nurse prescribers extended formulary ... list of poms, alone or in combination. the list of poms is...
TRANSCRIPT

To: Interested Organisations
020 7084 2642
020 7084 2121
Our reference: MLX 303Date: 14 April 2004
Dear Sir/Madam
NURSE PRESCRIBERS EXTENDED FORMULARY: PROPOSALS TO EXPAND THERANGE OF PRESCRIPTION ONLY MEDICINES
INTRODUCTION1. We are writing to consult you in accordance with section 129(6) of the Medicines Act1968 about proposals to expand the range of prescription only medicines (POMs) that may beprescribed by Extended Formulary Nurse Prescribers, as set out in Schedule 3A to thePrescription Only Medicines (Human Use) Order 1997 (known as the Nurse Prescribers'Extended Formulary). This would be achieved by amendment to the Prescription OnlyMedicines (Human Use) Order 1997 (“the POM Order”) and the NPEF.
2. This consultation letter has been produced jointly by the Medicines and Healthcareproducts Regulatory Agency (MHRA) and the Department of Health and also seeks views on awider range of conditions treatable by Extended Formulary Nurse Prescribers. This consultationis also being circulated in Wales, Scotland and Northern Ireland. This consultation abides by thesix consultation criteria as set out in the revised Code of Practice on Consultation published bythe Cabinet Office (www.cabinet-office.gov.uk/regulation/Consultation/Code.htm).
APPLICATION TO ENGLAND, WALES, SCOTLAND AND NORTHERN IRELAND3. The proposed changes to the POM Order would apply throughout the United Kingdom.However, the pace at which extended formulary nurse prescribing develops and thearrangements for appropriate training within national health organisations, are matters for eachof the separate administrations. Extended formulary nurse prescribing introduced byorganisations providing health care outside the NHS would have to comply with the legislativerequirements and those organisations should also consider developing accompanying guidance.
NURSE PRESCRIBERS EXTENDED FORMULARY: BACKGROUND TOPROPOSALS TO EXPAND THE RANGE OF PRESCRIPTION ONLY MEDICINES 4. Since April 2002, Extended Formulary Nurse Prescribers (EFNPs), who havesuccessfully completed a programme of preparation and training, are able to prescribe from a

specific list of POMs, alone or in combination. The list of POMs is set out in Schedule 3A tothe POM Order and is known as the Nurse Prescribers' Extended Formulary (NPEF). The NPEFwas expanded in January 2004. EFNPs are currently able to prescribe for a range of medicalconditions which are set out in the British National Formulary and Drug Tariff and which forconvenience are appended at Annex A.
5. As part of the previous consultation (MLX 293 – April 2003) on the expansion of theNPEF, a number of controlled drugs were proposed for the treatment of myocardial infarctionand for palliative care. As outlined in that consultation the inclusion of any controlled drugs alsorequires amendment to the Misuse of Drugs Regulations 2001 (SI 3998/2001) which are theresponsibility of the Home Office. The Home Office would need to consider the advice of theAdvisory Council on the Misuse of Drugs before considering such a change to the 2001Regulations. These discussions are ongoing at the date of this MLX.
6. Also as part of the previous consultation, the advice of the Committee on Safety ofMedicines (CSM) was sought on the principle of including, on an exception basis, appropriateBlack Triangle medicines in the NPEF. The CSM had agreed that continuing the exclusion ofBlack Triangle products was over-restrictive. These are licensed products, and Black Trianglestatus relates to the requirement for intense reporting of adverse drug reactions (ADRs). Sincethe original NPEF was introduced, all nurses have become reporters of ADRs, so there was noconcern that ADRs for Black Triangle products would go unreported. This is mentioned here inthe context of several proposals in this consultation which propose the inclusion of substanceswhich currently have Black Triangle status.
7. From Autumn 2003, proposals to further expand the NPEF and the range of conditionstreatable by EFNPs were considered by a joint Working Group of the Committee on Safety ofMedicines (CSM) and the Medicines Commission (referred to from now on as the PrescribingWG). These proposals build on the work of the DH Emergency Care Strategy Team (ECST) todevelop procedures and new working practices aimed at improving patient experience andclinical outcomes. Increasingly, experienced nurses and advanced nurse practitioners are able tocomplete all the components of care within their competence. Nurses are supporting the plannedextension of Walk-in-Centres, improving and maintaining arrangements for providing primarycare Out-of Hours services and helping to reduce unnecessary burdens on ambulance servicesand Accident and Emergency Departments. By increasing the range of medications included inthe NPEF, trained independent nurse prescribers will, in appropriate circumstances, be able toprovide comprehensive care for patients - without the need for inappropriate or unnecessaryreference to medical colleagues.
PROPOSALS8. Proposed additions to the conditions currently treatable under the NPEF: It isproposed to expand the range of medical conditions that EFNPs can diagnose and manage(Annex A) to include:
Central Nervous System� acute dystonias � acute severe pain after trauma � changing painful dressings � emergency treatment of meningitis � nausea and vomiting (outside palliative care)� prophylaxis and treatment of nausea and vomiting in the postoperative period

� generalised tonic-clonic seizures
Circulatory� acute pulmonary oedema associated with cardiac failure� angina pectoris � fluid replacement and potassium replacement (hypovolaemia and dehydration) � plasma substitutes for patients with a low blood volume � “Thromboprophylaxis” - defined as deep vein thrombosis, acute coronary syndrome,
congestive heart failure in bed-bound patients, and perioperatively � ventricular fibrillation or pulseless ventricular tachycardia
Eye� Ophthalmic conditions - diagnostic use in ophthalmology, tear deficiency,
inflammation following ophthalmic surgery, corneal trauma
Gastrointestinal conditions� prophylaxis of acid aspiration during surgery.
Infections� cellulitis (defined as treatment for ascending cellulitis of the leg, to be distinguished
from inflammation associated with varicose ulcers).� tetanus treatment
Musculoskeletal� pain and inflammation/soft tissue injury
Oral conditions � dental infections
Poisoning� poisoning
Respiratory� acute exacerbation of chronic bronchitis� acute reversible airways obstruction (acute severe asthma or acute exacerbation of
chronic obstructive pulmonary disease) � anaphylaxis� conditions requiring oxygen supplementation (e.g. hypoxaemia) � croup
Skin� psoriasis� molluscum contagiosum
Substance Dependence� acute alcohol withdrawal

9. It should be remembered that Pharmacy (P) and General Sales List (GSL) productsrelevant to a condition also become prescribable (with certain limitations within the NHS) byEFNPs when that condition is added to the NPEF.
10. We would welcome views on the proposals to extend the range of conditionstreatable by EFNPs.
11. Proposed extension, in restricted circumstances, of “off label” or “off licence”prescribing: The CSM has advised that, in palliative care where it is in the best interests of thepatient, certain medicines may be prescribed for use outside the licensed indications for thatmedicine (commonly known as “off label” or “off licence” prescribing. For clarification, thisdoes not include the prescribing of medicines that are not licensed in the UK). A number ofproposals set out in paragraphs 13 and 14 below propose a further extension, in restrictedcircumstances, of “off label” or “off licence prescribing. We would welcome views on thisproposal.
12. Proposed extension of the prescribing of controlled drugs: The proposals at paragraph13, highlighted by a hash (#), contain some substances that are listed as controlled drugs underthe Misuse of Drugs Regulations 2001 (SI 3998/2001). Their inclusion in the NPEF will requirean amendment to the 2001 Regulations, which are the responsibility of the Home Office. TheHome Office would need to consider the advice of the Advisory Council on the Misuse of Drugsbefore considering such a change to the 2001 Regulations. We would welcome comments onthe proposal to include these controlled drugs in the NPEF.
13. Proposed amendments to the POM Order (see also paragraph 14): The proposedadditions to the POM Order are marked with an asterisk (*) which relates either to a newsubstance or to a proposed new route of administration. The treatments areas shown in the firstcolumn will not form part of the POM Order and will instead be subject to guidance. (Forconvenience, substances currently in the POM Order and proposed for new conditions are alsoincluded in the table below, without an asterisk.) Where appropriate and for clarification, theviews of the Prescribing WG or the views of the CSM Paediatric Working Group are alsoincluded. The proposals have yet to be considered by the CSM and this will occur after thisconsultation (see also paragraph 20). Views on the proposals set out below are welcome.
Treatment area Substance Requirements as to use,route of administration,or pharmaceutical form
nausea and vomiting Cyclizine hydrochloride* Cyclizine lactate*Metoclopramide Prochlorperazine mesilate* Prochlorperazine maleate*
oral parenteraloral and parenteral oral and rectaloral and rectal
The Prescribing WG were not supportive of the prescribing of metoclopramide for young people(as per the BNF) but did not object in principle to its inclusion in the NPEF for this conditionoutside of palliative care and recommended that the treatment of nausea and vomiting need nolonger be restricted to palliative care.

acute myocardial infarction Alteplase*Reteplase *Streptokinase*Tenecteplase*
}} parenteral}}
The Prescribing WG noted that paramedics can already, or will shortly be able to, administerstreptokinase, tenecteplase, and reteplase. In some instances paramedics will be accompanied byEFNPs, or might seek advice from EFNPs on the use of such medicines. It was thereforeappropriate that EFNPs should be able to prescribe these substances. The WG furtherrecommended that DH guidance should make it clear that where these substances were to beadministered, resuscitation facilities were essential. The WG noted that tenecteplase has “BlackTriangle” status.
Anaphylaxis Adrenaline* Chlorphenamine*Hydrocortisone sodium succinate*
}} parenteral}
The Prescribing WG noted that the parenteral administration of Adrenaline (1 mg in 1 ml),Chlorphenamine and Hydrocortisone are among those substances listed under Article 7 of thePOM Order for administration by anyone in an emergency for the purpose of saving life. TheWG recommended that EFNPs should also be able to prescribe for anaphylaxis, and thatadrenaline and chlorphenamine should be added to the NPEF.
Acute pulmonary oedemaassociated with cardiacfailure
Furosemide* oral and parenteral
ventricular fibrillation orpulseless ventriculartachycardia
Amiodarone* parenteral
The Prescribing WG were aware of a proposed consultation [NB: now published as MLX 302 on24 March 2004] to add intravenous amiodarone to the list of substances that paramedics canadminister on their own initiative for the treatment of sick and injured persons. As thatconsultation proposes the administration of intravenous amiodarone for ventricular fibrillation orpulseless ventricular tachycardia, the WG recommended that the same proposal be made for theNPEF.
“Thromboprophylaxis” -for conditions defined asdeep vein thrombosis(DVT), acute coronarysyndrome, congestive heartfailure in bed-boundpatients, andperioperatively.
Certoparin sodium*Dalteparin sodium*Enoxaparin*Reviparin sodium* Tinzaparin sodium*
}}} parenteral}}

In recommending the inclusion of these substances to the NPEF for the treatment of theconditions specified, the Prescribing WG were aware that while all the substances mentionedwere licensed for prophylaxis, not all were licensed for the treatment of deep vein thrombosis.(The WG also recommended that EFNPs be able to prescribe dispersible aspirin for myocardialinfarction and suspected myocardial infarction and angina pectoris, but not DVT.)
acute reversible airwaysobstruction (acute severeasthma or acuteexacerbation of chronicobstructive pulmonarydisease)
Hydrocortisone sodium succinateIpratropium bromide*
parenteralinhalation
The Prescribing WG noted that the parenteral administration of Hydrocortisone is among thosesubstances listed under Article 7 of the POM Order for administration by anyone in anemergency for the purpose of saving life. The WG recommended that EFNPs should also be ableto prescribe parenteral Hydrocortisone and that it should be added to the NPEF.
Acute exacerbation ofchronic bronchitis
Oxytetracycline dihydrate oral
acute severe pain aftertrauma
Morphine*# parenteral, oral andrectal
The Paediatric WG fully supported the need for adequate pain relief for children although thatcould involve off-label use. However, other than major trauma, the WG considered that theNPEF should not cover the prescribing of intravenous opiates to a neonate or young child in theabsence of a definitive diagnosis. Nor could the WG envisage a situation in a Walk-in Centre orAccident and Emergency situation which would require an EFNP to prescribe slow-releaseMorphine.
pain and inflammation/softtissue injury
Diclofenac sodium oral
EFNPs can already treat pain and inflammation/soft tissue injury and Diclofenac sodium (oraland rectal routes of administration) is already included in the NPEF. The NPEF does notdifferentiate between prescribing for adults, adolescents or children. The Paediatric WG was,however, doubtful of the benefit of prescribing Diclofenac sodium in the context of emergencyor first contact care as Paracetamol and Ibuprofen would provide adequate initial cover.
generalised tonic–clonicseizures
Diazepam*#
Lorazepam*# Midazolam*#
parenteral, oral andrectalparenteral parenteral, buccal
Croup Budesonide* Dexamethasone sodium phosphate*
inhalationoral
The Paediatric WG noted that the proposed single dose of Dexamethasone sodium phosphate –Oral would be an ‘off-label’ use.

Local analgesia (other thanfor ophthalmic conditions)when procedure requires it
Prilocaine* Tetracaine*
external and parenteralexternal
acute alcohol withdrawal Chlordiazepoxide hydrochloride*Diazepam*#
oralparenteral, oral andrectal
fluid replacement(hypovolaemia anddehydration)
Glucose 5% and 10%*Sodium chloride 0.9%*Sodium chloride 0.9% & Glucose 5%*Sodium chloride 0.18% & Glucose 4%*
}}parenteral}}
potassium replacement(hypokalaemia)
Glucose 5% with Potassium + 40mmol/L readymade infusion bag*
Sodium chloride 0.9% with Potassium + 40mmol/Lready made infusion bag*
}}}parenteral}}
The Prescribing WG advised, in the interests of patient safety and in line with guidance from theNational Patient Safety Agency, that ready made potassium-containing infusions should beprescribed.
diagnostic use inophthalmology
Fluorescein* Tropicamide* Oxybuprocaine hydrochloride*Proxymetacaine hydrochloride*Tetracaine hydrochloride* (see below)
}}}ophthalmic drops}}
The Prescribing WG expressed reservations about the use of tetracaine, as it can be disruptive tothe corneal epithelium, and recommended that this should only be used when other agents arejudged insufficiently powerful. This matter will be considered further by the CSM in duecourse.
tear deficiency Acetylcysteine* ophthalmic drops
The Prescribing WG considered that it could be difficult to determine when acetylcysteine (asopposed to one of the other tear supplements, such as non-POM artificial tears) was indicated.This matter will be considered further by the CSM in due course.
inflammation followingophthalmic surgery
Diclofenac sodium* Ophthalmic drops
corneal trauma Diclofenac sodium* Ophthalmic drops
tetanus treatment Tetanus immunoglobulin* parenteral

prophylaxis of acidaspiration during surgery
Cimetidine* Omeprazole*Omeprazole sodium* Ranitidine*
parenteral oral parenteralparenteral
prophylaxis and treatmentof nausea and vomiting inthe postoperative period.
Granisetron hydrochloride*Ondansetron hydrochloride*Tropisetron hydrochloride*
parenteraloral and parenteralparenteral
plasma substitutes forpatients with a low bloodvolume (e.g. in cases ofshock arising from burns orsepticaemia).
Gelatin 3.5–4%*Dextran 70*Etherified starch (hexastarch,hydroxyethyl starch and Pentastarch)*
}}parenteral}
acute dystonias Benzatropine mesilate* parenteral
psoriasis Calcipotriol*Calcitriol*Tacalcitol*
external externalexternal
molluscum contagiosum Salicylic acid* external
The Prescribing WG noted that in clinical terms molluscum contagiosum are similar to warts andvery common in children especially pre-school age. They can resolve spontaneously but the timeit takes is variable. Only a few treatments are useful, mainly salicylic acid but this is notspecifically indicated for Molluscum contagiosum. The WG did not object in principle to theinclusion of this condition in the NPEF, appreciating that this would involve “off label”prescribing.
vaccine to protect travellersagainst meningococcalinfection
Meningococcal PolysaccharideVaccine A, C, W135 and Y*
parenteral
The Prescribing WG noted the views of the JCVI in 2003 which recommended that travellers inthe recognised risk groups intending to visit high risk areas should be offered the “ACWY”vaccine, which gives protection against meningitis strains A, C, W and Y. The WG thereforerecommended the inclusion of Meningococcal Polysaccharide Vaccine A, C, W135 and Y in theNPEF.
Flushing cannulae Sodium chloride 0.9%* parenteral
Reconstitution of injections Sodium chloride 0.9%* parenteral
14. Further proposed amendments to the POM Order concerning antimicrobials: Inconsidering the following proposals, the Prescribing WG were advised by the Specialist

Advisory Committee on Antimicrobial Resistance (SACAR). Antimicrobial drugs are the onlymedicines that commonly have effects beyond the immediate patient. Antimicrobial drugresistance remains a world-wide problem and in the UK led to the 2000 House of Lords Reporton Antimicrobial Resistance, in which it had been concluded that antimicrobial drug resistancewas a “major threat to public health”. Evidence published in recent years suggests that for somecommon conditions, (such as throat infections, otitis media, sinusitis and bronchitis),antibacterial drugs often afford little benefit to patients. Some concern remains that anexpansion of the numbers of prescribers will lead to an increase in antimicrobial prescribing. ThePrescribing WG have reached the following recommendations on the basis of the assumptionthat Extended Formulary Nurse Prescribing will not lead to an overall increase in antimicrobialprescribing. This assumption may be confirmed by the current evaluation of Extended FormularyNurse Prescribing being undertaken by the University of Southampton, although a report will notbe available until late autumn 2004 and would be based on the current more limited list ofantimicrobial drugs in the NPEF. Views on the proposals set out below are welcome.
dental infections Amoxicillin trihydrate Erythromycin Erythromycin stearateErythromycin ethyl succinate
oraloral oraloral
The Prescribing WG were less convinced that the prescribing of metronidazole andmetronidazole benzoate (oral and rectal) should be extended to dental infections. This matterwill be considered further by the CSM in due course.
acute exacerbation ofchronic bronchitis
Amoxicillin trihydrate Erythromycin Erythromycin stearateErythromycin ethyl succinate
oraloral oraloral
cellulitis ( as defined inparagraph 8)
Benzylpenicillin sodium*Erythromycin Erythromycin stearateErythromycin ethyl succinateFlucloxacillin*
parenteraloral oraloraloral and parenteral
emergency treatment ofmeningitis
Benzylpenicillin sodium* parenteral
PROPOSALS NOT RECOMMENDED FOR INCLUSION IN THE NPEF.15. The Prescribing WG considered a number of further proposals for inclusion in the NPEFthat they were inclined not to recommend. These will also be considered by the CSM in duecourse. Views are welcome.
Bacterial tonsillitis - Phenoxymethylpenicillin potassium - oralAs outlined above, SACAR had advised that the treatment of many conditions was beingreviewed to identify when antimicrobial drugs were really required. Tonsillitis, as an example,had been routinely treated with antibiotics in the past, but it was now recognised that antibiotics

were usually inappropriate unless there were pyogenic complications. The Prescribing WGrecommended that no antimicrobial drug be included in the NPEF for the treatment of tonsillitis.
Uncomplicated community-acquired pneumonia - Erythromycin – oral In addition to views concerning the prescribing of antimicrobial drugs, the WG considered that community-acquired pneumonia was not straightforward to diagnose without investigation andtherefore inappropriate in an emergency/first contact context.
Psoriasis - Tazarotene – external The Prescribing WG did not support the inclusion of tazarotene on the basis that it was contra-indicated in pregnancy and not one of the first line choices for the topical treatment of psoriasis.
Rosacea - Metronidazole - externalIn addition to discussion with SACAR, the Prescribing WG considered that Rosacea is oftenless easily diagnosed, (i.e. less easily differentiated from other diseases some of which may bedermatological manifestations of significant systemic diseases), than say acne vulgaris. The WGwas therefore reluctant to recommend the inclusion of Rosacea in the NPEF.
Prevention of ischaemic events - Clopidogrel hydrogen sulphate – oralThe proposal had been made in the context of EFNPs providing emergency/first contact care.However, the BNF carries a caution for the use of clopidogrel for the first few days after amyocardial infarction or ischaemic stroke and the Prescribing WG could not thereforerecommend its inclusion in the NPEF.
Cardiopulmonary resuscitation - adrenaline acid tartrate and atropine sulphate -parenteralAdrenaline (1 mg in 1 ml) and atropine are listed under Article 7 of the POM Order assubstances that can be administered in an emergency for the purpose of saving life. It was nottherefore necessary to add these substances to the NPEF in order that nurses could administerthem. The Prescribing WG could not envisage circumstances in which nurses would need toprescribe these drugs for dispensing to a patient. The WG concluded therefore that that theaddition of adrenaline and atropine to the NPEF for the purpose of cardiopulmonary resuscitationwas unnecessary.
Hyperglycaemia - Human soluble insulin – parenteralThe Prescribing WG did not support the addition of human soluble insulin, as this wasappropriate for long-term management of diabetes rather than first contact care.
Prophylaxis of asthma in the context of providing ‘complete care’ once the patient hasrecovered from the acute problem - Beclometasone dipropionate – inhalationThe Prescribing WG considered this proposal was outside the concept of first contact andemergency care and that the addition of a single inhaled steroid did not really provide ‘completecare’ as suggested. Continuing management and prescribing for long-term conditions such asasthma was regarded as more appropriate for Supplementary Prescribing.
Postoperative pain relief - Morphine sulphate: parenteral, oral and rectalThe WG considered postoperative pain relief to be the direct responsibility of the anaesthetistand did not therefore recommend inclusion of this condition in the NPEF.
Emergency treatment of meningitis - Cefotaxime and ceftriaxone - parenteral asalternatives to benzylpenicillin

As outlined above, the Prescribing WG recommended the inclusion of benzylpenicillin in theNPEF for this condition.
Cellulitis - Phenoxymethylpenicillin potassium – oralThe Prescribing WG considered parenteral penicillin to be more effective than oral penicillin inthe treatment of cellulitis and therefore did not recommend the inclusion of oralphenoxymethylpenicillin in the NPEF.
Lower urinary tract infection in children - Trimethoprim – Oral.The Paediatric WG were concerned about the prescribing of Trimethoprim in this context as arelatively small proportion of urinary tract pathogens are now sensitive to Trimethoprim and themanagement of young children with urinary tract infections requires specialist investigations.They concluded that, as the proposal was the treatment of children with confirmed results, it wasinappropriate for emergency/first contact care.
Lower respiratory tract infection in children - - Trimethoprim – Oral.The Paediatric WG did not view Trimethoprim for lower respiratory tract infection as a firstchoice antibiotic for this condition and furthermore considered that the diagnosis is difficult tomake with certainty.
REGULATORY IMPACT16. An initial regulatory impact assessment is at Annex B. Comments are sought on thisassessment.
COMMENTS ON PROPOSALS17. You are invited to comment on:
� the additions to the conditions currently treatable under the NPEF – paragraph 8� the proposed extension of “off label” prescribing – paragraph 11� the proposed extension of the prescribing of controlled drugs – paragraph 12� the proposed additions to the NPEF (Schedule 3A of the POM Order) – paragraphs 13
and 14� the proposals not recommended by the Prescribing Working Group or the Paediatric
Working Group – paragraph 15
CIRCULATION OF PROPOSALS 18. This consultation letter is being sent in hard copy to those organisations listed. This list isnot exhaustive. Copies of the consultation are also available from our website -www.mhra.gov.uk – and replies are welcome from all interested parties. The DH/MHRA willnot enter into correspondence about the proposals contained in this MLX.
19. A form is attached for your reply. Comments should be addressed to Martin Bagwell,MHRA, Market Towers, 1, Nine Elms Lane, London SW8 5NQ. Alternatively, they may bee-mailed to [email protected] Replies should arrive no later than 13 July2004. Comments received after this date will not be taken into account.
20. The CSM will be asked to consider the proposals in the light of comments received andtheir advice will be conveyed to Ministers. Subject to the agreement of Ministers, we plan toimplement changes by Statutory Instrument later this year. Statutory Instruments are availablefrom the Stationary Office and may also be viewed on their website http://www.hmso.gov.uk

MAKING COPIES OF THE REPLIES AVAILABLE TO THE PUBLIC21. To help inform debate on the issues raised by this consultation, and within the terms ofthe Code of Practice on Access to Government Information, the Agency intends to make publiclyavailable copies of comments that it receives. Copies will be made available as soon as possibleafter the public consultation has ended.
22. The Agency’s Information Centre at Market Towers will supply copies on request. Anadministrative charge, to cover the cost of photocopying and postage, may be applied.Alternatively, personal callers can inspect replies at the Information Centre by prior appointment(telephone 020-7084 2351).
23. It will be assumed that your comments can be made publicly available in this way, unlessyou indicate that you wish all or part of them to be treated as confidential and excluded from thisarrangement.
Yours faithfully
Anne Thyer Paul RobinsonExecutive Support Medicines, Pharmacy and Industry Group MHRA DH
ANNEX A
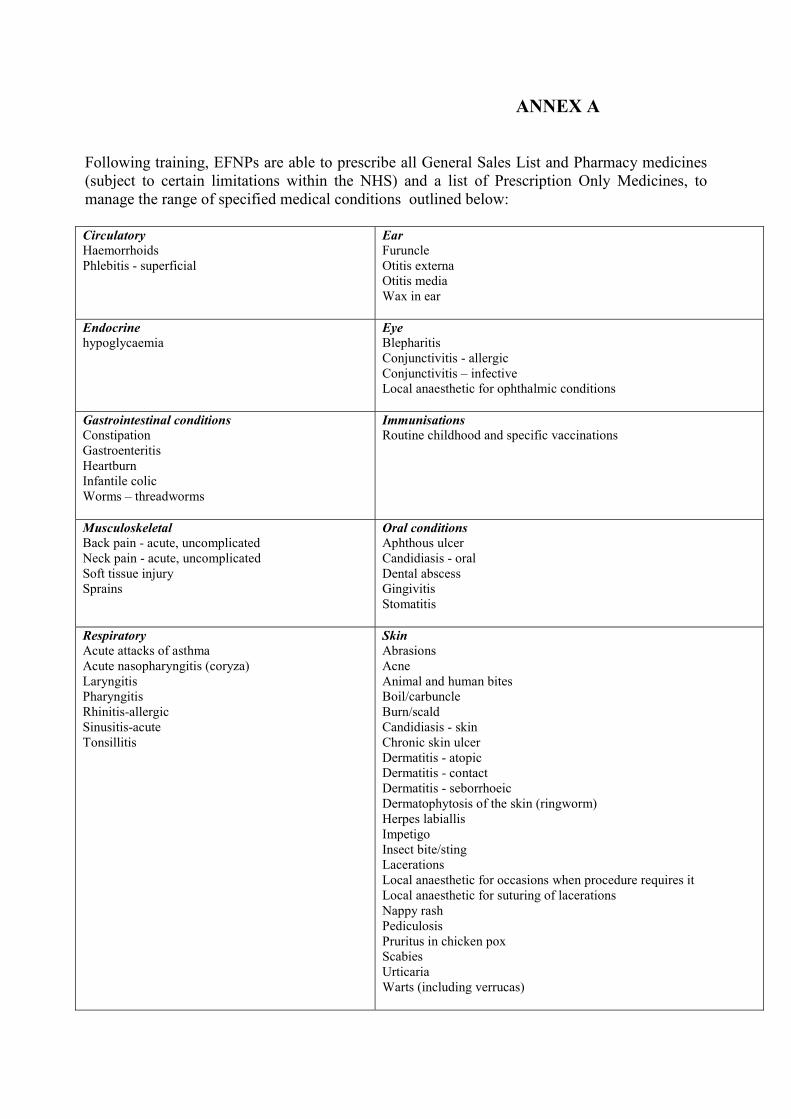
Following training, EFNPs are able to prescribe all General Sales List and Pharmacy medicines(subject to certain limitations within the NHS) and a list of Prescription Only Medicines, tomanage the range of specified medical conditions outlined below:
CirculatoryHaemorrhoidsPhlebitis - superficial
EarFuruncleOtitis externaOtitis mediaWax in ear
Endocrinehypoglycaemia
EyeBlepharitisConjunctivitis - allergicConjunctivitis – infectiveLocal anaesthetic for ophthalmic conditions
Gastrointestinal conditionsConstipationGastroenteritisHeartburnInfantile colicWorms – threadworms
ImmunisationsRoutine childhood and specific vaccinations
MusculoskeletalBack pain - acute, uncomplicatedNeck pain - acute, uncomplicatedSoft tissue injurySprains
Oral conditions Aphthous ulcerCandidiasis - oralDental abscessGingivitisStomatitis
RespiratoryAcute attacks of asthmaAcute nasopharyngitis (coryza)LaryngitisPharyngitisRhinitis-allergicSinusitis-acuteTonsillitis
SkinAbrasionsAcneAnimal and human bitesBoil/carbuncleBurn/scaldCandidiasis - skinChronic skin ulcerDermatitis - atopicDermatitis - contactDermatitis - seborrhoeicDermatophytosis of the skin (ringworm)Herpes labiallisImpetigoInsect bite/stingLacerationsLocal anaesthetic for occasions when procedure requires itLocal anaesthetic for suturing of lacerationsNappy rashPediculosis Pruritus in chicken poxScabiesUrticariaWarts (including verrucas)

ANNEX A (cont’d)
Substance DependenceSmoking cessation
Urinary systemUrinary tract infection (women) - lower, uncomplicated
Female genital systemBacterial vaginosisCandidiasis – vulvovaginalContraceptionDysmenorrhoeaEmergency ContraceptionLaboratory confirmed uncomplicated genitalChlamydia infection (and the sexual partners of thosepatients)Menopausal vaginal atrophyPreconceptual counsellingTrichomonas vaginalis infection (and the sexualpartners of those patients)
Male genital systemBalanitis
PALLIATIVE CARE
Bowel colicCandidiasis - oralConstipationCoughDry mouthExcessive respiratory secretionsFungating malodorous tumoursNausea and vomitingNeuropathic painPain control

ANNEX B
DRAFT - REGULATORY IMPACT APPRAISAL
EXTENDED FORMULARY NURSE PRESCRIBING: AMENDMENTS TO THEPRESCRIPTION ONLY (HUMAN USE) ORDER 1997
THE ISSUE AND OBJECTIVE1. Issue: To amend the Prescription Only (Human Use) Medicines Order to extend theNurse Prescribers Extended Formulary (NPEF), as set out in the March 2004 public consultationletter and subsequent recommendations of the Committee on Safety of Medicines (CSM).
2. Objective: To enhance patient care by improving access to health care through anincreased use of nurses' skills.
SCOPE OF THE RIA3. The changes proposed to medicines legislation will apply to activities undertaken by theNational Health Service throughout the United Kingdom and also to the independent healthcaresector. The extent to which Extended Formulary Nurse Prescribing is adopted within nationalhealth organisations is a matter for each of the devolved administrations. These national servicesare not regarded as a “business, charity or voluntary organisation” for the purpose of this RIA.Health services provided outside the NHS are regarded as businesses and the RIA thereforeconcentrates on the impact of the proposed changes on these groups (referred to from now on asthe independent healthcare sector). However, Extended Formulary Nurse Prescribing does notcreate a new regulatory environment with which the independent healthcare sector must complyat the outset. Whether businesses, employers and individual health professionals adopt thesearrangements is entirely a voluntary decision for them based on their commercial andprofessional judgement.
ISSUES OF EQUITY OR FAIRNESS: 4. Government wants to facilitate the continuing professional development of nurses and theutilisation of their professional skills and competencies by extending the NPEF. Extension of theNPEF will ensure better use of professional skills and more timely access to treatment bypatients. The Government wants to ensure that patients both in the NHS and the independenthealthcare sectors are treated in the same way with more access to professional skills and timelytreatment.
RISK ASSESSMENT5. The proposed extension of the NPEF will not endanger public health. Nurses will only beable to prescribe from the NPEF after completing the relevant training courses, and availableevidence suggests that nurses are capable and careful prescribers who only prescribe within theircompetencies. The proposed amendments have been carefully considered, both by an extensivepublic consultation exercise and by the CSM, and no public health risks have been identified.
OPTIONS6. Two options have been identified
Option 1 - do nothing.

Option 2 - amend medicines regulations as proposed to further expand the range of drugslisted in the NPEF.
IDENTIFICATION OF BENEFITS7. Option 1: This would maintain the status quo but would lose the benefit of patients beingable to access timely and appropriate treatment, in an extended range of circumstances, withoutthe need for a doctor's prescription. This would not maximise the use of the professional skills ofnurses.
8. Option 2: Will allow safe and effective practice to operate which has advantages for bothpatients (e.g. timely access to treatment, a reduction in waiting times) and health care staff (e.g.maximising use of professional skills, facilitating professional and career development). Nurseswill only be able to prescribe after appropriate professional training, and will prescribe onlywithin their competencies, thus protecting patient safety.
COMPLIANCE COSTS FOR BUSINESS, CHARITIES AND VOLUNTARYORGANISATIONS9. Business sectors affectedThe independent healthcare sector providing healthcare outside any arrangements funded by theNHS, who choose to adopt and implement Extended Formulary Nurse Prescribing.
10. Costs for a typical business if Extended Formulary Nurse Prescribing is adoptedAs outlined above, Option 2 does not create a new regulatory environment for businesses asutilisation is entirely a voluntary decision for businesses in the light of benefits to theirorganisation, to patients and to the health professionals employed by those businesses. Costs willbe incurred in attending the appropriate training course(s) and in providing locum cover.However, where EFNP is adopted, we expect the long-term benefits to outweigh the costs.
11. Impact on small businessThis RIA follows the joint DH/MCA formal consultation with a wide range of interests coveringthe NHS, health professionals, patient and other interest groups. To be completed
COMPETITION ASSESSMENT12. The proposal to introduce supplementary prescribing has been considered against theOFT’s competition filter. The results clearly show that the proposal would have no adverseeffects on competition within the health care “market”. The proposal introduces no incentives ordisincentives.
RESULTS OF CONSULTATION 13. Formal public consultation has shown….. To be completed.
SUMMARY AND RECOMMENDATIONS14. Option 2 is recommended because it best meets the Government's objective. Thebenefits of this option in terms of public health, future savings to the NHS and the effective useof resources are judged to outweigh the costs to business, which are not thought to be significant.

Option 1 ("Do Nothing")
Option 2(Amend Regulations)
Healthcare businesses Retain the range ofconditions and drugs in theexisting NPEF.
Allows safe and effectiveprescribing practice.Maximises use ofresources and professionalskills of nurses resulting inpotential longer termsavings and significantbenefit to patients
Citizens (in this context,patients)
Reduction in waiting timesand timely access toappropriate professionalskills.
ENFORCEMENT, SANCTIONS, MONITORING AND REVIEW15. The Medicines and Healthcare products Regulatory Agency will be responsible forenforcing the legislation. The Department of Health has commissioned an evaluation ofExtended Formulary Nurse Prescribing. The University of Southampton is undertaking thiswork, which should be completed in the second half of 2004.
DECLARATION:
I have read the Regulatory Impact Assessment and I am satisfied that the benefits justify thecosts.
Signed by the responsible Minister: ……………………………………
Date: ……………………………………
Contacts: Anne Thyer Paul RobinsonExecutive Support Medicines, Pharmacy and Industry Group MHRA Department of Health020 7084 2642 0113 [email protected] [email protected]

MLX 303: HARD COPY CONSULTATION LIST
NB: this list is not intended to be exhaustive. Copies of the consultation are also available from ourwebsite - www.mhra.gov.uk – and replies are welcome from all interested parties.
Action for Sick ChildrenAdvisory Committee on Misuse of DrugsArthritis CareAll Party Pharmaceutical GroupAssociation of British Cardiac NursesAssociation of Nurse PrescribingAssociation for Palliative MedicineAssociation for Residential CareAssociation of Anaesthetists of Great Britain and Northern IrelandAssociation of British Health Care IndustriesAssociation of British Pharmaceutical IndustriesAssociation of Independent Multiple PharmaciesAssociation of Medical MicrobiologistsAssociation of Surgeons of Great Britain and IrelandBritish Association of DermatologistsBritish Association for A&E MedicineBritish Association of Pharmaceutical PhysiciansBritish Association of Pharmaceutical WholesalersBritish Cardiac Patients AssociationBritish College of OptometristsBritish Contact Dermatitis GroupBritish Dental AssociationBritish Dental Trade AssociationBritish Diabetic AssociationBritish Dietetic AssociationBritish Generic Manufacturers AssociationBritish Heart FoundationBritish Institute of Regulatory AffairsBritish Medical AssociationBritish Oncological AssociationBritish Pharmacological SocietyBritish Society for Antimicrobial ChemotherapyBritish Society of GastroenterologyCarers National AssociationChemist & DruggistCollege of HealthCollege of OptometristsCollege of Pharmacy PracticeCommunity Practitioners and Health Visitors AssociationCommunity Pharmacy MagazineCompany Chemists Association Consumers AssociationCo-operative Pharmacy Technical Panel

Dental Defence UnionDental Formulary Subcommittee of the Joint Formulary Committee Dental Protection LtdDispensing Doctors AssociationDoctor MagazineDrug & Therapeutics BulletinDrug Information Pharmacists GroupEuropean Association of Hospital PharmacistsFaculty of Pharmaceutical MedicineGeneral Dental CouncilGeneral Dental Practitioners Association.General Medical CouncilGeneral Practitioners CommitteeGuild of Healthcare PharmacistsHealth & Safety ExecutiveHealth Development AgencyHealth Professions CouncilHealth Promotion EnglandHealth Service CommissionerHealth Which?Independent Healthcare AssociationJoint Consultants CommitteeJoint Formulary Committee Joint Royal Colleges Ambulance Service Liaison CommitteeLong Term Medical Conditions AllianceMedical Defence UnionMedical Protection Society LtdMedical Research CouncilMIMS LtdNational Association of GP Co-operativesNational Consumer CouncilNational Care Standards CommissionNational Patient Safety AgencyNational Pharmaceutical AssociationNeonatal and Paediatric Pharmacists GroupNursing and Midwifery CouncilOTC BulletinOverseas Doctors Association in the UK LtdPaediatric Chief Pharmacists GroupPatients AssociationPharmaceutical JournalPharmaceutical Services Negotiating CommitteePrescription Pricing AuthorityPrimary Care Pharmacists AssociationProprietary Association of Great BritainPublic Health Laboratory ServiceRegistered Nursing Home AssociationRoyal College of AnaesthetistsRoyal College of General Practitioners

Royal College of MidwivesRoyal College of NursingRoyal College of Obstetricians & GynaecologistsRoyal College of OphthalmologistsRoyal College of Paediatrics and Child HealthRoyal College of PathologistsRoyal College of Physicians (London)Royal College of PsychiatristsRoyal College of RadiologistsRoyal College of Surgeons (England)Royal College of Surgeons (Faculty of Dental Surgery)Royal Colleges of Physicians : Faculty of Pharmaceutical MedicineRoyal Colleges of Physicians : Faculty of Public Health MedicineRoyal Pharmaceutical Society of Great BritainRoyal Society of ChemistryRoyal Society for the Promotion of HealthScrip LtdSmall Business ServiceSocial Audit Society of HomoeopathsSociety of Pharmaceutical MedicineSpecialist Advisory Committee on Antimicrobial ResistanceSt John AmbulanceUK Clinical Pharmacy AssociationUnison

To: Martin BagwellMHRAMarket Towers1 Nine Elms LaneLONDON SW8 5NQ
From : ________________________________________________________________________________________________________________________
CONSULTATION LETTER MLX 303: NURSE PRESCRIBERS EXTENDEDFORMULARY: PROPOSALS TO EXTEND RANGE OF PRESCRIPTION ONLYMEDICINES
* 1. I support the proposals contained in the MLX
* 2. I have no comment to make on the proposals in the MLX
*3. My comments on the proposals in the MLX are below/attached.
* My reply may be made freely available.* My reply is confidential.* My reply is partially confidential (indicate clearly in the text any confidential elements)
Signed : _____________________________________________
* Delete as appropriate