omega 3’s and cardiovascular disease: high vs. low · pdf fileomega 3’s and...
TRANSCRIPT
Omega 3’s and Cardiovascular Disease: High vs. Low Dose?
Terry A. Jacobson M.D., F.N.L.A. Emory University Atlanta, GA

Structure of Omega-3 and Omega-6 Fatty Acids
Din JN et al. BMJ. 2004;328:30-35.Reprinted with permission from BMJ Publishing Group.
COOEt
Omega-6 fatty acids Omega-3 fatty acids
COOH
CH3
COOHCH3
Plant derived
C18:2n-6Linoleic acid
C18:3n-3-Linolenic acid
Marine derived
COOHCH3 C20:5n-3Eicosapentaenoic acid
COOH
CH3
C20:4n-3Arachidonic acid
COOH
CH3
C22:5n-6Docosapentaenoic acid
COOHCH3 C22:6n-3Docosahexaenoic acid

Major Dietary Sources of EPA and DHAU.S. Department of Agriculture, 2013. USDA National Nutrient Database for Standard Reference.
EPA mg/100g DHA mg/100g EPA and DHA mgAnchovy 763 1292 2055Herring, Atlantic 909 1,105 2,014Salmon, farmed 862 1,104 1,966Salmon, wild 411 1,429 1,840Mackerel, Atlantic 504 699 1,203Bluefish 323 665 988Sardines, Atlantic 473 509 982Trout 259 677 936Golden bass (tilefish) 172 733 905Swordfish 127 772 899Tuna, white (albacore) 233 629 862Mussels 276 506 782Oysters, wild 274 210 484King Mackerel 174 227 401Tuna, light (skipjack) 91 237 328Snapper 48 273 321Flounder and sole 168 132 300Clams 138 146 284Grouper 35 213 248Halibut 80 155 235Lobster 117 78 195Scallops 72 104 176Blue Crab 101 67 168Cod, Pacific 42 118 160Shrimp 50 52 102Catfish, farmed 20 69 89

Available Forms of Omega-3 Fatty Acids for Supplement and Pharmaceutical use
Harris WS and Jacobson TA. In Clinical Lipidology: A Companion to Braunwald’s Heart Disease: Expert Consult (2nd edition) Editor Christie M. Ballantyne (2014, in press)

ECLIPSE STUDY: Epanova Compared to Lovaza in a Pharmacokinetic Single-dose Evaluation
Kataoka Y et al. Future Cardiol. 2013;9:177-186

AHA Recommendations for Omega-3 FA Intake
Kris-Etherton PM et al. Circulation 2002;106:2747-2757.
Population Recommendation
Patients without documented CHD
Eat a variety of (preferably oily) fish at least twice a week. Include oils and foods rich in -linolenic acid (flaxseed, canola, and soybean oils; flaxseeds; and walnuts)
Patients with documented CHD
Consume ~1 g of EPA+DHA per day, preferably from oily fish. EPA+DHA supplements could be considered in consultation with the physician
Patients needing triglyceride lowering
2–4 grams of EPA+DHA per day provided as capsules under a physician’s care

What Percent of Whale Blubberin Maui is EPA & DHA?

n-3 Fatty Acid Randomized Controlled Trials Assessing Cardiovascular Outcomes
Trial, Year Population Interventions Compared
Duration years
Lipid Effects Endpoints RR (95% CI)
DART 1989
2,033 men with recent MI (mean 41 days)
2 servings/wk fatty fish (or fish oil capsules) vs other dietary advice
2 No change in TC IHD events Total deaths
0.84 (0.66-1.07) 0.71 (0.54-0.93)
GISSI-P 1999
11,324 men with recent MI (≤ 3 mo)
Usual care plus 882 mg/day EPA+DHA, vitamin E, both or neither
3.5 No change in TC, LDL-C or HDL-C; 5% decrease in TG
Major CV events Non-fatal events Cardiac deaths Sudden deaths
0.90 (0.82-0.99) 0.98 (0.83-1.15) 0.78 (0.65-0.92) 0.74 (0.58-0.93)
JELIS 2007
18,645 patients with total cholesterol ≥ 6.5 mmol/l (with and without CHD history)
1.8 g/day EPA vs usual care 4.6 No change in TC, LDL-C or HDL-C; 6% decrease in TG
Coronary events Non-fatal events Coronary deaths Sudden deaths
0.81 (0.69-0.95) 0.81 (0.68-0.96) 0.94 (0.57-1.56) 1.06 (0.55-2.07)
GISSI-HF 2008
6975 patients with heart failure
840 mg/day EPA+DHA vs placebo (not defined)
3.9 No change in TC, LDL-C or HDL-C; 5% decrease in TG
Total death Death or hospitalization for CVD
0.91 (0·83-0·99) 0.94 (0.89-099)
DART = Diet and Reinfarction Trial; GISSI-P = Gruppo Italiano per lo Studio della Soppravvivenza nel Infarto Miocardico –Prevenzione; JELIS = Japan EPA Lipid Intervention Study; GISSI-HF = Gruppo Italiano per lo Studio della Soppravvivenza nel Infarto Miocardico – Heart Failure
Harris WS and Jacobson TA. In Clinical Lipidology: A Companion to Braunwald’s Heart Disease: Expert Consult (2nd edition) Editor Christie M. Ballantyne (2014, in press)
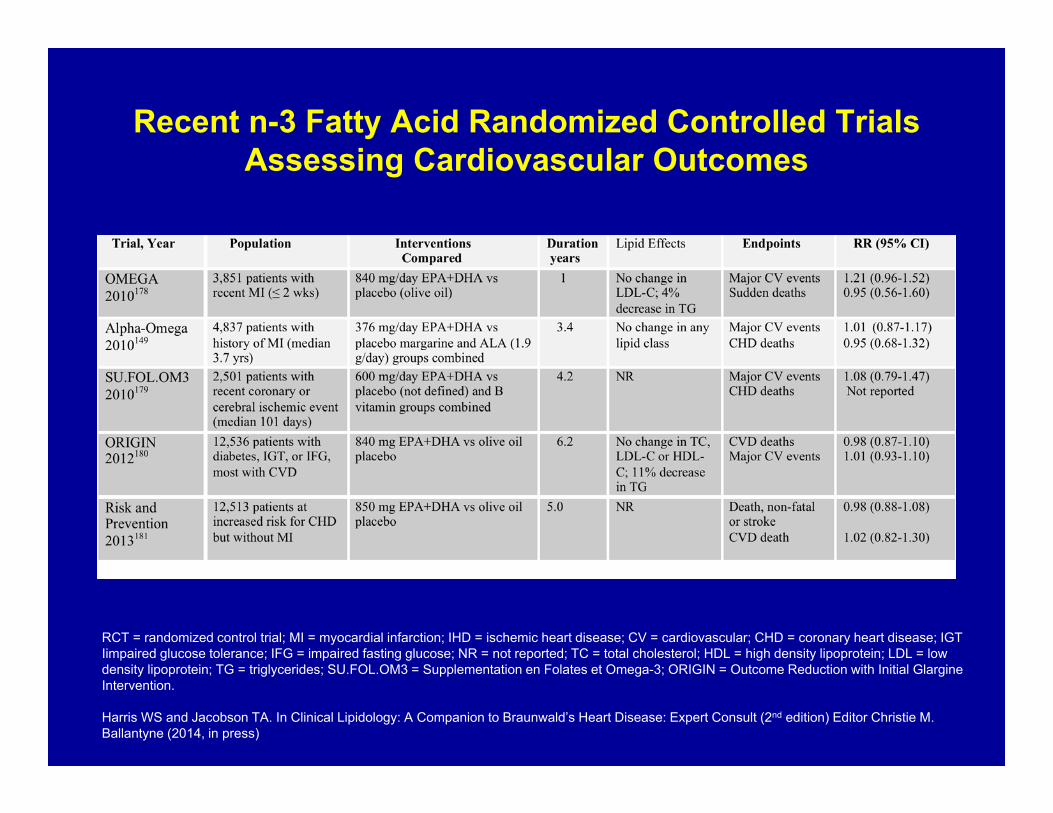
Recent n-3 Fatty Acid Randomized Controlled Trials Assessing Cardiovascular Outcomes
RCT = randomized control trial; MI = myocardial infarction; IHD = ischemic heart disease; CV = cardiovascular; CHD = coronary heart disease; IGT Iimpaired glucose tolerance; IFG = impaired fasting glucose; NR = not reported; TC = total cholesterol; HDL = high density lipoprotein; LDL = low density lipoprotein; TG = triglycerides; SU.FOL.OM3 = Supplementation en Folates et Omega-3; ORIGIN = Outcome Reduction with Initial Glargine Intervention.
Harris WS and Jacobson TA. In Clinical Lipidology: A Companion to Braunwald’s Heart Disease: Expert Consult (2nd edition) Editor Christie M. Ballantyne (2014, in press)

Association Between Omega-3 Fatty Acid Supplementation and Risk of Major Cardiovascular Disease Events: A Systematic Review and Meta-analysis (2012)
Error bars indicate 95% CIs; PUFAs, polyunsaturated fatty acids; RR, relative risk.
Rizos EC et al. JAMA. 2012;308(10):1024-1033.

Association Between Omega-3 Fatty Acid Supplementation and Risk of Major Cardiovascular Disease Events: A Systematic Review and Meta-analysis (2012)
Error bars indicate 95% CIs; PUFAs, polyunsaturated fatty acids; RR, relative risk.
Rizos EC JAMA. 2012;308(10) 1024-1033.

Are n-3 Fatty Acids Still Cardioprotective?
• Observational Studies• Mechanism of Action• Randomized Controlled Trials• Meta-Analysis• n-3 Dose: High vs. Low• Design of Future Outcome Trials

Mozaffarian, D. et al. JAMA 2006;296:1885-1899.

Are n-3 Fatty Acids Still Cardioprotective?
Mechanism of Action
1.Benefit of omega 3’s probably unrelated to changes in lipids
- no ∆ in lipids in JELIS- no ∆ in lipids in GISSI-Prevenzione- no ∆ in lipids in GISSI-Heart Failure
2. Many non-lipid mechanisms of action
3. The different cardiovascular benefits of omega 3’s aredependent on their doses, with antiarrythmic effects at low
doses, and lipid lowering effects at higher doses

Are n-3 Fatty Acids Still Cardioprotective?
Lipid Changes:
1. No evidence reducing TG’s reduces CHD or CVD events
2. High dose omega 3’s (> 2-4 grams/day) are required to change lipid levels
3. No RCT evidence yet that lipid lowering doses of omega 3’s (>2-4g/day) reduce CHD risk or have better outcomes than low doses of omega 3’s (1-2g/day).

Are n-3 Fatty Acids Still Cardioprotective?
• Observational Studies• Mechanism of Action• Randomized Controlled Trials• Meta-Analysis• n-3 Dose: High vs. Low• Design of Future Outcome Trials

Omega 35,666
The GISSI-Prevenzione TrialPost-MI
• Hard endpoints. Duration: 3.5 years (start 1993)
• 172 centers in Italy involved, managed by the Mario Negri Institute
Total Number of Patients11,324
Vitamin E2,836
Control2,830
Vitamin E2,830
Control2,828
Control5,658
1 capsule/day

Control Omega 3 RR P-Value
All-Cause Mortality 10.6% 8.4% 21% 0.0064Sudden Death 3.3% 1.8% 44% 0.0006
GISSI-Prevenzione Trial: Early Effect on All-Cause Mortality
Days
R Marchioli, et al., Circulation 2002; 105:1897-190318
Omega 3

CONFIDENTIAL
©2006

• n > 18,000 (Japan) • All administered statins• 1o & 2o prevention• 5 yr f/u• 1,800 mg EPA/day • Mean TG= 150 mg/dL
Yokoyama M et al. Lancet 2007;370:215

14,981 Primary prevention 3,664 Secondary prevention
18,645 Random allocation
7,503 EPA group
7,478 Control group
1,823 EPA group
1,841 Control group
Cohort Profile

Addition of Eicosapentaenoic Acid (EPA) to Statin Therapy in Japanese Patients
*Sudden cardiac death, fatal and non-fatal MI, unstable angina, angioplasty, stenting, or CABG.CHD=coronary heart disease; LDL-C=low-density lipoprotein cholesterol; TC=total cholesterol. Yokoyama M et al. Lancet. 2007;369:1090-8.
3.52.8
0
2
4
8
10
Statin
Major CHD Events*
Statin (n=9319)Statin + EPA 1.8 g (n=9326)
Eve
nt ra
te (%
)
Lipid Effects
TCLDL-C TG
P<0.0001
Cha
nge
from
bas
elin
e (%
)
-40
-30
-20
-10
0
10
20
19% ReductionP=0.011
6

No at RiskControlEPA
0 1 4 5 Years
9,319 8,931 8,671 8,433 8,192 7,9589,326 8,929 8,658 8,389 8,153 7,924
Cum
ulat
ive
Inci
denc
e of
Maj
or
Cor
onar
y Ev
ents
(%
)4
P=0.011
EPA
Control3
2
1
0
Hazard ratio: 0.81 (0.69-0.95)
-19%-19%
Kaplan-Meier Estimates of Major Coronary Events
↓
2 3

Major Coronary Events Incidence
No. of events (%)
ControlN=9,319
EPAN=9,326 P Value Hazard Ratio
(95% CI)
Major coronary events 324 (3.5) 262 (2.8) 0.011 0.81 (0.69-0.95)
Sudden cardiac death 17 (0.2) 18 (0.2) 0.854 1.06 (0.55-2.07)
Fatal MI 14 (0.2) 11 (0.1) 0.557 0.79 (0.36-1.74)
Nonfatal MI 83 (0.9) 62 (0.7) 0.086 0.75 (0.54-1.04)
Unstable angina 193 (2.1) 147 (1.6) 0.014 0.76 (0.62-0.95)
CABG or PTCA 222 (2.4) 191 (2.1) 0.135 0.86 (0.71-1.05)
The JELIS Study:Conclusions
• The addition of eicosapentaenoic acid (EPA) to low-dose statin therapy significantly reduced the incidence of major coronary events, largely driven by a reduction in unstable angina, when compared with patients taking statins alone
• The benefits in secondary prevention were greater than those in primary prevention

Recent n-3 Fatty Acid Randomized Controlled Trials Assessing Cardiovascular Outcomes
RCT = randomized control trial; MI = myocardial infarction; IHD = ischemic heart disease; CV = cardiovascular; CHD = coronary heart disease; IGT Iimpaired glucose tolerance; IFG = impaired fasting glucose; NR = not reported; TC = total cholesterol; HDL = high density lipoprotein; LDL = low density lipoprotein; TG = triglycerides; SU.FOL.OM3 = Supplementation en Folates et Omega-3; ORIGIN = Outcome Reduction with Initial Glargine Intervention.
Harris WS and Jacobson TA. In Clinical Lipidology: A Companion to Braunwald’s Heart Disease: Expert Consult (2nd edition) Editor Christie M. Ballantyne (2014, in press)



Are Omega’s Still Cardioprotective?:Why Current Trials Failed
• n-3 PUFA do not reduce CVD events
• n-3 PUFA have little benefit on top of aggressive medical treatments including statins, anti-platelet agents, etc.
• n-3 PUFA trials have been inadequately powered to detect a clinically meaningful effect on CHD deaths, the endpoint most likely to be effected based on both epidemiological and clinical trial data
• n-3 PUFA background therapy has increased due to increased fish consumption and greater use of fish oil supplements
• n-3 PUFA doses in clinical trials, have been too low (0.5- 1.0 g EPA and DHA) to effect long term plaque stabilization (2-4gms)
• n-3 PUFA have a limited benefit on CHD deaths after a threshold intake has been reached of ≥ 250 mg/day.

Are Omega’s Still Cardioprotective?:Why Current Trials Failed
• n-3 PUFA do not reduce CVD events
• n-3 PUFA have little benefit on top of aggressive medical treatments including statins, anti-platelet agents, etc.
• n-3 PUFA trials have been inadequately powered to detect a clinically meaningful effect on CHD deaths, the endpoint most likely to be effected based on both epidemiological and clinical trial data
• n-3 PUFA background therapy has increased due to increased fish consumption and greater use of fish oil supplements
• n-3 PUFA doses in clinical trials, have been too low (0.5- 1.0 g EPA and DHA) to effect long term plaque stabilization (2-4gms)
• n-3 PUFA have a limited benefit on CHD deaths after a threshold intake has been reached of ≥ 250 mg/day.

Are Omega’s Still Cardioprotective?:Why Current Trials Failed
• n-3 PUFA do not reduce CVD events
• n-3 PUFA have little benefit on top of aggressive medical treatments including statins, anti-platelet agents, etc.
• n-3 PUFA trials have been inadequately powered to detect a clinically meaningful effect on CHD deaths, the endpoint most likely to be effected based on both epidemiological and clinical trial data
• n-3 PUFA background therapy has increased due to increased fish consumption and greater use of fish oil supplements
• n-3 PUFA doses in clinical trials, have been too low (0.5- 1.0 g EPA and DHA) to effect long term plaque stabilization (2-4gms)
• n-3 PUFA have a limited benefit on CHD deaths after a threshold intake has been reached of ≥ 250 mg/day.

Are Omega’s Still Cardioprotective?:Why Current Trials Failed
• Populations consuming little or no fish intake have not been studied
• n-3 PUFA therapy has not been tested at doses required to significantly effect lipoproteins (triglycerides, non-HDL-C, apo B, or apo C-III)
•• n-3 PUFA therapy has not been tested in individuals with high triglycerides
or with other related lipid abnormalities (low HDL-C) despite a suggestion of potential large benefit in post-hoc analysis of randomized trials

Are n-3 Fatty Acids Still Cardioprotective?
• Observational Studies• Mechanism of Action• Randomized Controlled Trials• Meta-Analysis• n-3 Dose: High vs. Low• Design of Future Outcome Trials

JELIS: Change from Baseline in Omega 3 Fatty Acid Levels (ug/ml)
Itakura , H et al. J. Atheroscler. Thromb. 2011, 18 : 99 – 107.
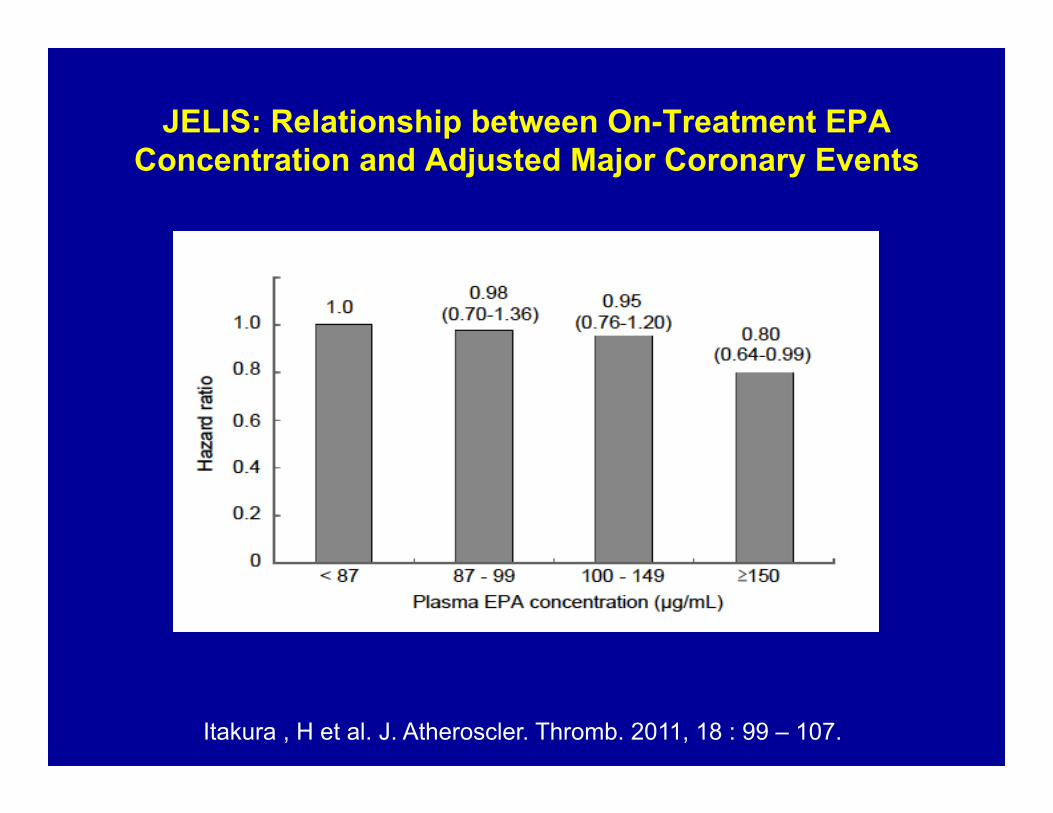
JELIS: Relationship between On-Treatment EPA Concentration and Adjusted Major Coronary Events
Itakura , H et al. J. Atheroscler. Thromb. 2011, 18 : 99 – 107.

JELIS: !
% of Patients Achieving EPA≥ 150ug/ml: Control Group (10%) vs EPA Group (61%)
Itakura , H et al. J. Atheroscler. Thromb. 2011, 18 : 99 – 107.

Are Omega’s Still Cardioprotective?:Why Current Trials Failed
• n-3 PUFA do not reduce CVD events
• n-3 PUFA have little benefit on top of aggressive medical treatments including statins, anti-platelet agents, etc.
• n-3 PUFA trials have been inadequately powered to detect a clinically meaningful effect on CHD deaths, the endpoint most likely to be effected based on both epidemiological and clinical trial data
• n-3 PUFA background therapy has increased due to increased fish consumption and greater use of fish oil supplements
• n-3 PUFA doses in clinical trials, have been too low (0.5- 1.0 g EPA and DHA) to effect long term plaque stabilization (2-4 gms)
• n-3 PUFA have a limited benefit on CHD deaths after a threshold intake has been reached of ≥ 250 mg/day.
Definition of Insanity
“Insanity” “is doing the same thing over and over again and expecting different results.”

Are n-3 Fatty Acids Still Cardioprotective?
• Observational Studies• Mechanism of Action• Randomized Controlled Trials• Meta-Analysis• n-3 Dose: High vs. Low• Design of Future Outcome Trials

Summary of Key OMEGA-3 Outcomes Studies
40
GISSI study JELIS study REDUCE‐ITPopulation Italian Japanese International
N 11,324 18,645 ~8,000
Male: Female 85% male 31% male ‐
Risk profile Recent MI (≤ 3 mths; median 16 days)
80% 1o prevention; TC ≥ 6.5 mmol/l; excluded
MI ≥ 6 months
Established vascular dxDiabetes (+)
TG 200‐499mg/dl
OM‐3 formulation & dosage Omacor 1 g/day (EPA/DHA)
Epadel 1.8 g/day (pure EPA) EPA‐E 4 g/day
Follow‐up 3.5 years 4.6 years 4‐5 years
Statin use 4.7% baseline/45.5% at end
All on Low Dose Background Statins
All on Background Statins(LDL‐C goal)
Endpoint Death, non‐fatal MI, stroke MACE MACE
Result RRR 10%/15% (2‐ or 4‐way analysis) RRR 19% Powered for 15% RRR
LDL‐C Increased ~3% > control groups
No DifferenceBetween both groups ‐‐
SCD RR = 0.74/0.55 RR= 1.06 ‐‐

Summary: Are n-3 Fatty Acids Still Cardioprotective?
• Although recent n-3 fatty acid intervention studies have not demonstrated a beneficial effect on total cardiovascular outcomes, the totality of evidence suggests that CHD mortality is reduced at a low doses
• Properly designed clinical trials are needed assessing populations with low background n-3 fatty acid intake and using higher n-3 fatty acid doses (2-4gms) to either affect lipids or other mechanisms involved in plaque stabilization
• The risk-benefit ratio of n-3 fatty acids for reducing risk for cardiovascular disease still remains favorable in the right patient at the right dose.