nulife module 6 screening for malignancies edited
TRANSCRIPT

SCREENING FOR MALIGNANCIES

2
OBJECTIVE
Concept of preventive oncology,
screening and early detection
3
EXPECTED OUTCOME
Standard methodologies for screening
Cancer cervix, breast, uterus, ovaries, others

4
SCREENING FOR MALIGNANCY
Genital Cancers
Cervix, Endometrium, Ovary
Others
Breast, Colorectal, Oral

5
CANCER CERVIX
Commonest cancer in Indian women
Third commonest in the world
Annual global incidence : 500,000
India contributes 100,000 (1/5th)
Every year world wide 200,000 women die
Magnitude more than evident

6
Opportunities For Cancer Control Interventions

7
7
Communicating Effectively With Parents and Patients
Include HPV vaccines in discussion of all vaccines
recommended for adolescents
Use a short, matter-of-fact approach to HPV vaccine
recommendation
Emphasize cancer prevention

8
Strategies for Increasing HPV Vaccine Uptake
The strongest predictor of a person being vaccinated is a physician recommendationa
Have the conversation!
Educate yourself to educate parents and patients about vaccines
Most parents want to vaccinate their children
Discuss all adolescent vaccines before they are due
Address parents’ questions
Questions may reflect interest rather than vaccine refusal
Immunize at every opportunity
Offer the HPV vaccine when other vaccines are being administered
8
a. Nichol KL. Cleve Clin JMed. 2006;73:1009-1015
9
SCREENING FOR CA CERVIX
No organised screening programme in India
Recommended in:
Sexually active women over 30 yrs
Sexually active for more than 10 yrs

10
SCREENING METHODS
VIA
VILI
Cervical Smear from Ecto & Endo Cx
HPV testing whenever possible
Introduce Colposcopy when possible
11
PAP TEST (CERVICAL / VAGINAL CYTOLOGY)
Uses
Screening and diagnosis of CIN
Detection of Genital infection
Evaluate Hormonal status
For additional information regarding cytology follow-
up a gynecologist should be consulted
12
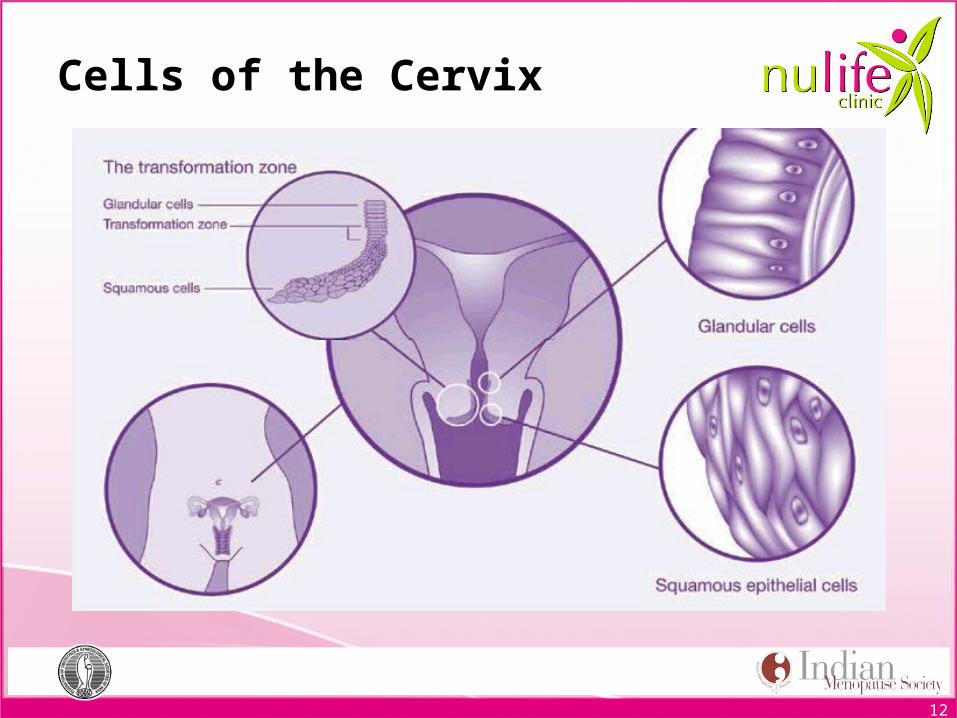
Cells of the Cervix
13
The Bethesda system 2001
Negative for Intraepithelial Lesion or Malignancy
Infection
– Trichomonas vaginalis
– Fungal infection such as Candida species
– Bacterial vaginosis
– Actinomyces species
– Herpes simplex virus
Other findings
– Reactive cellular changes;
– Inflammation (includes typical repair)
– Radiation effects
– Intrauterine contraceptive device
– Glandular cells present after hysterectomy
– Atrophy
14
TBS 2001
Epithelial Cell Abnormalities
Squamous cells
Atypical squamous cell of undetermined significance (ASC-US)
Atypical squamous cell cannot exclude HSIL (ASC-H)
Low-grade squamous intraepithelial lesion (LSIL)
High-grade squamous intraepithelial lesion (HSIL)
Squamous cell carcinoma
Glandular cells
Atypical glandular cells (AGC) (specify endocervical, endometrial, or not otherwise specified)
Atypical glandular cells, favor neoplastic (specify endocervical or not otherwise specified)
Endocervical adenocarcinoma in situ (AIS)
Adenocarcinoma
Other
Endometrial cells in a woman ≥40 years of age

15
15
Population†
USPSTF ( us preventive task force)
ACS/ASCCP/ASCP( ameirican cancer society, american socieity of colposcopy and cervical pathology, american society for clinical pathology)
Younger than 21 years
Recommends against screening.Grade: D recommendation.
Women should not be screened regardless of the age of sexual initiation or other risk factors.?
21–29 yearsRecommends screening with cytology every 3 years. Grade: A recommendation.
Screening with cytology alone every 3 years is recommended.
30–65 years
Recommends screening with cytology every 3 years or for women who want to lengthen the screening interval, screening with a combination of cytology and HPV testing every 5 years. Grade: A recommendation.
Screening with cytology and HPV testing (“co-testing”) every 5 years (preferred) or cytology alone every 3 years (acceptable) is recommended.
HPV vaccinatedWomen who have been vaccinated should continue to be screened.
Recommended screening practices should not change on the basis of HPV vaccination status.
MARCH 14 2012 Recommendations for Cx. Cancer screeningModified from CA Cancer J Clin. 2012;62:147-172 .
04/15/2023

Older than 65 years
Recommends against screening women who have had adequate prior screening¶ and are not otherwise at high risk for cervical cancer. Grade: D recommendation.
Women with evidence of adequate negative prior screening¶ and no history of CIN2+ within the last 20 years should not be screened. Screening should not be resumed for any reason, even if a woman reports having a new sexual partner.
After hysterectomy
Recommends against screening in women who have had a hysterectomy with removal of the cervix and who do not have a history of a high-grade precancerous lesion (ie, CIN 2 or 3) or cervical cancer.Grade: D recommendation
Women of any age following a hysterectomy with removal of the cervix who have no history of CIN2+ should not be screened for vaginal cancer. Evidence of adequate negative prior screening is not required. Screening should not be resumed for any reason, including if a woman reports having a new sexual partner.
high-risk populations who may need more intensive or alternative screenin. These special populations include women 1) with a history of cervical cancer, 2) who were exposed in utero to diethylstilbestrol (DES), and 3) who are immune-compromised (eg, infection with human immunodeficiency virus).
16

17
WHO RECOMMENDATIONS
Cytology is recommended for large-scale cervical cancer screening if sufficient resources exist
New programmes should start screening women aged 30 years or more, and include younger women only when the highest-risk group has been covered
Existing organized programmes should not include women less than 25 years of age in their target populations.
If a woman can be screened only once in her lifetime, the best age is between 35 and 45 years

18
How to take a Pap Smear ?
Patient in dorsal position
Good illumination is necessary
Cusco’s speculum is inserted to visualise & fix the cervix
Inspection of cervix done & findings are noted
Ayres spatula is inserted first. It is placed at cervical os so that longer end goes into cervical canal and smaller end rests on ectocervix

19
How to take a Pap Smear
Spatula is rotated through 360 degrees maintaining contact with ectocervix
Do not use too much force [bleeding /pain]
Do not use too little force [inadequate sample]
Sample is smeared(both sides of spatula) evenly on the slide and fixed immediately

20
How to take a Pap Smear
Endocervical sample is collected using
an endocervical brush
Insert the cytobrush into canal, so that
last bristles of brush are visible
Rotate the brush through 180 degrees.
[ more rotations increase the chance of
bleeding ]
Sample is rolled on the slide and fixed .

21
FIXATION OF SMEAR
Fixation is done immediately with fixative like 95% alcohol or cytofix spray to avoid air drying
Spray should be kept at 10 inches, to avoid destruction of cells by propellent in the spray
Smear should be monolayer for proper penetration of cell surface by fixative

22
Interpretation Of PAP’S Smear
In menopausal women not taking estrogen replacement therapy, the presence of endometrial cells is an abnormal finding and should be followed up with an endometrial biopsy to try to determine the reason for the presence of these cells.
Koilocytosis This finding is often based on the presence of "koilocytes" having enlarged nuclei, surrounded by a clear "halo" of cytoplasm. Koilocytes often (but not invariably) point to the presence of of human papilloma virus (HPV) in the cells.

23
Interpretation Of PAP’S Smear
Inflammation merely means the cervix is irritated for some
reason. In the absence of any symptoms or any other significant
abnormality on the Pap, it can be safely ignored.
If inflammation is severe enough, it may interfere with the ability
of the cytologist to accurately read the Pap. In such cases, it is wise
to repeat the Pap at more frequent intervals (6-9 months) rather
than the usual once a year.
Inflammation by itself need not be treated. If other abnormalities
are identified in addition to the inflammation, you may treat the
other problems and the inflammation will probably go away.

24
CERVICAL SMEAR
Percentage reduction in Invasive Ca
– Annual : 93%
– 3 Yrly : 91%
– 5 Yrly : 84%
False Pos : Rare False Neg : 10-35%
Specificity : 94% Sensitivity : 52%
Shortcomings

25
LIMITATIONS
Difficulty in preserving & transporting
Lack of trained technicians to analyze
Problems in getting women back for results, follow-up,
referral, and treatment when necessary.
26
VIA
Speculum exam
Application of 3-5% acetic acid
Viewing the cervix with the naked eye to identify
colour changes
Abnormal tissue appears white
Positive, Negative or Suspicious for cancer

27
VIA RESULTS
NEGATIVE POSITIVE

28
VIA RESULTS
SUSPICIOUS FOR CANCER

29
STRENGTHS OF VIA
Simple, easy-to-learn approach
Low start-up & sustaining costs
All types of health care providers can perform test
Results available immediately
Possible to integrate VIA into PHC

30
LIMITATION
Post menopausal women
Not suitable as SCJ inside canal
Results not as reliable
IMS Clinical Practice Guidelines on Menopause 2013

31
HPV
Primary cause of cervical cancer
Most women with high-grade CIN have detectable HPV DNA
HPV positive, Pap smear normal women are at increased risk of CIN
Lorinz A et al. Human papilloma virus infection of the cervix. Relative risk association of 15 common anogenital types. Obstet Gynecol 2000, 79:328-337

32
HPV DNA CERVICAL SAMPLERand LBC Sampler
33
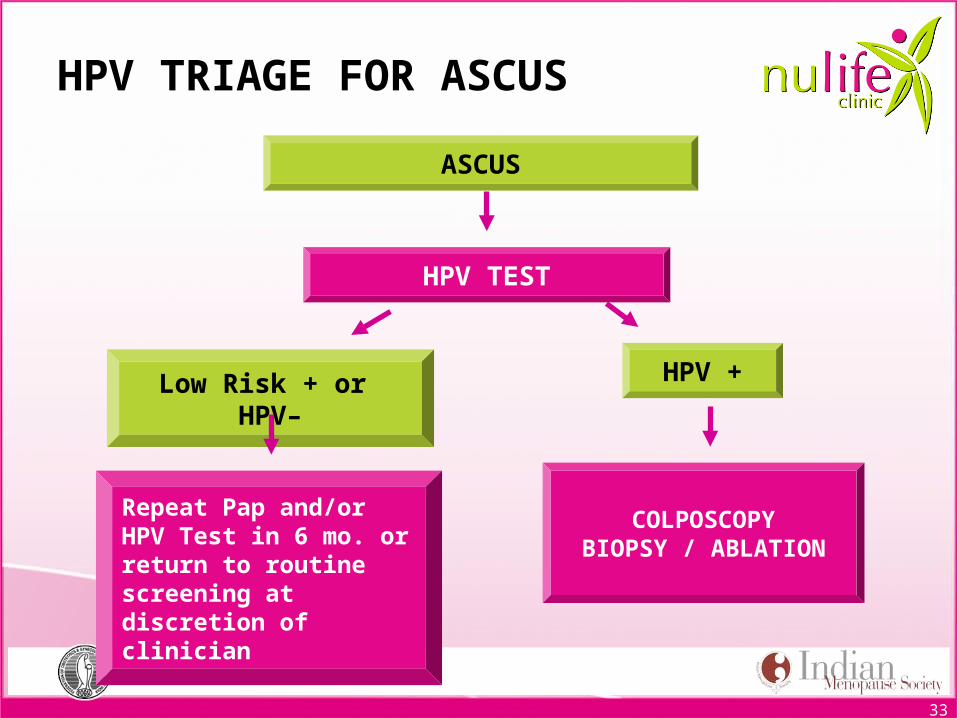
Low Risk + or HPV–
ASCUS
HPV TEST
HPV +
Repeat Pap and/or HPV Test in 6 mo. or return to routine screening at discretion of clinician
COLPOSCOPYBIOPSY / ABLATION
HPV TRIAGE FOR ASCUS

34
STRENGTHS OF HPV
High-risk HPV DNA testing
For triage management of post-menopausal women
with unequivocal cytology results
Once in 5 yrs till age 65
IMS Clinical Practice Guidelines on Menopause 2013

35
LIMITATIONS OF HPV
High cost
Not easily available
Lower specificity than cytology
Samples to be sent to a special lab
Follow-up visit required for report

36
INDICATIONS FOR COLPOSCOPY
HSIL or Invasive Ca on Smear
Persistent LSIL on Smear
Positive VIA / VILI
Positive HPV DNA test
LSIL in a non compliant woman
Suspicious looking cervix
Therapeutic

37
CIN as Seen in Colposcopy
CIN 1: Mild dysplasia; includes condyloma (anogenital warts)2
CIN 2: Moderate dysplasia2
CIN 3: Severe dysplasia; cancer in situ (CIS); FIGO Stage 02,3
CIN 1 CIN 2 CIN 3
1. Wright TC Jr, Cox JT, Massad LS, et al, for the ASCCP-Sponsored Consensus Congress. JAMA. 2002;287:2120–2129. 2. Bonnez W. In: Richman DD, Whitley RJ, Hayden FJ, eds. Washington, DC: American Society for Microbiology Press; 2002:557–596. 3. Canadian Cancer Society. Cervical Cancer: What you need to know. Available at: http://www.cancer.ca/vgn/images/portal/cit_86751114/63/40/151140772cw_library_wyntk_cervical_en.pdf. Accessed March 13, 2006. 4. Reprinted with permission from Sellors JW, Sankaranarayanan R, eds. Colposcopy and Treatment of Cervical Intraepithelial Neoplasia. A Beginner’s Manual. Lyon, France: International Agency for Research on Cancer; 2003.
Photo courtesy of Dr. J. Monsonego Photo courtesy of Dr. J. Monsonego From IARC, 2003.4
Colposcopy findings confirmed by histology1
38
BREAST CANCER : INDIA
28/100,000 Urban, 6/100,000 Rural
More than doubled over last 20 yrs
100,000 new cases annually
43 - 46 years
Late marriage, small families
Shorter lactation
Obesity

39
BREAST CANCER
Breast self examination monthly
Clinical exam annually
Annual mammograms from age 40
High risk screening to start 10 yrs earlier than
youngest affected family member

40
BREAST SELF-EXAMINATION
A women checks her own breasts & can look for
irregularities, lumps, changes in breast size or shape,
nipple discharge, or irregular tissue thickening.
Not much data to show a statistically significant
reduction in detection of breast cancer
However in India, increases awareness and may detect
and downstage the cancers
41
CLINICAL BREAST EXAMINATION
A clinical breast examination (CBE) is a physical examination of
the breast performed by Clinician.
Aim – main goal of CBE is to differentiate normal physiologic
nodularity from a discrete breast mass If a discrete mass is
identified , evaluation in this case is mandatory to exclude breast
cancer. CBE is able to identify 10 to 25% of breast cancer which
are missed by mammography . Specificity of CBE is 85 to 99% but
Predictive value is its major limitation. Lesion detected by CBE
only 6 to 46 % are malignant depending on the age of the patient.

42
MODALITIES OF BREAST IMAGING
USG
Mammography
MRI

43
USG
Commonly used in young females
Increases the sensitivity of mammography
Operator dependent
Not approved for screening
Useful to distinguish solid from cystic lesions
Useful in guiding aspiration and biopsies
Findings suspicious of malignancy on usg- solid mass, irregular, taller than wider, > 4 lobulations

44
MAMMOGRAPHY
Highly sensitivity, older women
Findings suspicious of malignancy-
Irregular, spiculated mass
Clustered microcalcifications (< 5 mm in diameter)
Solid mass with ill defined borders
Architectural distortion
Enlarging, solid well circumscribed mass
Focal asymmetric density
Enlarged axillary nodes with loss of architecture

45
BREAST CANCER SCREENING
Screening by mammography results in reduction of
mortality by 30% in women> yrs.
Mammographic screening programme is not
sustainable in developing countries.
Physical Examination of breast by trained personnel
has sensitivity of 75% and specificity of 90%.
BSE may help but there is no evidence that it improves
survival.

46
MALIGNANCY LEFT BREAST

47
MAGNIFICATION VIEW

48
USG OF MALIGNANT LESION

49
MRI BREAST
Dedicated breast coil
Highly sensitive, poorly specific
Leads to unnecessary biopsies
Does not visualize calcifications
Has no place in routine evaluation of breast lumps

50
MRI BREASTOnly indications-
Occult primary with positive axillary nodes
To distinguish scar from recurrence in operated breast cancer patients
Residual tumour- positive margins
Invasive lobular carcinoma
To know extent of disease – multifocal/ multicentric
Contralateral cancers
Discordant clinical exam, mammography/ usg findings
Implants
Screening of high risk women
51
ENDOMETRIAL CANCER
No screening programme : opportunistic
Categorize the high risk group and counsel
Pap Smear : Sensitivity 40%
USG : TAS : No Value
TVS : Effective, non-invasive

52
Risk of endometrial cancer
Obesity,
Nulliparity,
Hypertension,
Diabetes,
Polycystic ovarian syndrome,
Endometrial hyperplasia,
Early menarche,
Late menopause,
Unopposed estrogen therapy,
Family history of cancer, past history of breast cancer and
Tamoxifen therapy

53
Risk of endometrial cancer
Decreased by Prolonged use of OCPs and
progestins.
Reduced risk by HRT specially in obese women

54
ENDOMETRIAL THICKNESS
Post-menopausal Bleeding
Must investigate promptly
ET : > 4mm
Sensitivity : 96% for Endo Ca
HT : 4mm
Tamoxifen : 8mm

55
Interpret the findings
4x4cms
What is the incidence of Endometrial Ca at 50 yrs?

56
Pipelle
Sensitivity in detecting
Endmetrial caner ?
What percentage need
further investigation?

57
OVARIAN CANCER
No effective screening
No recognised pre-invasive stage
Inaccessible for visualisation or sampling
60-70% diagnosed in Stage III

58
Risk factors for ovarian cancer
Increasing age,
Nulliparity,
Use of fertility-enhancing drugs such as clomiphene
citrate for more than 1 year,
Family history of ovarian, breast or colorectal cancer,
and past history of breast cancer.
Obesity might increase some types but not all, whereas

59
Decreased risk of ovarian cancer
Use of oral contraceptive pills is a very potent way to
decrease ovarian cancer risk.
Certain gynecological surgeries like tubal ligation,
hysterectomy and cure of endometriosis are protective
against ovarian cancer
Exercise could help to decrease the risk

60
OVARIAN CANCER
CA 125
> 35u/ml in 80% Epithelial cancers
Raised in Endometriosis, PID, Koch’s
Other tumour markers: CA602 & CA546
TVS
Colour Doppler

61
STOMACH CANCER
In women aged 30–69 years, the second most common fatal cancers was stomach (14.1%). Stomach cancer rates were higher in rural than in urban areas of India due to increased prevalence of chronic H. pylori infection.
Million death study cancer mortality in India: a nationally representative survey 2012. This may include stomach and primary liver cancer.
Prevalence of hepatitis B virus in India was less than 1.9% in 72,000 pregnant women aged 15–49 years who were tested in 2002.
Million death study 2012
62
PREVENTION
Thirty seven percent of all female cancer deaths were from infection-related cervical, stomach, and liver cancers and 18.3% were from tobacco-related cancers.
This underscores the importance of vaccination, control of infection.
Vaccination against hepatitis B virus would reduce future liver cancer deaths and cirrhosis.
Use of tobacco in pan and beedi should be strongly discouraged.
IMS Clinical Practice Guidelines on Menopause 2013

63
HBV Screening Algorithm for At-Risk Patients
HBsAg and anti-HBS test
HBsAg +
HBsAg -
Anti-HBs +
Anti-HBs -
Collect baseline data • ALT • HBeAg, anti-Hbe • HBVDNA level and • Go to evaluation and
monitoring algorithm
Immune to HBV, no follow-up needed
HBV Evaluation and Monitoring Algorithm
LokASF, et al. Hepatology. 2009:50:1-36
Vaccinate

64
ORAL CANCER
Oral examination every 3 years
High risk group annually
Detect precancerous lesions

65
COLORECTAL CANCER
50 years
Stool for occult blood annually
5 yearly: Flexible sigmoidscopy or
Double contrast Barium enema
Colonoscopy every 10 years

66
Preventive strategies for all cancers
Stop smoking
Control weight
Exercise (vigorous exercise for at least 2–3 h/week)
< 15 g/day alcohol intake
Diet rich in vegetables, fibers and fruits (five fruit and
vegetables/day but only two fruits, maximum three),
low intake of animal fat, and a low proportion of
carbohydrates

67
When should women report
Abnormal vaginal bleeding, abdominal or pelvic pain, distension, abnormal vaginal discharge, hematuria, or rectorrhagia can reveal an endometrial, ovarian or colon cancer.
Breast nipple discharge or palpation of a lump, induration of a localized zone of the breast, a skin abnormality on the area of the breasts (skin or nipple retraction, 'peau d’orange') can indicate breast cancer.
Unusual cough, dyspnea, hemoptysis or thoracic pain can reveal a lung cancer.
Occurrence of venous thrombosis in women without a family history can reveal a cancer and needs some complementary investigations.

68
CASE
51 yr old, post menopausal 3 yrs
Routine screening
Smear : LSIL
Refd for management
What would you advise?
Vaginal estrogen for 1 month and rpt
Anxious, refer for Colposcopy

69
70
CASE
Smear : HSIL
What would you do?
Refd for Colposcopy

71

72
What would you do?
LLETZ
HPE : HSIL
Follow up?
Smear after 6 mths : Normal
Smear after 12 mths : ASC-H
Advise?
Rpt Colposcopy

73

74
Diagnosis?
Healed cervix after LLETZ
Rpt Smear after 12 months

75
CASE
45-year-old P2 complains of amenorrhea one year with 15-20 hot flashes/day
History of Lt radical mastectomy for breast cancer 7 years ago with complete cure
BP 130/85, Wt 60 kg. Ht 163cm
Right Breast, abdominal & pelvic examinations revealed no abnormal findings
Fasting sugar 95 mg/dl & lipid profile WNL
Treatment?

76
TREATMENT
For hot flushes
Non-hormonal : Lifestyle modification
Venlaflaxine 37.5 mg twice a day
For Osteoporosis
Bisphosphonates and others

77
BREAST CANCER SURVIVORS
Inc incidence of Ca Breast
Improved survival times after treatment
Induce early menopause & climacteric symptoms
More breast cancer survivors with vasomotor
symptoms

78
Hormone Therapy and Breast CancerEstrogen Alone
Estrogen alone increases percentage mammographic density, not as much as estrogen and progesterone together (Level A).
Estrogen increases the risk of breast cancer after more than 5 years of use, particularly in recently postmenopausal women (Level B).
The attributable or excess risk for 5 years usage is 0/1000 to 2.59 per 1000 (Level C).It falls under the rare category.
Increased risk dissipates within 5 years of discontinuing the HT (Level B).
Tumors in HT used women are usually ER positive and lobular type (Level C).
IMS Clinical Practice Guidelines on Menopause 2013

79
Hormone Therapy and Breast CancerEstrogen + Progesterone
E + P increases percentage mammographic density significantly (Level A).
E + P particularly with synthetic progesterones increases the risk of invasive breast cancer within 3–5 years of initiation and increases progressively beyond that time (Level B).
Emerging data from 2 independent studies report that micronized progesterone/dydrogesterone does not increase the risk if given for less than 5 years (Level C).
The risk returns to approximately that of non-users within 3 years of cessation (Level B).
IMS Clinical Practice Guidelines on Menopause 2013

80
BREAST CANCER SURVIVORS
Consider HT in some women whose quality of life
impaired by estrogen deficiency, after adequate
counselling
Risk of recurrence must be explained
Fair trial with alternative therapies given prior to
starting HT/Tibolone
Lowest effective dose for shortest duration

81
All these are possible with screening except
a) Early detection of disease
b) Improving the treatment results
c) Decreasing mortality due to disease
d) Eradication of disease