteria to reduce discharge delays for inpatients in the postanesthesia care unit. J Clin Anesth 2008;20:175–9.
65 Gutmanis I, Speziale J, Bussel L, et al. The South West local health integration network behavioural supports Ontario experience. Hcq 2016;18:50–6.
66 Lees- Deutsch L, Jackson J, Balaji A, et al. Developing a process for Criteria- Led discharge: selection of patients for efficient and effective discharge (speed). J Nurs Care Qual 2020;35:35:140–6.
67 Toronto Central Community Care Access Centre. ALC avoidance leading practices and improvement strategies for the acute care sector. Ontario, Canada, 2015.
68 Arendts G, Fitzhardinge S, Pronk K, et al. Front- loading allied health intervention in the emergency department does not reduce length of stay for admitted older patients. Int J Clin Pract 2013;67:807–10.
69 Béland F, Bergman H, Lebel P, et al. A system of integrated care for older persons with disabilities in Canada: results from a randomized controlled trial. J Gerontol A- Biol 2006;61:367–73.
70 Blecker S, Goldfeld K, Park H, et al. Impact of an intervention to improve weekend hospital care at an academic medical center: an observational study. J Gen Intern Med 2015;30:1657–64.
71 Boutette M, Hoffer A, Plant J, et al. Establishing an integrated model of subacute care for the frail elderly. Healthc Manage Forum 2018;31:133–6.
72 Bowen A, Kumar R, Howard J, et al. Nurse led discharge: improving efficiency, safely. Clin Govern Int J 2014;19:110–6.
73 El- Eid GR, Kaddoum R, Tamim H, et al. Improving hospital discharge time: a successful implementation of six sigma methodology. Medicine 2015;94:e633.
74 Graham L, Neal CP, Garcea G, et al. Evaluation of nurse- led discharge following laparoscopic surgery. J Eval Clin Pract 2012;18:19–24.
75 Maessen JMC, Dejong CHC, Kessels AGH, et al. Length of stay: an inappropriate readout of the success of enhanced recovery programs. World J Surg 2008;32:971–5.
76 Mahto R, Venugopal H, Vibhuti VS, et al. The effectiveness of a hospital diabetes outreach service in supporting care for acutely admitted patients with diabetes. QJM 2009;102:203–7.
77 Meehan L, Banarsee R, Dunn- Toroosian V, et al. Improving outcomes for patients discharged early using a home assessment scheme. London J Prim Care 2018;10:62–7.
78 Panis LJGG, Verheggen FWSM, Pop P, et al. The impact of hospital discharge on inappropriate hospital stay. Int J Health Care Qual Assur Inc Leadersh Health Serv 2004;17:189–93.
79 Sampson MJ, Crowle T, Dhatariya K, et al. Trends in bed occupancy for inpatients with diabetes before and after the introduction of a diabetes inpatient specialist nurse service. Diabet Med 2006;23:1008–15.
80 Starr- Hemburrow L, Parks JM, Bisaillon S. Home first: reducing ALC and achieving better outcomes for seniors through inter- organizational collaboration. Healthc Q 2011;14:70–6.
81 Taber DJ, Pilch NA, McGillicuddy JW, et al. Improved patient safety and outcomes with a comprehensive interdisciplinary improvement initiative in kidney transplant recipients. Am J Med Qual 2013;28:103–12.
82 Udayai K, Kumar P. Implementing six sigma to improve hospital discharge process. Int J Pharm Sci Res 2012;3:4528–32.
83 Calveley P. Doing, not talking: hospital admission avoidance. Nursing and Residential Care 2007;9:230–2.
84 Central East LHIN ALC Task Group. Alternate level of care systems issues and recommendations. Ontario, Canada, 2008.
85 Joint Improvement Team. Home First - Ten Actions to Transform Discharge. United Kingdom, 2013.
86 Krystal A. Southlake at home Webinar. Canada, 2019. 87 LHIN Collaborative. Sharing Best Practices: Transition Management
in Ontario - Home First: Implementation Guide and Toolkit. Ontario, Canada, 2011.
88 North West Community Care Access Centre. Wait at home fact sheet. Ontario, Canada, 2011.
89 Shah N. A new philosophy towards solving the alc crisis (home first. Ontario, Canada, 2010.
90 Shah N. A call to action on ER/ALC: promoting effective care across the health continuum. Ontario, Canada, 2011.
91 Starr- Hemburrow L. Home First - Optimizing Patient Flow and Patient Centred Care Canada, 2010.
92 Province of New Brunswick. Health annual report 2016-2017. New Brunswick, Canada, 2017.
93 Behan D. Delayed transfers of care — an early review of progress. J Integr Care 2005;13:43–8.
94 Levin KA, Crighton E. Measuring the impact of step down intermediate care on delayed discharge: an interrupted time series analysis. J Epidemiol Community Health 2019;73:674–9.
95 Manville M, Klein MC, Bainbridge L. Improved outcomes for elderly patients who received care on a transitional care unit. Can Fam Physician 2014;60:e263–71.
96 Rae B, Busby W, Millard PH. Fast- tracking acute hospital care - from bed crisis to bed crisis. Aust. Health Review 2007;31:50–62.
97 Shah A. The impact of the community care (delayed discharge) act 2003 on the length of stay and bed occupancy in old age psychiatry units in England. Int J Geriatr Psychiatry 2007;22:1164–5.
98 Adams S. Care & Repair England. Reducing Delayed Transfer of Care through housing interventions: Evidence of Impact. United Kingdom, 2017.
99 Expedited discharge fund helps uninsured patients. Plan frees up beds for patients who can pay. Hosp Case Manag 2008;16:70–5.
100 Manzano- Santaella A. Payment by results and delayed discharges. Bri J Healthcare Manag 2009;15:440–3.
101 Gaughan J, Gravelle H, Siciliani L. Testing the bed- blocking hypothesis: does nursing and care home supply reduce delayed Hospital discharges? Health Econ 2015;24(Suppl 1):32–44.
102 Katsaliaki K, Brailsford S, Browning D, et al. Mapping care pathways for the elderly. J Health Organ Manag 2005;19:57–72.
103 Qin S, Thompson C, Bogomolov T, et al. Hospital occupancy and discharge strategies: a simulation- based study. Intern Med J 2017;47:894–9.
104 NHS Improvement. Guide to reducing long Hospital stays. United Kingdom, 2018.
105 Hamilton AB, Finley EP. Qualitative methods in implementation research: an introduction. Psychiatry Res 2019;280:112516.
106 Southam- Gerow MA, Dorsey S. Qualitative and mixed methods research in dissemination and implementation science: introduction to the special issue. J Clin Child Adolesc Psychol 2014;43:845–50.
107 Qualitative Research in Implementation Science group. Qualitative methods in implementation science. United States: National Cancer Institute, Division of Cancer Control and Population Sciences, 2019: 1–31.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from

29Cadel L, et al. BMJ Open 2021;11:e044291. doi:10.1136/bmjopen-2020-044291
Open access
108 Shelton RC, Cooper BR, Stirman SW. The sustainability of evidence- based interventions and practices in public health and health care. Annu Rev Public Health 2018;39:55–76.
109 Geerligs L, Rankin NM, Shepherd HL, et al. Hospital- based interventions: a systematic review of staff- reported barriers and facilitators to implementation processes. Implementation Sci 2018;13:36.
110 Green LW, Glasgow RE. Evaluating the relevance, generalization, and applicability of research: issues in external validation and translation methodology. Eval Health Prof 2006;29:126–53.
111 Balasubramanian BA, Cohen DJ, Davis MM, et al. Learning evaluation: blending quality improvement and implementation research methods to study healthcare innovations. Implementation Sci 2015;10:31.
112 Glasby J, Littlechild R, Pryce K. Show me the way to go home: a narrative review of the literature on delayed Hospital discharges and older people. Br J Soc Work 2004;34:1189–97.
113 Zhao G, Kennedy C, Mabaya G, et al. Patient engagement in the development of best practices for transitions from hospital to home: a scoping review. BMJ Open 2019;9:e029693.
on January 15, 2022 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2020-044291 on 11 February 2021. D
ownloaded from