nursing management of genitourinary dysfunction: nursing management of genitourinary dysfunction:...
TRANSCRIPT
NURSING NURSING MANAGEMENT OF MANAGEMENT OF GENITOURINARY GENITOURINARY DYSFUNCTION: DYSFUNCTION: Theoretical Skills and
Knowledge, Scientific Principles, Critical Thinking, Healthcare
Promotion, Wellness and Illness, and Stress Adaptation

Lecture Objectives:Lecture Objectives:
1.1. Describe common renal and urinary Describe common renal and urinary disorders that occur in children.disorders that occur in children.
2.2. Assess a child for a renal or urinary Assess a child for a renal or urinary tract disorder.tract disorder.
3.3. Formulate nursing diagnoses related Formulate nursing diagnoses related to renal or urinary tract disorders.to renal or urinary tract disorders.
4.4. Establish outcomes related to the Establish outcomes related to the care of a child with renal or urinary care of a child with renal or urinary disorder.disorder.
5.5. Plan nursing care related to urinary Plan nursing care related to urinary or renal disorders.or renal disorders.

Lecture Objectives Lecture Objectives (cont.)(cont.)
6.6. Implement nursing care for the child with Implement nursing care for the child with a renal or urinary disorder.a renal or urinary disorder.
7.7. Evaluate outcomes for achievment and Evaluate outcomes for achievment and effectiveness of care.effectiveness of care.
8.8. Analyze methods for making nursing care Analyze methods for making nursing care of the child with a renal or urinary of the child with a renal or urinary disorder more family centered.disorder more family centered.
9.9. Compare and contrast acute and chronic Compare and contrast acute and chronic renal failure.renal failure.
10.10. Discuss the types of renal dialysis.Discuss the types of renal dialysis.11.11. Assess for signs of kidney transplant Assess for signs of kidney transplant
rejection.rejection.
Reading Assignment:Reading Assignment:
Wong, Perry & Hockenberry Ch. 50; p 1643-1669
Renal System Renal System AssessmentAssessment Physical assessmentPhysical assessment
– Palpation, percussionPalpation, percussion
Health historyHealth history
– Previous UTIs, calculi, stasis, Previous UTIs, calculi, stasis, retention, pregnancy, STDs, retention, pregnancy, STDs, bladder cancerbladder cancer
– Meds: antibiotics, Meds: antibiotics, anticholinergics, antispasmodicsanticholinergics, antispasmodics
– Urologic instrumentationUrologic instrumentation
– Urinary hygieneUrinary hygiene
– Patterns of eliminationPatterns of elimination
Nursing Assessment Nursing Assessment of Urinary Tract Infection of Urinary Tract Infection
(UTI)(UTI) Nausea, vomiting, anorexia, Nausea, vomiting, anorexia,
chills, nocturia, frequency, chills, nocturia, frequency, urgencyurgency
Suprapubic or lower back Suprapubic or lower back pain, bladder spasms, pain, bladder spasms, dysuria, burning on urinationdysuria, burning on urination

Nursing Assessment Nursing Assessment of Urinary Tract Infection of Urinary Tract Infection
(UTI)(UTI) Objective dataObjective data
– FeverFever– Hematuria, foul-smelling urine; Hematuria, foul-smelling urine;
tender, enlarged kidneytender, enlarged kidney– Leukocytosis, positive findings for Leukocytosis, positive findings for
bacteria, WBCs, RBCs, pyuria, bacteria, WBCs, RBCs, pyuria, ultrasound, CT scan, IVPultrasound, CT scan, IVP

Diagnostic StudiesDiagnostic Studies
Renal scanRenal scan CystogramCystogram Retrograde Retrograde
pyelogrampyelogram UltrasoundUltrasound CTCT MRIMRI Renal arteriogramRenal arteriogram
UAUA Urine C&SUrine C&S BUNBUN CreatinineCreatinine KUBKUB IVPIVP VCG/VCUGVCG/VCUG

Normal UrinalysisNormal Urinalysis pH: 5 to 9pH: 5 to 9 Sp gr: 1.001 to 1.035Sp gr: 1.001 to 1.035 Protein: <20 mg/dlProtein: <20 mg/dl Urobilinogen: up to 1 Urobilinogen: up to 1
mg/dlmg/dl None of the None of the
following: following: – GlucoseGlucose – KetonesKetones – HgbHgb– WBCsWBCs
– RBCsRBCs– CastsCasts– NitritNitrit
ee

Normal Characteristics of Normal Characteristics of UrineUrine
Color rangeColor range ClearClear Newborn production—approx 1-2 Newborn production—approx 1-2
ml/kg/hr ml/kg/hr Child production—approx 1 Child production—approx 1
ml/kg/hrml/kg/hr
Urinary Tract Infection Urinary Tract Infection (UTI)(UTI)
Is it Is it reallyreally that that serious?serious?
Concept of Concept of “asymptomatic “asymptomatic bacteria” in urinary bacteria” in urinary tracttract

Urinary Tract Infection Urinary Tract Infection (UTI)(UTI)
CausesCauses Escherichia coliEscherichia coli most most
common pathogencommon pathogen StreptococciStreptococci Staphylococcus Staphylococcus
saprophyticussaprophyticus Occasionally fungal and Occasionally fungal and
parasitic pathogensparasitic pathogens

Classification of UTIClassification of UTI
Upper tract:Upper tract: involves renal involves renal parenchyma, pelvis, and parenchyma, pelvis, and uretersureters– Typically causes fever, chills, Typically causes fever, chills,
flank painflank pain Lower tract:Lower tract: involves lower involves lower
urinary tracturinary tract– Usually no systemic Usually no systemic
manifestationsmanifestations

Classification of UTIClassification of UTI Lower tractLower tract CystitisCystitis UrethritisUrethritis Glomerulo-Glomerulo-
nephritisnephritis
Upper tractUpper tract PyelonephritisPyelonephritis VURVUR

Classification of UTIClassification of UTI
Uncomplicated Uncomplicated infectioninfection
Complicated infectionsComplicated infections– StonesStones– ObstructionObstruction– CathetersCatheters– Diabetes or neurologic Diabetes or neurologic
diseasedisease– Recurrent infections Recurrent infections
Types of UTIsTypes of UTIs
Recurrent—repeated episodesRecurrent—repeated episodes Persistent—bacteriuria despite Persistent—bacteriuria despite
antibioticsantibiotics Febrile—typically indicates Febrile—typically indicates
pyelonephritispyelonephritis Urosepsis—bacterial illness; Urosepsis—bacterial illness;
urinary pathogens in bloodurinary pathogens in blood

Etiology and Etiology and Pathophysiology of UTIPathophysiology of UTI Physiologic and mechanical Physiologic and mechanical
defense mechanisms defense mechanisms maintain sterilitymaintain sterility– Emptying bladderEmptying bladder– Normal antibacterial Normal antibacterial
properties of urine and tractproperties of urine and tract– Ureterovesical junction Ureterovesical junction
competencecompetence– Peristaltic activityPeristaltic activity
Etiology and Pathophysiology Etiology and Pathophysiology of UTIof UTI
Alteration of defense Alteration of defense mechanisms increases mechanisms increases risk of UTIrisk of UTI
Organisms usually Organisms usually introduced via ascending introduced via ascending route from urethraroute from urethra
Less common routes Less common routes – BloodstreamBloodstream– Lymphatic systemLymphatic system

Etiology and Pathophysiology Etiology and Pathophysiology of UTIof UTI
Contributing factor: urologic Contributing factor: urologic instrumentationinstrumentation– Allows bacteria present in Allows bacteria present in
opening of urethra to enter opening of urethra to enter urethra or bladderurethra or bladder
Sexual intercourse promotes Sexual intercourse promotes “milking” “milking” of bacteria from perineum and of bacteria from perineum and vaginavagina– May cause minor urethral traumaMay cause minor urethral trauma

Etiology and Pathophysiology Etiology and Pathophysiology of UTIof UTI
UTIs rarely result from UTIs rarely result from hematogenous routehematogenous route
For kidney infection to For kidney infection to occur from hematogenous occur from hematogenous transmission, must have transmission, must have prior injury to urinary tractprior injury to urinary tract– Obstruction of ureterObstruction of ureter– Damage from stonesDamage from stones– Renal scarsRenal scars


Etiology and Pathophysiology Etiology and Pathophysiology of UTIof UTI
UTI is a common nosocomial UTI is a common nosocomial infectioninfection– Often Often E. coliE. coli– Seldom Seldom PseudomonasPseudomonas
Urologic instrumentation Urologic instrumentation common predisposing factorcommon predisposing factor
Clinical Manifestations of Clinical Manifestations of UTIUTI
Symptoms Symptoms – DysuriaDysuria– Frequent urination (>q2h)Frequent urination (>q2h)– UrgencyUrgency– Suprapubic discomfort or Suprapubic discomfort or
pressurepressure

Clinical Manifestations of Clinical Manifestations of UTIUTI
Urine may contain visible Urine may contain visible blood or sediment (cloudy blood or sediment (cloudy appearance)appearance)
Flank pain, chills, and fever Flank pain, chills, and fever indicate infection of upper indicate infection of upper tract (pyelonephritis)tract (pyelonephritis)

Pediatric ManifestationsPediatric Manifestations
FrequencyFrequency Fever in some casesFever in some cases Odiferous urineOdiferous urine Blood or blood-tinged Blood or blood-tinged
urineurine Sometimes NO symptoms Sometimes NO symptoms
except generalized sepsisexcept generalized sepsis

Pediatric ManifestationsPediatric Manifestations
Pediatric patients with Pediatric patients with significant bacteriuria may significant bacteriuria may have no symptoms or have no symptoms or nonspecific symptoms like nonspecific symptoms like fatigue or anorexiafatigue or anorexia
So how do you find out?So how do you find out?

Diagnostic Studies of UTIDiagnostic Studies of UTI Dipstick Dipstick Microscopic Microscopic
urinalysisurinalysis Culture Culture

Diagnostic Studies of UTIDiagnostic Studies of UTI
Clean-catch is preferredClean-catch is preferred U-bag for collection from childU-bag for collection from child Specimen obtained by Specimen obtained by
catheterization or suprapubic catheterization or suprapubic needle aspiration has more needle aspiration has more accurate resultsaccurate results– May be necessary when clean-May be necessary when clean-
catch cannot be obtainedcatch cannot be obtained
Diagnostic Studies of UTIDiagnostic Studies of UTI
Sensitivity testing determines Sensitivity testing determines susceptibility to antibioticssusceptibility to antibiotics
Imaging studies for suspected Imaging studies for suspected obstruction obstruction – IVP or Abd CT IVP or Abd CT

Collaborative Care for UTI Collaborative Care for UTI Drug Therapy: AntibioticsDrug Therapy: Antibiotics
Uncomplicated cystitis: Uncomplicated cystitis: short-term course of short-term course of antibioticsantibiotics
Complicated UTIs: long-term Complicated UTIs: long-term treatmenttreatment
Collaborative Care for Collaborative Care for UTI UTI
Drug Therapy: Drug Therapy: AntibioticsAntibiotics
Trimethoprim-sulfamethoxazole Trimethoprim-sulfamethoxazole (TMP-SMX) or nitrofurantoin(TMP-SMX) or nitrofurantoin
AmoxicillinAmoxicillin CephalexinCephalexin Others Others
– Gentamycin, carbenicillin Gentamycin, carbenicillin ++++
Pyridium (OTC)Pyridium (OTC) Combination agents (e.g., Urised) Combination agents (e.g., Urised)
used to relieve painused to relieve pain– Preparations with methylene blue Preparations with methylene blue
tinttint

Collaborative Care for Collaborative Care for UTI UTI
Drug TherapyDrug Therapy For repeated UTIsFor repeated UTIs– Prophylactic or suppressive Prophylactic or suppressive
antibiotics antibiotics – TMP-SMX administered daily TMP-SMX administered daily
to prevent recurrence or to prevent recurrence or single dose before events single dose before events likely to cause UTIlikely to cause UTI
Etiology and Etiology and Pathophysiology Pathophysiology
of Acute Pyelonephritisof Acute Pyelonephritis Inflammation caused by Inflammation caused by bacteria, fungi, protozoa, or bacteria, fungi, protozoa, or viruses infecting kidneysviruses infecting kidneys
Urosepsis: systemic Urosepsis: systemic infection from urologic infection from urologic sourcesource– Can lead to septic shock and Can lead to septic shock and
death in 15% of casesdeath in 15% of cases

Etiology and Etiology and Pathophysiology Pathophysiology
of Acute Pyelonephritisof Acute Pyelonephritis Usually infection Usually infection is via ascending is via ascending urethral routeurethral route
Frequent causes Frequent causes – E. coliE. coli– ProteusProteus– KlebsiellaKlebsiella– EnterobacterEnterobacter

Etiology and Etiology and Pathophysiology Pathophysiology
of Acute Pyelonephritisof Acute Pyelonephritis Commonly starts in renal Commonly starts in renal medulla and spreads to medulla and spreads to adjacent cortexadjacent cortex
Recurring episodes lead to Recurring episodes lead to scarred, poorly functioning scarred, poorly functioning kidney and chronic kidney and chronic pyelonephritispyelonephritis

Clinical Manifestations Clinical Manifestations of Acute Pyelonephritis of Acute Pyelonephritis Vary from mild to “classic” and very severeVary from mild to “classic” and very severe
Presenting symptomsPresenting symptoms
– N/V, anorexia, chills, nocturia, frequency, N/V, anorexia, chills, nocturia, frequency, urgencyurgency
– Suprapubic or low back pain, dysuriaSuprapubic or low back pain, dysuria
– Fever, hematuria, foul-smelling urineFever, hematuria, foul-smelling urine
Costovertebral tenderness Costovertebral tenderness
Symptoms often subside in a few days, Symptoms often subside in a few days, even without therapyeven without therapy
– Bacteriuria and pyuria still persistBacteriuria and pyuria still persist

Diagnostic Studies Diagnostic Studies of Acute Pyelonephritis of Acute Pyelonephritis
UrinalysisUrinalysis WBC casts WBC casts CBCCBC Imaging studies Imaging studies
(IVP or CT)(IVP or CT) UltrasoundUltrasound

Collaborative Care Collaborative Care of Acute Pyelonephritis of Acute Pyelonephritis
Hospitalization Hospitalization Parenteral Parenteral
antibioticsantibiotics

Collaborative Care Collaborative Care of Acute Pyelonephritisof Acute Pyelonephritis
Relapses treated with 6-Relapses treated with 6-week course of antibioticsweek course of antibiotics
Reinfections treated as Reinfections treated as individual episodes or individual episodes or managed with long-term managed with long-term therapytherapy– Prophylaxis may be used for Prophylaxis may be used for
recurrent infectionsrecurrent infections

Types of Types of GlomerulonephritisGlomerulonephritis
Most are postinfectiousMost are postinfectious– Pneumococcal, Pneumococcal,
streptococcal, or viralstreptococcal, or viral May be distinct entity May be distinct entity oror May be a manifestation of May be a manifestation of
systemic disordersystemic disorder– SLESLE– Sickle cell diseaseSickle cell disease– OthersOthers

Glomerulonephritis Glomerulonephritis SymptomsSymptoms
Generalized edema due to Generalized edema due to decreased glomerular decreased glomerular filtrationfiltration– Begins with periorbitalBegins with periorbital– Progresses to lower extremities Progresses to lower extremities
and then to ascitesand then to ascites HTN due to increased ECFHTN due to increased ECF OliguriaOliguria

Glomerulonephritis Glomerulonephritis Symptoms Symptoms
HematuriaHematuria– Bleeding in upper urinary Bleeding in upper urinary
tract→smoky urinetract→smoky urine ProteinuriaProteinuria
– Increased amount of protein = Increased amount of protein = increased severity of renal increased severity of renal diseasedisease

Acute Post-Streptococcal Acute Post-Streptococcal GlomerulonephritisGlomerulonephritis
Is a noninfectious renal diseaseIs a noninfectious renal disease– Autoimmune Autoimmune
Onset 5 to 12 days after Onset 5 to 12 days after otherother type of type of infection infection
Often group A ß-hemolytic streptococciOften group A ß-hemolytic streptococci Most common in 6 to 7 years oldMost common in 6 to 7 years old Uncommon in <2 years oldUncommon in <2 years old Can occur at any ageCan occur at any age

Diagnosing Diagnosing APSGAPSG

PrognosisPrognosis
95%—rapid improvement to 95%—rapid improvement to complete recoverycomplete recovery
5% to 15%—chronic 5% to 15%—chronic glomerulonephritisglomerulonephritis
1%—irreversible damage1%—irreversible damage

Nursing Management of Nursing Management of APSGAPSG
Manage edemaManage edema– Daily weightsDaily weights– Accurate I&OAccurate I&O– Daily abdominal girthDaily abdominal girth
NutritionNutrition– Low sodium, low to Low sodium, low to
moderate proteinmoderate protein Susceptibility to Susceptibility to
infectionsinfections Bed rest is not necessaryBed rest is not necessary

Nephrotic SyndromeNephrotic Syndrome
Most common presentation of Most common presentation of glomerular injury in childrenglomerular injury in children
CharacteristicsCharacteristics– ProteinuriaProteinuria– HypoalbuminemiaHypoalbuminemia– HyperlipidemiaHyperlipidemia– EdemaEdema– Massive urinary protein lossMassive urinary protein loss

Types of Nephrotic Types of Nephrotic SyndromeSyndrome
Minimal change nephrotic Minimal change nephrotic syndrome (MCNS)syndrome (MCNS)– AKAAKA
Idiopathic nephrosisIdiopathic nephrosis Nil diseaseNil disease Uncomplicated nephrosisUncomplicated nephrosis Childhood nephrosisChildhood nephrosis Minimal lesion nephrosisMinimal lesion nephrosis
Congenital nephrotic syndromeCongenital nephrotic syndrome Secondary nephrotic syndromeSecondary nephrotic syndrome

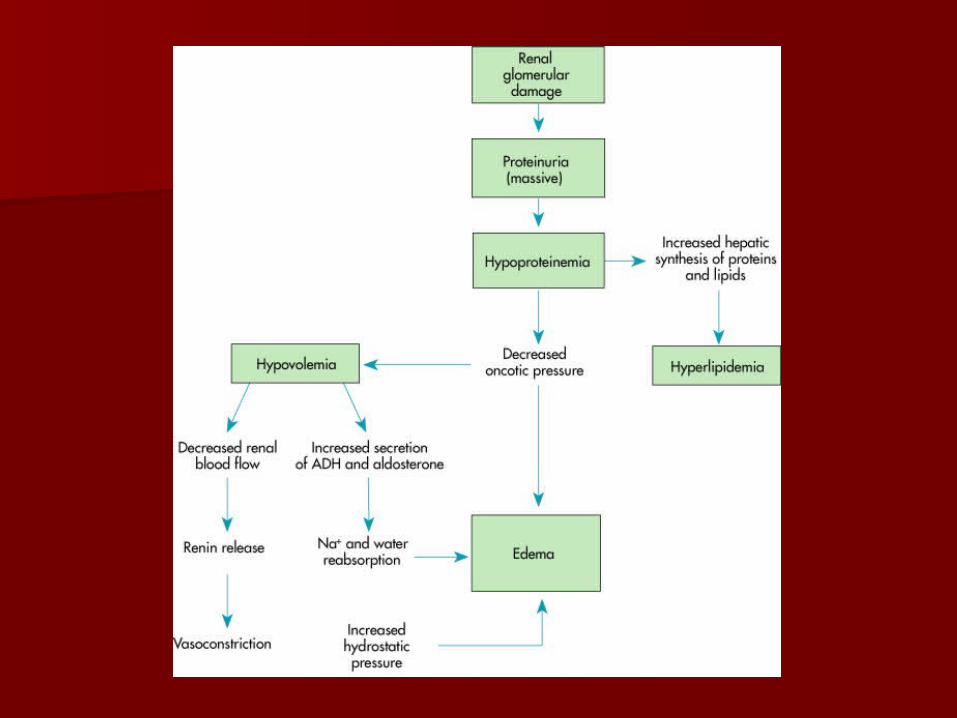
Changes in Nephrotic Changes in Nephrotic SyndromeSyndrome
Glomerular membraneGlomerular membrane– Normally impermeable to large Normally impermeable to large
proteinsproteins– Becomes permeable to proteins, Becomes permeable to proteins,
especially albuminespecially albumin– Albumin lost in urine Albumin lost in urine
(hyperalbuminuria)(hyperalbuminuria)– Serum albumin decreased Serum albumin decreased
(hypoalbuminemia)(hypoalbuminemia)– Fluid shifts from plasma to interstitial Fluid shifts from plasma to interstitial
spacesspaces HypovolemiaHypovolemia AscitesAscites
Nephrotic Syndrome Nephrotic Syndrome ManagementManagement
Supportive careSupportive care DietDiet
– Low to moderate protein Low to moderate protein – Sodium restrictions when Sodium restrictions when
large amount edema presentlarge amount edema present SteroidsSteroids
– 2 mg/kg divided into BID doses2 mg/kg divided into BID doses– Prednisone drug of choice ($$ Prednisone drug of choice ($$
and safest)and safest) Immunosuppressant therapy Immunosuppressant therapy
(Cytoxan)(Cytoxan) DiureticsDiuretics

Family IssuesFamily Issues
Chronic condition with Chronic condition with relapsesrelapses
Developmental milestonesDevelopmental milestones Social isolation Social isolation
– Lack of energyLack of energy– Immunosuppression/protectionImmunosuppression/protection– Change in appearance due to Change in appearance due to
edemaedema– Self-imageSelf-image

Nursing InterventionsNursing Interventions
Aseptic technique during Aseptic technique during catheterizationscatheterizations
Avoid unnecessary Avoid unnecessary catheterization and early removal catheterization and early removal of indwelling cathetersof indwelling catheters
Prevents nosocomial infections Prevents nosocomial infections
– Wash hands before and after contactWash hands before and after contact– Wear gloves for care of urinary Wear gloves for care of urinary
systemsystem
Nursing InterventionsNursing Interventions
Routine and thorough perineal Routine and thorough perineal care for all hospitalized patientscare for all hospitalized patients
Avoid incontinent episodes by Avoid incontinent episodes by answering call light and offering answering call light and offering bedpan at frequent intervalsbedpan at frequent intervals

Nursing InterventionsNursing Interventions
Ensure adequate fluid intake Ensure adequate fluid intake (patient with urinary problems may (patient with urinary problems may think will be more uncomfortable)think will be more uncomfortable) – Dilutes urine, making bladder less Dilutes urine, making bladder less
irritableirritable– Flushes out bacteria before they can Flushes out bacteria before they can
colonizecolonize– Avoid caffeine, alcohol, citrus juices, Avoid caffeine, alcohol, citrus juices,
chocolate, and highly spiced foodschocolate, and highly spiced foods Potential bladder irritantsPotential bladder irritants
Nursing InterventionsNursing Interventions
Discharge to home instructionsDischarge to home instructions Follow-up urine cultureFollow-up urine culture
Recurrent symptoms typically occur in 1 Recurrent symptoms typically occur in 1 to 2 weeks after therapyto 2 weeks after therapy
– Encourage adequate fluids even after Encourage adequate fluids even after infectioninfection
– Low-dose, long-term antibiotics to Low-dose, long-term antibiotics to prevent relapses or reinfectionsprevent relapses or reinfections
– Explain rationale to enhance Explain rationale to enhance compliancecompliance

Hemolytic-Uremic Hemolytic-Uremic SyndromeSyndrome
PathophysiologyPathophysiology Diagnostic Diagnostic
evaluationevaluation Therapeutic Therapeutic
managementmanagement PrognosisPrognosis Nursing Nursing
considerationconsideration

Wilms’ Tumor Wilms’ Tumor
EtiologyEtiology Diagnostic evaluationDiagnostic evaluation Therapeutic Therapeutic
managementmanagement– Surgical removalSurgical removal– Chemotherapy and/or Chemotherapy and/or
radiationradiation Nursing considerationsNursing considerations

Renal FailureRenal Failure
Acute renal failure Acute renal failure (ARF)(ARF)
Chronic renal failure Chronic renal failure (CRF)(CRF)

Acute Renal Failure Acute Renal Failure (ARF)(ARF)
Definition: kidneys suddenly unable to Definition: kidneys suddenly unable to regulate volume and composition of regulate volume and composition of urineurine
Not common in childrenNot common in children Principal feature is oliguria Principal feature is oliguria
– Associated with azotemia, metabolic Associated with azotemia, metabolic acidosis, and electrolyte disturbancesacidosis, and electrolyte disturbances
Most common pathologic cause: Most common pathologic cause: transient renal failure resulting from transient renal failure resulting from severe dehydrationsevere dehydration

Acute Renal Failure Acute Renal Failure (ARF)(ARF)
Pathophysiology—usually Pathophysiology—usually reversiblereversible
Diagnostic evaluationDiagnostic evaluation Therapeutic managementTherapeutic management Nursing considerationsNursing considerations

Complications of ARFComplications of ARF
HyperkalemiaHyperkalemia HypertensionHypertension AnemiaAnemia SeizuresSeizures HypervolemiaHypervolemia Cardiac failure with Cardiac failure with
pulmonary edemapulmonary edema

Chronic Renal Failure Chronic Renal Failure (CRF)(CRF)
Begins when diseased kidneys Begins when diseased kidneys cannot maintain normal cannot maintain normal chemical structure of body chemical structure of body fluidsfluids
Clinical syndrome called Clinical syndrome called uremiauremia

Potential Causes of CRFPotential Causes of CRF
Congenital renal and Congenital renal and urinary tract malformationsurinary tract malformations
VUR associated with VUR associated with recurrent UTIsrecurrent UTIs
Chronic pyelonephritisChronic pyelonephritis Chronic glomerulonephritisChronic glomerulonephritis
CRF (cont’d)CRF (cont’d)
PathophysiologyPathophysiology Diagnostic evaluationDiagnostic evaluation Therapeutic management Therapeutic management
– Manage diet, hypertension, Manage diet, hypertension, recurrent infections, recurrent infections, seizures seizures
Nursing considerationsNursing considerations

DialysisDialysis Peritoneal Peritoneal
dialysisdialysis HemodialysisHemodialysis HemofiltratioHemofiltratio
nn

Peritoneal DialysisPeritoneal Dialysis The preferred method of dialysis for The preferred method of dialysis for
childrenchildren Abdominal cavity acts as Abdominal cavity acts as
semipermeable membrane for semipermeable membrane for filtrationfiltration
Can be managed at home in some Can be managed at home in some casescases
Warmed solution enters peritoneal Warmed solution enters peritoneal cavity by gravity, remains for cavity by gravity, remains for period of time before removalperiod of time before removal

HemodialysisHemodialysis
Requires creation of a vascular Requires creation of a vascular access and special dialysis access and special dialysis equipmentequipment
Best suited for children who Best suited for children who can be brought to facility 3 can be brought to facility 3 times/week for 4 to 6 hourstimes/week for 4 to 6 hours
Achieves rapid correction of Achieves rapid correction of fluid and electrolyte fluid and electrolyte abnormalitiesabnormalities

TransplantationTransplantation From living related donorFrom living related donor From cadaver donorFrom cadaver donor Primary goal is LT survival of Primary goal is LT survival of
grafted tissuegrafted tissue Role of immunosuppressant Role of immunosuppressant
therapytherapy