nutrition in pregnancy - postgraduate medical journal · nutrition inpregnancy births calories 8000...
TRANSCRIPT

Postgraduate Medical Journal (May 1979) 55, 295-302
Nutrition in pregnancy
F. E. HYTTENM.D., Ph.D., F.R.C.O.G.
Division of Perinatal Medicine, Clinical Research Centre, Watford Road, Harrow, Middlesex HAI 3UJ
SummaryEpidemiological evidence shows that women living inaffluent circumstances have bigger babies with a lowermortality than underpriviliged women. How much ofthat effect is due to nutrition alone is not known butsupplementary feeding in pregnancy of chronically illnourished women does appear to increase mean birthweight, and famine conditions in a basically wellnourished community reduce the birth weight; in bothcases the birth weight difference is relatively small andcould be accounted for by no more than fetal adiposetissue.The fetus may be much less vulnerable to vagaries of
maternal diet than has been thought because of protec-tive physiological mechanisms associated with preg-nancy. Firstly the mother's energy balance changes, sothat if she has access to extra food in the first half ofpregnancy she will store large amounts of depot fat asan energy buffer against possible privation later.Secondly, there are widespread changes in nutrientmetabolism one of which is to lower plasma levels ofmost nutrients, and that may tip the balance ofadvantage away from maternal tissue towards theplacenta. Finally, the placenta itself has developedelaborate mechanisms to acquire nutrients from thematernal circulation. A notable exception to that ruleis glucose for which no active transport mechanism hasevolved and which might therefore be regarded as alow priority nutrient; it may be that the generoussupply of glucose for the fetus which would be providedby a well fed woman does little more than allow thefetus to build up its fat stores.
IntroductionThe subject of nutrition embraces everything from
population statistics to the subtle activities of intra-cellular enzymes. Information throughout that rangeis particularly thin and fragmentary in pregnancy,but with a bravery born of ignorance the authorwould like to collect together some of the phenomenaassociated with nutrition in pregnancy and try tomake some kind of coherent if superficial picture.Although it is obvious to the clinician that most
poorly nourished and socially deprived women re-
produce easily, and that healthy well fed mothersmay produce poorly grown infants, it is neverthelesspart of medical folk-lore that successful reproductiondepends on good nutrition. Large scale statisticssupport that idea: women in affluent circumstanceshave bigger babies and fewer perinatal deaths thansocially under-privileged women, but interpretationof those differences is bedevilled by the fact thatnutritional variables never operate in isolation.Affluent mothers are not only better fed, they enjoyand have had a life-long experience of superiorhealth, education, housing and medical care; theyplan their families advantageously and they smokeless. Thus, the large differences in perinatal mortalitywhich occur within a single small country such asBritain from the high rates in Clydeside and Mersey-side to the low rates in South-East England un-doubtedly reflect more than simple differences ofdiet during pregnancy.The most persuasive evidence that diet itself may
have an effect on reproductive performance was pro-vided by the involuntary 'feeding experiment' madeon a national scale in Britain during World War II.A dramatic fall in the stillbirth rate (per thousandtotal births), from 38 in 1940 to 28 in 1945 was con-sidered by Duncan, Baird and Thomson (1952) to bedue mainly to improved maternal nutrition whichfollowed an enlightened food-rationing policy underwhich pregnant and lactating women receivedpriority; civilian medical services were attenuatedand there was no advance in treatment that wouldplausibly have reduced stillbirths so substantially atthat time.
But even in a wholly nutritional context interpre-tation is not straightforward. How much of an effectis due to 'nutritional status', that elusive concept ofbeing well grown and well nourished which is sodifficult to define and measure, and how much to theactual diet taken during pregnancy? Again the twooverlap. Women who live in socio-economic circum-stances where they are poorly fed as children, growpoorly, and eat poorly as adults, are the ones whoeat poorly in pregnancy.The combined effect is not as great as one might
0032-5473/79/0500-0295$02.00 © 1979 The Fellowship of Postgraduate Medicine
copyright. on M
ay 26, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.55.643.295 on 1 M
ay 1979. Dow
nloaded from
expect. Gambian women who are small and, byWestern standards, ill nourished, also have smallweight gains in pregnancy; when most of pregnancycoincides with the wet season with its associated loadof increased agricultural work and infectious diseasethe mean weight gain can be as little as 2-2 kg(Thomson et al., 1966). Yet the seasonal fluctuationin birth weight is small and not statistically signifi-cant, and the infants generally thrive.
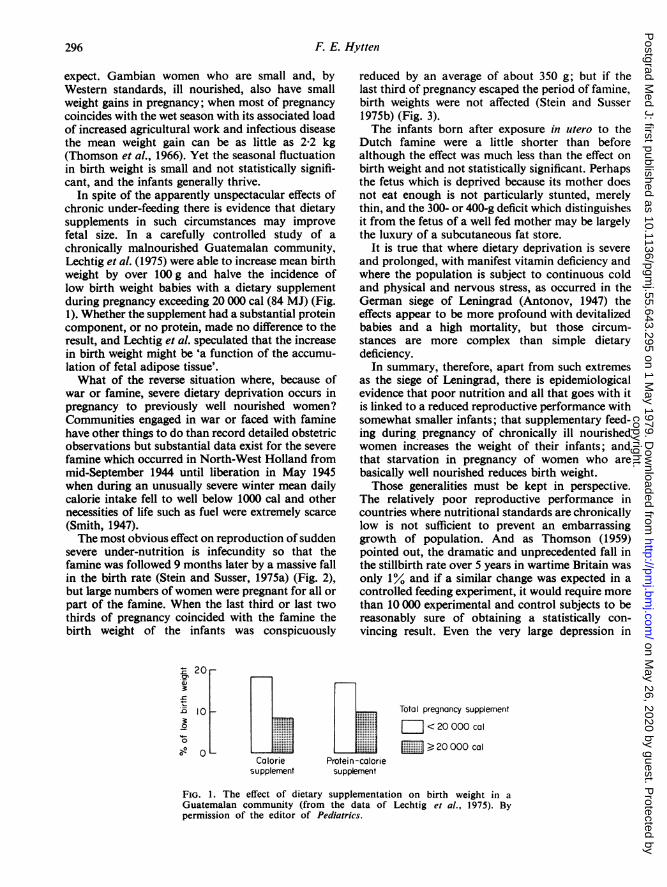
In spite of the apparently unspectacular effects ofchronic under-feeding there is evidence that dietarysupplements in such circumstances may improvefetal size. In a carefully controlled study of achronically malnourished Guatemalan community,Lechtig et al. (1975) were able to increase mean birthweight by over 100 g and halve the incidence oflow birth weight babies with a dietary supplementduring pregnancy exceeding 20 000 cal (84 MJ) (Fig.1). Whether the supplement had a substantial proteincomponent, or no protein, made no difference to theresult, and Lechtig et al. speculated that the increasein birth weight might be 'a function of the accumu-lation of fetal adipose tissue'.What of the reverse situation where, because of
war or famine, severe dietary deprivation occurs inpregnancy to previously well nourished women?Communities engaged in war or faced with faminehave other things to do than record detailed obstetricobservations but substantial data exist for the severefamine which occurred in North-West Holland frommid-September 1944 until liberation in May 1945when during an unusually severe winter mean dailycalorie intake fell to well below 1000 cal and othernecessities of life such as fuel were extremely scarce(Smith, 1947).The most obvious effect on reproduction of sudden
severe under-nutrition is infecundity so that thefamine was followed 9 months later by a massive fallin the birth rate (Stein and Susser, 1975a) (Fig. 2),but large numbers ofwomen were pregnant for all orpart of the famine. When the last third or last twothirds of pregnancy coincided with the famine thebirth weight of the infants was conspicuously
20
°~ 10
0
oCalorie Protein
supplement suppk
reduced by an average of about 350 g; but if thelast third of pregnancy escaped the period of famine,birth weights were not affected (Stein and Susser1975b) (Fig. 3).The infants born after exposure in utero to the
Dutch famine were a little shorter than beforealthough the effect was much less than the effect onbirth weight and not statistically significant. Perhapsthe fetus which is deprived because its mother doesnot eat enough is not particularly stunted, merelythin, and the 300- or 400-g deficit which distinguishesit from the fetus of a well fed mother may be largelythe luxury of a subcutaneous fat store.
It is true that where dietary deprivation is severeand prolonged, with manifest vitamin deficiency andwhere the population is subject to continuous coldand physical and nervous stress, as occurred in theGerman siege of Leningrad (Antonov, 1947) theeffects appear to be more profound with devitalizedbabies and a high mortality, but those circum-stances are more complex than simple dietarydeficiency.
In summary, therefore, apart from such extremesas the siege of Leningrad, there is epidemiologicalevidence that poor nutrition and all that goes with itis linked to a reduced reproductive performance withsomewhat smaller infants; that supplementary feed-ing during pregnancy of chronically ill nourishedwomen increases the weight of their infants; andthat starvation in pregnancy of women who arebasically well nourished reduces birth weight.Those generalities must be kept in perspective.
The relatively poor reproductive performance incountries where nutritional standards are chronicallylow is not sufficient to prevent an embarrassinggrowth of population. And as Thomson (1959)pointed out, the dramatic and unprecedented fall inthe stillbirth rate over 5 years in wartime Britain wasonly 1% and if a similar change was expected in acontrolled feeding experiment, it would require morethan 10 000 experimental and control subjects to bereasonably sure of obtaining a statistically con-vincing result. Even the very large depression in
Total pregnancy supplement
J -< 20 000 cal
: : >20 000 cal
FIG. 1. The effect of dietary supplementation on birth weight in aGuatemalan community (from the data of Lechtig et a!., 1975). Bypermission of the editor of Pediatrics.
F. E. Hytten296copyright.
on May 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.55.643.295 on 1 May 1979. D
ownloaded from

Nutrition in pregnancy
Births Calories8000 4000
7000 3500
6000 3000
5000 2500
4000 2000
3000 1500
2000 1000
J A JO J A1944 1945
(Calendar months s
A
I \I-
I \\ /
II11111 \\\\,1111//
\ I\ /
,v
I I
J O J A J 0O1946
;tarting with January)
FIG. 2. The effect of the famine in North-West Holland in 1944-45on fertility (from the data of Stein and Susser, 1975a). Calorieration; ---- total births.
birth weight of the infants born to the starving Dutchwomen appears to have had no permanent effect ontheir subsequent growth and intellectual develop-ment (Stein et al., 1975).Throughout evolution pregnant women will have
been subjected to nutritional deprivation from foodshortage, and pregnant women seem always to havebeen subject to a range of nutritional taboos andrestrictions. Even today nutritional advice given byobstetricians to their patients is generally restrictiverather than generous. The obvious ability of thepregnant woman and her fetus to weather the gamutof hazards from crop failure to obstetrical advicemay well be due to physiological changes in nutrientmetabolism which makes her more resilient todeprivation and her fetus less vulnerable than per-haps has been believed.
Changes in energy balancePhysiological changes in pregnancy are charac-
teristically anticipatory and a good example is pro-vided by a major change in energy balance. Theaverage healthy woman eating to appetite gains12.5 kg of body weight, a weight gain associated withthe best clinical outcome, and this is considerablymore than can be accounted for in the product of
3400
FamineOctober 1944 -May 1945
3300--
* 3200
-c
3100
3000
Pregnancycohorts
FIG. 3. The effect of the famine in North-West Hollandin 1944-45 on birth weight (from the data of Stein andSusser, 1975b).
297copyright.
on May 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.55.643.295 on 1 May 1979. D
ownloaded from

298 F. E. Hytten
conception, the growth of uterus and breasts and theexpansion of volume of blood and other body fluids(Hytten and Leitch, 1971). The balance amounts toabout 3-5 kg and is body fat. Figure 4 shows the
6r5
,'
_~~~~~~/
3
eJ2 / /
0 10 20 30 40
Weeks of pregnancy
FIG. 4. Components of the weight gained by the normalpregnant woman (from Hytten and Leitch, 1971)....... Uterus and contents; ---- maternal stores;
blood and body fluids.
various components of weight gain separately; thepattern of accumulation of the extra body fat differsfrom that of the other components, beginning earlyin pregnancy, showing maximum rate of gain in mid-pregnancy and almost stopping in the last trimester.That pattern is confirmed by measurements of skinfold thickness which further shows the characteristiccentripetal distribution of fat accumulation inprenancy: over the abdomen, back and upper thighsthere is a progressive increase in skin fold thicknessup to about 30 weeks after which there is no furtherincrease; over the arms and lower part of the thighsthere is no increase or even a loss.The accumulation of depot fat on a scale otherwise
unknown in healthy adult life makes obviousbiological sense. The average woman will enter thelast trimester of pregnancy with a very considerablebuffer against possible deprivation of food amount-ing to more than 30 000 cal (126 MJ). In Westernsociety the healthy pregnant woman needs no suchbuffer, but the majority of the world's women doarduous manual labour until the day they give birthand it is generally in those parts of the world thatfood supplies are uncertain; such conditions werepresumably the rule when mammalian reproductionwas evolving. Analogous anticipatory fat storageoccurs in mammals before hibernation and in birdsbefore migration. Figure 5 shows that the energyaccumulated in body fat by the average pregnantwoman in the first 2 trimesters of pregnancy couldcompletely subsidize the extra maintenance costs oflate pregnancy.
The evidence suggests that the stimulus to accumu-late body fat is not simply through the appetite-satiety centres driving the mother to eat more but bya more fundamental change in the control of energybalance. The total quantity of body fat is controlledby a central 'lipostat' and if this is set higher, as itcan be, e.g. in female rats by progesterone, then thenew level of body fat is achieved either by eatingmore, or expending less energy, or both. The preg-nant woman normally does both, although to whatextent either is possible in some developing com-munities is not known. Appetite usually increaseswithin the first trimester, but even without aconscious increase almost all women eat more thanusual by a daily average of some 200 cal (840 kJ),about half the specific requirement shown in Fig. 5.
80 _70
50-
40-3r n - .....iiiiiiiiii
O2010 I
0 10 20 30 40
Weeks of pregnancy
FIG. 5. The cumulative energy costs of pregnancy (fromHytten and Leitch, 1971). 03 Maintenance; fat;O protein.
They also reduce energy output in several ways:women are relatively listless in pregnancy, they spendmore time at rest and they perform fewer strenuoustasks; moreover they appear to perform those taskswith more economy of effort than when they are notpregnant and there is a general relaxation ofvoluntary muscle. A reduction in circulating freethyroid hormone also suggests that all maternaltissue may be metabolizing at a somewhat reducedtempo.
Changes in nutrient metabolismMuch less is understood about the many changes
in nutrient metabolism. One of the most studied isglucose and Dr Lind (1979) will be dealing with thataspect in detail. The fasting level of glucose in plasmafalls within the first few weeks of pregnancy to a newlevel some 10-15ca below the non-pregnant con-centration (Lind, 1975) and that has been interpreted(e.g. by Freinkel, 1969) as 'accelerated starvation'
copyright. on M
ay 26, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.55.643.295 on 1 M
ay 1979. Dow
nloaded from

Nutrition in pregnanco,
due to the continuous withdrawal of glucose andamino acids by the fetus. The concept is unconvin-cing because the fall occurs at the beginning ofpregnancy when competition by the fetus weighingonly a few milligrams cannot be seriously enter-tained, and because prolonged starvation in preg-nancy (Felig and Lynch, 1970; Tyson et al., 1976)fails to show a progressive disadvantage to thepregnant woman (Fig. 6). Whatever its explanation,the reduced fasting glucose concentration stands incurious contrast to the progressive relaxation ofglucose tolerance following a glucose load in spite ofan increasing insulin response. It is difficult to seewhat purpose might be served by this change ofcontrol but presumably the fetus has a better chanceof sharing the maternal meal if glucose levels in theplasma perfusing the placenta remain higher forlonger.Glucose is not alone in showing reduced fasting
levels; the plasma levels of most nutrients fall inpregnancy (Fig. 7). Only lipid fractions tend to rise,and while it is possible to explain some of the changesin the figure the majority are enigmatic (Hytten,1978a).The homoeostatic control of nutrient levels in
blood and tissue fluids reflects two kinds of physio-logical need: the need to have a certain total quantityof a substance available in the circulation, and theneed to have a substance at a particular concentra-tion. Thus it is the total quantity of some proteinfractions in the circulation which matters; offibrinogen for effective haemostasis, of y-globulinfor effective control of infection and of haemoglobinwhere the total is matched with some precision to the
(o)300
·.o -150 2 24 36 48 60 72
a.
(c)
o 40
a. , 2 24 36 48 60 72
need for oxygen carriage. For other substances theefficient function of the body requires a preciselycontrolled concentration: ionized calcium andhydrogen are examples.
In pregnancy both types of control are affected.For example Ca++ and H+ are preserved at theusual non-pregnant concentrations, but osmolalityand Pco2 whose levels are subject to equally carefulcontrol are maintained during pregnancy at muchlower levels. As examples of changes in totalquantity, there is a greatly increased amount offibrinogen in the circulation, enough to raise theconcentration considerably even in the expandedplasma volume; and there is also a considerable risein the total circulating haemoglobin, quite sufficientto cover the needs for extra oxygen carriage but notenough to prevent a fall in concentration as theplasma volume rises; on the other hand the totalquantity of circulating albumin falls, and with italbumin concentration and colloid osmotic pressure.How the levels of most nutrients are controlled is
a mystery. Why do the fat-soluble vitamins tend torise in concentration while the water-soluble vita-mins invariably decline? Why does fasting glucosefall in early pregnancy to a new level, and why doamino acids show a complex pattern of changewhere some remain unchanged, but the majorityfall?The answers to those, and many other questions,
are unlikely to be found before the fundamentals ofcontrol are understood at least for the non-pregnant;at present there is no information about how nutrientlevels in the blood are governed. For example, untilone knows what controls the 'fasting' blood sugar in
(b)
-- --
(d)
0 -
I I I12 24 36 48 60 72 84
Fasting (hr)
FIG. 6. The effect of starvation on plasma levels of glucose and alaninein normal pregnancy (data (a) and (c) from Tyson et al., 1976; (b) Felig andLynch, 1970; (d) Felig et al., 1972). The dotted lines refer to pregnantsubjects the solid lines to non-pregnant women.
299copyright.
on May 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.55.643.295 on 1 May 1979. D
ownloaded from

F. E. Hytten
200r
c
oc
o
oo_o
e
Triglycerides
- a-Tocopherol
Glycerol
Non- esterified/ fatty acids
Na+Ca++ and Mg++Glucose
- Amino acidsVitamin 812
' Vitamin C
' Folate; vitamin B6
0 10 20 30 40Weeks of pregnancy
FIG. 7. Changes in pregnancy of the plasma concentrations of somenutrients. The levels shown in this figure are percentages of thenon-pregnant level taken as 100% (Hytten, 1978a).
the normal person -why one woman should pre-serve a level of 5, and another a level of 4 mmol/l,one is not likely to be able to interpret the fall inlevel which occurs in early pregnancy. And that iseven more true of nutrients like folate where there isno certainty that any homoeostatic control exists atall.The preponderant pattern of reduction in the
plasma levels of nutrients suggests a commonmechanism or perhaps a common purpose. Nomechanism is known and because of the differencesof pattern of fall none seems likely. Dilution by theincreasing plasma volume cannot explain the suddendrop in concentration shown by glucose and aminoacids in early pregnancy, although it could explainthe more gradual change in folate concentration.Dietary deficiency or failure of absorption is cer-
tainly not responsible at least for most of the lowlevels described, although many can be artificiallyraised by large dietary supplements. Nor is it likelythat excessive excretion in the urine plays more thana marginal role: all women show a reduced fastingblood sugar but not all have glycosuria and there islittle relation between amino acid excretion andblood levels. For example, histidine, which is lost ingreatest amounts in the urine, has an unchangedplasma level in pregnancy.Although dietary deficiency is the popular scape-
goat for the reduced nutrient levels in normal preg-nancy it is worth emphasizing its implausibility: itseems excessively unlikely that a phenomenon affect-ing all healthy well nourished women having normalpregnancies and healthy babies is due to an inade-quate diet, and the reduced concentrations often
300
copyright. on M
ay 26, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.55.643.295 on 1 M
ay 1979. Dow
nloaded from

Nutrition in pregnancy
and it seems strange that the fetus should have torely on a favourable concentration gradient fromoccur in the presence of greatly increased totalcirculating quantities. Moreover, it is surely illogicalto believe that lower levels of some nutrients such asfolate or iron indicate dietary deficiency requiringsupplements, when other nutrients with equallyreduced levels such as glucose and some amino acidsare ignored.The changes in nutrient level are so widespread
and varied in detail that it would appear that levelsof many different nutrients are reduced by a resettingof many different mechanisms, and that suggests acommon purpose. Could it be that a general loweringof nutrient levels produces a balance which favourstransfer to the fetus rather than to maternal tissues?The placenta is clearly capable of taking up mostnutrients with considerable efficiency and is perhapsbetter able to do so than the maternal liver at the lowlevels which are usual in pregnancy.
It is characteristic of many nutrients that thereduced maternal plasma levels are matched by ahigher level in the fetal plasma with a level in theplacenta considerably in excess of either circulation(Table 1). The placenta is clearly capable of extract-ing a large store from the maternal circulation toprovide a consistent gradient towards the fetus. Itappears to achieve this, at least for some nutrients,by operating a 'biochemical valve'. Nutrients takeninto the placenta are transformed into derivativeswhich cannot return to the mother, a system whichoffers great advantage to the fetus, in the last resortat the expense of maternal nutrition. For example,the fetus may maintain normal folate levels while itsmother becomes grossly anaemic from folatedeficiency.That is to say, the nutritional symbiosis between
mother and fetus seems to involve the 'deliberate'change of nutrient levels in the maternal blood toshift the balance of advantage to the fetus. In a well
fed society the fetus has no need of this advantage,but if the mother is deficient then the fetus willexercise it to the detriment of the mother and itbecomes a true parasite.The relative sizes of mother and fetus allow the
fetus to take such essential nutrients as amino acidsfrom the mother, even if she is having to mobilizethem from her own tissues, without serious embar-rassment. Some other nutrients such as folate,however, may be in such short supply that therelentless fetal mechanism of acquisition can threatenthe mother's life.
ConclusionAlthough poor nutrition leads to a reduced re-
productive performance the effect is marginal andrequires large population groups to demonstrate it.The starvation of previously well nourished womenduring pregnancy, and the dietary supplementationof chronically ill nourished women has a relativelytrivial effect, a change in mean birth weight of nomore than about 300 g with an otherwise uncon-vincing effect on fetal size.
It is suggested that, in general, the fetus which isdeprived only because its mother does not eat enoughis not particularly stunted, merely lean, and the300-g deficit which distinguishes it from the fetusof a well fed, or a supplemented mother may belargely the luxury of a subcutaneous fat store.From the point of view of the fetus, nutrients
appear to be separated into two main groups. Thosewhich are vital to its growth and development andfor which mechanisms have evolved to ensuresupplies at all costs, and those which are in a senseoptional extras, used if available but dependingupon favourable concentration gradients from themother.
In the latter group are glucose and fatty acids.Obviously some fatty acids are essential for the fetus
TABLE 1. Approximate plasma levels of 4 water soluble nutrients in the mother before pregnancy and in late pregnancy, andin the fetus, compared to tissue levels in the placenta
Maternal plasmaPlacental Fetal
Before pregnancy Late pregnancy tissue plasma
Substance Per litre Per litre Per kg Per litre ReferenceFree amino acids (tamol) 2800 1800 10000 3300 Lindblad and Baldesten, 1967
Pearse and Sornson, 1969
Ascorbate (mg) 20 10 90 20 Barnes, 1947
Total riboflavin (jig) 60 30 2140 40 Lust, Hagerman and Villee, 1954
Folate (tg) 7 3 750 15 Landon and Hytten (unpublished)_~ ~~ ~~~ ~~ ~~ ~~ ~~~~~~~~~~~~~~~~~~~~~~~
301copyright.
on May 26, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.55.643.295 on 1 May 1979. D
ownloaded from

302 F. E. Hytten
and it seems strange that the fetus should have torely on a favourable concentration gradient fromthe mother for its supplies (Elphick, Hull andSanders, 1976; Elphick, Edson and Hull, 1978).However, since free fatty acids in the plasma risewhen the mother starves it seems unlikely that thefetus would ever be seriously deprived. Glucose, incontrast, is something of a luxury food, and theinfant's fat store, built from glucose, is largely afunction of the mother's plasma levels, high in thewell fed and low in the starved. When the mothereats well then the relaxed glucose tolerance allows thefetus a generous share; when she does not then thefetus gets enough glucose for its immediate needs orcan make it from non-carbohydrate precursors. If agenerous supply of glucose were essential to fetalgrowth and survival then evolution would presum-ably have seen to it that the placenta acquiredglucose actively, but glucose crosses to the fetus byfacilitated diffusion and depends for its placental tran-sport on a gradient from the mother (Hytten, 1978b).
It seems unlikely that fetal growth would benoticeably affected by marginal supplies of glucose,although it is possible that if the fetus does haveincreased levels of plasma glucose then the insuilinwhich it may release to control it will have a minorgrowth-promoting effect. But the essential nutrientssuch as amino acids and the vitamins are activelytransported to the fetus by a placenta which willacquire them inexorably regardless of the mother'sstate of nutrition, ensuring a reasonably well grownif lean baby.The author must reiterate that he is speaking as a
physiologist about the physiological safeguardsagainst maternal deprivation enjoyed by the fetus ofa basically healthy woman and which he believes itis very difficult to damage by overall restriction ofdiet. However, for the fetus of an apparently normalwoman which is growth-retarded perhaps because ofsome pathology affecting placental function, thesesafeguards may not be effective and dietary supple-ments are probably inappropriate.
In communities such as rural Guatemala, wheremost mothers are deprived, undergrown andgenerally unhealthy, extra feeding in pregnancy mayhelp to support the inifant's undoubted capacity tosurvive by parasitism, but the basic defect of pro-longed underfeeding of the mother must be tackledat a social rather than a clinical level.
ReferencesANTONOV, A.N. (1947) Children born during the siege of
Leningrad in 1942. Journal of Pediatrics, 30, 250.BARNES, A.C. (1947) Placental metabolism of vitamin C. 1.Normal placental content. American Journal of Obstetricsand Gynecology, 53, 645.
DUNCAN, E.H.L., BAIRD, D. & THOMSON. A.M. (1952) Thecauses and prevention of stillbirths and first week deaths. 1.The evidencc of vital statistics. Journal of Obstetrics and
Gynaecology of the British Commonwealth, 59, 183.ELPHICK, M.C., EDSON, J.L. & HULL, D. (1978) Transport of
free fatty acids across the perfused human placenta. IRCSMedical Science, 6, 114.
ELPHICK. M.C., HULL, D. & SANDERS, R.R. (1976) Concen-trations of free fatty acids in maternal and umbilical cordblood during elective Caesarean section. British Journal ofObstetrics and Gynaecology, 83, 539.
FELIG, P., KIM, Y.J., LYNCH, V. & HENDLER, R. (1972) Aminoacid metabolism during starvation in human pregnancy.Journal of Clinical Investigation, 51, 1195.
FELIG, P. & LYNCH, V. (1970) Starvation in human preg-nancy: hypoglycemia, hypoinsulinemia and hyper-ketonemia. Science. New York, etc., 170, 990.
FREINKEL, N. (1969) Homeostatic factors in fetal carbo-hydrate metabolism. In: Fetal Homeostasis, (Ed. by Wynn,R.M.) vol. 4, p. 85. Appleton-Century-Crofts, New York.
HYTTEN, F.E. (1978a) Physiological adjustments in preg-nancy. In: Scientific Basis of Obstetrics and Gynaecology(Ed. by MacDonald, R.R.), 2nd edn, p. 62. ChurchillLivingstone, Edinburgh.
HYTTEN, F.E. (1978b) Placental handling of glucose. In:Proceedings of 2nd Aberdeen International Colloquium onCarbohydrate Metabolism in Pregnancy and the Newborn.(In press )
HYTTEN, F.E. & LEITCH, I. (1971) The Physiology of HumanPregnancy. 2nd edn. Blackwell Scientific Publications,Oxford.
LECHTIG, A., HABICHT, J.-P., DELGARDO, H., KLEIN, R.,YARBOROUGH, C. & MARTORELL, R. (1975) Effect of foodsupplementation during pregnancy on birth weight.Pediatrics, 56, 508.
LIND, T. (1975) Changes in carbohydrate metabolism duringpregnancy. Clinics in Obstetrics and Gynaecology, 2, 395.
LIND, T. (1979) Metabolic changes in pregnancy relevant todiabetes mellitus. Postgraduate Medical Journal, 55, 353.
LINDBLAD, B.S. & BALDESTEN, A. (1967) The normal venousplasma free amino acid levels of non-pregnant women andof mother and child during delivery. Acta paediatricascandinavica, 56, 37.
LUST, J.E., HAGERMAN, D.D. & VILLEE, C.A. (1954) Thetransport of riboflavin by human placenta. Journal ofClinical Investigation, 33, 38.
PEARSE, W.H. & SORNSON, H. (1969) Free amino acids ofnormal and abnormal human placenta. American Journalof Obstetrics and Gynecology, 105, 696.
SMITH, C.A. (1947) Effects of maternal undernutrition uponthe newborn infant in Holland (1944-1945). Journal ofPediatrics, 30, 229.
STEIN, Z. & SUSSER, M. (1975a) Fertility, fecundity, famine:food rations in the Dutch famine 1944/5 have a causalrelation to fertility and probably to fecundity. HumanBiology, 47, 131.
STEIN, Z. & SUSSER, M. (1975b) The Dutch famine, 1944-1945, and the reproductive process. I. Effects on six indicesat birth. Pediatric Research, 9, 70.
STEIN, Z., SUSSER, M., SAENGER, G. & MAROLLA, F. (1975)Famine and Human Development: the Dutch HungerWinter of 1944-1945. Oxford University Press, New York.
THOMSON, A.M. (1959) Diet in pregnancy. 3. Diet in relationto the course and outcome of pregnancy. British Journal ofNutrition, 13, 509.
THOMSON, A.M., BILLEWICZ, W.Z., THOMPSON, B. &McGREGOR, I.A. (1966) Body weight changes duringpregnancy and lactation in rural African (Gambian)women. Journal of Obstetrics and Gynaecology of theBritish Commonwealth, 73, 724.
TYSON, J.E., AUSTIN, K., FARINHOLT, J. & FIEDLER, J. (1976)Endocrine-metabolic response to acute starvation inhuman gestation. American Journal of Obstetrics andGynecology, 125, 1073.
copyright. on M
ay 26, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.55.643.295 on 1 M
ay 1979. Dow
nloaded from