oncology oral drug development challenges and opportunities...
TRANSCRIPT

Oncology Oral Drug Development
Challenges and Opportunities
Mark J. Ratain, MD
University of Chicago
FierceLive! Webinar
Novel Technologies to Deliver Oral
Oncology Therapies
March 29, 2016

Oncology Oral Drug Development
Challenges and Opportunities
Clin Pharmacol Ther, 2013

Russian Roulette (from wikipedia.org)
• Russian roulette is a
potentially lethal game
of chance…

Black Box Warning for Nilotinib
Tasigna® [package insert]. East Hanover, NJ. Novartis Pharmaceuticals Corp.; 2015

Center for Drug Evaluation and Research. Clinical Pharmacology and Biopharmaceutics Review(s). Application number: 22-068.
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2007/022068s000_ClinPharmR.pdf

Nilotinib labeled to be taken
fasting
Tasigna® [package insert]. East Hanover, NJ. Novartis Pharmaceuticals Corp.; 2015


In other words, if you take nilotinib
with breakfast, you might die!!!
Tasigna® [package insert]. East Hanover, NJ. Novartis Pharmaceuticals Corp.; 2015


Reddy, N, Cohen, R, Whitehead, B et al, A phase I, open-label, three period, randomized crossover study to evaluate the effect of food on the
pharmacokinetics of lapatinib in cancer patients. Clin Pharmacol Ther. 2007;81:S16–S17 (Abstract PI-15).


Median and upper ranges of plasma lapatinib concentrations versus time following a 1,500-mg dose administered after fasting overnight, after a low-fat breakfast, and after a high-fat
breakfast.
Koch K M et al. JCO 2009;27:1191-1196
©2009 by American Society of Clinical Oncology


• Compared three
prandial conditions
consistent with the
label (i.e., not within
1 hr of a meal)

Biopharmaceutics Classification System (BCS)
(from Custodio, 2008)

Most kinase inhibitors are
Class 2 compounds
• Low solubility to bind to hydrophobic
backpocket
• High permeability to reach intracellular
target
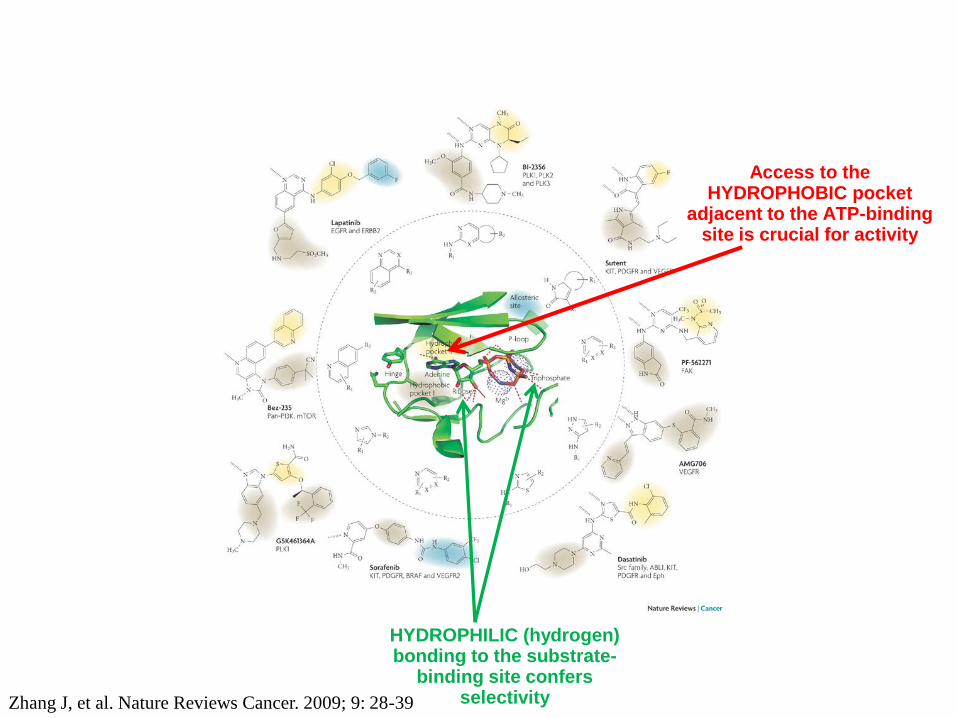
Access to the HYDROPHOBIC pocket
adjacent to the ATP-binding site is crucial for activity
HYDROPHILIC (hydrogen) bonding to the substrate-
binding site confers selectivity Zhang J, et al. Nature Reviews Cancer. 2009; 9: 28-39

CCR, 2010
Focus on 23 drugs with marked (+50%) food effect
Kang SP and Ratain MJ. Clinical Cancer Research. 2010; 16: 4446-4451.

©2010 by American Association for Cancer Research Kang SP and Ratain MJ. Clinical Cancer Research. 2010; 16: 4446-4451.
lapatinib
nilotinib
erlotinib
deferasirox
posaconazole

The value of a healthy
breakfast… Drug Estimated 2011
US monthly cost
Approximate food
effect on AUC
Monthly savings
with food
Lapatinib $3400 150% increase $2040
Nilotinib $8800 100% increase $4400
Erlotinib $4800 50% increase $1600
Pazopanib $6000 100% increase $3000
Abiraterone $5000 >300% increase $3750
Internal analysis
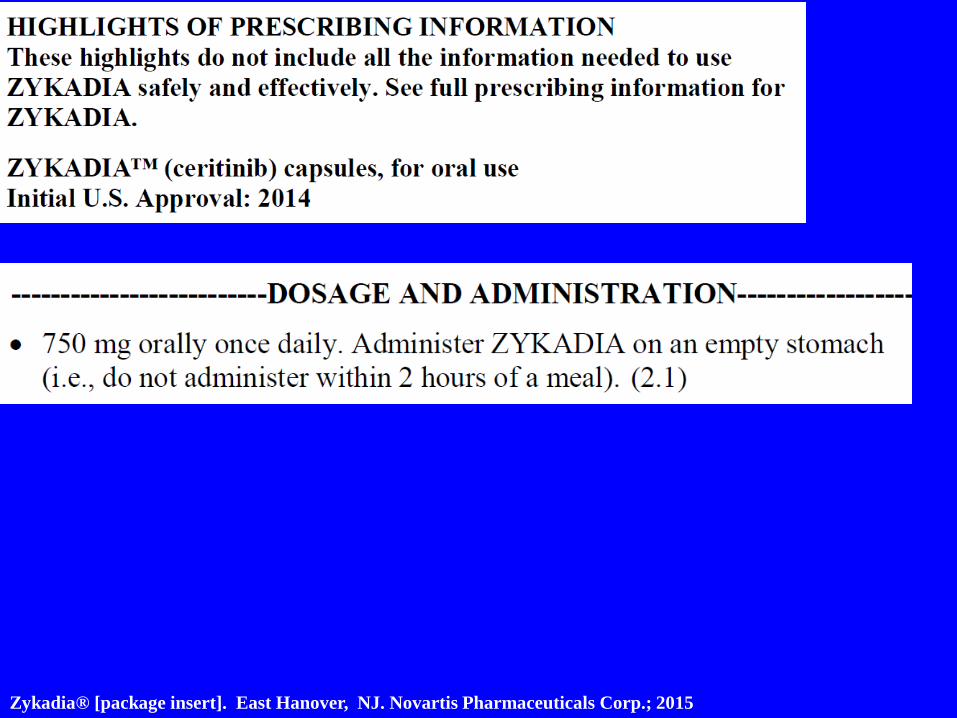
Zykadia® [package insert]. East Hanover, NJ. Novartis Pharmaceuticals Corp.; 2015

Center for Drug Evaluation and Research. Cross Discipline Team Leader Review Application number: 205755Orig1s000.
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/205755Orig1s000CrossR.pdf

Center for Drug Evaluation and Research. Summary Review. Application Number: 205755Orig1s000.
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/205755Orig1s000SumR.pdf

• 750 mg (5 CAPSULES) orally once daily on an
empty stomach (i.e., do not administer within 2
hours of a meal)
• OR 450 mg (3 CAPSULES) orally once daily
with food
???????????
Zykadia® [package insert]. East Hanover, NJ. Novartis Pharmaceuticals Corp.; 2015
Oncology Oral Drug Development
Challenges and Opportunities
• Reducing gastrointestinal toxicity
• Greatly enhancing bioavailability
• Eliminating revenue risks associated with
relabeling, if drug is initially labeled
under conditions that result in
suboptimal bioavailabity

Oncology Drug Development Challenges and Opportunities
©2016 Catalent Pharma Solutions. All rights reserved.
JEFF BROWNE
JULIEN MEISSONNIER
03.29.16

26
Class II Class I
Class IV
~35% ~30%
~25% ~10%
Class III
Source: Dr. S. Page, Roche, CRS Meeting July 12-16, 2008, NY
Class II
Class III
Class I
Class IV
~5% ~70%
~5% ~20%
1 1000000 10 100 1000 10000 100000
10
100
1
Cell
Perm
eab
ilit
y
(x1
0-6
cm
/sec)
Volume needed to dissolve anticipated dose (ml)
Compounds in Development
The Trend for Oral Cancer Drugs is Similiar to all NCE‘s... Need for Solubility Enhancing Technologies
Source: Catalent.com, Oct2014
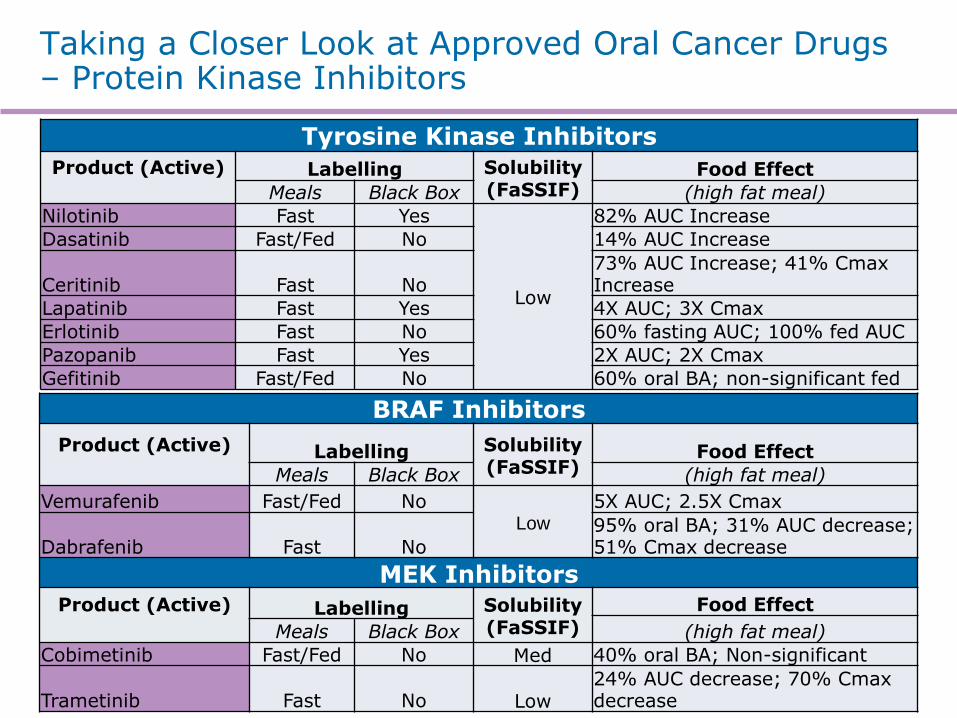
Taking a Closer Look at Approved Oral Cancer Drugs – Protein Kinase Inhibitors
Tyrosine Kinase Inhibitors
Product (Active)
Labelling Solubility (FaSSIF)
Food Effect
Meals Black Box (high fat meal)
Nilotinib Fast Yes
Low
82% AUC Increase
Dasatinib Fast/Fed No 14% AUC Increase
Ceritinib Fast No 73% AUC Increase; 41% Cmax Increase
Lapatinib Fast Yes 4X AUC; 3X Cmax
Erlotinib Fast No 60% fasting AUC; 100% fed AUC
Pazopanib Fast Yes 2X AUC; 2X Cmax
Gefitinib Fast/Fed No 60% oral BA; non-significant fed
BRAF Inhibitors
Product (Active)
Labelling Solubility (FaSSIF)
Food Effect
Meals Black Box (high fat meal)
Vemurafenib Fast/Fed No Low
5X AUC; 2.5X Cmax
Dabrafenib Fast No 95% oral BA; 31% AUC decrease; 51% Cmax decrease
MEK Inhibitors Product (Active)
Labelling Solubility
(FaSSIF)
Food Effect
(high fat meal) Meals Black Box
Cobimetinib Fast/Fed No Med 40% oral BA; Non-significant
Trametinib Fast No Low 24% AUC decrease; 70% Cmax decrease

Taking a Closer Look at Approved Oral Cancer Drugs – Other Classes of Compounds
HDAC Inhibitors
Product (Active)
Labelling Solubility (FaSSIF)
Food Effect
Meals Black Box (high fat meal)
Farydak (panobinosat)
Fast (rec) Fast/Fed Yes High
16% AUC Reduction; 44% Cmax Reduction
Farydak (panobinosat)
Mekinist (trametinib) Fast No Low 24% AUC decrease; 70% Cmax decrease
Androgen Enzyme/Receptor Inhibitors
Product (Active)
Labelling Solubility (FaSSIF)
Food Effect
Meals Black Box (high fat meal)
Enzalutamide Fast/Fed No Low
Non-significant
Abiraterone Fast No 10X AUC; 17X Cmax

Some Observations Regarding These Products
Food Effect
Most exhibit a positive food effect (AUC and Cmax)
Variability in Absorption
Safety: a number of these products have Black Box Warnings (Efficacy…exposure)
Majority are labeled to be taken fasted
Potential for poor patient compliance
- 1-2 hours before and after meals
Some are labelled simply based on administration during clinical trials
- Without regard to food
Labelled to take on empty stomach even though a clinically significant (PK) effect does not exist
80+ % Poorly Soluble Drugs

What Would an Ideal Target Product Profile for Orally Delivered Cancer Drugs Look Like?
Simple Dosing Regimen
High patient adherence
Without regard to food
Infrequent dosing… once daily
Wide Therapeutic Window
Minimal side effects
No Black Box Warnings
Less Variability Intra- and inter-patient
Consistent absorption
No Drug Interactions
Reduced transporter and metabolic effects
Target specific mechanism of action
Reduced lipophilicity

Bridging Drug Compound Properties to Formulation Approaches… Developability Classification System
Courtesy of R. Savla

32
… How does it help us select a suitable Formulation ?
We All Know The BCS But…
http://goo.gl/3v6GCq; https://goo.gl/DG0knr; https://goo.gl/6UaB59; https://goo.gl/D14HTV
Gordon’s Real BCS
Solubility High Low
Perm
eability
Hig
h
Low
Formulation Purgatory
Bioavilability Limbo

Developing a Modified Classification System
BCS – a regulatory tool
• Conservative, efficacy and patient safety in mind
— When is there no bio-inequivalence risk?
• Useful in late development and post-launch
DCS – a developability tool
• Aim: realistic, product development issues in mind
— What factors are likely to control the extent of oral absorption?
• Permeability, solubility/dose, dissolution rate
• Particularly useful in evaluating potential new drug candidates
Butler & Dressman 2010 J. Pharm. Sci. 99 (12) 4940–4954 33

BCS classification of compounds
BCS Classification
PE
RM
EA
BIL
ITY
H
L
SOLUBILITY H L
34 Source: Butler, J. The optimal use of biorelevant media & simple modeling for the prediction of in-vivo oral behaviour (http://www.apsgb.co.uk/Events/PastEvents/20110609/James%20Butler.pdf)
I
III IV
Good solubility and permeability
Good solubility Poor permeability
Poor solubility and permeability
IIa
IIb Solubility limited
Dissolution rate limited
Poor solubility Good permeability
II
DCS vs. BCS Classification of Compounds
DCS (Developability) vs. BCS Classification
Source: Dr. S. Page, Roche, CRS Meeting July 12-16, 2008, NY

Some Key Features of the DCS
Solubility limited absorbable dose (SLAD)
• Assumes a 500ml volume available for drug dissolution.
• Peff >1x10-4 cm/sec assumed to proportionally increase the effective volume available for dissolution of highly permeable drugs
• Represents the dose above which absorption is solubility limited. i.e. beyond this:
• Linear exposure/dose response may be lost
• Solubility related food effects are likely
• Reducing particle size alone cannot achieve complete absorption
Recommended particle size
• Derived from “dissolution number” equation
• Approach: set target dissolution number to 1, solve the equation for particle diameter, use this as the target x90.
Dn concept from Oh et al, Pharm Res 1993 10 (2) 264-270
35 J. Butler, 2013 Phys Chem Forum

Formulation strategies for DCS IIb compounds
PE
RM
EA
BIL
ITY
H
L
SOLUBILITY H L
I
IIa
IIb
III IV
Setting the Right Formulation Strategy for the Right Compound
36
*DCS: developability classification system
Source: Butler, J. The optimal use of biorelevant media & simple modeling for the prediction of in-vivo oral behaviour (http://www.apsgb.co.uk/Events/PastEvents/20110609/James%20Butler.pdf)
Increase Intrinsic Solubility -Lipid systems
-Solid dispersions
Increase dissolution rate -Milling
-Micronization
-Co-Micronization
Neat drug, powder in capsule/tablet
Lipid systems:w/o emulsions with permeation enhancers
Lipid systems with permeation enhancers

Solubility: Many compounds in Quadrant II!
37 J. Butler 2013 Phys Chem Forum

Why are We Still Playing Russian Roulette with Oncology Compounds…
All listed molecules are solubility limited at target dose
FeSSIF solubility drives a significant change in SLAD

Why are We Still Playing Russian Roulette with Tyrosine Kinase Inhibitors… Nilotinib
39
Weak base, highly insoluble max. dose 150-200 mg
FaSSIF solubility 0,2 µg/mL FeSSIF solubility 0,9 µg/mL
Estimated permeability 6.9 x10-4 cm/sec
BCS II, DCS IIb
Highly solubility limited
Recommended max particle size: 5 µm (d90) Solubility Limited Absorbable Dose 1 mg (FeSSIF 3 mg)
34 - 72% inter variability 31% intr variability 82 % positive food effect Marketed formulation is granulated API in capsule with poloxamer (DCS IIa option)
DCSIIb system cancel food effect (solid dispersions)

Why are We Still Playing Russian Roulette with Tyrosine Kinase Inhibitors… Erlotinib
40
Weak base, highly insoluble max. dose 150 mg
FaSSIF solubility 5 µg/mL FeSSIF solubility 200 µg/mL
Estimated permeability 7.4 x10-4 cm/sec
BCS II, DCS IIb
Solubility limited
Recommended max particle size: 20 µm (d90) – 110 µm under FeSSIF Solubility Limited Absorbable Dose: 17 mg (FeSSIF 720 mg)
60% exposure (fasted) 100% exposure (fed) Marketed formulation is API in tablet with surfactant, prescribed with an empty stomach
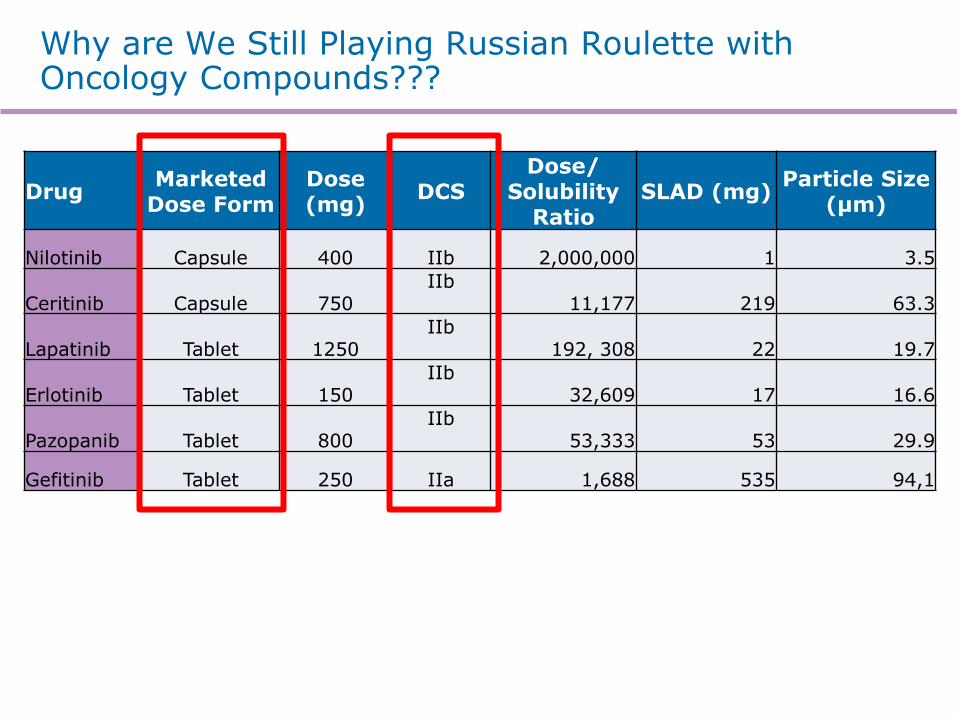
Why are We Still Playing Russian Roulette with Oncology Compounds???
Drug Marketed
Dose Form Dose (mg)
DCS Dose/
Solubility Ratio
SLAD (mg) Particle Size
(µm)
Nilotinib Capsule 400 IIb 2,000,000 1 3.5
Ceritinib Capsule 750 IIb
11,177 219 63.3
Lapatinib Tablet 1250 IIb
192, 308 22 19.7
Erlotinib Tablet 150 IIb
32,609 17 16.6
Pazopanib Tablet 800 IIb
53,333 53 29.9
Gefitinib Tablet 250 IIa 1,688 535 94,1

Marketed Protein Kinase Inhibitors Overview Formulation to Differentiate PKIs under Development
Catalent Pharma Solutions data analysis from 29 marketed PKIs, August 2015
82% low
solubility
40%
narrow therapeutic index
31%
HAVE A NON ADEQUATE DOSING
REGIMEN
78% non-
optimized DDS
22% milled
API and surfactants
7 Black Labels
42
SIMILAR PROPERTIES
SIMILAR FORMULATION RECEIPES
SUBOPTIMAL OUTCOMES

Take Abiraterone vs Enzalutamide as an example…is good enough good enough???
43
Both Compounds are Highly Similar Neutral, highly insoluble
Solubility 2 µg/mL
Estimated permeability 7,4 x10-4 cm/sec
BCS II, DCS IIb
Highly solubility limited
Recommended max particle size: 11 µm (d90) Solubility Limited Absorbable Dose: 7 mg
Enzalutamide suspension and solid form in early clinical evaluation always below lipid solutions Lipid solution removes food effect and enables linear escalation up to 600 mg
Phase I-II: Liquid filled hard gelatin capsule Market ready: Soft gelatin capsule

Zytiga® vs Xtandi® as an example…is good enough good enough???
Abiraterone acetate DCSIIa formulation
API in Tablet Formulation
− Indication: Treatment of patients with metastatic castration-resistant prostate cancer (CRPC) in combination with prednisone
− Dosage: 1,000 mg (4 X 250 mg) once daily
− Product Administration Directions: Must be taken on an empty stomach (no food at least 2 hours before and 1 hour after consumption)
− Food Effects: Approximately 17-fold and 10-fold higher, Cmax and AUC respectively, when a single dose of abiraterone acetate was administered with a high-fat (57% fat, 825 calories) meal compared to overnight fasting
Enzalutamide DCSIIb formulation
Lipid in Softgel & Spray Dried Dispersions
− Indication: Treatment of patients with metastatic castration-resistant prostate cancer (CRPC)
− Dosage: 160 mg (4 X 40 mg) once daily
− Product Administration Directions: Can be taken with or without food
− Food Effects: A high-fat meal did not alter AUC to enzalutamide or N-desmethyl enzalutamide
44

Comparability in DCSIIB Formulations Performance Rp Scherer Softgel vs Spray Dried Dispersions
45
Reference: PCT/US2013/059223

46
Fig from Porter CJH et al. , Nature Reviews | Drug Discovery, 2007, 6:231-248
Dispersion
Digestion
The rationale behind lipid-based solutions: dispersion – digestion for pre and post administration solubility
Avoid drug substance precipitation upon dispersion and digestion
Digested solution: Drug precipitation?
Fine o/w dispersion: Drug precipitation?
TG DG MG + FA
Formation of colloidal structures with endogenous biliary lipids
Digestion
Lipid Solution

Solid amorphous dispersions for DCS IIb drugs…
47
• Amorphous form of drug are high energy forms.
• Since there is no crystal lattice structure (no long range order), the energy barrier to dissolution is much reduced.
• Inherently unstable, and will tend to revert to the stable and usually least soluble form. Need to be stabilized (solid solutions, dispersions) with polymers.
— Hot Melt Extrusion and Spray Drying as processing technologies
47

DRUG DELIVERY SOLUTIONS
OPTIFORM® SOLUTION SUITE Enhanced Bioavailability in 12 Weeks
Early development followed by Phase 1 and Beyond…
1 ASSESS
2 ENHANCE
3 DELIVER
PRE-CLINICAL
Lipid Formulation
Particle Size Reduction
Solid Dispersion
• Molecule Characterization
• Assess Salt Form Benefits
• Preliminary Consultation to
select formulation technologies for ENHANCE
• Expert Consultation
• Extensive analytical data report
• 1-4 animal PK study material
1.Lipid system 2.Solid dispersion 3.Micronized Material 4.Salt Form (optional)
PHASE I & BEYOND
CU
STO
MER C
ON
DU
CTS A
NIM
AL S
TU
DIE
S
Salt Form Optimization
• Viable dose form prototypes for Phase I
• Optimized dose form development for Phase II and beyond
• CMC and Analytical
• Clinical and Commercial supply
48
Important Points to Take Home Today
1) Many of today’s oral cancer compounds fall into DCS IIb and conventional solid dose forms may not provide optimal bioavailability, i.e. poor absorption, marked food effect and significant variability
2) DCS is a valuable tool for aiding in the selection of suitable formulation strategies early in the development of these compounds
3) For DCS IIb cancer compounds, often an enabling formulation technology which allows pre-absorption drug solubility is required to assure enhanced bioavailability
4) Optiform® Solution Suite is a platform offered by Catalent incorporating 2) and 3) above which can be executed in 12 weeks or less

discover more. CATALENT PHARMA SOLUTIONS 14 SCHOOLHOUSE ROAD SOMERSET, NJ 08873
+ 1 866 720 3148
www.catalent.com