nuevos horizontes en inmunología: atezolizumab · pd-1 y b7-1. • no inhibe pd-l2 (menor...
TRANSCRIPT
Nuevos horizontes en inmunología: Atezolizumab
Dra. Margarita Majem
Hospital de la Santa Creu i Sant Pau
Barcelona
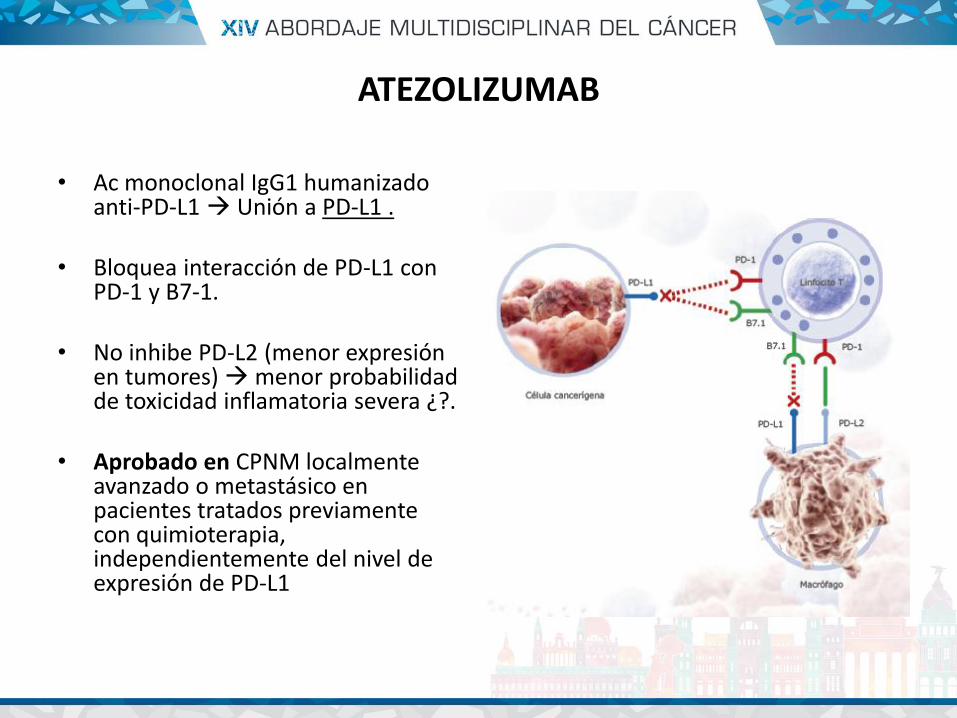
ATEZOLIZUMAB
• Ac monoclonal IgG1 humanizado anti-PD-L1 Unión a PD-L1 .
• Bloquea interacción de PD-L1 con PD-1 y B7-1.
• No inhibe PD-L2 (menor expresión en tumores) menor probabilidad de toxicidad inflamatoria severa ¿?.
• Aprobado en CPNM localmente avanzado o metastásico en pacientes tratados previamente con quimioterapia, independientemente del nivel de expresión de PD-L1
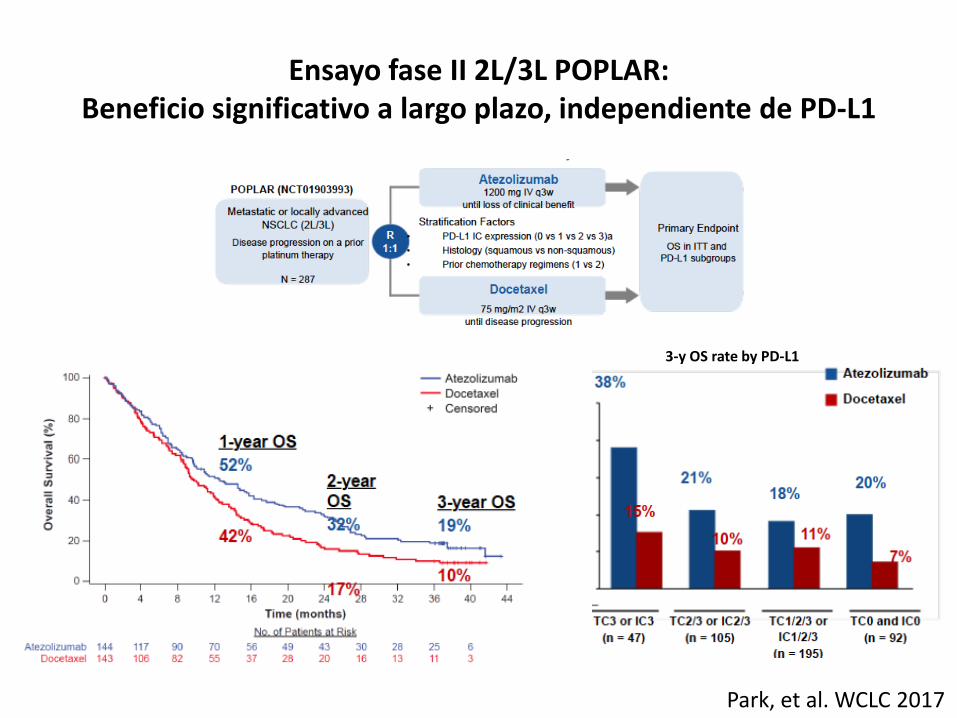
Ensayo fase II 2L/3L POPLAR: Beneficio significativo a largo plazo, independiente de PD-L1
Park, et al. WCLC 2017
3-y OS rate by PD-L1
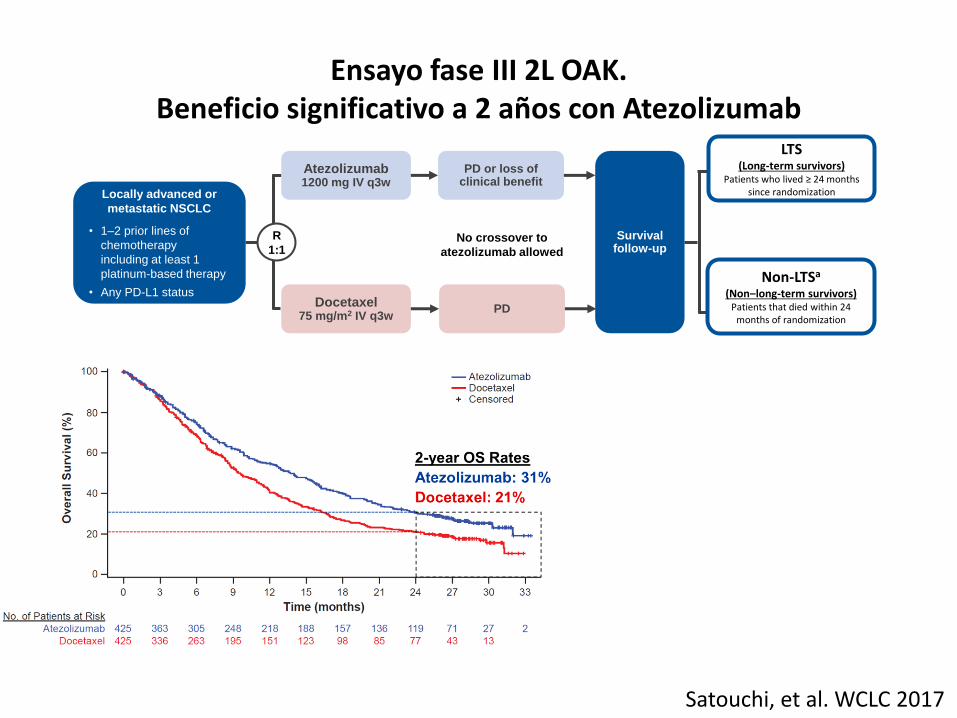
Satouchi, et al. WCLC 2017
Ensayo fase III 2L OAK. Beneficio significativo a 2 años con Atezolizumab
Non-LTSa
(Non‒long-term survivors) Patients that died within 24
months of randomization
LTS (Long-term survivors)
Patients who lived ≥ 24 months since randomization
R
1:1
Locally advanced or
metastatic NSCLC
• 1–2 prior lines of
chemotherapy
including at least 1
platinum-based therapy
• Any PD-L1 status
Atezolizumab 1200 mg IV q3w
Docetaxel 75 mg/m2 IV q3w
PD or loss of clinical benefit
PD
Survival follow-up
No crossover to
atezolizumab allowed
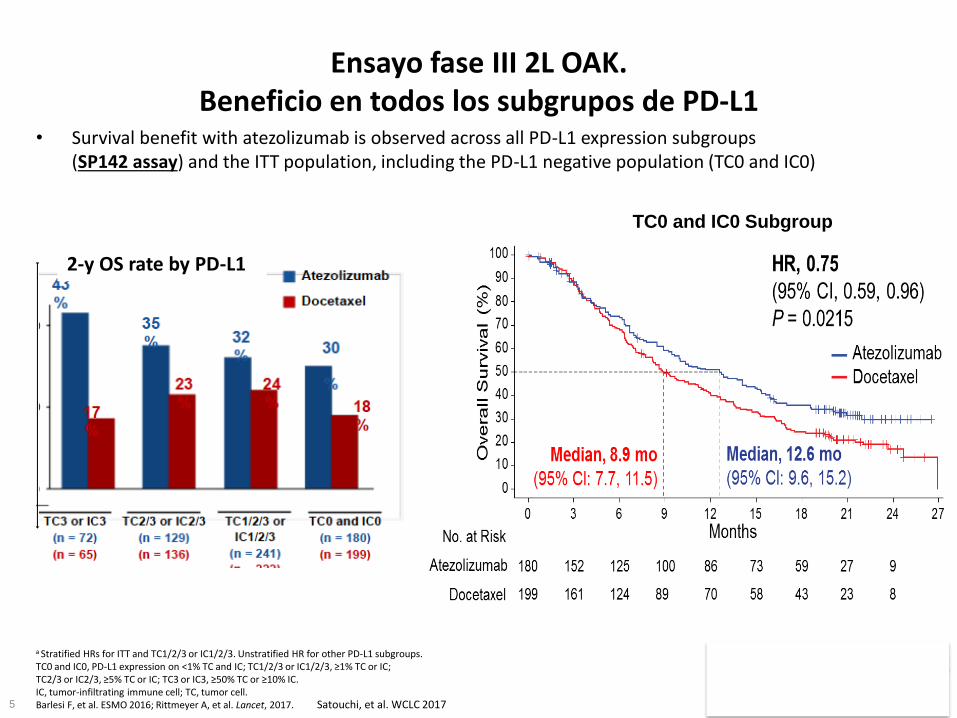
• Survival benefit with atezolizumab is observed across all PD-L1 expression subgroups (SP142 assay) and the ITT population, including the PD-L1 negative population (TC0 and IC0)
5
a Stratified HRs for ITT and TC1/2/3 or IC1/2/3. Unstratified HR for other PD-L1 subgroups. TC0 and IC0, PD-L1 expression on <1% TC and IC; TC1/2/3 or IC1/2/3, ≥1% TC or IC; TC2/3 or IC2/3, ≥5% TC or IC; TC3 or IC3, ≥50% TC or ≥10% IC. IC, tumor-infiltrating immune cell; TC, tumor cell. Barlesi F, et al. ESMO 2016; Rittmeyer A, et al. Lancet, 2017.
Ensayo fase III 2L OAK. Beneficio en todos los subgrupos de PD-L1
TC0 and IC0 Subgroup
Satouchi, et al. WCLC 2017
2-y OS rate by PD-L1
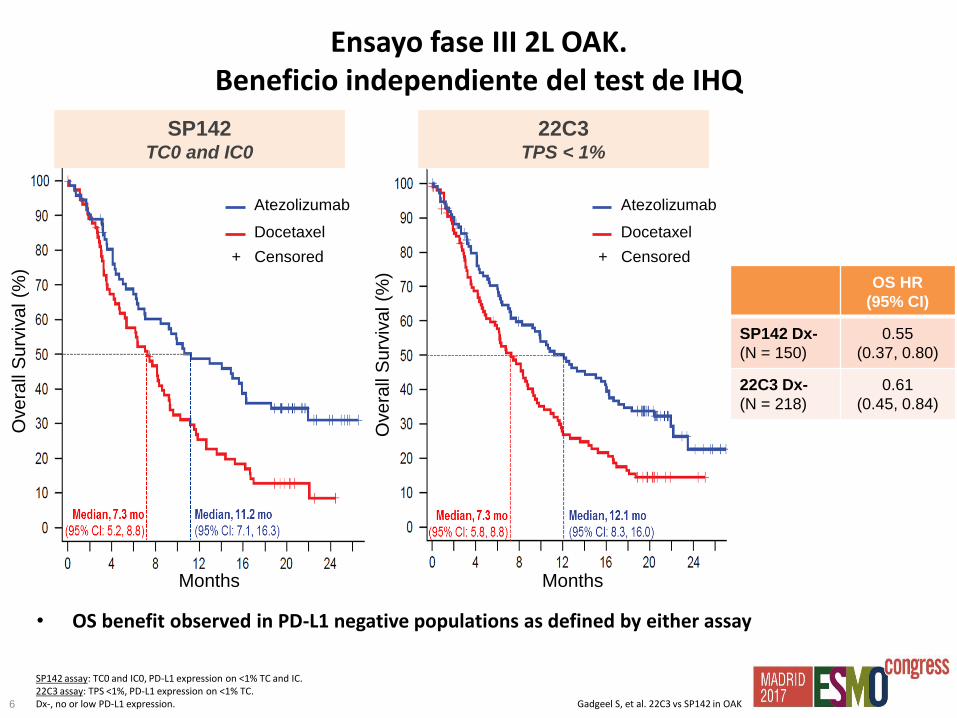
• OS benefit observed in PD-L1 negative populations as defined by either assay
6
SP142 assay: TC0 and IC0, PD-L1 expression on <1% TC and IC. 22C3 assay: TPS <1%, PD-L1 expression on <1% TC. Dx-, no or low PD-L1 expression. Gadgeel S, et al. 22C3 vs SP142 in OAK
OS HR
(95% CI)
SP142 Dx-
(N = 150)
0.55
(0.37, 0.80)
22C3 Dx-
(N = 218)
0.61
(0.45, 0.84)
+ Censored
Atezolizumab
Docetaxel
SP142 TC0 and IC0
Months
+ Censored
Atezolizumab
Docetaxel
22C3 TPS < 1%
Ove
rall
Su
rviv
al (%
)
Months
Ove
rall
Su
rviv
al (%
)
Ensayo fase III 2L OAK. Beneficio independiente del test de IHQ
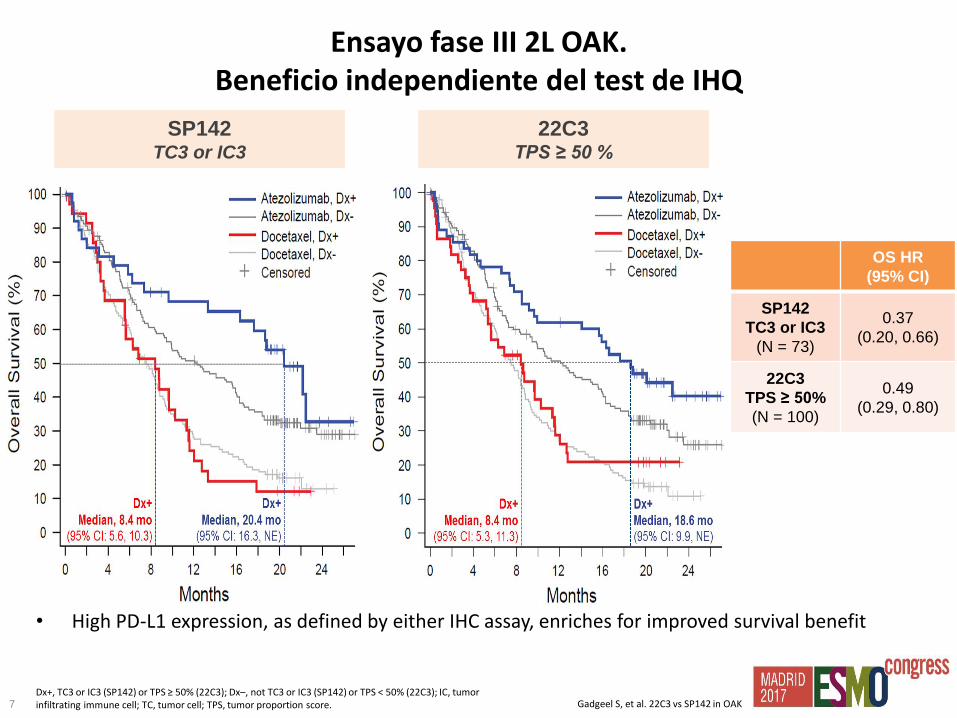
• High PD-L1 expression, as defined by either IHC assay, enriches for improved survival benefit
7 Dx+, TC3 or IC3 (SP142) or TPS ≥ 50% (22C3); Dx–, not TC3 or IC3 (SP142) or TPS < 50% (22C3); IC, tumor infiltrating immune cell; TC, tumor cell; TPS, tumor proportion score. Gadgeel S, et al. 22C3 vs SP142 in OAK
OS HR
(95% CI)
SP142
TC3 or IC3
(N = 73)
0.37
(0.20, 0.66)
22C3
TPS ≥ 50%
(N = 100)
0.49
(0.29, 0.80)
SP142 TC3 or IC3
22C3 TPS ≥ 50 %
Ensayo fase III 2L OAK. Beneficio independiente del test de IHQ
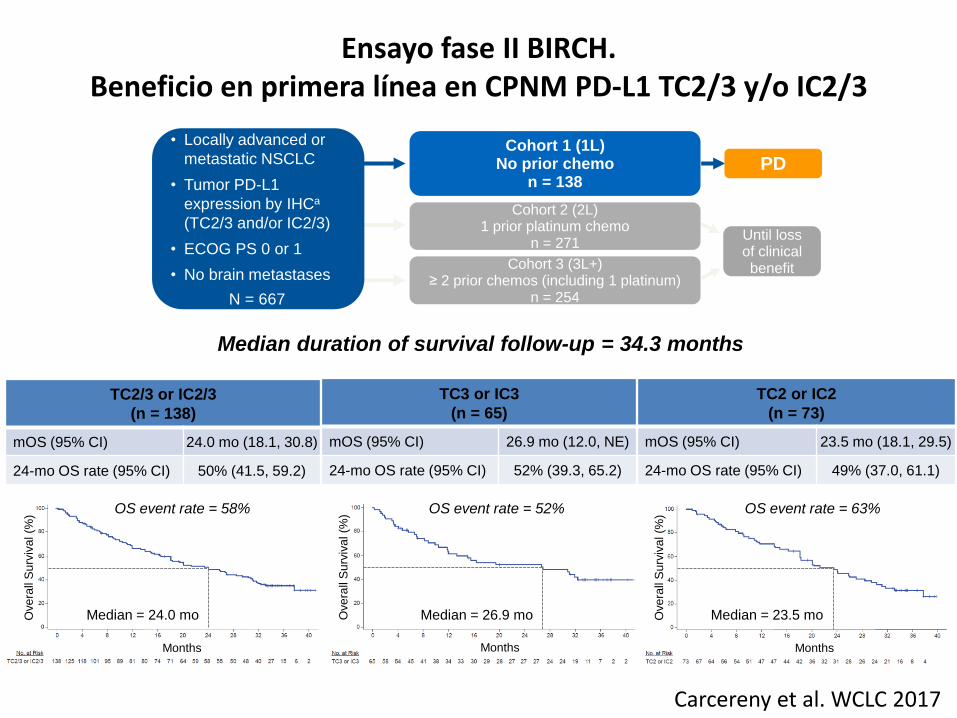
Ensayo fase II BIRCH. Beneficio en primera línea en CPNM PD-L1 TC2/3 y/o IC2/3
Carcereny et al. WCLC 2017
Cohort 1 (1L) No prior chemo
n = 138
Cohort 2 (2L) 1 prior platinum chemo
n = 271
Cohort 3 (3L+) ≥ 2 prior chemos (including 1 platinum)
n = 254
PD
Until loss of clinical benefit
• Locally advanced or
metastatic NSCLC
• Tumor PD-L1
expression by IHCa
(TC2/3 and/or IC2/3)
• ECOG PS 0 or 1
• No brain metastases
N = 667
Median duration of survival follow-up = 34.3 months
TC2/3 or IC2/3
(n = 138)
mOS (95% CI) 24.0 mo (18.1, 30.8)
24-mo OS rate (95% CI) 50% (41.5, 59.2)
TC3 or IC3
(n = 65)
mOS (95% CI) 26.9 mo (12.0, NE)
24-mo OS rate (95% CI) 52% (39.3, 65.2)
TC2 or IC2
(n = 73)
mOS (95% CI) 23.5 mo (18.1, 29.5)
24-mo OS rate (95% CI) 49% (37.0, 61.1)
Ove
rall
Su
rviv
al (%
)
Months
Ove
rall
Su
rviv
al (%
)
Months O
ve
rall
Su
rviv
al (%
) Months
Median = 26.9 mo Median = 24.0 mo Median = 23.5 mo
OS event rate = 52% OS event rate = 58% OS event rate = 63%

Atezolizumab en 2º línea CPNM
• Eficacia demostrada vs Docetaxel.
• Largos supervivientes.
• Beneficio independiente del nivel de expresión de PD-L1.
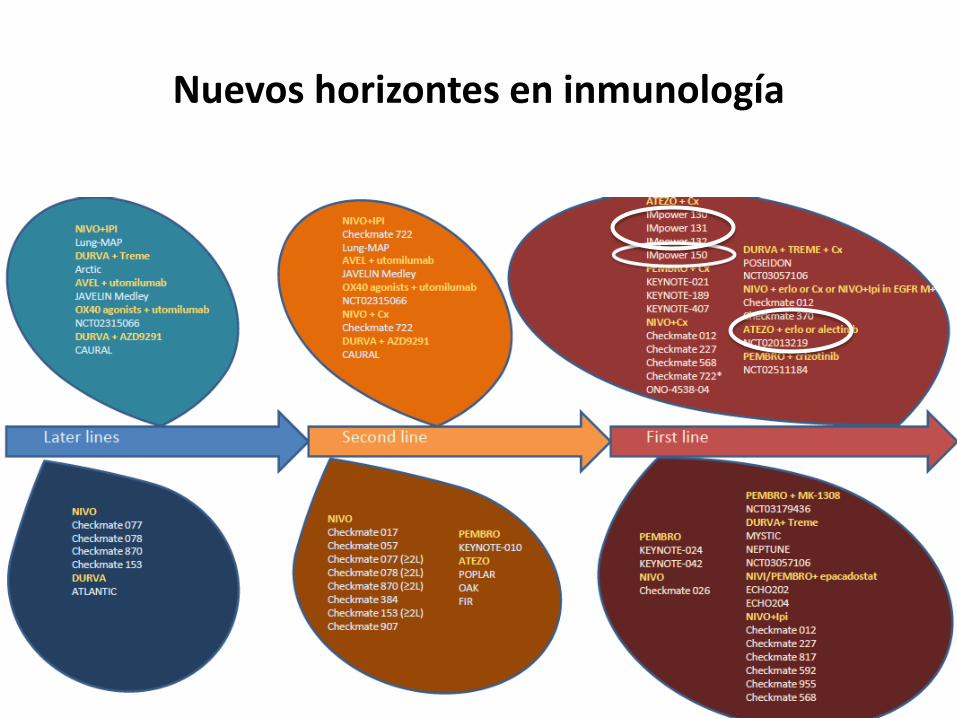
Nuevos horizontes en inmunología
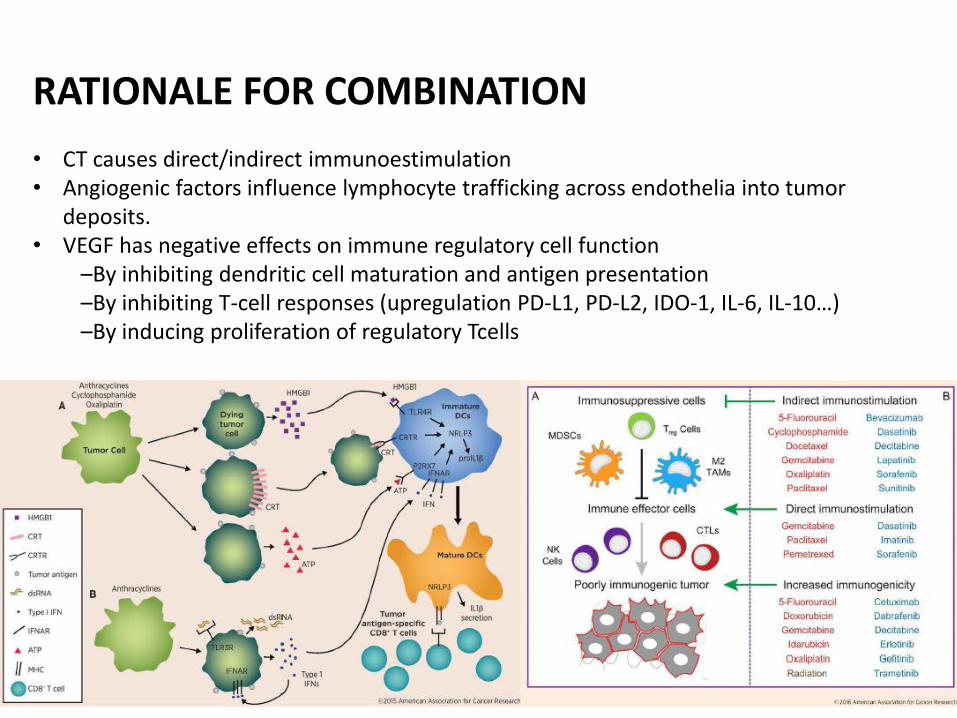
RATIONALE FOR COMBINATION • CT causes direct/indirect immunoestimulation • Angiogenic factors influence lymphocyte trafficking across endothelia into tumor
deposits. • VEGF has negative effects on immune regulatory cell function
–By inhibiting dendritic cell maturation and antigen presentation –By inhibiting T-cell responses (upregulation PD-L1, PD-L2, IDO-1, IL-6, IL-10…) –By inducing proliferation of regulatory Tcells
Reck M, et al. IMpower150 PFS analysis.
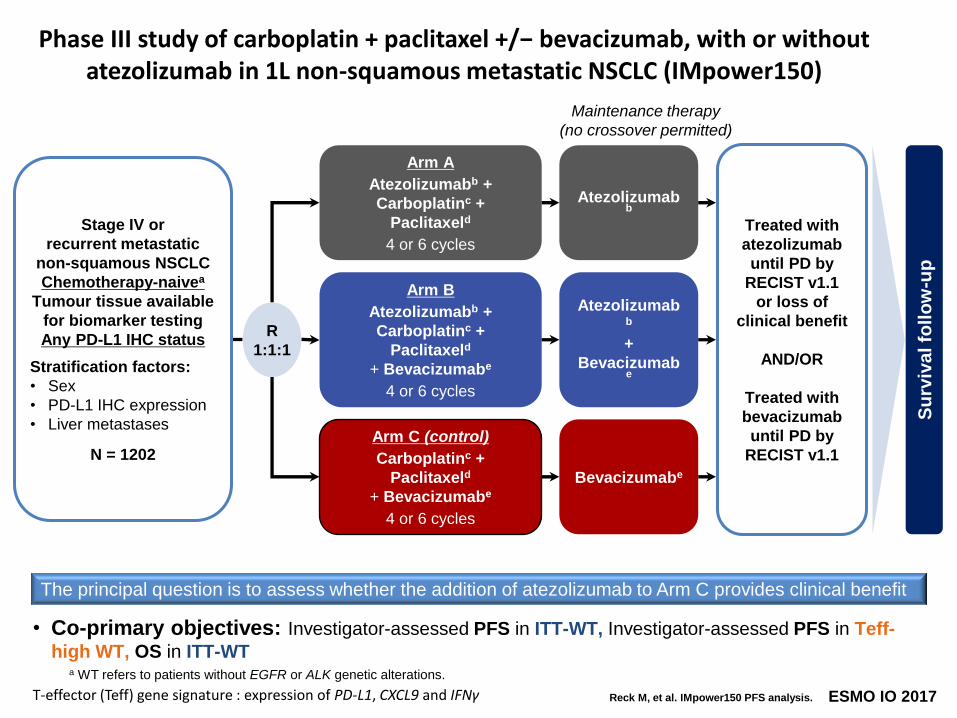
Phase III study of carboplatin + paclitaxel +/− bevacizumab, with or without atezolizumab in 1L non-squamous metastatic NSCLC (IMpower150)
Arm A
Atezolizumabb +
Carboplatinc +
Paclitaxeld
4 or 6 cycles
Atezolizumabb
Arm C (control)
Carboplatinc +
Paclitaxeld
+ Bevacizumabe
4 or 6 cycles
Bevacizumabe
Su
rviv
al fo
llo
w-u
p
Stage IV or
recurrent metastatic
non-squamous NSCLC
Chemotherapy-naivea
Tumour tissue available
for biomarker testing
Any PD-L1 IHC status
Stratification factors:
• Sex
• PD-L1 IHC expression
• Liver metastases
N = 1202
R
1:1:1
Arm B
Atezolizumabb +
Carboplatinc +
Paclitaxeld
+ Bevacizumabe
4 or 6 cycles
Atezolizumabb
+
Bevacizumabe
Maintenance therapy
(no crossover permitted)
Treated with
atezolizumab
until PD by
RECIST v1.1
or loss of
clinical benefit
AND/OR
Treated with
bevacizumab
until PD by
RECIST v1.1
The principal question is to assess whether the addition of atezolizumab to Arm C provides clinical benefit
ESMO IO 2017
• Co-primary objectives: Investigator-assessed PFS in ITT-WT, Investigator-assessed PFS in Teff-
high WT, OS in ITT-WT
T-effector (Teff) gene signature : expression of PD-L1, CXCL9 and IFNγ
a WT refers to patients without EGFR or ALK genetic alterations.
Reck M, et al. IMpower150 PFS analysis.
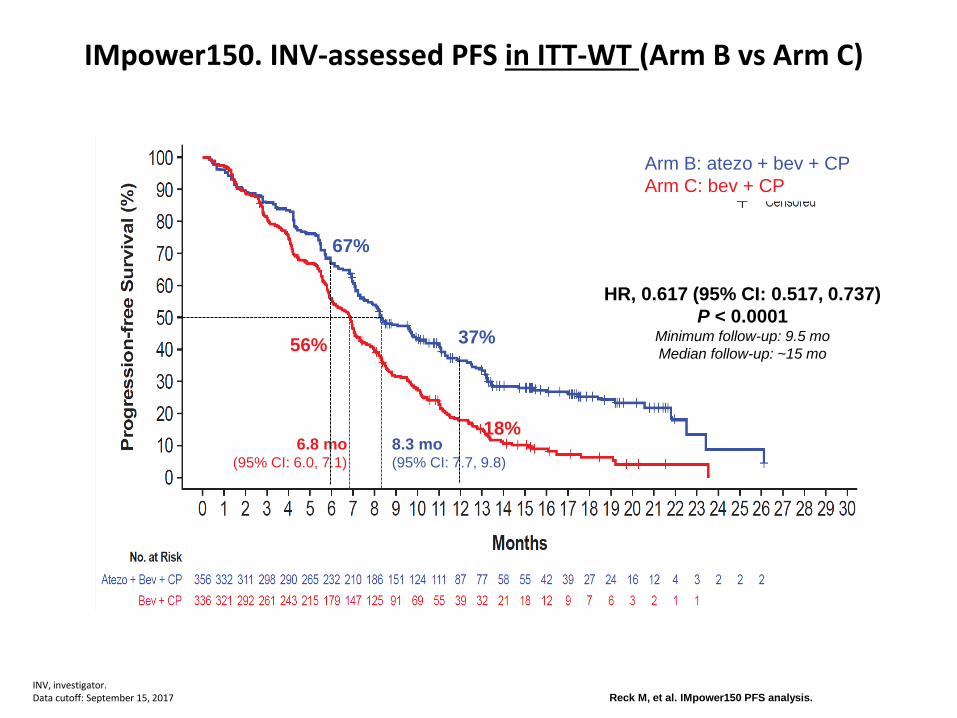
IMpower150. INV-assessed PFS in ITT-WT (Arm B vs Arm C)
INV, investigator. Data cutoff: September 15, 2017
6.8 mo (95% CI: 6.0, 7.1)
8.3 mo (95% CI: 7.7, 9.8)
HR, 0.617 (95% CI: 0.517, 0.737)
P < 0.0001 Minimum follow-up: 9.5 mo
Median follow-up: ~15 mo
Arm B: atezo + bev + CP
Arm C: bev + CP
18%
37% 56%
67%

Reck M, et al. IMpower150 PFS analysis.
INV, investigator. Data cutoff: September 15, 2017
IMpower150. INV-assessed PFS in Teff-high WT (Arm B vs Arm C)
6.8 mo (95% CI: 5.9, 7.4)
11.3 mo (95% CI: 9.1, 13.0)
HR, 0.505 (95% CI: 0.377, 0.675)
P < 0.0001 Minimum follow-up: 9.5 mo
Landmark PFS, % Arm B:
atezo + bev + CP
Arm C:
bev + CP
6-month 72% 57%
12-month 46% 18%
co-primary endpoint T-effector gene signature allows enrichment
Reck M, et al. IMpower150 PFS analysis.
Promising preliminary OS benefit for Arm B vs Arm C was observed; next OS interim data are anticipated in 1H 2018 1
5 Data cutoff: September 15, 2017
Impower 150. Preliminary OS in ITT-WT (Arm B vs Arm C)
HR, 0.775 (95% CI: 0.619, 0.970)
P = 0.0262 Minimum follow-up: 9.5 mo
14.4 mo
(95% CI: 12.8, 17.1)
19.2 mo
(95% CI: 16.8, 26.1)
Arm B: atezo + bev + CP
Arm C: bev + CP
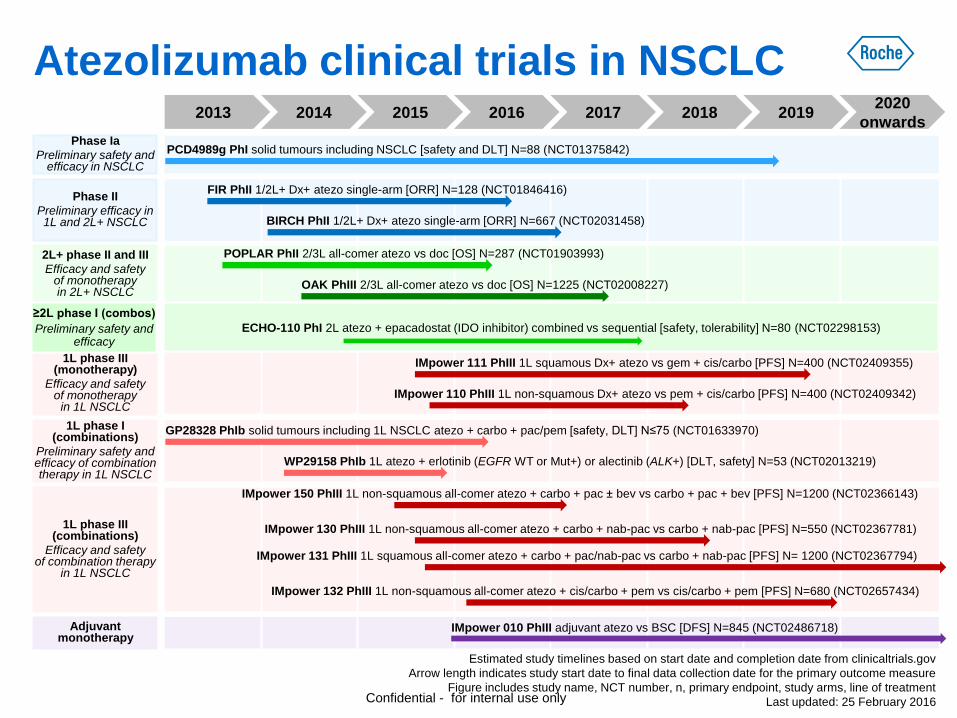
1L phase I (combinations)
Preliminary safety and efficacy of combination therapy in 1L NSCLC
Estimated study timelines based on start date and completion date from clinicaltrials.gov
Arrow length indicates study start date to final data collection date for the primary outcome measure
Figure includes study name, NCT number, n, primary endpoint, study arms, line of treatment
Last updated: 25 February 2016
2013 2016 2017 2018 2019 2020
onwards
2L+ phase II and III
Efficacy and safety of monotherapy in 2L+ NSCLC
2015
1L phase III (combinations)
Efficacy and safety of combination therapy
in 1L NSCLC
Adjuvant monotherapy
IMpower 111 PhIII 1L squamous Dx+ atezo vs gem + cis/carbo [PFS] N=400 (NCT02409355)
PCD4989g PhI solid tumours including NSCLC [safety and DLT] N=88 (NCT01375842)
POPLAR PhII 2/3L all-comer atezo vs doc [OS] N=287 (NCT01903993)
IMpower 131 PhIII 1L squamous all-comer atezo + carbo + pac/nab-pac vs carbo + nab-pac [PFS] N= 1200 (NCT02367794)
GP28328 PhIb solid tumours including 1L NSCLC atezo + carbo + pac/pem [safety, DLT] N≤75 (NCT01633970)
FIR PhII 1/2L+ Dx+ atezo single-arm [ORR] N=128 (NCT01846416)
BIRCH PhII 1/2L+ Dx+ atezo single-arm [ORR] N=667 (NCT02031458)
IMpower 132 PhIII 1L non-squamous all-comer atezo + cis/carbo + pem vs cis/carbo + pem [PFS] N=680 (NCT02657434)
IMpower 110 PhIII 1L non-squamous Dx+ atezo vs pem + cis/carbo [PFS] N=400 (NCT02409342)
WP29158 PhIb 1L atezo + erlotinib (EGFR WT or Mut+) or alectinib (ALK+) [DLT, safety] N=53 (NCT02013219)
OAK PhIII 2/3L all-comer atezo vs doc [OS] N=1225 (NCT02008227)
2014
IMpower 010 PhIII adjuvant atezo vs BSC [DFS] N=845 (NCT02486718)
Phase Ia
Preliminary safety and efficacy in NSCLC
1L phase III (monotherapy)
Efficacy and safety of monotherapy
in 1L NSCLC
Phase II
Preliminary efficacy in 1L and 2L+ NSCLC
IMpower 150 PhIII 1L non-squamous all-comer atezo + carbo + pac ± bev vs carbo + pac + bev [PFS] N=1200 (NCT02366143)
IMpower 130 PhIII 1L non-squamous all-comer atezo + carbo + nab-pac vs carbo + nab-pac [PFS] N=550 (NCT02367781)
Atezolizumab clinical trials in NSCLC
Confidential - for internal use only
≥2L phase I (combos)
Preliminary safety and efficacy
ECHO-110 PhI 2L atezo + epacadostat (IDO inhibitor) combined vs sequential [safety, tolerability] N=80 (NCT02298153)
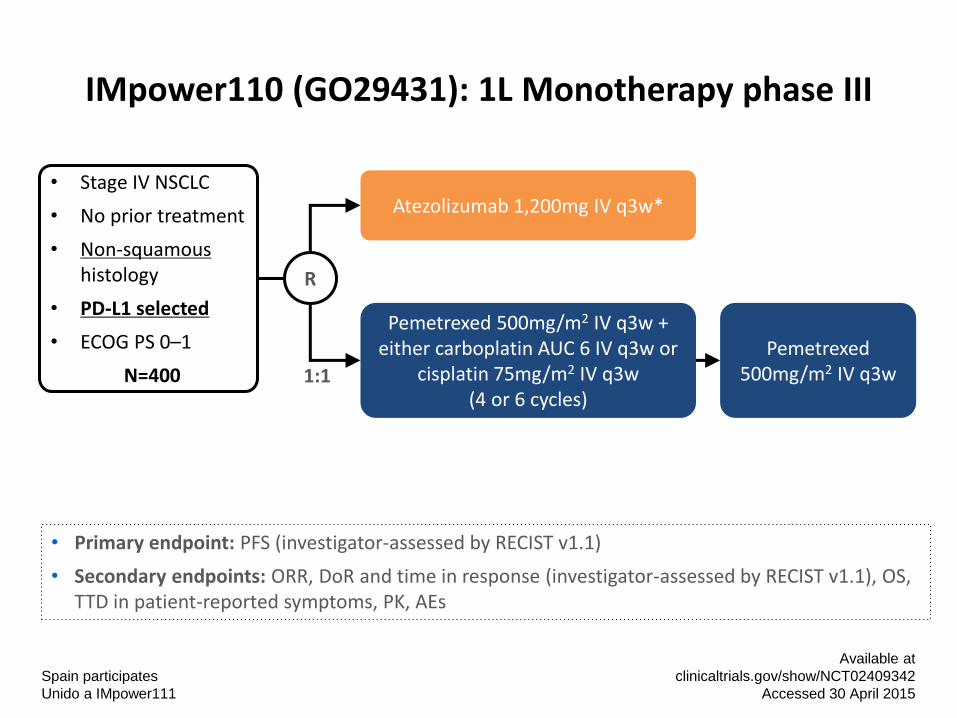
IMpower110 (GO29431): 1L Monotherapy phase III
Available at
clinicaltrials.gov/show/NCT02409342
Accessed 30 April 2015
• Primary endpoint: PFS (investigator-assessed by RECIST v1.1)
• Secondary endpoints: ORR, DoR and time in response (investigator-assessed by RECIST v1.1), OS, TTD in patient-reported symptoms, PK, AEs
Pemetrexed 500mg/m2 IV q3w + either carboplatin AUC 6 IV q3w or
cisplatin 75mg/m2 IV q3w (4 or 6 cycles)
Atezolizumab 1,200mg IV q3w* • Stage IV NSCLC
• No prior treatment
• Non-squamous histology
• PD-L1 selected
• ECOG PS 0–1
N=400 1:1
R
Pemetrexed 500mg/m2 IV q3w
Spain participates
Unido a IMpower111
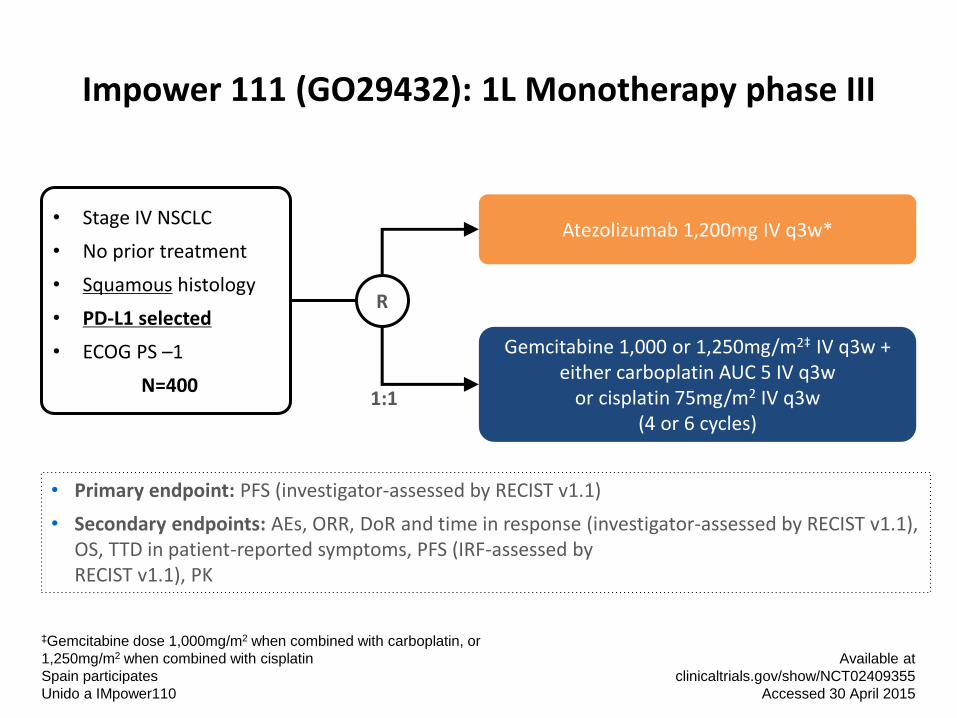
Impower 111 (GO29432): 1L Monotherapy phase III
‡Gemcitabine dose 1,000mg/m2 when combined with carboplatin, or
1,250mg/m2 when combined with cisplatin
Spain participates
Unido a IMpower110
Available at
clinicaltrials.gov/show/NCT02409355
Accessed 30 April 2015
• Primary endpoint: PFS (investigator-assessed by RECIST v1.1)
• Secondary endpoints: AEs, ORR, DoR and time in response (investigator-assessed by RECIST v1.1), OS, TTD in patient-reported symptoms, PFS (IRF-assessed by RECIST v1.1), PK
Gemcitabine 1,000 or 1,250mg/m2‡ IV q3w + either carboplatin AUC 5 IV q3w
or cisplatin 75mg/m2 IV q3w (4 or 6 cycles)
Atezolizumab 1,200mg IV q3w* • Stage IV NSCLC
• No prior treatment
• Squamous histology
• PD-L1 selected
• ECOG PS –1
N=400 1:1
R
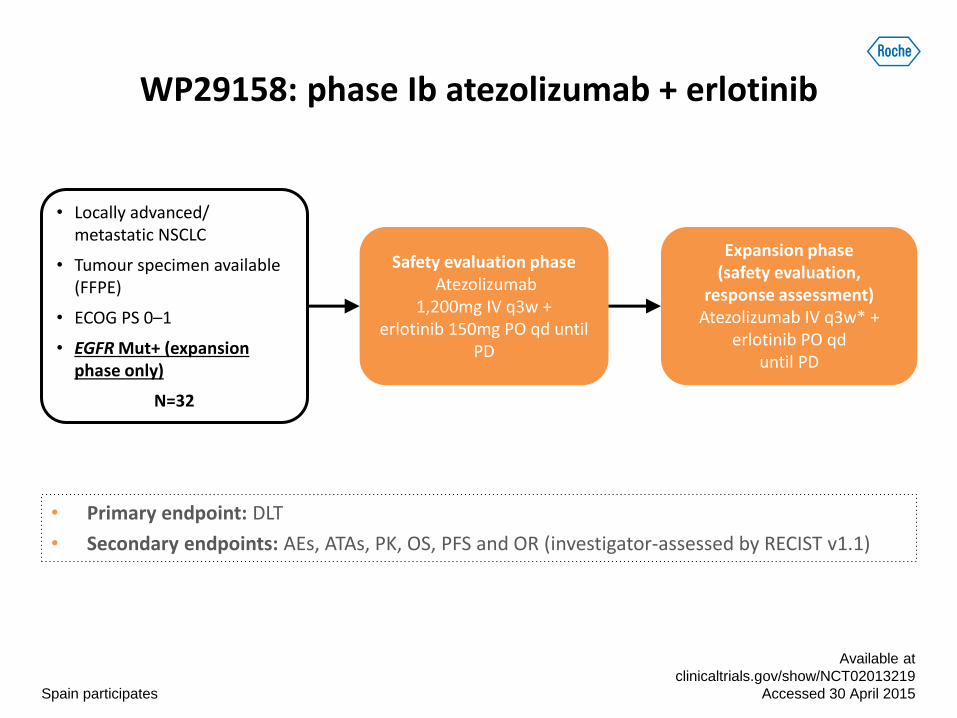
WP29158: phase Ib atezolizumab + erlotinib
• Primary endpoint: DLT
• Secondary endpoints: AEs, ATAs, PK, OS, PFS and OR (investigator-assessed by RECIST v1.1)
Available at
clinicaltrials.gov/show/NCT02013219
Accessed 30 April 2015
• Locally advanced/ metastatic NSCLC
• Tumour specimen available (FFPE)
• ECOG PS 0–1
• EGFR Mut+ (expansion phase only)
N=32
Expansion phase (safety evaluation,
response assessment) Atezolizumab IV q3w* +
erlotinib PO qd until PD
Safety evaluation phase Atezolizumab
1,200mg IV q3w + erlotinib 150mg PO qd until
PD
Spain participates
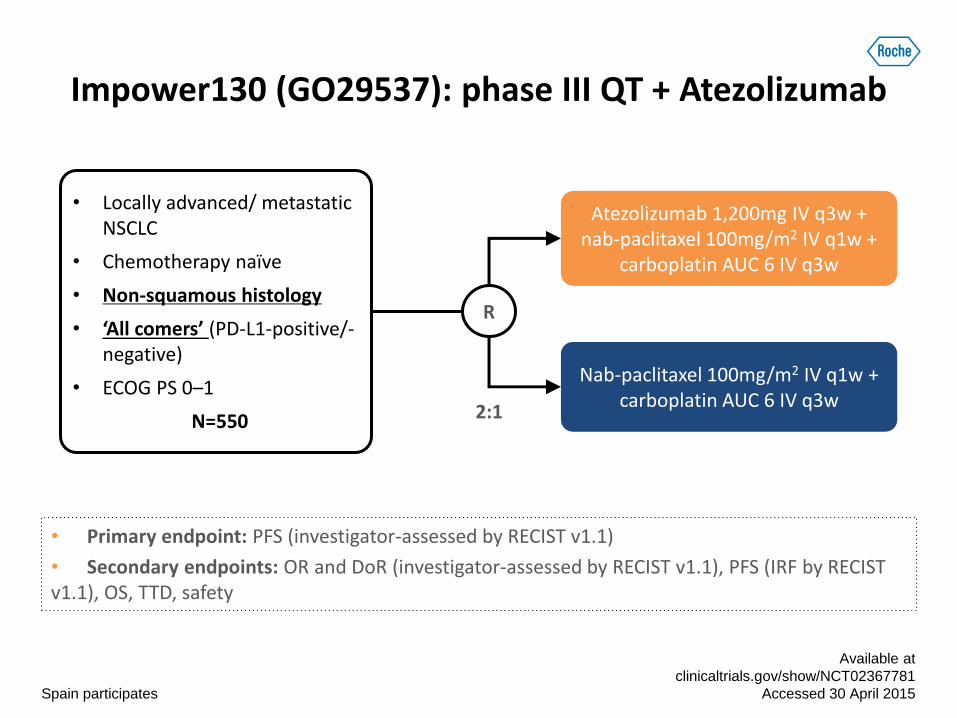
Impower130 (GO29537): phase III QT + Atezolizumab
• Primary endpoint: PFS (investigator-assessed by RECIST v1.1)
• Secondary endpoints: OR and DoR (investigator-assessed by RECIST v1.1), PFS (IRF by RECIST v1.1), OS, TTD, safety
Spain participates
Available at
clinicaltrials.gov/show/NCT02367781
Accessed 30 April 2015
Nab-paclitaxel 100mg/m2 IV q1w + carboplatin AUC 6 IV q3w
Atezolizumab 1,200mg IV q3w + nab-paclitaxel 100mg/m2 IV q1w +
carboplatin AUC 6 IV q3w
• Locally advanced/ metastatic NSCLC
• Chemotherapy naïve
• Non-squamous histology
• ‘All comers’ (PD-L1-positive/-negative)
• ECOG PS 0–1
N=550 2:1
R
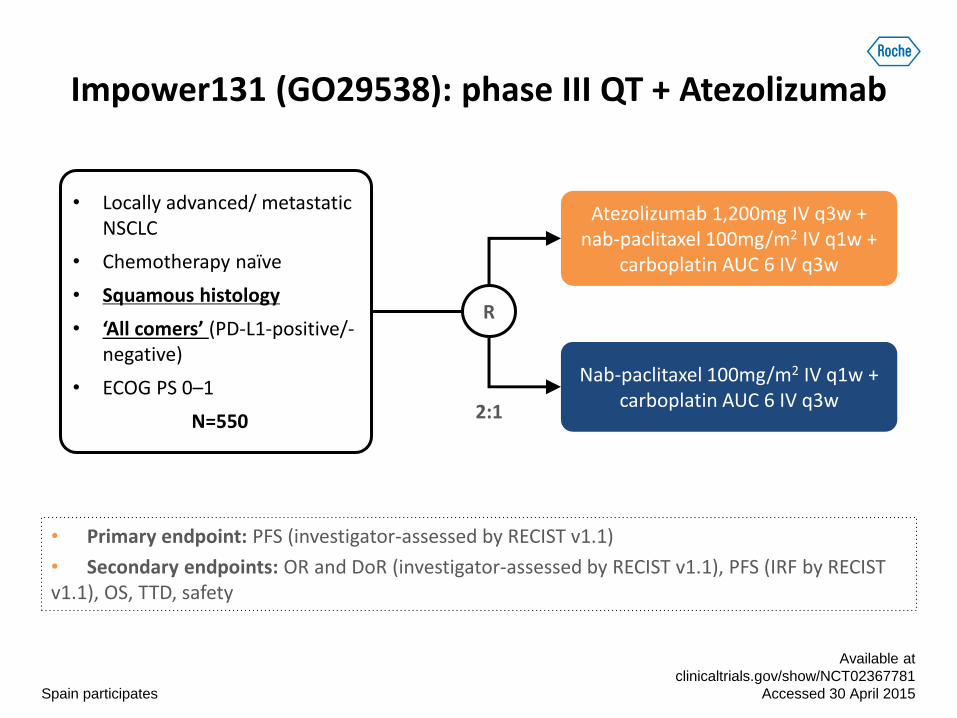
Impower131 (GO29538): phase III QT + Atezolizumab
• Primary endpoint: PFS (investigator-assessed by RECIST v1.1)
• Secondary endpoints: OR and DoR (investigator-assessed by RECIST v1.1), PFS (IRF by RECIST v1.1), OS, TTD, safety
Spain participates
Available at
clinicaltrials.gov/show/NCT02367781
Accessed 30 April 2015
Nab-paclitaxel 100mg/m2 IV q1w + carboplatin AUC 6 IV q3w
Atezolizumab 1,200mg IV q3w + nab-paclitaxel 100mg/m2 IV q1w +
carboplatin AUC 6 IV q3w
• Locally advanced/ metastatic NSCLC
• Chemotherapy naïve
• Squamous histology
• ‘All comers’ (PD-L1-positive/-negative)
• ECOG PS 0–1
N=550 2:1
R
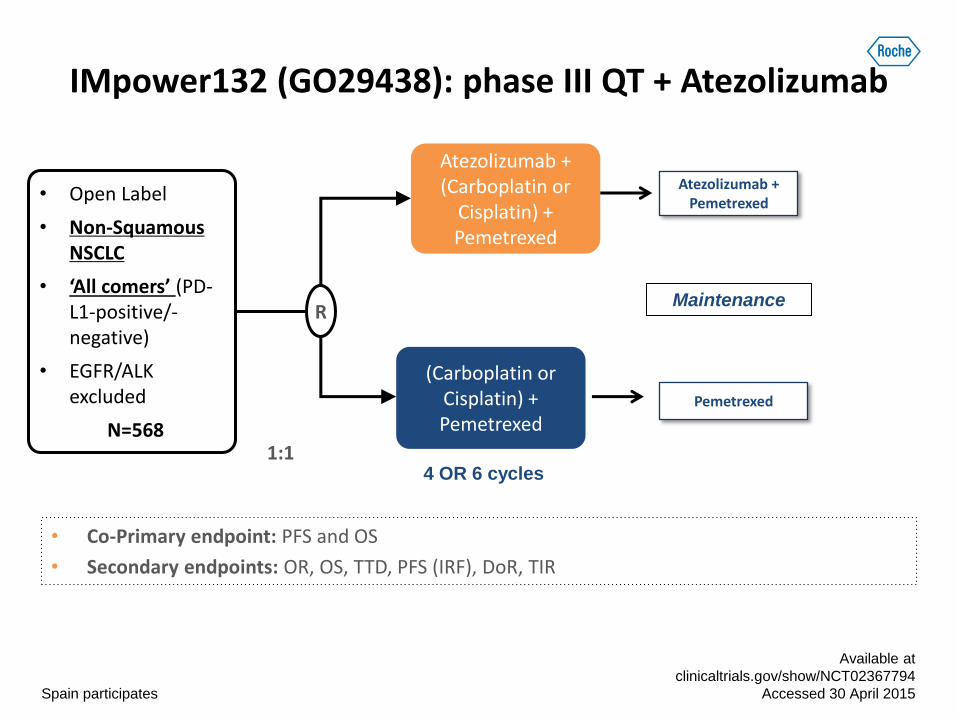
IMpower132 (GO29438): phase III QT + Atezolizumab
• Co-Primary endpoint: PFS and OS
• Secondary endpoints: OR, OS, TTD, PFS (IRF), DoR, TIR
Spain participates
Available at
clinicaltrials.gov/show/NCT02367794
Accessed 30 April 2015
(Carboplatin or Cisplatin) + Pemetrexed
Atezolizumab + (Carboplatin or
Cisplatin) + Pemetrexed
• Open Label
• Non-Squamous NSCLC
• ‘All comers’ (PD-L1-positive/-negative)
• EGFR/ALK excluded
N=568 1:1
R
Atezolizumab + Pemetrexed
Pemetrexed
Maintenance
4 OR 6 cycles
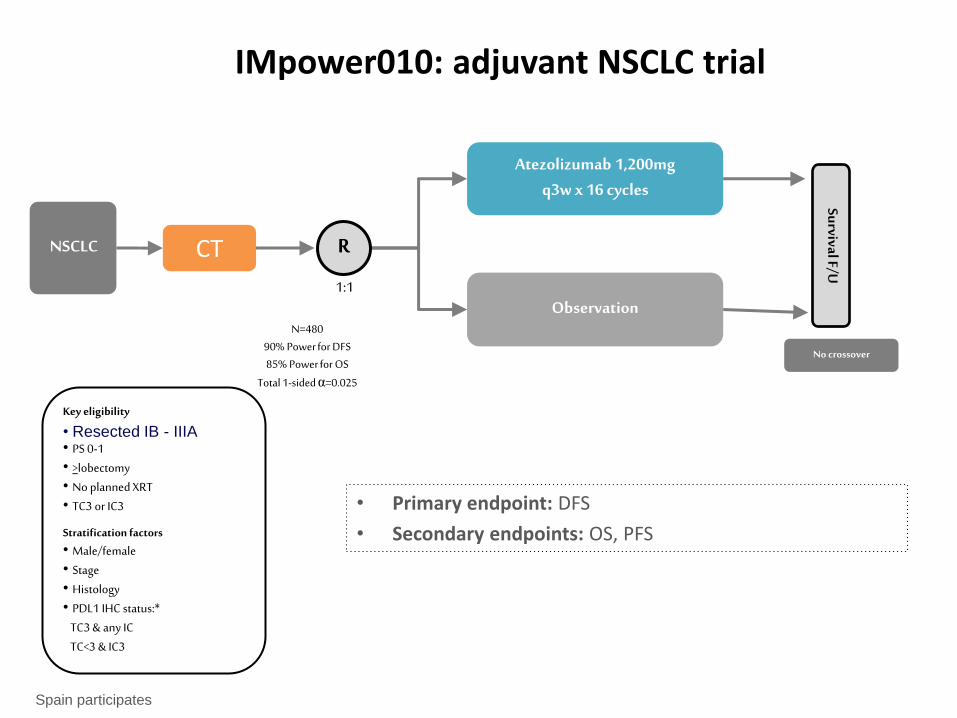
IMpower010: adjuvant NSCLC trial
Key eligibility
• Resected IB - IIIA • PS 0-1 • >lobectomy • No planned XRT • TC3 or IC3
Stratification factors
• Male/female • Stage • Histology • PDL1 IHC status:* TC3 & any IC TC<3 & IC3
Atezolizumab 1,200mg q3w x 16 cycles
Observation
NSCLC
No crossover
Survival F/U
N=480 90% Power for DFS 85% Power for OS
Total 1-sided α=0.025
1:1
R CT
Spain participates
• Primary endpoint: DFS
• Secondary endpoints: OS, PFS
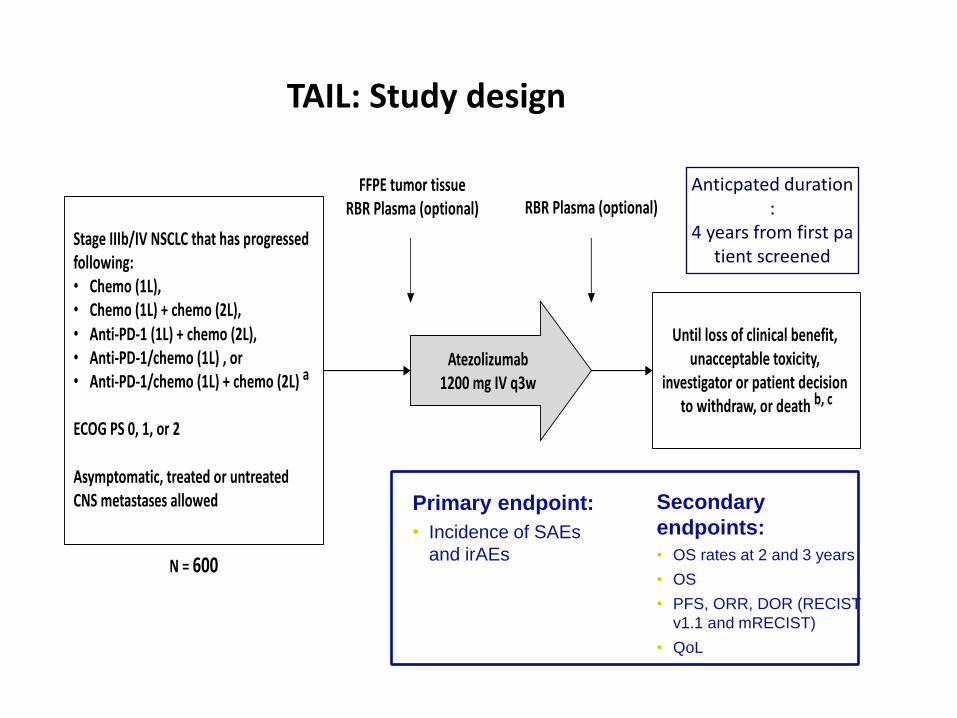
StageIIIb/IVNSCLCthathasprogressedfollowing:• Chemo(1L),• Chemo(1L)+chemo(2L),• Anti-PD-1(1L)+chemo(2L),• Anti-PD-1/chemo(1L),or• Anti-PD-1/chemo(1L)+chemo(2L)a
ECOGPS0,1,or2
Asymptomatic,treatedoruntreatedCNSmetastasesallowed
Untillossofclinicalbenefit,unacceptabletoxicity,
investigatororpatientdecisiontowithdraw,ordeath b,c
Atezolizumab1200mgIVq3w
FFPEtumortissueRBRPlasma(optional) RBRPlasma(optional)
N=600
TAIL: Study design
Primary endpoint:
• Incidence of SAEs
and irAEs
Secondary
endpoints:
• OS rates at 2 and 3 years
• OS
• PFS, ORR, DOR (RECIST
v1.1 and mRECIST)
• QoL
Anticpated duration:
4 years from first patient screened
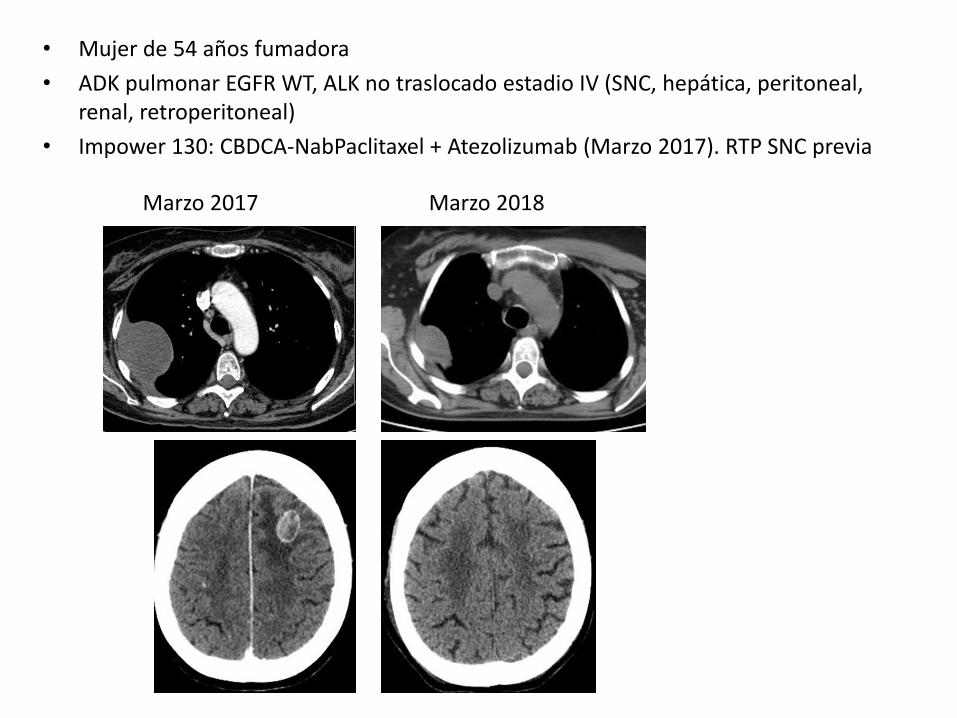
• Mujer de 54 años fumadora
• ADK pulmonar EGFR WT, ALK no traslocado estadio IV (SNC, hepática, peritoneal, renal, retroperitoneal)
• Impower 130: CBDCA-NabPaclitaxel + Atezolizumab (Marzo 2017). RTP SNC previa
Marzo 2017 Marzo 2018
CONCLUSIONES
• Eficacia demostrada en 2º línea, independiente de la histología y del nivel de expresión de PD-L1. LARGOS SUPERVIVIENTES
• Perfil de toxicidad manejable, en monoterapia o en combinación con QT.
• Numerosos estudios en marcha (monoterapia, Combos) en distintas indicaciones.
• Posibilidad de beneficiarse en un futuro de Atezolizumab en diferentes escenarios (adyuvancia, 1º línea, monoterapia, combinación, ….)

Gracias!!!!!
Dra. Margarita Majem
Hospital de la Santa Creu i Sant Pau
Barcelona