on hunger, transport costs and waiting time: challenges to arv adherence in three african countries...
TRANSCRIPT

On hunger, transport costs and waiting time: challenges to ARV adherence in
three African countries
Richard Laing, PSM/PARRobert Ogenyi, Botswana

2
Authors
Anita Hardon, Dorothy Akurut Aurugai, Christopher Comoro, Cosmas Ekezie, Henry Irunde, Trudie Gerrits, Catherine Hodgkin, Joyce Kglatwane, John Kinsman, Richard Kwasa, Janneth Maridadi, Alice Nakiyemba, Stephen E.D. Nsibmba, Robert Ogenyi, Thomas Oyabba, Florence Temu, Richard Laing

3
Overview of ART in Botswana, Tanzania, and Uganda
Country Population size
Estimated adult HIV prevalence
Number of treatment sites
Number of PLWA in need of treatment
Estimated percentage treated as of December 2005*
Botswana 1.8M 24% 32 84 000 85%
Tanzania 37 million 6.5% 44 315 000 7%
Uganda 25 million 6.7% 175 148 000 51%

4
Methods
Semi-structured interviews (SSIs) with ARV users, health workers and key informants
Focus group discussions (FGDs) with ARV users and key informants
Adherence interviews with ARV users (tools Botswana & Tanzania: two-day self-report recall, one-month visual analogue, pharmacy pill counts)
Exit interviews and observations
5
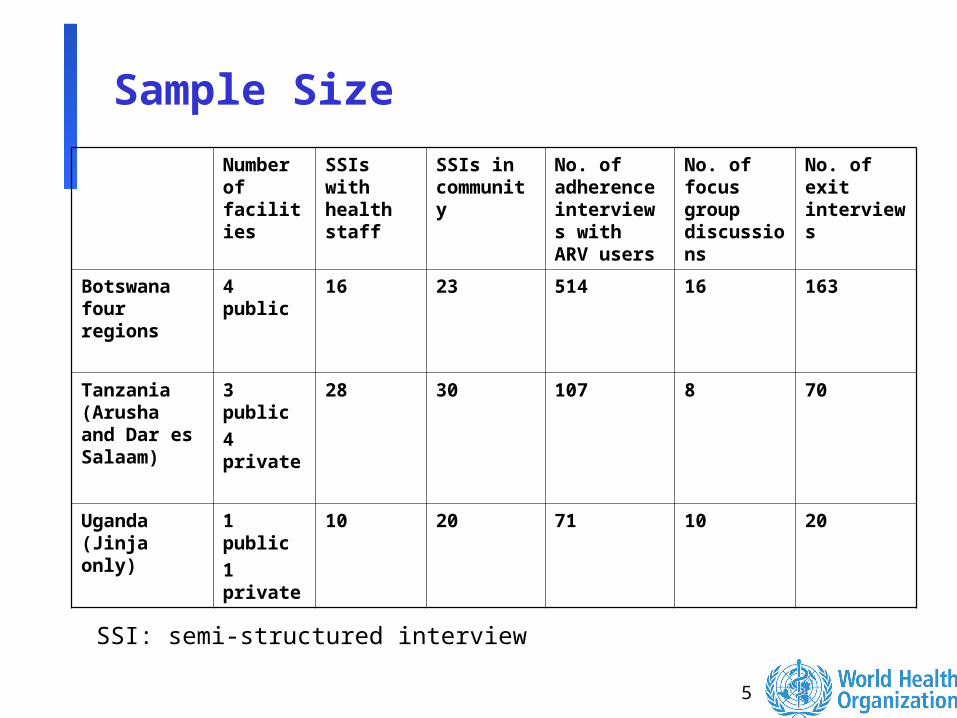
Sample Size
Number of facilities
SSIs with health staff
SSIs in community
No. of adherence interviews with ARV users
No. of focus group discussions
No. of exit interviews
Botswana four regions
4 public 16 23 514 16 163
Tanzania (Arusha and Dar es Salaam)
3 public4 private
28 30 107 8 70
Uganda (Jinja only)
1 public1 private
10 20 71 10 20
SSI: semi-structured interview

6
Quantitative results: adherence estimates
Two-day recall
One-month visual analogue
One-month pill count
Botswana 98% (n=508) 92% (n=496)
93% (n=443)
Tanzania 100% (n=107)
83% (n=107)
98% (n=107)
Average percentage of doses taken at the right time in the study population, by adherence measurement instrument

7
Quantitative results: adherence estimates – optimal level adherence 95%+
Two-day recall
One-month visual analogue
One-month pill count
Botswana 96% (n=508)
60% (n=496) 93% (n=443)
Percentage of respondents with optimal ARV adherence rates (at least 95%), by adherence measurement instrument
8
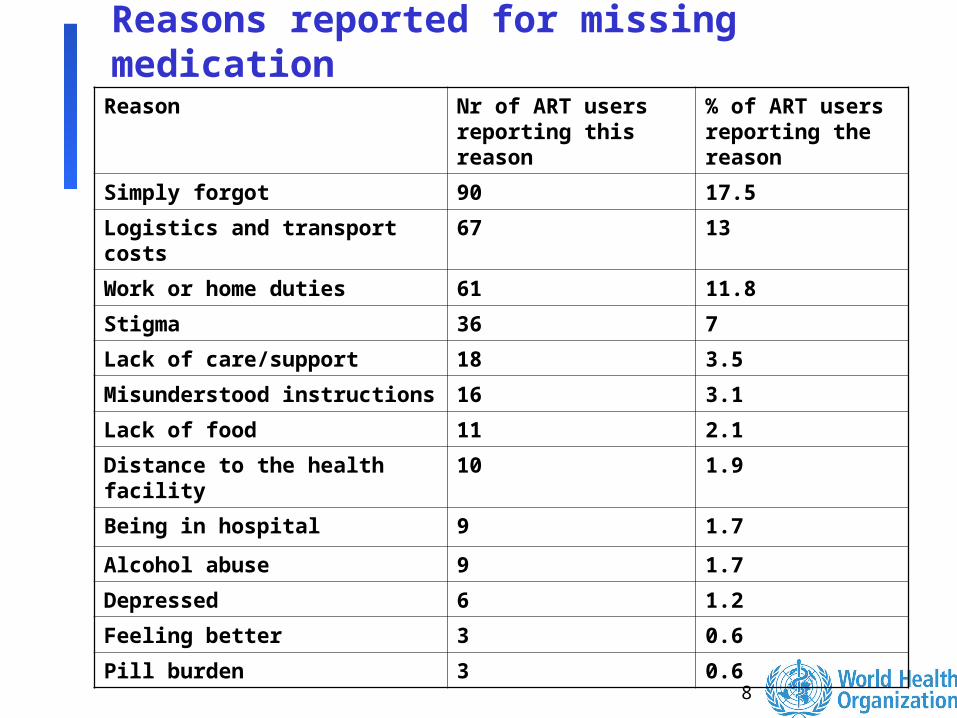
Reasons reported for missing medication
Reason Nr of ART users reporting this reason
% of ART users reporting the reason
Simply forgot 90 17.5
Logistics and transport costs
67 13
Work or home duties 61 11.8
Stigma 36 7
Lack of care/support 18 3.5
Misunderstood instructions 16 3.1
Lack of food 11 2.1
Distance to the health facility
10 1.9
Being in hospital 9 1.7
Alcohol abuse 9 1.7
Depressed 6 1.2
Feeling better 3 0.6
Pill burden 3 0.6

9
Qualitative results: what are the constraints to optimal adherence• Transport costs• User fees• Waiting times• Hunger• Stigma• Side-effects• Lack of counselling• Heavy workloads• Lack of space for confidential consultations• Lack of CD4 machines and ARV stock-outs
10
Transport costs“I have very many people in the village, they are dying because they don’t
have money to transport themselves to the hospital. You need to have this money monthly. And getting that money is a problem. So maybe, like people in Kyoga, if they can send that drug up to Kyoga, I think that could be good. Right now only Lira Referral Hospital gives ARVs, and that is 130 kilometres from our place (Kyoga). Very far!” (ARV user, Uganda)
“I once missed my appointment for refill because there were no vehicles coming here. I was in the stop from early morning and by noon I went back home. Fortunately I still had some medications.” (Male ARV user, Botswana).
“I was registered to start ART in Kilimanjaro Christian Medical Centre (KCMC) in Moshi a year ago. At that time there was no ART clinic near my village. Now there is a clinic near my home but I am denied transfer from KCMC to my home clinic. KCMC is very far from here, about 170 km away. Some times I do not have the fare to travel to KCMC, hence I miss my doses.” (Male ARV user, Tanzania).

11
Waiting times
In all three studies, the problem of long waiting times was cited as a major challenge to adherence.
In Tanzania, the mean time spent at the clinic was six hours.
In Botswana, most respondents reported that they spent around four hours at the clinic.
In Uganda, the average waiting time for ARV users was five hours in the public facility and one hour in the private facility.

12
Hunger
“The problem I have with ARVs is related to food. I have no money and ARVs increase appetite. I am not capable of buying food.” (Male ARV user, Tanzania)
“Majority of people say the ARV treatment makes them to eat a lot. They go to an extent of begging for old age pension from their grand parents. Others quit the treatment because they complain about the lack of food.” (FGD participant, Botswana)

13
Stigma
Some examples:Job loss (Tanzania)Abandonment or badly treated by partners (Botswana)Isolated by community members (Uganda)Fearing such stigmatization, ARV users often decide to hide
their HIV status.
“I cannot take my drugs when people are seeing. I always go and hide when I take them. Otherwise, people start whispering about you all the time.” (ARV user, female FGD, Uganda)
“I usually miss my medications when I visit friends because I have not told them about my HIV and so I do not want them to see my medications.” (Male ARV user, Botswana)

14
Side-effects
“I had side-effects and decided to take medication only once per day.” (Male FGD, Tanzania)
“Feeling a lot of heat in the body, especially after taking the drug and excess sweating makes one embarrassed in public. So, you feel like postponing the drug to a later time when you are not relating with people.” (Male ARV user, Uganda)

15
Lack of counselling .. And heavy workloads
“You find 25 patients and only one person attending all
these patients and he just tells you to go and collect
your medication." (Male FGD participant, Tanzania)
“You overwork like this without even a break because
there are too many people all coming one day and yet
you are very few.” (Health care worker FGD, Uganda)

16
ARV stock-outs
“We are grateful for the government for bringing medicine to the people, but we hear it is only for five years. Whenever I take these drugs, I am wondering whether in the next five years I will still have them free. Actually I get disturbed by that." (Male ARV user, FGD, Uganda)
17
Recommendations
Encourage small-scale studies using a combination of qualitative and quantitative rapid assessment tools (conducted by local researchers in collaboration with front-line health workers) to:
Estimate adherence levels Identify factors that facilitate or constrain adherence Indicate possible solutions
18
Recommendations 2
Emphasize the importance of treatment effectiveness and adherence in order to ensure sustainability of current efforts to scale up access to ART:
Provide resources for routine use of simple measures to monitor adherence
Evaluate innovative adherence support measures Scale up adherence support measures of proven
effectiveness
Key indicators to assess national programme efforts should be:
Percentage of ARV users continuing treatment after one year
Percentage of users achieving optimal adherence