oncology update july 2015
DESCRIPTION
ÂTRANSCRIPT

St. Francis Cancer Treatment Center
Oncology Update10I S S U E
J U L Y2 0 1 5
Dr. Dron Gauchan • Dr. Doug Clark Dr. M. Sitki Copur • Dr. Ryan Ramaekers
B r i n g i n g t h e b e s t c a n c e r c a r e t o y o u r c o m m u n i t i e s
In this issue:• CHI Health St. Francis Cancer
Treatment Center clinical trials team on the lead.
• Dr. Ryan Ramaekers of St. Francis Cancer Treatment Center namedto ASCO Workforce Advisory Group.
St. Francis at annual ASCO mee ng in Chicago
Dr. M. Sitki Copur attended the 51st annual meeting of American Society of Clinical Oncology in Chicago May 29-June 3. CIRI was also located in the exhibitor hall. The purpose for CIRI to be an exhibitor at ASCO was to make a clear commitment to the healthcare industry that CHI is a vested participant in the processes of research and innovation. The CIRI booth showcased the Center for Clinical Research (CCR) as well as the Center for Translational Research (CTR).
Rebecca Hadenfeldt, clinical research manager for CHI Health St. Francis and CHI Health Good Samaritan, was asked by CIRI to help support this booth. The administrators of CIRI were present as well and were able to make worthwhile connections with different vendors, IRBs, as well as pharmaceutical research representatives. It was very evident that CIRI is becoming a larger player in the Oncology world specifi cally with clinical trials and biospecimen research.
From left: Rebecca Hadenfeldt, Dr. M. Sitki Copur and Sydni Edwards, clinical project manager for CIRI.

Nivolumab (a programmed death 1 [PD-1] checkpoint inhibitor) and ipilimumab (a cytotoxic T-lymphocyte–associated
antigen 4 [CTLA-4] checkpoint inhibitor) have been shown to have complementary activity in metastatic melanoma. In a randomized, double-blind, phase 3 study, nivolumab alone or nivolumab plus ipilimumab was compared with ipilimumab alone in patients with metastatic melanoma. 945 previously untreated patients with unresectable stage III or IV melanoma were randomized to nivolumab alone, nivolumab plus ipilimumab, or ipilimumab alone. Progression-free survival and overall survival were coprimary end points. The median progression-free survival was 11.5 months with nivolumab plus ipilimumab, as compared with 2.9 months with ipilimumab (hazard ratio for death or disease progression, 0.42; P<0.001),
and 6.9 months with nivolumab (hazard ratio for the comparison with ipilimumab, 0.57; P<0.001). Treatment-related adverse events of grade 3 or 4 occurred in 16.3% of the patients in the nivolumab group, 55.0% of those in the nivolumab-plus-ipilimumab group, and 27.3% of those in the ipilimumab group. Among previously untreated patients with metastatic melanoma, nivolumab alone or combined with ipilimumab resulted in signifi cantly longer progression-free survival than ipilimumab alone. In patients with PD-L1–negative tumors, the combination of PD-1 and CTLA-4 blockade was more effective than either agent alone. (Check Mate Trial 067 Clinical Trials.gov number, NCT01844505.)
Reference: Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma N Eng J Med 2015; DOI: 10.1056/NEJMoa1504030.
Combined Nivolumab and Ipilimumabor Monotherapy in untreated Melanoma
A randomized, controlled trial of cavity shave margins in breast cancer
Routine resection of cavity shave margins (additional tissue circumferentially around the cavity left by partial
mastectomy) may reduce the rates of positive margins (margins positive for tumor) and reexcision among patients undergoing partial mastectomy for breast cancer. In this randomized, controlled trial, 235 patients with breast cancer of stage 0 to III who were undergoing partial mastectomy, with or without resection of selective margins were assigned in 1:1 ratio to have further cavity shave margins resected (shave group) or not to have further cavity shave margins resected (no-shave group).
Randomization occurred intraoperatively after surgeons had completed standard partial mastectomy. Positive margins were defi ned as tumor touching the edge of the specimen that was removed in the case of invasive cancer and tumor that was within 1 mm of the edge of the specimen removed in the case of ductal carcinoma in situ. The rate of positive margins was the primary outcome measure; secondary outcome measures included cosmesis and the volume of tissue resected. The median age of the patients was 61 years (range, 33 to 94). On
fi nal pathological testing, 54 patients (23%) had invasive cancer, 45 (19%) had ductal carcinoma in situ, and 125 (53%) had both; 11 patients had no further disease. The median size of the tumor in the greatest diameter was 1.1 cm (range, 0 to 6.5) in patients with invasive carcinoma and 1.0 cm (range, 0 to 9.3) in patients with ductal carcinoma in situ.
Groups were well matched at baseline with respect to demographic and clinicopathological characteristics. The rate of positive margins after partial mastectomy (before randomization) was similar in the shave group and the no-shave group (36% and 34%, respectively; P = 0.69). After randomization, patients in the shave group had a signifi cantly lower rate of positive margins than did those in the no-shave group (19% vs. 34%, P = 0.01), as well as a lower rate of second surgery for margin clearance (10% vs. 21%, P = 0.02). There was no signifi cant difference in complications between the two groups. Cavity shaving halved the rates of positive margins and reexcision among patients with partial mastectomy. (ClinicalTrials.gov number, NCT01452399.)
Reference: Chagpar AB, Killelea BK, Tsangaris TN et al. A Randomized, Controlled Trial of Cavity Shave Margins in Breast Cancer. N Eng J Med 2015; DOI: 10.1056/NEJMoa1504473.
Potentially PracticeChanging Data
Potentially PracticeChanging Data

Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer
Patients with advanced squamous-cell non–small-cell lung cancer (NSCLC) who have
disease progression during or after fi rst-line che-motherapy have limited treatment options. This randomized, open-label, international, phase 3 study evaluated the effi cacy and safety of nivolumab, a fully human IgG4 programmed death 1 (PD-1) immune-checkpoint–inhibitor antibody, as compared with docetaxel in this patient population. A total of 272 patients were randomly assigned to receive nivolumab, at a dose of 3 mg per kilogram of body weight every two weeks, or docetaxel, at a dose of 75 mg per square meter of body-surface area every 3 weeks. The primary end point was overall survival. The median overall survival was 9.2 months (7.3 to 13.3) with nivolumab versus 6.0 months (5.1 to 7.3) with docetaxel. The risk of death was 41% lower with nivolumab than with docetaxel (hazard ratio, 0.59 P<0.001). At 1 year, the overall survival rate was 42% with nivolumab versus 24% with docetaxel. The response rate was 20% with nivolumab versus 9% with docetaxel (P = 0.008).The median progression-free survival was 3.5 months with nivolumab versus 2.8 months with docetaxel. The expression of the PD-1 ligand (PD-L1) was nei-ther prognostic nor predictive of benefi t. Among patients with advanced, previously treated squa-mous-cell NSCLC, overall survival, response rate, and progression-free survival were signifi cantly better with nivolumab than with docetaxel, regard-less of PD-L1 expression level. (Check Mate 017 ClinicalTrials.gov number, NCT01642004.)
Reference: Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus Docetaxel in Advanced Squa-mous-Cell Non–Small-Cell Lung Cancer. N Eng J Med 2015; DOI: 10.1056/NEJMoa1504627.
Potentially PracticeChanging Data
Palbociclib in hormone-receptor posi ve advanced breast cancer
Growth of hormone-re-ceptor–positive breast cancer is dependent on cyclin-dependent kinases 4 and 6 (CDK4 and CDK6), which promote
progression from the G1 phase to the S phase of the cell cycle. The effi cacy of palbociclib (an inhibitor of CDK4 and CDK6) and fulvestrant in advanced breast cancer was assessed in a phase 3 study involving 521 patients with advanced hormone-receptor–positive, human epidermal growth factor receptor 2–negative breast cancer that had relapsed or progressed during prior endocrine therapy.
Patients were randomly assigned in a 2:1 ratio to receive palbociclib and fulvestrant or placebo and fulvestrant. Premenopausal or perimenopausal women also received goserelin. The primary end point was in-vestigator-assessed progression-free survival. Secondary endpoints included overall survival, objective response rate, clinical benefi t rate, patient reported outcomes, and safety. A preplanned interim analysis was performed by an independent data and safety monitoring commit-tee after 195 events of disease progression or death had occurred. The median progression-free survival was 9.2 months (7.5 to not estimable) with palbociclib–ful-vestrant and 3.8 months ( 3.5 to 5.5) with placebo–fulvestrant (hazard ratio for disease progression or death,0.42; P<0.001). The most common grade 3 or 4 adverse events in the palbociclib–fulvestrant group were neutropenia, leukopenia (25.2% vs. 0.6%), anemia (2.6% vs. 1.7%), thrombocytopenia (2.3% vs. 0%), and fatigue (2.0% vs. 1.2%). Febrile neutropenia was reported in 0.6% of palbociclib-treated patients and 0.6% of pla-cebo-treated patients. The rate of discontinuation due to adverse events was 2.6% with palbociclib and 1.7% with placebo. Among patients with hormone-receptor–positive metastatic breast cancer who had progression of disease during prior endocrine therapy, palbociclib combined with fulvestrant resulted in longer progres-sion-free survival than fulvestrant alone. (PALOMA3 ClinicalTrials.gov number, NCT01942135.)
Reference: Turner NC, Ro J, Andre F, et al. Palbociclib in Hormone-Receptor–Positive Advanced Breast Can-cer. N Eng J Med 2015; DOI: 10.1056/NEJMoa1505270.
Potentially PracticeChanging Data
Relay for Life This year the CHI Health St. Francis Cancer Treatment Center Staff teamed with the First Christian Church and the team name was “Christian Cancer Slayers,” with 30 members participating. The team had two large fundraisers throughout the winter and spring months, raising a total of $6,750 for the American Cancer Society, Hall County for 2015, this put the team in seconnd place. Thank you to all the team members!
St. Francis Cancer Treatment Center Cancer applies for teams in cancer care delivery project launched by Na onal Cancer Ins tute and American Society of Clinical Oncology (NCI-ASCO) In a joint effort, the National Cancer Institute and American Society of Clinical Oncology launched a “Teams in Cancer Care Delivery Project” with the main goal of applying the science of team-based care to oncology. Clinicians, researchers, and patients will author manuscripts and presentations involving concepts of team-based care and clinical scenarios addressing a point in the cancer continuum, evidence-based concept, and cancer type. The main purpose of this project is to bring together scientists and clinicians working on issues relevant to the effectiveness of teams involved in cancer care delivery. The project also aims to inform the research agenda for teamwork, team effectiveness, and team performance. Other goals include providing the clinical oncology community with practical strategies for how to organize effective healthcare teams, to identify areas to build the foundation for team research in cancer care delivery, such as taxonomy, operational defi nitions and measurement. St. Francis Cancer Treatment Center is applying as a team. Team members include Dr. M. Sitki Copur, Dr.
Ryan Ramaekers, Dr. Dron Gauchan, Dr. Douglas Clark, Dr. Brant Luebbe, Dr. James Omel, oncology pharmacist Angie Obermiller, genetic counselor Kimberly Brussow, clinical research manager Rebecca Hadenfeldt, oncology nurse navigator Courtney Fuller, oncology nurse manager Mary Mickey and social worker Allison Sokol. The project Timeline is as follows: June 15, 2015: Deadline for Teams Applications. July 20, 2015: Selection of teams. Aug. 28, 2015: Meeting of Teams at ASCO Headquarters in Alexandria, Virginia. Sept. 2015-Jan. 2016: Teleconferences with teams to provide monthly updates. Jan. 8, 2016: Draft manuscripts and presentations due. Feb. 25, 2016: NCI-ASCO Teams in Cancer Care Delivery Workshop. March 7, 2016: Revised manuscripts due. March 25, 2016: Final draft of manuscripts due to ASCO Staff. April 4, 2016: Deadline for submission to JOP. July 2016: Publication of manuscripts in the JOP. We have put together a great team and we are hopeful that our team will be selected.
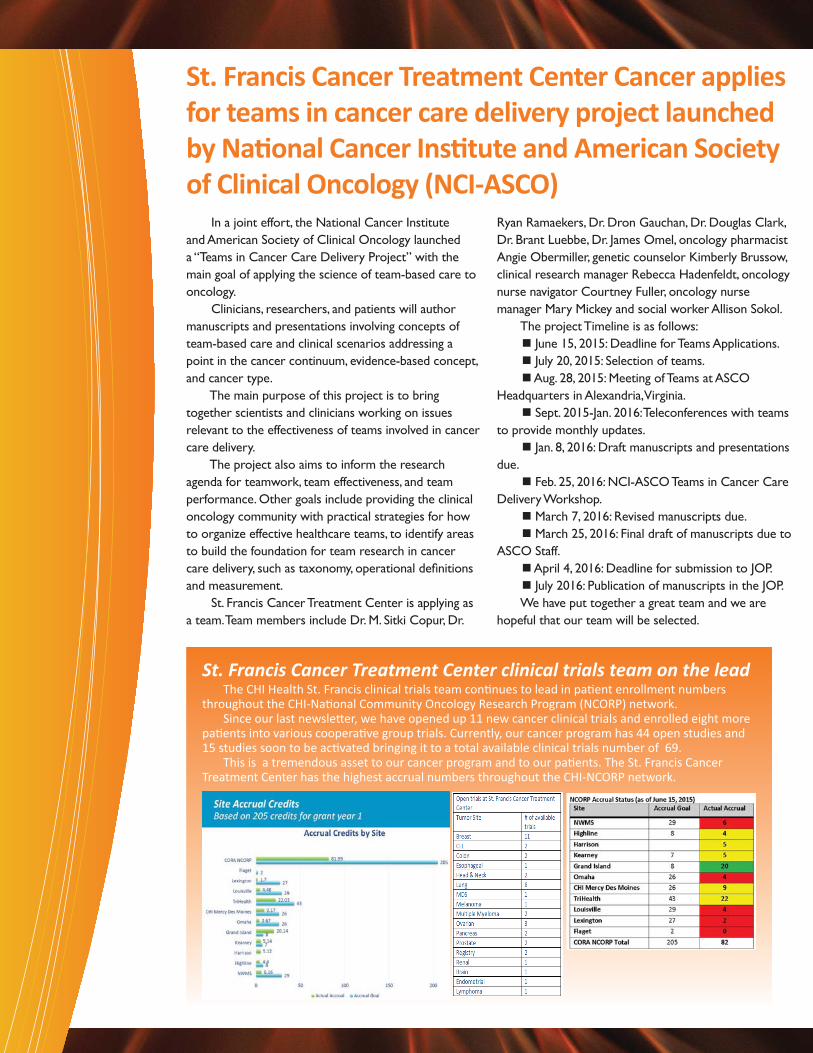
St. Francis Cancer Treatment Center clinical trials team on the lead The CHI Health St. Francis clinical trials team con nues to lead in pa ent enrollment numbers
throughout the CHI-Na onal Community Oncology Research Program (NCORP) network. Since our last newsle er, we have opened up 11 new cancer clinical trials and enrolled eight more pa ents into various coopera ve group trials. Currently, our cancer program has 44 open studies and 15 studies soon to be ac vated bringing it to a total available clinical trials number of 69. This is a tremendous asset to our cancer program and to our pa ents. The St. Francis Cancer Treatment Center has the highest accrual numbers throughout the CHI-NCORP network.

High-dose rate brachytherapy machine now in use atSt. Francis Cancer Treatment Center Radia on OncologyBy Dr. Douglas Clark
CHI Health St. Francis now has a high-dose rate
brachytherapy machine that allows patients with a variety of
cancers to complete all their necessary radiation treatment at
the St. Francis Cancer Center.
Previously, patients completing the external beam portion
of their treatment at our facility had to go to Omaha when they
needed brachytherapy treatment. Brachytherapy is a form of
radiation treatment involving radioactive sources that delivers
the bulk of radiation dose over short distances.
It enables radiation oncologists to deliver higher doses to
tumors while better sparing surrounding healthy tissue. Although
this form of treatment is new to St. Francis Cancer Center, it has
been offered elsewhere for a number of years.
Patients with several different types of cancers that may
benefi t from this new treatment modality include: women with
early stage breast cancer and women with gynecologic cancers.
Other patients with very specifi c cancer presentations may also
benefi t and consultation with one of our oncologists would be
worthwhile to determine eligibility.
Elotuzumab Therapy for Relapsed or Refractory Mul ple Myeloma Elotuzumab, an immunostimulatory monoclonal antibody targeting signaling lymphocytic activation molecule F7 (SLAMF7), showed activity in combination
with lenalidomide and dexamethasone in a phase 1b–2 study in patients with relapsed or refractory multiple myeloma. In this phase 3 study, we randomly assigned patients to receive elotuzumab plus lenalidomide and dexamethasone (elotuzumab group) or lenalidomide and dexamethasone alone (control group). Coprimary end points were progression-free survival and the overall response rate. Final results for the coprimary end points are reported on the basis of a planned interim analysis of progression-free survival. Overall, 321 patients were assigned to the elotuzumab group and 325 to the control group. After a median follow-up of 24.5 months, the rate of progression-free survival at 1 year in the elotuzumab group was 68%, as compared with 57% in the control
group; at 2 years, the rates were 41% and 27%, respectively. Median progression-free survival in the elotuzumab group was 19.4 months, versus 14.9 months in the control group P<0.001). The overall response rate in the elotuzumab group was 79%, versus 66% in the control group (P<0.001). Common grade 3 or 4 adverse events in the two groups were lymphocytopenia, neutropenia, fatigue, and pneumonia. Infusion reactions occurred in 33 patients (10%) in the elotuzumab group and were grade 1 or 2 in 29 patients. Patients with relapsed or refractory multiple myeloma who received a combination of elotuzumab, lenalidomide, and dexamethasone had a signifi cant relative reduction of 30% in the risk of disease progression or death. (ELOQUENT-2 ClinicalTrials.gov number, NCT01239797.)
Reference: Lonial S, Dimopoulos M, Palumbo A, et al. Elotuzumab Therapy for Relapsed or Refractory Multiple Myeloma. N Eng J Med 2015; DOI: 10.1056/NEJMoa1505654
Potentially PracticeChanging

FDA Hematology/Oncology Drug Approvals• Ramucirumab (CYRAMZA, Eli Lilly and Company) for use in combina on with FOLFIRI for the treatment of pa ents
with metasta c colorectal cancer (mCRC) whose disease has progressed on a fi rst line bevacizumab-, oxalipla n- and fl uoropyrimidine-containing regimen. Ramucirumab is a recombinant human monoclonal IgG1 an body that binds to the human vascular endothelial growth factor- receptor 2 (VEGF-R2), preven ng the interac on of VEGF-R2 to its ligands. April 24, 2015.
• Dinutuximab (Unituxin, United Therapeu cs Corpora on), in combina on with granulocyte-macrophage colony-s mula ng factor (GM-CSF), interleukin-2 (IL-2), and 13-cis-re noic acid (RA), for the treatment of pediatric pa ents with high-risk neuroblastoma who achieve at least a par al response to prior fi rst-line mul agent, mul modality therapy. March 10, 2015.
• Filgras m-sndz (ZARXIO Injec on, Sandoz Inc.), as a biosimilar to US-licensed Neupogen for the fi ve indica ons for which US-licensed Neupogen is approved. The formula on of ZARXIO diff ers from that of US-licensed Neupogen in one inac ve component. March 6, 2015.
• Nivolumab (OPDIVO, Bristol-Myers Squibb Company) for the treatment of pa ents with metasta c squamous non-small cell lung cancer (NSCLC) with progression on or a er pla num-based chemotherapy. March 4, 2015.
• Panobinostat (FARYDAK capsules, Novar s Pharmaceu cals) in combina on with bortezomib and dexamethasone for the treatment of pa ents with mul ple myeloma who have received at least two prior regimens, including bortezomib and an immunomodulatory agent. Feb. 23, 2015.
St. Francis Cancer Treatment Center publications/presentations Genetic counseling data 2009 through 2015 at CHI Health St. Francis Cancer Treatment Center, was presented as an e-abstract at the 51st annual meeting of American Soci-ety of Clinical Oncology, which took place May 29-June 3 in Chicago. Since our last issue, St. Francis Cancer team has had one commentary published and another one in press in the Journal of Clinical oncology. The fi rst one is titled “Cost-Effectiveness of Molecu-
lar Profi ling for early Breast Cancer” authored by Dr. Dron Gauchan, Dr. Ryan Ramaekers and Dr. M. Sitki Copur. The second one is titled “Germline BRCA ½ Mutations: Are They Good Enough to Determine Who Will Respond to Poly(ADP-Ribose) Polymerase Inhibitor Therapy in Advanced Cancer” authored by Dr. M. Sitki Copur, Dr. Dron Gauchan, Kimberly Brussow, Dr. Douglas Clark and Dr. Ryan Ramaekers. Three more other manuscripts have also been submitted which are in peer review in different journals.
Dr. M. Sitki Copur, medical oncology director at CHI Health St. Francis Cancer Treatment Center, has been invited to serve on the Special Awards Selection Committee (SASC) for a three-year term, beginning June 3, 2015. The SASC is a 13-member committee that selects the recipients of the following ASCO Special Awards: American Cancer Society Award and Lecture B.J. Kennedy Award and Lecture for Scientifi c Excel-lence in Geriatric Oncology David A. Karnofsky Memorial Award and Lecture Distinguished Achievement Award Excellence in Teaching Award Gianni Bonadonna Breast Cancer Award and Lecture Humanitarian Award
Partners in Progress Award Pediatric Oncology Award and Lecture Public Service Award Science of Oncology Award and Lecture Special Recognition Award ASCO’s Immediate Past President (which is Peter Yu, MD, FACP, FASCO, starting June 3) Chairs this committee. Dr. Ryan Ramaekers of the CHI Health St. Francis Cancer Treatment Center has been invited to serve in the ASCO Workforce Advisory Group, which collects and analyzes work-force-related data and collaborates with the ASCO Board and other ASCO committees, task forces and advisory groups to provide workforce-related perspective on ASCO programs and policy and practice development and analysis.
Copur, Ramaekers both invited toserve on special ASCO committees

Kicking the habitSt. Francis Cancer Treatment Center offers free tobacco cessation classes to its patients, and anyone in the community, who wants to quit using tobacco.
The Freedom From Smoking® program was developed by the American Lung Association, and teaches participants how to quit in a supportive setting.
The seven-week, eight-session program is lead by Cancer Treatment Center staff members Ann Tvrdy, MSN, CRNI, and Connie Hameloth, RN, who are both certified facilitators.
“Freedom From Smoking® was developed by a team of physicians, psychologists and health educators,” Hameloth said. “Over the past 25 years, it has been continually tested, updated and improved, so participants can feel confident that they are receiving the best possible assistance from a top-rated program.”
If you have a patient who is interested and could benefit from this program, please contact Ann or Connieat (308) 398-5450 for information on upcoming classes.
By Dr. M. Sitki Copur, MD, FACP
Electronic cigarettes (e-cigarettes) are devic-es that deliver vaporized nicotine to their users. Because e-cigarettes produce a vapor rather than smoke, using them is commonly called “vaping.” Most e-cigarettes consist of a rechargeable, battery-operated heating element; a replaceable or refi llable nicotine-containing cartridge; and a heater that converts the contents of the cartridge into a nicotine-containing vapor that is then inhaled by the user. Some e-cigarettes look very much like a traditional cigarette but others do not. There are more than 250 types of e-cigarettes for sale in the United States, making it diffi cult to characterize e-cigarettes as a single product. There is some agreement that, at least in short term, e-cigarettes are less harmful than regular cigarettes for their users. Regular cigarette smoke contains more than 7,000 chemicals, many of them created when tobacco is burned, while vapor from most e-cigarettes contains propylene glycol and water and a number of known/unknown fl avoring agents, and of course nicotine, “the culprit” for the addiction itself. Some e-cigarettes have been found to contain a variety of dangerous contaminants. It has been claimed and viciously marketed that secondhand e-cigarette vapor is less dangerous to bystanders than secondhand cigarette smoke; how convenient and smart to re-promote the habit of smoking as an acceptable social behavior! The sensation of using an e-cigarette (holding them in a certain way, viewing a glowing tip, blowing “smoke,” etc.) may satisfy the cravings of some smokers more completely than other nicotine replacement products such as patches or gum; again how convenient and smart to keep the addiction behavior going on and on. Contrary to the commonly held belief, e-cig-arettes are not “safe.” To start with, nicotine is a harmful and highly addictive drug that can increase the risk of a range of health and developmental issues, especially among teens and pregnant women. Tests by the US Food and Drug Administration (FDA) found that some e-cigarettes are contam-inated with dangerous chemicals, including some that can cause cancer. Simply put, until e-cigarettes are regulated, we cannot be sure of what is being inhaled. Most dangerous of all is the appeal to children. Vapor is less irritating than smoke, and comes in fl a-vors such as bubblegum, cola, and chocolate. Some children who would not try regular cigarettes will be tempted by e-cigarettes. As soon as they start, they will become addicted to nicotine and suffer
from the health effects and expense of that addic-tion. Others who start with e-cigarettes will go on to use real cigarettes, and face the deadly diseases they cause. Because they are convenient and socially acceptable, more workplaces, restaurants and other public places that have gone smoke-free in the past will now accommodate the use of e-cigarettes, de-stroying decades-long efforts to motivate smokers to quit. Once e-cigarettes become acceptable in public places, many smokers who would otherwise beat their nicotine addiction will “vape” in public places yet will continue to smoke in non-smoke free zones. It is not known whether e-cigarettes are less or more effective than current nicotine replace-ment products as quit-smoking aids. Nicotine replacement products are carefully regulated by the FDA, and the companies that make them are required to prove that they are safe and effective in helping smokers to quit. These requirements must apply to the companies that make e-cigarettes. It’s not known how many smokers who try e-ciga-rettes are able to switch completely to e-cigarettes, and how many become “dual users.” It is also not known how many kids may become addicted to the nicotine in e-cigarettes, and how many may become smokers or dual users. The best advice for smokers is to stop using any form of tobacco and/or nicotine as soon as possible. Smokers who want to quit can try stop-ping on their own with or without other guidance. They can also try one or more of the options that can help them quit, such as a telephone quitline; one or a combination of the seven FDA-approved cessation medications (fi ve nicotine replacements [gum, patch, inhaler, lozenges, and nasal spray] and two prescription medications [bupropion and varenicline]); and/or counseling from their physician, nurse, pharmacist, or other qualifi ed health care professional. St. Francis Cancer Treatment Center offers the American Lung Association’s Freedom From Smoking® program, a seven-week, eight-session class lead by Ann Tvrdy and Connie Hameloth. For more information about the program or class dates and times, please call (308) 398-5450. The toll-free Nebraska Tobacco Quitline, 1-800-QUIT-NOW (784-8669), gives Nebraska res-idents 24/7, free access to counseling and support services. Tobacco Free Hall County is also available to provide educational and prevention seminars around tobacco and nicotine in all its forms. Please contact Tobacco Free Hall County coordinator San-dy Yager at (308) 385-5520 for more information.
Debate continues on e-cigarettes

C O N TAC T I N F O R M AT I O N St. Francis Cancer Treatment Center2116 West Faidley AvenueGrand Island, NE 68803(308) 398-5450ht tp : / / c h ihea l ths t f ranc i s . o rg /
This newsletter is published by
the St. Francis Medical Center
Marketing and Communications
department. To unsubscribe,
please contact comminications
coordinator Terry Douglass
at (308) 398-6526 or
Oncology Update Issue 10 July 2015
Providers:M. Sitki Copur, MD, FACP
Medical Director of OncologyRyan Ramaekers, MDDron Gauchan, MDDoug Clark, MDDeborah Nelson, APRN, AOCNPMonica McDonald, APRNJami Kezeor, APRNMegan Schriner, PA
Clinical Trials:Sarah Einspahr, RN, OCNMary Gulzow, CRA, CCRPRebecca Hadenfeldt, BSN, CCRPJennifer Scott, BSN, OCNMaureen Thomson, RNKatherine Usasz, CRA
Center for Translational Research Alicia Wicht, CRA
Pharmacists:Angie Obermiller, PharmD
Oncology Pharmacy Supervisor
Jon Olsen, PharmD
Mark Tharnish, PharmD
Navigators:
Courtney Fuller, RN, OCN
Breast Cancer Nurse Navigator
Ashley Wissing, MA
Patient Navigator
Nutritionist
Maureen Hilderbrand, RD, LMNT
Genetic Counselor:
Kim Brussow, CGC
Tumor Registry
Leslie Mlinar, CTR
Patient & Family Counselor:
Allison Sokol, MS, LMHP
Oncology Project Coordinator
Ann Tvrdy, MSN, CRNI
Certified Tobacco Cessation Facilitator
Community Outreach Coordinator
Connie Hameloth, RN
Certified Tobacco Cessation Facilitator
Management:Max Norvell, PharmD
Director of OncologyMary Mickey, RN, OCN
Clinical Manager, Medical OncologyHeather Williams, CMD RTT (R)(T)
Clinical Manager, Radiation Therapy
Meet our team
Cancer Treatment Locations:
St. Francis Cancer Treatment Center2116 West Faidley AvenueGrand Island, NE 68803(308) 398-5450
St. Francis Cancer Treatment Center2nd Street & Marian RoadHastings, NE 68901(402) 461-5588
Visit us online:
http://chihealthstfrancis.org/
St. Francis2620 West Faidley AvenueGrand Island, NE 68803