objectives - richiebrace.com · payne cb: the past, present, and future of podiatric biomechanic s....
TRANSCRIPT
1
THE NEWBIOMECHANICS
VS.THE OLD ROOT
THEORY
DOUGLAS H. RICHIE JR., DPMSEAL BEACH, CA
www.SealBeachPodiatry.comNEW YORKPodiatric Clinical Conference
SponsorParis Orthotics
www.ParisOrthotics.com
OBJECTIVES
1. Review pertinent clinical concepts of Root Theory
2. Present new, conflicting experimental evidence
3. Propose clinical applications of thesenew insights
“It behooves the podiatry profession to first of all establish a common nomenclature which is specific in its meaning so that knowledge can be accurately transmitted. Secondly, the foot must be classified as to its various functional and structural types, with specific clinical methods for measurement and evaluation so that one foot type at a time can be given detailed study to further our knowledge of the problems we face.”
Merton L. Root, 1963
Criticisms of the Root Theory
7. Static measures = dynamic function
McPoil and Hunt 1995, Michaud 1997, Keenan 1997, Levitz and Sobel 1997, 1998, Payne 1997, 1998.
1. Reliability of clinical measurements2. Dynamic subtalar joint position3. Criteria for normalcy
4. Single axis model
5. Frontal plane rearfoot motion significance
6. Kinematic patterns of RF motion

2
Criteria for a “Normal Foot”
“In the individual with normal lower extremities, the following conditions exist during normal static stance upon a level surfac e (ground).
I. The legs in the sagittal bisection of the calcanei are perpendicular to the ground (vertical) and parallel to each other in both extremities.
II. Thesubtalar joints of both feet are positioned at their neutral positions.
III. The midtarsal joints are locked in their fully pronated positions.
IV. The full plantar surface of the forefoot of each foot rests upon the ground, all metatarsals bear weight, and the plantar surface of the forefoot parallels the plantar surface of the heel.”
Root, ML, Orien, WP, Weed, JH: Clinical Biomechanics: Normal and Abnormal Function of the Foot, Vol 2. Los Angeles, Clinical Biomechanics Corp, 1977.
“There is also no evidence that the posterior bisection of the calcaneus is perpendicular to the plantar surface of the calcaneus, which is used as the reference plane for the frontal-plane forefoot deformity.”
Payne CB: The past, present, and future of podiatric biomechanics. JAPMA 88:53, 1998
KINETICS
KINEMATICS
Forces acting on a body part
Timing and movement of a body part
Kinematics of Rearfoot Motion

3
“As the midstanceperiod begins, the leg begins to externally rotate and the subtalar joint begins to supinate.”
Root, ML, Orien, WP, Weed, JH: Clinical Biomechanics: Normal and Abnormal Function of the Foot, Vol 2. Los Angeles, Clinical Biomechanics Corp, 1977.
“Just before the end of the midstanceperiod, subtalar joint supinationmoves the foot into a slightly supinated position.”
“Pronation of the foot is abnormal if the amount of pronation, during any period of locomotion, becomes excessive or if any pronationoccurs at a time when the foot should be supinating.”
“When treating the foot, the objective of functional orthopedic therapy is to reestablish normal motion and position of the footduring the stance phase of gait.”
“Abnormal compensatory pronation of the foot is the most common cause of pathology within the foot.”
Root, ML, Orien, WP, Weed, JH: Clinical Biomechanics: Normal and Abnormal Function of the Foot, Vol 2. Los Angeles, Clinical Biomechanics Corp, 1977.
“Abnormal pronation of the foot is defined as abnormal pronation of the entire foot which occurs at the subtalar joint. Abnormal pronationof the foot usually refers only to abnormal subtalar joint pronation, but, rarely, abnormal ankle joint pronation may also be included.”
“Normal” Rearfoot Motion
2 opposing views
1. Achieves neutral position beforeheel off
2. Remains at resting position untilheel off
Root, et al
McPoil & Cornwall, 1994Pierrynowski & Smith, 1996
Mosseley, 1996Liu, 1997
Rearfoot angle vs RCSP
Should We Control Calcaneal Eversion?
When does STJ achieve neutral?
CONTROVERSIES
ControversyRoot et al.:
• RCSP & NCSPcalcaneus to ground
Others:• Rearfoot angle calcaneus to leg
Figure A & B: The resting calcaneal stance position is determined by measuring the posterior biscetion line of the heel to the ground with the foot relaxed.

4
Fig. 3. A plot of the mean pattern of rearfoot motion as well as the mean angles for RSFP and SJNP for the 100 feet. The two unmarked lines represent plus or minus on standard deviation from the mean pattern of rearfoot motion.
NCSP
RCSP
Subtalar Neutral = Normal?
• Nine subjects
• Three dimensional treadmill analysis
• Max eversion at 44% of gait cycle
• Neutral STJ position at 66% and 74% ofgait cycle
Pierrynowski, M.R., Smith, S.B.: Rear foot inversion/eversion during gait relative to the subtalar joint neutral position. Foot and Ankle 17: 406, 1996
Subtalar Joint
When does pronation end and supination begin?
McPoil and Cornwall 1994
• 36% of gait cycle
• 44% of gait cycle
Pierrynowski, 1996
What initiates supination?
Independent JointsIndependent Axes
Figure A, B. The subtalar joint is moved to its end range of inversion (A) and eversion. (B)Motion and excursion values are recorded.
A B

5
Figure 1-33:From the neutral subtalar joint position this foot inverts 20°when the subtalar joint is fully supinated and everts 10°when the subtalar joint is fully pronated. This foot has a normal rearfoot, and its full range of subtalar joint motion, measured in a frontal plane, is 30°.
§ 15 cadaveric legs
§ Unlocked vs locked tibiotalar joint
§ Manual vs radiographic measurments
Taylor, K.F., Bojescul, J.A., Howard, R.S., Mizel , M.S., McHale, K.A., Measurement of Isolated Subtalar Range of Motion: A Cadaver Study. Foot and Ankle Intl 22:426-432, 2001
Clinical MeasurementCalcaneal Inversion - Eversion
“This study demonstrates that the clinical measurements of calcaneal eversion and inversion did not correlate well with radiographic measurements.”
“The contribution of the tibiotalar joint to apparent subtalar motion, as measured clinically and radiographically, was found to be one-third of the arc of motion.”
Clinical MeasurementCalcaneal Inversion - Eversion
Taylor, K.F., Bojescul, J.A., Howard, R.S., Mizel , M.S., McHale, K.A., Measurement of Isolated Subtalar Range of Motion: A Cadaver Study. Foot and Ankle Intl 22:426-432, 2001
Axis of Motion of the Pedal Joints
Fact vs. Fiction
“In this model, the subtalar and midtarsal joints have been described as dual screws connected to the talonavicular joint in opposite directions. This model introduced the concept of the position of the subtalar joint.
The range of motion of the midtarsal joint is controlled by subtalar joint position. In a pronated subtalar joint, the two axes of the midtarsal joint are in a more parallel orientation, increasing the range of motion. In a supinatedsubtalar joint, the two axes of the midtarsal joint are in a more oblique orientation, decreasing the range of motion.”
- Justin Wernick- Russell G. Volpe
Valmassy , R: Clinical Biomechanics of the Lower Extremities. St. Louis, Mosby-Year Book, Inc. 1996

6
Bi-axial Model of MTJ
Van Langelaan
Benink
Lundberg
(1983)
(1985)
(1989)
Refuted by:
Independence vs Interdependence of joint movements
Should We Control Calcaneal Eversion?
When does STJ achieve neutral?
Rearfoot angle vs RCSP
CONTROVERSIES
Huson A: Biomechanics of the tarsal mechanism. A key to the function of the normal human foot. JAPMA 90:12, 2000.
“The tarsal bones together form an articulated ring of bones. The talus articulates with the calcaneus, the calcaneus with the cuboid, the cuboid with the navicular, and the navicular with the talus: a so-called kinematic chain with only 1 kinematic degree of freedom. Under weightbearing conditions, this kinematic chain acts as a mechanism in engineering terms, if a motion is imposed upon one of the links, the other links are also forced to move.”
Figure 1. An osteoligamentous dissected specimen of the foot exarticulated at the ankle joint. The dorsal capsules of the talonavicular and calcaneocuboid joints have been removed. The foot is held in the neutral position corresponding with upright standing.
Figure 2. The talus has been moved as it does in supination of the foot while the calcaneus, cuboid, and navicular are kept immobile. The talar head has left the navicular socket laterally, creating a wide gap at the medial side of the talonavicular joint. Huson A: Biomechanics of the tarsal mechanism. A key to the function of the
normal human foot. JAPMA 90:12, 2000.
“Because of the complex mechanical relationships between the tarsal motions and between these and other complex motions in the tarso-metatarsal joints, the use of axes of rotation as tools for a reliable quantitative clinical evaluation of foot function has no firm basis so far.

7
HINGE AXIS?
VanLangelaan E.J. A Kinematical Analysis of the Tarsal Joints. Acta Orthop Scand 54: 204, 1983
Lundberg et al. Kinematics of the Ankle / Foot Complex: Plantarflexion and Dorsiflexion. Foot and Ankle 9: 194, 1989
Singh A.K. : Kinematrics of the Ankle : A HinjeAxis Model. Foot & Ankle 13:439, 1992
• Six cadaver specimens• Axis-finder rod• LED path photography• MRI serial cuts• Single axis, at tips of malleoli

8

9
Traditional Biomechanical Exam
• Static Measurements
• Open Kinetic Chain
• Calcaneus is Point of Reference
“The assessment of the range of motion of the subtalarjoint is done in a non-weightbearing position, but there is a difference between the weightbearing and non-weightbearing range of excursion of the calcaneus in the frontal plane, indicating motion in the joint.
Static measurements are used as part of the biomechanical assessment of patients, but in light of these reports and other work on the reliability of the measurements, their usefulness must be reconsidered.”
Payne CB: The past, present, and future of podiatric biomechanics. JAPMA 88:53, 1998
Figure A: With the patient standing in the angle and base of gait and the subtalar joint held in its neutral position, the angle of the bisection of the lower leg relative to the ground determines the tibial position.
AFigure A & B: The resting calcaneal stance position is determined by measuring the posterior biscetion line of the heel to the ground with the foot relaxed.

10
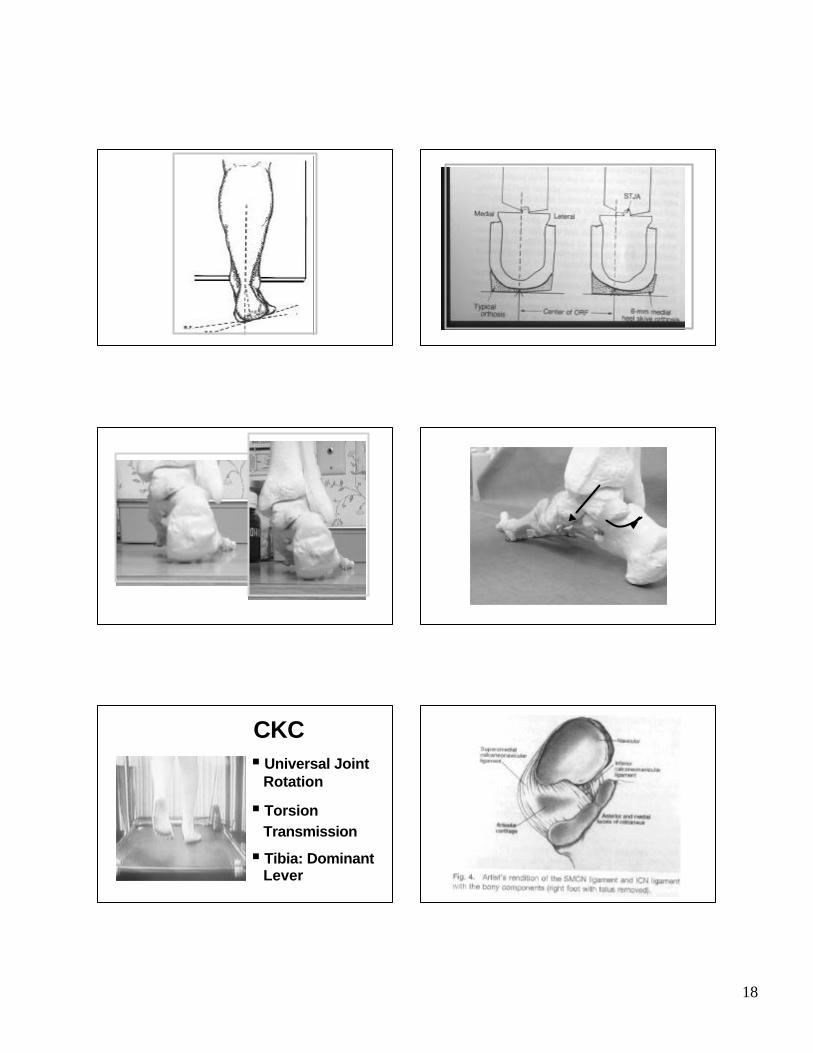
• PT Tendon removed
• Spring ligament removed
CKC§ Universal Joint
Rotation
§ Torsion Transmission
§ Tibia: Dominant Lever
• PT Tendon removed
• Spring ligament removed
The Myth of the Subtalar Joint
Importance of STJ control of LE
CONTROVERSIES
Should We Control Calcaneal Eversion?
When does STJ achieve neutral?
Rearfoot angle vs RCSPIndependence vs Interdependence of joint movements

11
Calcaneus = Subtalar Joint = Foot
3 Myths of Podiatric Biomechanics
1. The calcaneus controls the subtalar joint
2. The subtalar joint controls the foot
3. The foot controls the leg
“Frontal plane movement of the calcaneus has been the primary indicator for measurement of foot pronation in studies on foot orthoses, while control of excessive foot pronation has been the primary objective in the prescription of functional foot orthoses.”
- William R. Olson
Valmassy , R: Clinical Biomechanics of the Lower Extremities. St. Louis, Mosby-Year Book, Inc. 1996
Figure 1-44: Closed chain pronation of the subtalar joint.
Pronation of the subtalar joint in the weight bearing foot results in eversion of the calcaneus , and the talus adducts and plantarflexes relative to the calcaneus . The leg follows the talus in a transverse plane and internally rotates. In a sagittal plane, the leg also moves to some extent with the talus. As the talus plantarflexes , the proximal aspect of the tibia moves forward to flex the knee slightly.
“One method of estimation of correction for the severe pronator is the “5-to-1 rule” Five degrees of plaster correction produces 1º of calcaneal inversion (rearfootchange). Measurement of the patient presents with an RCSP of 10º everted on the involved left side. Utilizing the 5 to 1 rule in an attempt to bring the rearfoot back to a vertical position, a 50 degree inverted orthotic correction should be ordered.”
- Richard Blake
Valmassy , R: Clinical Biomechanics of the Lower Extremities. St. Louis, Mosby-Year Book, Inc. 1996

12
Controlling Calcaneal Eversion Effects of Functional Foot Orthoses
AUTHORDECREASED
EVERSION
Clarke et al.CavanaghRogers et alSmith et alTaunton et alSims
2.5º2º per 6mm wedge
1-2º1.2º1-2º2º
“Simms and Cavanagh noted that although studies have claimed that foot and ankle symptoms are usually dramatically decreased with the use of foot orthoses, the objective improvement in rearfoot motion is considerably more modest, suggesting that therapeutic success is not necessarily due to restoring the foot to what is functionally considered “normal.” This raises the possibility that foot orthoses are effective for reasons that are not entirely clear.”
Payne CB: The past, present, and future of podiatric biomechanics. JAPMA 88:53, 1998
“Variation in the spatial location of the subtalar joint axis affected the overall biomechanics of the foot during weight bearing activities.”
Kirby KA: Subtalar joint axis location and rotational equilibrium theory of foot function. Journal Am Pod Med Assoc 91:465, 2001
Kirby KA: Subtalar joint axis location and rotational equilibrium theory of foot function. Journal Am Pod Med Assoc 91:465, 2001
“Therefore, during many weightbearingmotions, the foot may approximate a relatively rigid unit with all the bones of the foot rotating around the central pivot of the talus at the subtalar joint axis.”
Kirby KA: Subtalar joint axis location and rotational equilibrium theory of foot function. Journal Am Pod Med Assoc 91:465, 2001
“Finally, Huson’s theory on the constraint mechanism of the human tarsus, which has been supported by the tarsal kinematic research of Cornwall and McPoil, and the roentgen stereophotogrammetry studies done by Van Langelaan, Benink , and Lundberg and Svenssonare all consistent with the current author’s theory that the subtalar joint axis is the primary inversion/eversion axis of the foot.”
STJ: Pivitol Joint?“The authors believe that the finding that the magnitude of navicular(midfoot) movement is greater than that of calcaneus (rearfoot) illustrates the importance of the midfoot for typical foot function during walking.”
Cornwall MW, McPoil TG: Three-dimensional movement of the foot during the stance phase of walking. JAPMA 89:56, 1999.

13
Figure 1. An osteoligamentous dissected specimen of the foot exarticulated at the ankle joint. The dorsal capsules of the talonavicular and calcaneocuboid joints have been removed. The foot is held in the neutral position corresponding with upright standing.
Figure 2. The talus has been moved as it does in supination of the foot while the calcaneus, cuboid, and navicular are kept immobile. The talar head has left the navicular socket laterally, creating a wide gap at the medial side of the talonavicular joint.
“The tibiofibular talar unit does not function independently of the subtalar or midtarsal joint but acts cooperatively in closed-kinetic chain performance. The complex movement pattern known as supination and pronation of the foot must occur in concert with talar movement in the ankle housing unless spontaneous or surgical ankylosis has occurred in the ankle”
Vogler HW, Bojsen-Moller F: Tarsal functions, movement and stabilization mechanisms in foot, ankle and leg performance. JAPMA 90:112, 2000.
“Talar positioning on top of the calcaneus is determined by ankle movement and midtarsaljoint motions and varies depending on whether these are open- or closed-kinetic-chain events. Changes in any one of these joints alter the position and function of the others to varying degrees.”
Vogler HW, Bojsen-Moller F: Tarsal functions, movement and stabilization mechanisms in foot, ankle and leg performance. JAPMA 90:112, 2000.
“The subtalar joint provides most of the transverse plane motion which is necessary at the distal extremity to allow internal and external leg rotation during the stance phase of gait. The subtalar joint pronates to allow internal leg rotation and supinates to allow external leg rotation.”Root, ML, Orien, WP, Weed, JH: Clinical Biomechanics: Normal and Abnormal Function of the Foot, Vol 2. Los Angeles, Clinical Biomechanics Corp, 1977.
Two Lever Theory“The ankle connects two unequal levers, the leg and the foot. The longer lever contains only a pair of bones, the tibia and fibula. The more massive tibia conveys most of the body weight directly on the talus and acts as a solid lever in ankle injuries. The foot, on the other hand, is composed of numerous small bones intercepted by joints, which weaken it as a lever.”
Kelikian, 1985

14
Two Lever Theory
“Between these two unequal levers (unequal in bulk, length and strength) lies the talus. When the foot is dorsiflexed at the ankle, the talus becomes firmly lodged in the tibiofibular socket and serves as part of the proximal lever or the leg”
Kelikian, 1985
Transverse Plane
Internal rotation of tibia =
Internal rotation of talus
Tibial Rotation During Stance
• 25 Subjects
• External markers
• 3-D motion of foot and shank
Nester CJ., Hutchins S., Bowker P., Shank rotation: A measure of rearfootmotion during normal walking. Foot and Ankle 21: 578-583, 2000
Tibial Rotation During Stance
Max velocity of tib internal rotation = 7% of gait cycleMax velocity of tib external rotation = at toe offMax amount rotation of tibia = 12º internalTotal range rotation of tibia = 17º
Nester CJ., Hutchins S., Bowker P., Shank rotation: A measure of rearfoot motion during normal walking. Foot and Ankle 21: 578-583, 2000
15
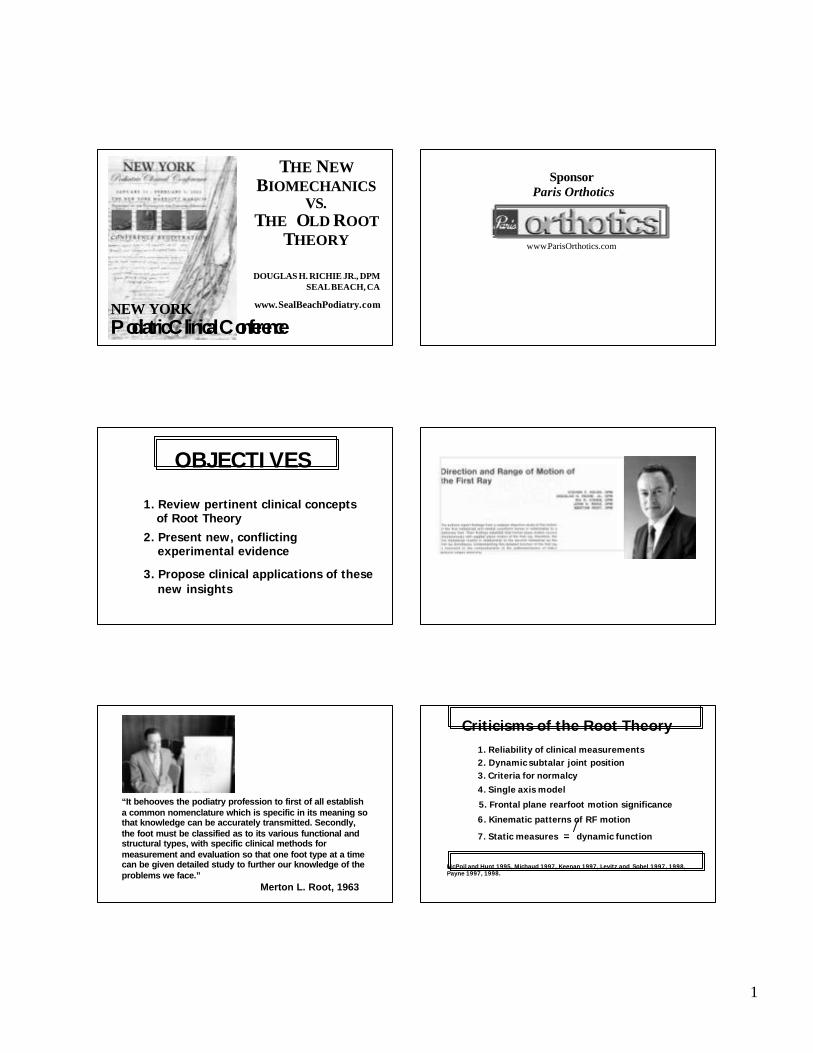
Angular displacement
Ang 310
5
0
-5
-10time (one gait cycle)
Toe off
Ang 1Ang 4
Ang 2
Ang 5
deg
rees
Nester CJ., Hutchins S., Bowker P., Shank rotation: A measure of rearfootmotion during normal walking. Foot and Ankle 21: 578-583, 2000
“We found that external rotation of the shank (indicating supination) began much earlier, at around 16% of the gait cycle. This is most likely a consequence of the fact that motion of the shank in the transverse plane can occur at the ankle and mid-tarsal joints without any change in the angle between the heel and shank in the frontal plane .”
Nester CJ, Hutcdhins S, Bowker P: Shank rotation: A measure of rearfoot motion during normal walking. Foot and Ankle International 21:578, 2000
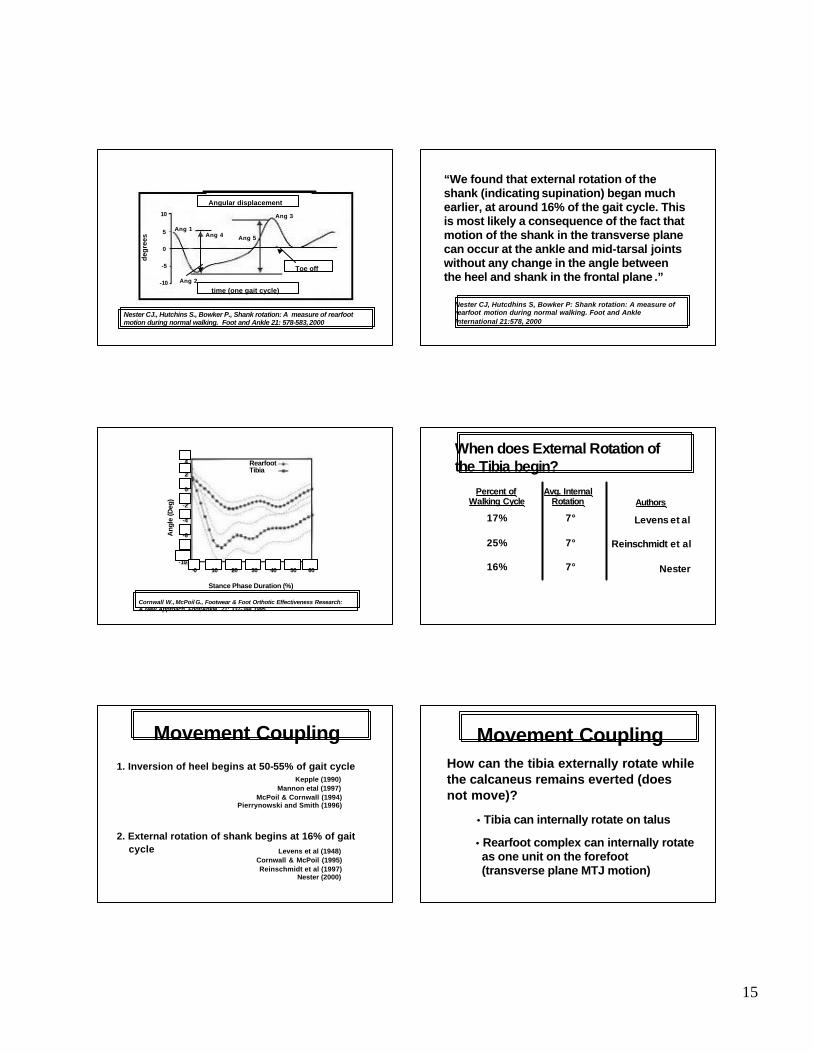
RearfootTibia
Ang
le (D
eg)
Stance Phase Duration (%)
4
2
0
-2
-4
-6
-8
-100 10 20 30 40 50 60
Cornwall W., McPoil G., Footwear & Foot Orthotic Effectiveness Research: A New Approach. Foot/Ankle 21: 337-344 1995
When does External Rotation of the Tibia begin?
Percent ofWalking Cycle Authors
Avg. Internal Rotation
17%
25%
16%
7°
7°
7°
Levens et al
Reinschmidt et al
Nester
1. Inversion of heel begins at 50-55% of gait cycleKepple (1990)
Mannon etal (1997)McPoil & Cornwall (1994)
Pierrynowski and Smith (1996)
2. External rotation of shank begins at 16% of gait cycle Levens et al (1948)
Cornwall & McPoil (1995)Reinschmidt et al (1997)
Nester (2000)
Movement Coupling
• Tibia can internally rotate on talus
How can the tibia externally rotate while the calcaneus remains everted (does not move)?
Movement Coupling
• Rearfoot complex can internally rotate as one unit on the forefoot(transverse plane MTJ motion)

16
Tibiotalar Delay• The talus does not immediately follow
internal / external rotation of the tibia.
• Ant. Talo-Fib and Sup Deltoid have to tighten before talar motion is observed.
Huson A, VanLangelaan EJ, Spoor CW: Tibiotalar delay and tarsal gearing. J Anat 149:244-245, 1986
“Lateral rotation of the lower leg in the stance phase of gait allows a slight delay in transmitting this transverse plane rotation to the foot. This action is believed to be related to that of the horizontally aligned ligament fibers that surround the ankle and talus that must absorb these forces before transmitting them”
Vogler HW, Bojsen-Moller F: Tarsal functions, movement and stabilization mechanisms in foot, ankle and leg performance. JAPMA 90:112, 2000.
Transverse Plane Movements In Gait
Ankle
Midtarsal
18°
15°
McCullough, Burge
Nester
Nester10.6°

17
Ankle vs STJ“Transformation of leg rotation into calcaneal eversion-inversion, and vice versa, has been suggested to occur mainly at the subtalar joint. When this is true, subtalar joint fusion must result in a significant loss of movement transferred between calcaneus eversion-inversion and tibial rotation. However, as shown previously, it did not.”
Hintermann B., Nigg BM: Influence of arthrodeses on kinematics of the axially loaded ankle complex during dorsiflexion/plantarflexion. Foot & Ankle 16:633, 1995
Foot & Ankle International/Vol.21, No. 3/March 2000
Fig. 5 Movement coupling between calcaneal eversion-inversion and tibial rotation for the five test subjects (mean curves of three repetitions). The dashed line represents a theoretical 1:1 coupling from the calcaneus to the tibia. HS (heel strike); MS (midstance); TO (takeoff); SD (mean standard deviation in the horizontal (x) and vertical (y) direction)
Stacoff, Nigg, Reinschmidt, 2000
“Considering motion at only one of the three, i.e. the subtalar joint, is unlikely to describe the eventual motion which results from all three in combination since it does not account for factors affecting the other joints.”
Nester , 1997
Ankle, Subtalar and Mid-tarsal joints
“Rear foot Complex”Downing, 1978
Nester, 1997
“Tarsal Mechanism”Huson, 1991
“Ankle Joint Complex”Hintermann, Nigg, 1994
Ankle Joint Complex3 Segments: tibia, talus and calcaneus2 Joints: ankle, subtalar
Universal Joint:inversion of calcaneus = external rotation of tibiaeversion of calcaneus = internal rotation of tibia
18
CKC§ Universal Joint
Rotation
§ Torsion Transmission
§ Tibia: Dominant Lever
19
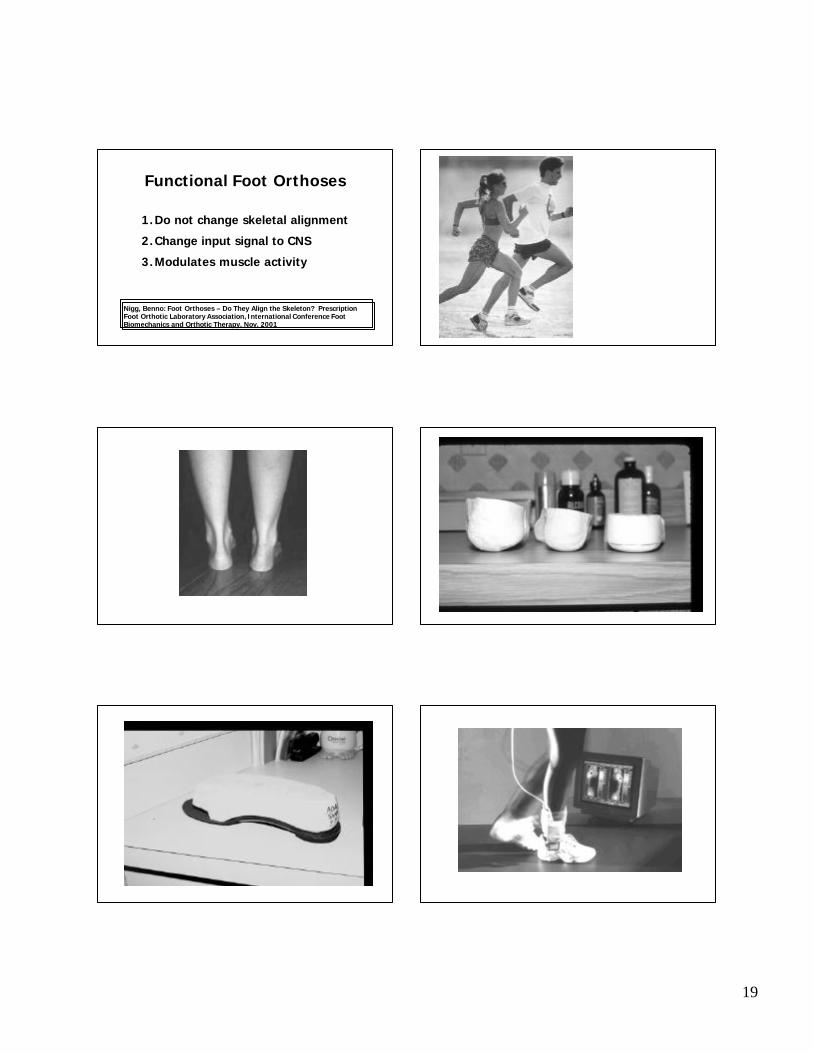
Functional Foot Orthoses
1.Do not change skeletal alignment
2.Change input signal to CNS
3.Modulates muscle activity
Nigg, Benno: Foot Orthoses – Do They Align the Skeleton? Prescription Foot Orthotic Laboratory Association, International Conference Foot Biomechanics and Orthotic Therapy. Nov. 2001

20
Shin Muscle Activity On Various Sport Surfaces:
An EMG StudyBy:
DOUGLAS H. RICHIE, D.P.M.HERBERT A. DeVRIES, Ph.D.CLIFFORD K. ENDO, D.P.M.
JOURNAL AMERICAN PODIATRIC MEDICAL
ASSOCIATION
VOL 83, No. 4, APRIL., 1993
- Two separate counters- Kistler accelerometer triggers timing circuit- Concentric phase begins at g Max through
mid-swing- Eccentric phase begins at mid-swing through
contact and g Max
ECCENTRICvs.
CONCENTRIC PHASES

21
Stationary Run
Eccentric Phase – Leg flexors lengthen immediately after foot touchdown
Concentric Phase – Leg flexors shorten immediately after g Max during propulsion
22
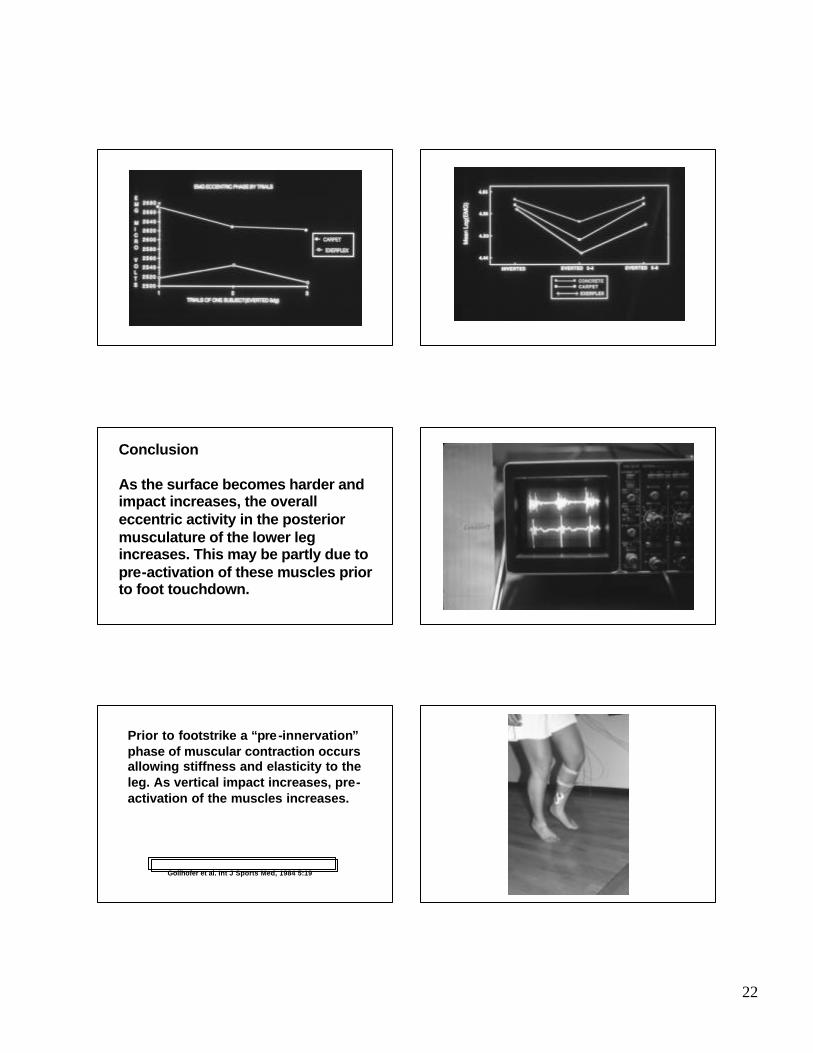
Conclusion
As the surface becomes harder and impact increases, the overall eccentric activity in the posterior musculature of the lower leg increases. This may be partly due to pre-activation of these muscles prior to foot touchdown.
Prior to footstrike a “pre-innervation” phase of muscular contraction occurs allowing stiffness and elasticity to the leg. As vertical impact increases, pre-activation of the muscles increases.
Gollhofer et al. Int J Sports Med, 1984 5:19
23
Where Do We Go From Here?
1. Re-design podiatric biomechanics curriculum
2. Emphasize importance of joint interdependence and foot-leg interdependence
3. Prioritize clinical & laboratory research
4. Beliefs must be based upon sound scientific methodology
“The field of foot orthopedics, and to some degree foot surgery, is a conglomeration of theory, techniques of treatment, and treatment modalities that are too frequently not based upon scientific fact.”
Merton L. Root, 1963
Where Do We Go From Here?
5. It is o.k. to say: “I don’t know…”