oculosystemic disease essentials - illinois college of ... · oculosystemic disease essentials...
TRANSCRIPT
8/23/14
1
Oculosystemic Disease Essentials
Steven Ferrucci, OD, FAAO Chief, Sepulveda VA
Professor, MBKU/SCCO
Disclosures
! Speakers bureau and/or Advisory Board for: ! Alcon ! Autogneomics ! Macula Risk ! MacuLogix ! Nicox ! Science-Based Health ! ThromboGenics
What is diabetes?
• DM is a chronic disorder characterized by a lack of insulin or increased resistance to insulin
• Insulin is needed for proper uptake of glucose
• Clinical result is hyperglycemia – retinopathy – nephropathy – neuropathy
Statistics
• Approximately 23.6 million Americans with diabetes
• ≈8.3% of total population • 11.3 % of adults • 25-30% undiagnosed ( 7 million)
• Another 79 million Americans have pre-diabetes and are likely to develop diabetes if do not change habits – 35% of adults age 20 or older
Statistics, cont.
• Globally, Type 2 DM affects 5.9% of adult population – 46% ages 40-59
• Highest percentage in Eastern Mediterranean and Middle East (9.2%) and North America (8.4%)
• Total Numbers: 246 million Worldwide – India 40.9 million – China 39.8 million – Then USA, Russia, Germany, Japan, Pakistan, Brazil,
Mexico and Egypt
Statistics
! In 2007, medical expenditures for diabetes $116 billion ! $27 B direct care ! $58 B to treat diabetes related complications ! $31 B in excess general medical costs ! Costs: 2.3 x higher in diabetic vs non-diabetic pt
! Actual national burden of diabetes likely exceeds $174 B when indirect costs considered
! Seventh leading cause of death in 2006

8/23/14
2
The Diabetes Epidemic
• Incidence has increased 13.5% from 2005, and over 700% in last 40 years
• WHY??
The Diabetes Epidemic • Improvements in diabetes care
– Pts living longer with diabetes
• Growth in elderly populations: – 10% > 60 vs 16-20% > 80
• Increasing prevalence of obesity which causes increased insulin resistance
• Increased number or minority populations in US – Rates of DM among minority populations are often 2-3
times greater
TYPE 1
• Formerly IDDM or juvenile onset
• Prevalence: 0.2%
• 10% of all DM
• Most common age of onset < 30
• Destruction of insulin producing B-cells in pancreas (auto-immune? viral?)
• Total lack of endogenous insulin
• Need to be on insulin to survive
TYPE 2
• Formerly NIDDM or adult onset
• Prevalence: 3.1%
• 90% of all DM
• Most frequent age of onset > 40
• Often asymptomatic
• Characterized by insulin resistance
• Strong genetic predisposition
Gestational Diabetes
• Affects 4% of all pregnancies
• High risk populations: – Pregnant woman greater than age 25 – Abnormal body weight – Have first degree relatives with diabetes – Hispanic, Asian, Native American , African American
descent
• Screen in 24th to 28th week of pregnancy
Gestational Diabetes • Plasma glucose concentration at or above any 2 of
4 values on OGTT – 1. Fasting, 95 mg/dL – 2. 1 hour, 180 mg/dL – 3. 2 hour, 155 mg/dL – 4. 3 hour, 140 mg/dL
• May be treated with diet changes or insulin if needed
• At higher risk for developing type 2 later in life – 5 fold increase at 5 yrs, 9 fold after 5 years
8/23/14
3
Pre-Diabetes ! Blood sugar levels higher than normal, but not yet
high enough to be diagnosed with DM ! FBS: 100-126 mg/dl ! A1c: 5.7-6.4
! ADA estimates 79 million Americans have pre-diabetes ! 30 minutes of exercise combined with 5-10%
reduction in body weight resulted in 58% reduction in diabetes
Symptoms
• Often asymptomatic, especially Type 2
• Classic symptoms – polydipsia – polyphagia – polyurea
• Others: weight loss, delayed wound healing, dry mouth, dry skin, recurrent infections, refractive changes
Risk Factors • Family history
• Specific ethnic backgrounds – African Americans – Native Americans – Hispanic – Asian American – Pacific islander
• Sedentary Lifestyle
• Pertinent medical history – obesity – cardiovascular disease – HTN – High cholesterol – Polycystic ovarian syndrome – Psychiatric illness – Gestational DM – IFG/IGT
Traditional Diagnosis Criteria
• Fasting blood glucose > 126 mg/dL
• OGTT > 200 mg/dL (2 hour sample)
• Any random testing >200 mg/dl should be referred for further testing
• Random testing > 200 mg/dL with symptoms very suggestive of DM
New Diagnosis Criteria ! Panel of “experts” at ADA annual meeting are
recommending A1C be used for diagnosis of diabetes
! Glycosolated hemoglobin
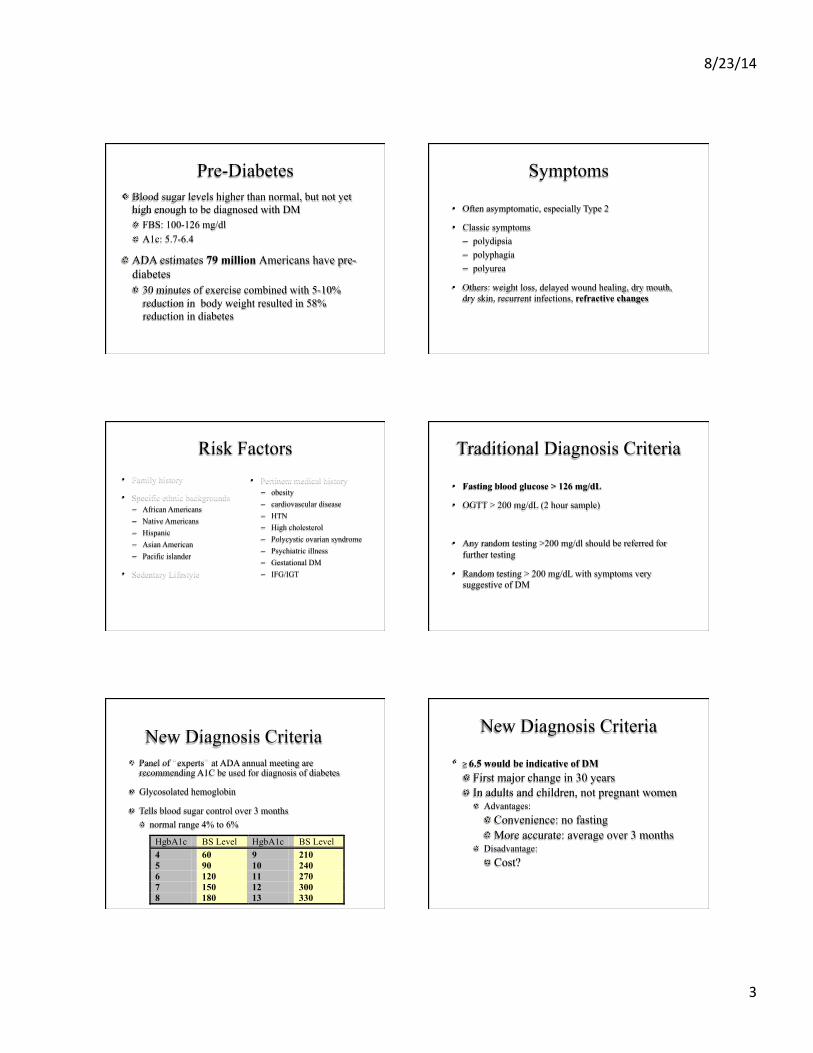
! Tells blood sugar control over 3 months ! normal range 4% to 6%
HgbA1c BS Level HgbA1c BS Level 4 60 9 210 5 90 10 240 6 120 11 270 7 150 12 300 8 180 13 330
New Diagnosis Criteria
! ≥ 6.5 would be indicative of DM ! First major change in 30 years ! In adults and children, not pregnant women ! Advantages: ! Convenience: no fasting ! More accurate: average over 3 months
! Disadvantage: ! Cost?

8/23/14
4
Recommended Criteria for Screening Asymptomatic Individuals for Type 2 DM
• All pts >45 yrs at 3 yr intervals
• Younger age or more frequently in pts who: – are obese – have a first-degree relative with diabetes – are members of high-risk ethnic population – gestational diabetes or delivered a baby > 9 lbs – are hypertensive – HDL < 35mg/dl or triglycerides > 250 mg/dl – have impaired glucose regulation
Treatment of Type 2 DM
! Goal: to produce desirable blood glucose levels with minimal adverse effects and maximal patient compliance
! Treatment begins with diet and exercise and ends with insulin
! Often, adequate control can be achieved with oral agents ! If not, insulin is utilized
Medical Management
! Sulfonylureas (glyburide, glipizide) ! Often first line
! Low cost, low side effects
! Metformin (glucophage) ! First line/Second line to sulfonylureas or in combo
! Glitazones (Avandia, Actos) ! NEJM May, June 2007: Avandia has an increased cardiovascular risk ! FDA Sept 2010: US patients can only take if unable to control blood sugar
with any other drug ! If already on drug, must sign statement that they understand
risks if wish to continue
Medical Management
! Aplha-glucosidase inhibitors ! Acarbose (Precose) and Miglitol (Glyset) ! Used alone or in combo with sulfonylureas
! Meglitinides ! Repaglanide (Prandin) and Nateglinide (Starlix) ! Best used to control mealtime glucose
! DPP-4 Inhibitors ! Sitagliptin (Januvia) and Saxagliptin (Onglyza) ! Relatively new class of meds ! Only lower BS if levels are elevated
Medical Management
! Exenatide (Byetta) ! Injectable drug used to treat Type 2 DM
! Pramlintide Acetate (Symlin) ! Used as injection in Type 1 or Type 2 DM in conjunction with
mealtime insulin
! Liraglutide (Victoza) ! Once daily injected medication for tx of type 2 DM
! FDA Approved January 2010
Newest meds
! Alogliptin ( Nesina, Takeda Pharmaceuticals) ! DPP-4 Inhibitor
! FDA approved January 2013
! 14 clinical trials; 8,500 patients ! Safe and effective
! Reduced HbA1c at 6 mos by 0.4-0.6 points
! Kazano=alogliptin and metformin
! Oseni=alogliptin and pioglitazone
8/23/14
5
Medical Management
! Insulin ! Replaces natural insulin in body ! Used with type 2 patients who do not respond to oral agents
! Long acting Insulins ! Glargine (Lantus) and Detemir (Levemir) ! Last 24 hrs with no peak ! More expensive than traditional insulin
! Inhaled insulin ! FDA approved Jan 2006 (Exubera by Pfizer) ! Removed from market 2010
! Poor sales? ! Lung CA?
! Afreeza (MannKind)
Current recommendations for Treatment of Type 2 DM
• Control BS: HgbA1c < 7
• Control HTN: <120/80
• Control Cholesterol levels: Total cholesterol < 200
• No smoking
• Exercise
• Normal BMI
• Yearly foot exams, dental exams, and dilated retinal exams
Diabetic Retinopathy
• Leading cause of blindness 20-74 year old
• 8-12% of all new cases of legal blindness
• 50,000 Americans legally blind
• Early diagnosis and treatment can decrease vision loss by 50-60%
• Factors which influence development of DR – duration of disease – control of BS
Diabetic Retinopathy
• Duration of Disease: Type 2 – <10 years 1% – 11-13 years 23% – > 16 years 60%
• Control of BS (UKPDS) – for every 1% decrease in HgbA1C there is a 35%
reduction in risk for retinopathy
Diabetic Retinopathy
• Non-proliferative Diabetic Retinopathy (NPDR) – mild – moderate – severe – very severe
• Proliferative Diabetic Retinopathy (PDR) – Including high-risk
Mild NPDR
! Microaneurysms (ma)
! Dot/blot hemorrhages
! Follow Up: 1 year
8/23/14
6
Moderate NPDR
! Marked hemorrhages/ma
! Cotton wool spots (CWS)
! Venous beading (VB)
! Intra-retinal microvascular abnormalities to mild degree (IRMA’s)
! Follow up: 6 months
Severe/ Very Severe NPDR
! 4-2-1 Rule: ! Marked hemes/ma in all 4 quadrants ! VB in 2 or more quadrants ! Marked IRMA’s in one quadrant
! Very severe: 2 of the 3 above criteria
! Follow-up: 3-4 mos or refer to Retinal specialist
Proliferative Diabetic Retinopathy (PDR) • Hallmark is retinal neovascularization
– response to ischemia from capillary closure – new vessels are fragile and easily rupture
• Neo divided into 2 categories – NVD: on or within 2 DD of optic disc – NVE: neovascularization elsewhere
– Follow-up: Retinal consult within 2 weeks
High Risk PDR
! NVD >1/4 to 1/3 disc area
! Any NVD with a PRH or VH
! Moderate to severe NVE with VH or PRH
! Poses very high risk of severe VH and vision loss within 2 years
! Follow-up: Retinal specialist 24-48 hrs
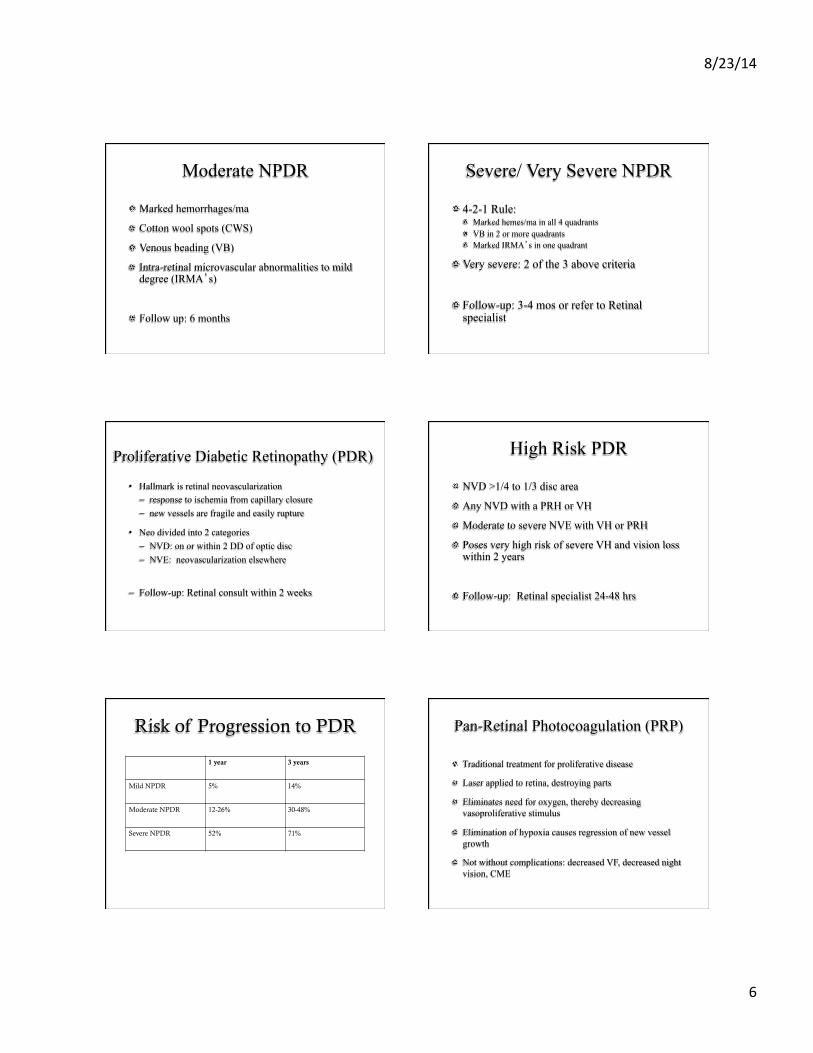
Risk of Progression to PDR
1 year 3 years
Mild NPDR 5% 14%
Moderate NPDR 12-26% 30-48%
Severe NPDR 52% 71%
Pan-Retinal Photocoagulation (PRP)
! Traditional treatment for proliferative disease
! Laser applied to retina, destroying parts
! Eliminates need for oxygen, thereby decreasing vasoproliferative stimulus
! Elimination of hypoxia causes regression of new vessel growth
! Not without complications: decreased VF, decreased night vision, CME
8/23/14
7
ETDRS and DRS
! Proved benefit of immediate PRP ! Showed an overall reduction rate of severe vision loss
(ie 5/200) of approximately 50% in treated vs. untreated eyes ! <4% chance of severe vision loss in 5 years w/ tx
! PRP in 2 to 3 sessions (1200-1600 spots)
! Treat CSME first, if present
Clinically Significant Macular Edema(CSME)
! Characteristics ! retinal thickening at or within 500 microns (1/3 DD) of
center of macula ! hard exudates at or within 1/3 DD if associated with
thickening of adjacent retina ! thickening greater than 1 DD in size part of which is
within 1 DD of center of macular
! May occur at any stage of retinopathy
! Treatment: retinal consult within 2 weeks
CSME
! Level of Retinopathy ! mild NPDR 3%
incidence of DME ! moderate to severe
NPDR 40% ! Proliferative 71%
! Type 2: Duration and Insulin ! no insulin ! 10 years 5% ! 20 years 15%
! on insulin ! 10 years 10% ! 20 years 30-35%
Focal Macular Laser (FML)
! Standard Treatment for CSME
! ETDRS: proved benefit of FML in improving vision
! Reduces the risk of moderate vision loss (doubling of the visual angle) from 30% to less than 15% ! so 50% reduction in MVL after 3 years
! Real goal is to prevent further loss, not to improve vision
Anti-Vegf
! RISE/RIDE studies ! Pts with DME received intravitreal Lucentis
0.3 mg or 0.5 mg monthly for 2 years ! 33.6% of pts receiving 0.3 mg gained > 15 letters
! 45.7% of pts receiving 0.5 mg gained > 15 letters
! Only 12.3% in placebo group gained > 15 letters
! 3-4 fold increases in treated patients
What is Hypertension?
! Systolic BP > 140 or
! Diastolic BP > 90
! Affects ≈ 70 million Americans
! Essential HTN
! Malignant HTN
! Secondary HTN
SYSTOLIC DIASTOLIC Normal <120 <80 Pre-hypertension
120-139 80-89
Stage 1 hypertension
140-159 90-99
Stage 2 hypertension
>160 >100

8/23/14
8
Essential HTN: >140/90
! Most common type of HTN ! 90-95%
! Family History common
! Risk Factors include: ! Sedentary lifestyle, smoking , stress, alcohol intake, obesity,
high sodium intake, vitamin D deficiency, aging
! Usually controlled with 1 or 2 oral meds
Secondary HTN
! By definition results from an identifiable cause ! Cushings Syndrome
! Hypo/hyperthyroidism
! Kidney disease
! Pregnancy (pre-eclampsia)
! Coarctation of the aorta ! Certain prescription and illegal dugs
Malignant HTN: BP>210/130
! Ocular findings ! Papillidema
! Exudates
! CWS
! FSH
! AV changes
! Systemic Findings ! None
! HA’s
! Vomiting
! Coma
Malignant HTN
! Immediate referral for BP lowering ! ER or PCP
! MRI to r/o space occupying lesion
! MRA to r/o “venous sinus thrombus’
! LP if needed
Malignant HTN
! 80% of patients with malignant HTN die within 1 year
! 95% mortality within 3 years
Hypertension
! Other Complications ! Retinopathy ! Left ventricular Hypertrophy ! Angina ! Myocardial infarction ! Heart Failure ! Stroke ! Peripheral vascular disease ! Chronic kidney disease
8/23/14
9
Hypertension
! Risk ! Each increase of 20 mmHg systolic or 10 mmHg
diastolic doubles risk of complications
! Risk reduction with treatment ! 35-40% reduction in stroke ! 20-25% reduction in myocardial infarction ! >50% reduction in heart failure
Hypertension Treatment
! Lifestyle ! Weight reduction
! BMI goal 18.5-25
! Diet ! Sodium restriction ! DASH diet
! Dietary Approaches to Stop Hypertension
! Physical activity ! Moderation of alcohol consumption
DASH Diet
! Dietary Approaches to Stop Hypertension ! Proven to lower BP in as little as 14 days
! Best with moderate or less or pre-hypertension
! Includes whole grains, poultry, fish, and nuts and has reduced amounts of fats, red meats, sweets, and sugared beverages.
! www.dashdiet.org
Hypertension Treatment ! Medical management ! Thiazide diuretics (hydrochlorothiazide)
! Work by helping body reduce sodium and water thereby decreasing blood volume
! Beta blockers (atenolol) ! Reduce workload on heart, causing decreased heart rate
! Angiotensin-converting enzyme (ACE) inhibitors (lisinopril, captopril) ! Help relax blood vessels by blocking the formation of enzymes
which narrow blood vessels
Hypertension Treatment ! Medical management, cont ! Angiotensin II receptor blockers (losartan)
! Relax blood vessels by blocking action of the enzymes which narrow blood vessels
! Calcium Channel Blockers (verapamil, diltiazem) ! Help relax the smooth muscles of the arteries and heart, thereby
decreasing blood pressure
! Renin inhibitors (aliskiren) ! Newer drug which works on renin, an enzyme produced in the
kidneys which starts hypertensive cascade
Hypertensive Retinopathy
! Pts with HTN retinopathy suffer (obviously) from systemic HTN
! However, at times, this may be first clue to pts underlying disease
! Pts are almost always asymptomatic, unless they have rare finding of edema or papilladema, which would cause decreased acuity
8/23/14
10
Hypertensive Retinopathy
! Typically pts with HTN retinopathy are middle aged or older ! HTN more common in middle aged men than
women ! But more common in elderly woman than elderly
men
! Much more prevalent in African-Americans than Caucasians
Hypertensive Retinopathy
! Clinical findings include ! Retinal artery narrowing and attenuation ! Retinal artery nicking and crossing changes ! Flame shaped hemes ! Cotton wool spots ! Rarely retinal or macula edema ! May have macular star
! Disc edema
Hypertensive Retinopathy ! Keith Wagner Baker
Classification System ! Grade 1 Hypertensive
Retinopathy ! Retinal arterial narrowing
and straightening
! Grade 2 ! AV Nicking
Hypertensive Retinopathy ! Keith Wagner Baker
Classification System ! Grade 3
! Retinal hemorrhages ! Cotton wool spots ! Hard exudates
! Macular star
! Grade 4 ! Grade 3 with ONH
edema
Hypertensive Retinopathy
! Rare to have either macula edema or optic disc edema unless there is malignant HTN, where BP is elevated in 250/130 range ! However presentation of macular star and disc
edema is almost pathognomonic for HTN crisis
! CWS typically do not appear until diastolic BP is > 110
Hypertensive Retinopathy
! Monitor fundus q 12 months ! Sooner if severe
! Pt education
! Management involves appropriate tx of underlying HTN, with referral to primary care physician or internist
! If papilledema from HTN, consider medical emergency!! ! Immediate referral and/or trip to ER!!

8/23/14
11
Retinal Plaques
! Several different types of plaques can often be visualized in the retinal vasculature
! Pt is typically elderly, has HTN, CAD, hypercholesterolemia/hyperlipidemia, and/or atherosclerotic disease
! Often totally asymptomatic and found on routine exam
Retinal Plaques ! May present with amarosis fugax, transient episodes of
monocular blindness
! Rarely, may report transient ischemic attack (TIA) , which is above with hemiparesis, parasthesia or aphasia
! Three different types of plaques, but all share strong association to significant cardiovascular disease
Retinal Plaques
! Cholesterol (Hollenhorst) plaque ! shiny yellow-orange in appearance ! typically from the ipsilateral carotid artery ! Rarely causes occlusion, unless multiple ! Typically occurs at bifurcations ! Mobile in nature
Retinal Plaques
! Calcific ! Appears more whitish than HH ! Classically within arteriole, not at bifurcation ! Typically immobile ! Often causes BRAO ! Often from cardiac arethromas of heart valves
Retinal Plaques
! Fibrino-platelet ! Appear as dull white to gray, long plugs ! Typically within arterioles, not at bifurcations ! May break-up and dissolve with time ! May lead to BRAO or CRAO ! Often associated with carotid disease or mitral valve
insufficiency
Retinal plaques
! No direct management of plaques is needed
! Management is aimed at discovering source of embolus to decrease risk of other emboli, occlusion, or stroke
! Pts need referral to internist for complete physical
8/23/14
12
Retinal Plaques
! Examination should include ! Complete physical, including cardiac risk factors and BP
evaluation ! Carotid ultrasound ! Stress echocardiogram ! Fasting BS ! Lipid profiles ! Cardiac enzymes
Retinal Plaques
! After ruling out underlying etiology, see patient regularly, q 6 -12 mos, to evaluate for additional plaques or other disease associated with vascular disease ! BRVO/CRVO ! BRAO/CRAO ! NTG
Retinal Plaques
! If carotid stenosis or coronary artery disease is found treatment may include ! Carotid endarterectomy ! Angioplasty ! Aspirin therapy ! Other anti-coagulation therapy, such as coumadin
! Pts with cholesterol HH emboli have 15% mortality at 1 yr, 29% by year 3, and 54% by 7 years ! Mostly from cardiac disease
Hyperlipidemia ! Elevation of lipids in the bloodstream ! Cholesterol and triglycerides are most commonly
affected ! High lipids causes accelerated atherosclerosis
(hardening of the arteries) ! Increased risk of plaque formation, heart disease, stroke, and
other vascular disease
! Can be genetic, but most often affected by lifestyle ! Obesity, sedentary lifestyle, smoking ! Also associated with diabetes, kidney disease, pregnancy, and
hypo-thyroidism
Hyperlipidemia
! Diagnosis ! Fasting Lipid Profile
! Total Cholesterol ! LDL (low-density lipoproteins)
! high levels associated with increased heart attack ! HDL (high-density lipoproteins)
! protective against heart attack ! Triglycerides ! Total Chol/HDL ratio
Hyperlipidemia
! Total cholesterol ! < 200 desirable ! 200-239 borderline high ! > 240 high
! HDL (“good” cholesterol) ! < 40 for men and < 50 for women is low ! > 60 considered protective for heart disease
! LDL (“bad” cholesterol) ! <100 desirable ! 100-129 borderline ! 130-159 borderline high ! >160 high
8/23/14
13
Hyperlipidemia
! Triglycerides ! < 150 is desirable ! 150-199 borderline high ! > 200 is high
! Total chol/HDL ! 3.5:1 is optimal ! Below 5:1 is acceptable ! Above 5:1 unhealthy
Hyperlipidemia
! National Cholesterol Education Program (NCEO) recommends cholesterol screenings for: ! Males and females > 20 every 5 yrs ! More often if risk factors
! Diabetes ! Obesity ! Family history ! > 65 years of age
Hyperlipidemia
! Treatment ! Exercise ! Weight loss ! Elimination of trans-fats ! Increase omega-3’s ! Identify and treat other risk factors
! Hypertension ! Diabetes
! Smoking cessation
What is Obesity?
! Increased body weight caused by excessive accumulation of fat
! BMI defined as patient’s weight (kg) divided by height (m2) ! BMI categories of obesity
! Normal 20-24.9 ! Overweight 25-29.9 ! Obesity 30-34.9 ! Moderate obesity 35-39.9 ! Extreme obesity over 40
BMI 25 - 29.9 = Overweight
BMI > 30 Obese
BMI > 40 Morbidly Obese
BMI > 50 Super Morbidly Obese
What is Obesity?
BMI = Weight in Kg
(Height in Meters)2
Body Mass Index
8/23/14
14
BMI Table Statistics
! 1/3 of US adults are obese
! 1 in 6 US children is overweight
! #2 modifiable risk factor for death (tobacco)
! May result in reduced life expectancy for the 1st time in 200 years! ! Obese patients have 6.7 years less life expectancy than
non-obese patients ! New England Journal of Medicine
! 300,000 Deaths Each Year (Directly Related)
Obesity: Ocular Complications
! AMD
! Diabetic retinopathy
! Cataract
! Pseudotumor cerebri (papilledema)
! Floppy lid syndrome
! Ocular hypertension
! Exophthalmos/proptosis
Obesity: Systemic Complications
! HTN
! Dyslipidemia
! Type 2 DM
! CAD
! Stroke
! Gall bladder disease
! Osteoarthritis
! Malignancies
Other Scary Stuff
! 165 Million Americans will be obese by 2030 ! ½ of all American men will be obese by 2030 ! US healthcare spending expected to increase $66
Billion per year by 2030 if this trend continues ! 165 million obese Americans would correlate to an
additional 8 million cases of DM, 6.8 million cases of heart disease and stroke, and 0.5 million cases of cancer
! A 1% reduction in BMI would prevent as many as 2.4 million cases of DM and 1.7 million cases of heart disease and stroke