nsclc epidemiology - continuing medical …supportive care plus cisplatincisplatin--based regimens...
TRANSCRIPT

1
Advances in Internal MedicineAdvances in Internal MedicineLUNG CANCERLUNG CANCER
What’s old, what’s new, and what to What’s old, what’s new, and what to expectexpect
Thierry M. Jahan, M.D.,Thierry M. Jahan, M.D.,Thoracic Oncology ProgramThoracic Oncology Program
UCSF Helen Diller Family Comprehensive UCSF Helen Diller Family Comprehensive Cancer CenterCancer Center
Objectives
• Recognize the changing epidemiology of lung cancer
• Understand the treatment options for early and advanced disease
• Recognize the role of targeted agents and their toxicities
• Recognize the heterogeneity of lung cancer and tumor biology based individualized treatments
• EPIDEMIOLOGY
Jemal, CA Cancer J Clin 2008; 58: 71
Cancer Incidence Deaths
Colon 108,070 49,960
Breast 184,450 40,930
Prostate 186,320 28,660
Total 478,840 119,550
NSCLC Epidemiology
LungLung 215,020215,020 161,840161,840
Statistics for 2008

2
Prototypical U.S. Lung Cancer patient 1950’s-60’s
• 60-70 Year Old Males
• Long Smoking History
• Large Squamous Cell Tumors
• Cowboy Image• Started in 1950s
The Changing Face of Lung Cancer in the U.S.
Annual Age-adjusted Cancer Death Rates, US 1930-2002
Men Women
1987
Etiology Smoking and lung cancer incidence

3
Etiology:Environmental causes
� Smoking:� Tars, tobacco, aromatic amines, Polycyclic aromatic
hydrocarbons
� Environmental:� Second hand smoke, radon
� Occupational:– Asbestos, uranium, beryllium, vinyl chloride, nickel chromates,
coal products, mustard gas, chloromethyl ethers, gasoline , diesel exhaust
Smoking cessation and mortality in women
Nurses Health Study• 104,519 subjects• Lung CA OR Current smokers 21.87(17.85-26.80)
– Past smokers 4.93 (4.00-6.08)
Kenfield, JAMA 2008; 299: 2037
Effect of smoking cessationLung cancer mortality: 21%↓ first 5 yrs
87% ↓ 20-30yrs93% ↓ ≥ 30 yrs
All cause mortality: Level of non-smoker 20yrs
Lung cancer in never smokers
• Women are more likely than men to have non-smoking related cancer
• Incidence rates/100,000:• Women 15-20 Men 4-13.7
• Higher frequency of adenocarcinoma
Wakelee et al, J Clin Oncol, 2007; 25: 472
Gender differences and risk of lung cancer (LC) with smoking
• OR LC in smokers : women 1.2-1.7 times higher than men when adjusted for tobacco dose exposure
• RR for LC in smokers: women 27.9 and men 9.6
Zang, JNCI 1996;88:183
Risch, Am J Epi, 1993;138:281
Schoenberg, Am J Epi 1989;130:688

4
Gender differences in biology
�CYP and GSTM 1 (glutahtione S-transferases) :2 enzyme systems for the metabolism of PAH and intermediate products of tobacco smoke.
�CYP1A1 *2A and *2B assoc with inc risk of LC (OR 4.7 CI 1.2-19)�GSTTI null phenotype OR 1.2 (CI1.0-1.6)
F –OR 3.0 (1.09-8.4) M – OR 1.4 (.5-4.0)
�Higher levels of DNA adducts
Taioli, Int J Epi 2003;32:60
Tang, Carcinogensis, 1998;19:1949
Gender differences in biology
• Hormones and lung cancer• Estrogen receptors are present in lung tumors• Estradiol promotes growth of lung tumors in
preclinical models• Conflicting reports on the influence of hormones
on development of LC in case control and cohort studies
• HRT adversely affects treatment outcomes (MS 79 vs 39 mo p=0.02)
Dubey , Lancet Oncol, 2006, 7:416Ganti, JCO 2005,24:59
SCREENING
National Cancer Institute: SEER Cancer Statistics Review, 1975National Cancer Institute: SEER Cancer Statistics Review, 1975--2001.2001.
Stage IV36%
Unstaged8%
Stage III37%
Stage Stage I/III/II
16%16%
Lung Cancer Stage Distribution at Time of Diagnosis

5
Screening
• IELCAP (Early Lung Cancer Action Program)
• 31,567 H/O tobacco use, second hand , occupational exposure, radon.
• Baseline and annual CT screening• 5500 Positive results requiring further w/u• 535 required biopsy• Lung cancer detected in 484 (1.6%) of which 85%
stage I.
NEJM 2006, 357, 17
Screening
• NLST (National lung screening trial)• Randomized comparison of CT and CXR
• 50,000 enrolled and closed to accrual• Enpoint: survival• Results expected ~ 2009
TREATMENT
Principles of Cancer Therapy
• Diagnosis
• Stage
• Medical condition (performance status, co-morbid diseases)

6
Performance statusKarnofsky Scale Zubrod Scale
Normal, no evidence of disease 100 Able to perform normal activity with only minor 90 symptoms
Normal activity 0
Normal activity with effort, some symptoms 80Able to care for self but unable to do 70normal activities
Symptomatic and ambulatory 1
Cares for self
Requires occasional assistance, cares for 60most needs Requires considerable assistance 50
Ambulatory >50% of time 2
Occasional assistance
Disabled, requires special assistance 40
Severely disabled 30
Ambulatory ≤50% of the time 3
Nursing care needed
Very sick, requires active supportive 20treatment Moribund 10
Bedridden 4
Treatment of NSCLC
• Practically 3 groups:
Local : stage I, II, some IIIA → surgery
adjuvant chemotherapy
Regional: some IIIA, IIIB, → RT ± chemo
Metastatic: Systemic Rx (cytotoxics and targeted agents)
• Early NSCLC
Evolution In Approach To SurgeryOpen or Closed: Does Size Matter?
Thoracotomy Thoracoscopy
7
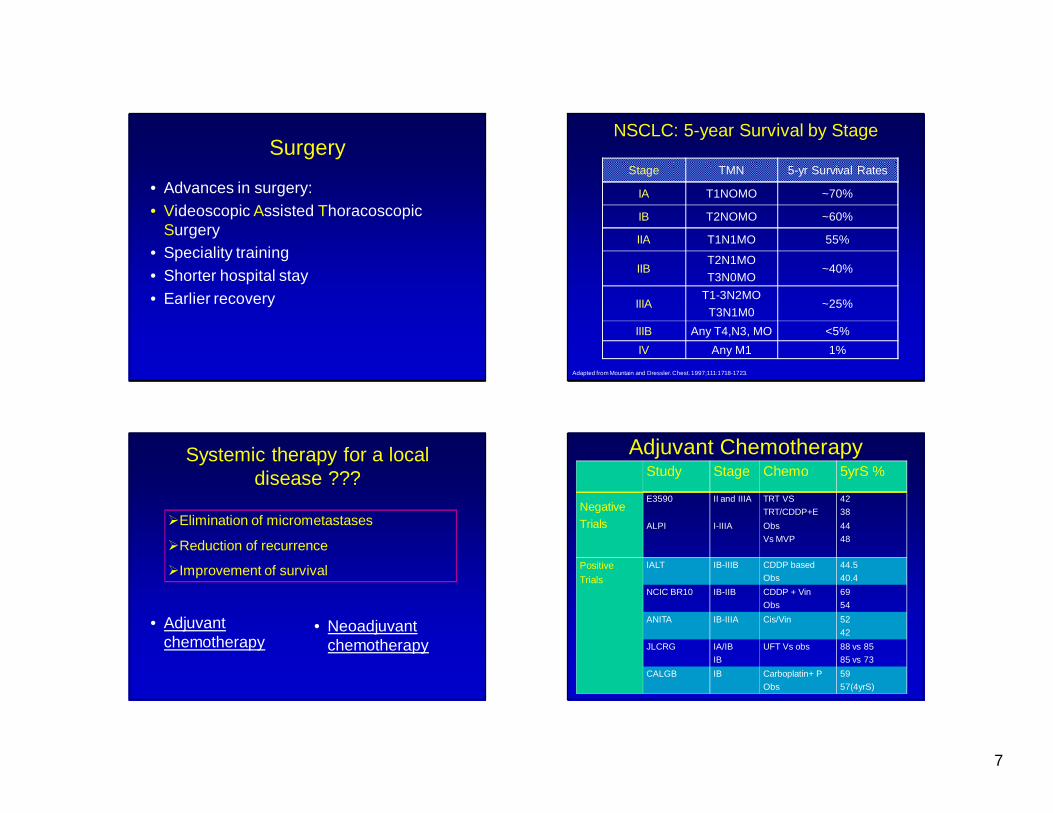
Surgery
• Advances in surgery:• Videoscopic Assisted Thoracoscopic
Surgery• Speciality training• Shorter hospital stay• Earlier recovery
NSCLC: 5-year Survival by Stage
Stage TMN 5-yr Survival Rates
IA T1NOMO ~70%
IB T2NOMO ~60%
IIA T1N1MO 55%
IIBT2N1MO
T3N0MO~40%
IIIAT1-3N2MO
T3N1M0~25%
IIIB Any T4,N3, MO <5%
IV Any M1 1%
Adapted from Mountain and Dressler. Chest. 1997;111:1718-1723.
Systemic therapy for a local disease ???
• Adjuvant chemotherapy
• Neoadjuvant chemotherapy
�Elimination of micrometastases
�Reduction of recurrence
�Improvement of survival
Adjuvant Chemotherapy
Negative
Trials
Study Stage Chemo 5yrS %
E3590 II and IIIA TRT VS
TRT/CDDP+E
42
38
ALPI I-IIIA Obs
Vs MVP
44
48
Positive
Trials
IALT IB-IIIB CDDP based
Obs
44.5
40.4
NCIC BR10 IB-IIB CDDP + Vin
Obs
69
54
ANITA IB-IIIA Cis/Vin 52
42
JLCRG IA/IB
IB
UFT Vs obs 88 vs 85
85 vs 73
CALGB IB Carboplatin+ P
Obs
59
57(4yrS)

8
5yr OS �15%
MST 73 mo vs 94 mo
Winton ASCO 2004, N Engl J Med 2005; 352:2589-2597 Overall survival - ITT population
Months
Su
rviv
al D
istr
ibu
tion
Fu
nct
ion
1.00
0.75
0.50
0.25
00 20 40 60 80 100 120
OBS.. NVB + CDDP
Median months 43.8 65.8
5yr S 52% 42%
P-value 0.013
Hazard Ratio 0.79 [0.66 -0.95]
Obs
NVB + CDDP
ANITA Trial
Douillard, ASCO, 2005.7
Adjuvant chemotherapy in the elderly
•• OS for >65 was better with chemo vs obs OS for >65 was better with chemo vs obs
HR 0.61 (CI 0.38HR 0.61 (CI 0.38--0.98) p0.98) p--0.040.04• OS lesser for patients >75 compared to those aged 66-74
HR 1.95 (CI 1.11-3.41, p-0.02)
Pepe et al , ASCO 2006, 24: Abstract # 7009
Early Lung cancerWhat’s new?
Good Performance Status
Should be offered to >65 yrs
Those over the age of 75 require further study
� VATS procedures can reduce surgical morbidity
�Adjuvant chemotherapy is the Standard of Care for resected NSCLC
9
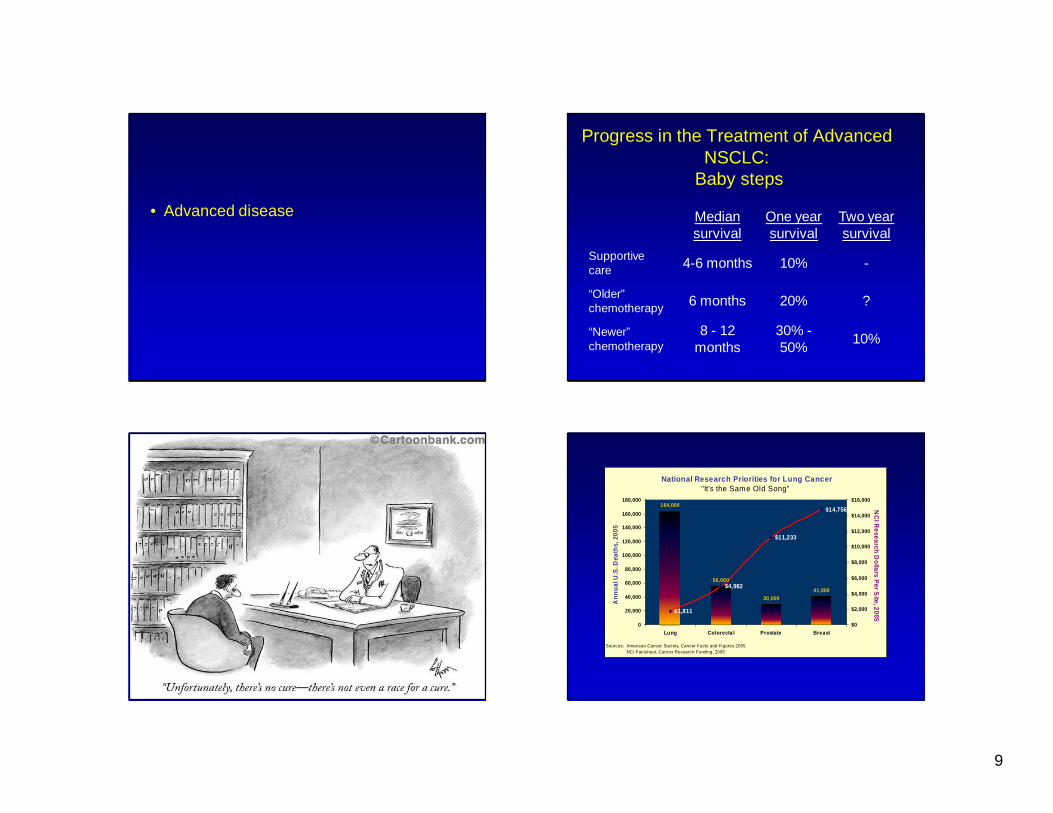
• Advanced disease
Progress in the Treatment of Advanced NSCLC:
Baby steps
Median survival
One year survival
Two year survival
Supportive care 4-6 months 10% -
“Older” chemotherapy 6 months 20% ?
“Newer” chemotherapy
8 - 12 months
30% -50%
10%
164,000
56,000
30,00041,000
$1,811
$4,982
$11,233
$14,756
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
Lung Colorecta l Prostate Breast
Sources: American Cancer Society, Cancer Facts and Figures 2005NCI Factsheet, Cancer Research Funding, 2005
Ann
ual U
.S. D
eath
s, 2
005
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
National Research Priorities for Lung Cancer"It's the Same Old Song"
NC
I Research D
ollars Per S
ite, 2005

10
• Treatment of advanced diseaseCytotoxic chemotherapyTargeted agents
NonNon--small Cell Lung Cancer Collaborative Group. small Cell Lung Cancer Collaborative Group. BMJ.BMJ. 1995;311:8991995;311:899--909.909.
NSCLC - Chemotherapy
Supportive care plus Supportive care plus cisplatincisplatin--based regimensbased regimens
Supportive careSupportive care
PercentagePercentageSurvivalSurvival
6060
100100
Time From Randomization (months)Time From Randomization (months)66 1212 1818 2424
0000
2020
7070
3030
9090
5050
8080
4040
1010
•• P P =.09, in favor of chemotherapy=.09, in favor of chemotherapy•• HR 0.73HR 0.73
Platinum Chemotherapy Versus Supportive Care in NSCLC
First line chemotherapy for NSCLC
Schiller et al. NEJM 2002;346:92
MS 7.9mo 1yrS 33%
0 5 10 15 20 25 30
Months
0.0
0.2
0.4
0.6
0.8
1.0
Survival by Treatment GroupAll Randomized Cases
Cis/PaclitaxelCis/GemcitabineCis/DocetaxelCarbo/Paclitaxel
0 5 10 15 20 25 30
Months
0.0
0.2
0.4
0.6
0.8
1.0
Survival by Treatment GroupAll Randomized Cases
Cis/PaclitaxelCis/GemcitabineCis/DocetaxelCarbo/Paclitaxel
65 yr old male with lung cancer and good PS progresses after 4 cycles of carboplatin
and paclitaxel. What would you recommend?
2 mo r e
c y cl e s
o f sa m
e c .. .
D i ff e r e
n t si n g l
e a ge n t
c y .. .
S i ng l e
a g en t t
a r ge t e
d t .. .
R ef e r
t o ho s p
i c e
0%
17%
65%
17%
1. 2 more cycles of same chemo just in case more is better
2. Different single agent cytotoxic chemotherapy
3. Single agent targeted therapy4. Refer to hospice

11
Response(%)Median survival (months)
1-year-survival (%)
Docetaxel 75 mg/m2 (n=55)Best supportive care (n=49)
0 3 6 9 12 15 18 21
Cumulative probability
0.0
0.2
0.4
0.6
0.8
1.0
Doc 67.5 37
BSC
4.612
p=0.03
Survival time (months)
Relapsed disease
�QOL with Docetaxel
Shepherd, J Clin Oncol 2000, 18:2095
Second Line TherapyPemetrexed vs. Docetaxel
Pemetrexed (n=283) Docetaxel (n=288)
Sur
viva
l Dis
trib
utio
n F
unct
ion
Months
0.00
0.25
0.50
0.75
1.00
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0 22.5
MST 8.3 mos1-yr OS: 29.7%
HR 0.99
95% CI of HR (0.82, 1.20)
MST 7.9 mos1-yr OS: 29.7%
Hanna JCO, 2004,22:1589
Single agents used in second line therapy
JCO 2004,
18:3722
Single agents used in second line therapy

12
• Treatment of advanced diseaseCytotoxic chemotherapyTargeted therapy
“Normalizing” Tumor Vasculature withAnti-angiogenic Therapy
R.K. Jain. Nat Med 7:987, 2001R.K. Jain. Nat Med 7:987, 2001
“Pruning” of abnormal immature vessels with chemo. Results in better delivery of therapeutics
Ultimately results in blood supply unable to support tumor growth
Bevacizumab Blocks Angiogenesis
Recombinant humanized monoclonal antibody to VEGF-A

13
E4599. Ph III RCT :Bevacizumab and CP vs CP in non-squamous NSCLC
RANDOMIZE
Paclitaxel 200 mg/m 2 IV + Carboplatin AUC 6 IV q 3 wk
X6 cycles
Paclitaxel 200 mg/m2 IV + Carboplatin AUC 6 IV q 3 wk
X6 cyclesBevacizumab 15mg/kg q3 wk til PD
Stratification by:
• Stage (IIIB or IV)
• Geographic regionSandler. NEJM 2006; 355: 2542
IIIB and IV non-squamous
No brain mets
No hemoptysis
No prior chemotherapy
Sandler, ASCO annual meeting, 2005,LBA4
Bevacizumab related toxicity
PC PCB
Gr 4/5 Neutropenia
Hypertension
16.4%
0.7
24%
6%
Gr ¾ Thromboembolism
3% 3.8%*
Hemorrhage 1% 4%
Rx related deaths 2 9 (5 due to hemoptysis)
* p=NS
Epidermal Growth Factor Receptor (EGFR)
Baselga. Eur J Cancer 2001;37 Suppl 4:S16-S22.

14
Tyrosine Kinase Inhibitors
Gefitinib EGFR NSCLCErlotinib EGFR NSCLCImatinib PDGF/C-kit/Bcr-Abl CML,GISTSunitinib VEGF, PDGF, CKIT, RET RCC, GISTCI1033 Pan ERBB (irreversible)GW572016 EGFR/ErbB-2EKB 569 EGFRPTK 787 VEGF, PDGFAMG 706 VEGF PDGF CKIT RET
TGFαTGFα
TKI TKI
Erlotinib (Tarceva)- Phase III BR 21
ECOG PS 1,2,3Prior 1-2 regimens
Erlotinib 150 mg/d Placebo 150 mg/d
Stratification
PS : 0/1 vs 2/3
Prior chemo: 1 vs 2
Prior response to chemo: CR vs PR vs SDShepherd et al, NEJM, 2005, 353:123
Shepherd et al. ASCO 2004 # 7022
Radiographic responses to erlotinib can be dramatic and sustained

15
Significant Clinical predictors to response
Overall response %
P value
Gender Male
Female
6
14
0.006
Histology Adenoca
Other
14
4
<0.001
Ethnic group Asian
Other
19
7.5
0.02
Smoking status Current or ever
Never
12
23
<0.001
Toxicities of EGFR -TKIs
• Acneiform rash 60%• Diarrhea 50%• Transaminitis• Anorexia• Wt loss• Interstitial lung
disease <2%
Rx: moisturizing lotionssun screentopical steroids, clindamycin, Doxycycline
Sur
viva
l dis
trib
utio
n fu
nctio
n
Months
Grade 2/3 (n=17)
Grade 1 (n=26)
No rash (n=14)
Median survival (95% CI)
No rash 1.5 (1–2.2) Grade 1 8.5 (4.8–14.8) p<0.0001*
Grade 2/3 19.6 (10.8–22.1+) p<0.0001*
0 5 10 15 20 25 30
1.00
0.75
0.50
0.25
0.00
*vs no rash
Pérez-Soler R, et al. Lung Cancer 2003;41(Suppl. 2): S246 (Abs. P-611)
Erlotinib
Survival by rash
• SPECIAL POPULATIONS• The elderly

16
Age in Lung CancerRelationship to Prognosis ?????
• MSKCC (JCO 4:1604, 1986)
• ECOG (JCO 4:702, 1986)
• ECOG (JCO 23:175,2005)
– prognosis not related to age– Elderly experience more toxicities
• SWOG (JCO 1991;9:1618)
– Elderly – favorable survival
Randomized Trial of Vinorelbine vs. BSC in the Elderly
The ELVIS Trial
R
A
N
D
O
M
I
Z
E
N
MS
1 yr Survival
QOL
Better
Vinorelbine 80 28 wks 32%
BSC 81 21 wks. 14%
Gridelli, Oncologist 2001;6(S1) 4-7
Chemo-naive
>70 yrs
Treatment in advanced disease
• Conclusions• Multiple cytotoxic chemotherapy available• Options also include targeted agents • Treatment is associated with prolongation
of survival and improved symptoms• Treatment choice is dependent on
performance status, co-morbidities
Treatment in advanced disease
• Conclusions• Be aware of toxicities of targeted agents• Age is not a discriminator in treatment
decisions . Elderly “fit” should be offered anti-cancer treatments.

17
Individualized therapy - Genomic predictors?
Potential Biomarkers for Lung Cancer Treatment
• Platinum – ERCC1• Taxanes – BRCA1• Gemcitabine – RRM1• Pemetrexed – TS expression• Gene expression• EGFR – EGFR mutation, FISH• VEGF - ??
Excision Repair Cross Complementing-1 Enzyme
(ERCC1)
• Involved in DNA repair after damage from cisplatin
• High levels of DNA repair enzyme are linked to cisplatin resistance
4781121161194224355991120163202
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5YearsNo at riskChemotherapy
Control
Control
Chemotherapy
Ove
rall
Sur
viva
l
Adjusted HR=0.65, 95%CI [0.50Adjusted HR=0.65, 95%CI [0.50--0.86], p = 0.0020.86], p = 0.002
Effect of adjuvant chemotherapy on survival in Effect of adjuvant chemotherapy on survival in patients with patients with ERCC1 negative tumorsERCC1 negative tumors
Effect of adjuvant chemotherapy on survival in Effect of adjuvant chemotherapy on survival in patients with patients with ERCC1 negative tumorsERCC1 negative tumors
Soria, ASCO 2006, Abstr # 7010IALT study

18
Adjusted HR=1.14, 95%CI [0.84Adjusted HR=1.14, 95%CI [0.84--1.55], P = 0.401.55], P = 0.40
346285121147165336996127149170
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5YearsNo at risk
ChemotherapyControl
Ove
rall
Sur
viva
lControl
Chemotherapy
Effect of adjuvant chemotherapy on survival in Effect of adjuvant chemotherapy on survival in patients with patients with ERCC1 positive tumorsERCC1 positive tumors
Effect of adjuvant chemotherapy on survival in Effect of adjuvant chemotherapy on survival in patients with patients with ERCC1 positive tumorsERCC1 positive tumors
Soria, ASCO 2006, Abstr # 7010IALT study
Lung cancer - What have we learned?
• Early disease: Adjuvant chemotherapy improves survival
• Advanced disease: Systemic therapy improves survival and QOL
Lung cancer - What have we learned?
• Recognize the unique toxicity profile oftargeted agents
• Biomarkers will provide the platform for
personalized treatment
• Have I missed anything?

19
• Back up slides
Lung Metagene Prognosis
A. Potti, ASCO, 2006, Abstr # 7026
Future Plan
Incorporate LMP into prospective clinical trials of
adjuvant chemotherapy
Biomarker Selection for EGFR Inhibitors:
GGCGGGCCAAACTGCTGGGTGCG
EGFR protein expression by immunohistochemistry
EGFR gene copy number by FISH
EGFR Mutational status
Structure of the EGFR-ATP Binding Site
Red: deletionsLight blue: missense mutationsDark blue: gefitinib
From: Lynch TJ et al. N Engl J Med. 2004;350:2129-2139.
Exons 18, 19, 20 and 21- Tyrosine kinase domain
In frame deletions and missense mutations

20
EGFR mutation and response
RR % OS
EGFR WT
EGFR MT
10
46 p=0.005
No significant difference
Bell, JCO 2005,23:8081
FISH predicts benefit of EGFR-TKIs
Log-rank: p=0.008HR=0.44 (0.23, 0.82)
Log-rank: p=0.59HR=0.85 (0.48, 1.51)
ISEL FISH + BR21 FISH +
Cox: p=0.07HR=0.61 (0.36, 1.04)
BR21 FISH -
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16
Gefitinib Placebo
Proportionsurviving
Time (months)
ISEL FISH -
Cox: p=0.42 HR=1.16 (0.81, 1.64)
Time (months)
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12 18 3024
Erlotinib Placebo
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16
Gefitinib Placebo
Proportionsurviving
Time (months) Time (months)
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12 18 3024
Erlotinib Placebo
Biomarkers
• Conclusions
• EGFR biomarkers: Gene copy number predicts response and survival to EGFR-TKIs.
Mutation predicts response but not improved survival
• Ongoing and planned biomarker trials will evaluate biomarker based treatment approach
Lung cancer - What have we learnt?
• Early disease: Adjuvant chemotherapy improves survival
• Locally advanced disease: Combined chemoradiation improves survival
• Advanced disease: Systemic therapy improves survival and QOL
• Biomarkers will provide the platform for personalized treatment

21
• Thank youN=83Unresectable
stage IIIB NSCLC
Gandara et al. 2006, Clin Lung Ca; 8;116..
Docetaxel(75-100 mg/m2)
q3wfor 3 cycles
Concurrent Chemoradiotherapy → Consolidation Docetaxel in Unresectable
Stage IIIB NSCLC: SWOG 9504
Cisplatin(50 mg/m2 on days 1, 8, 29, 36) +
Etoposide(50 mg/m2 on days 1-5, 29-33) +
Radiotherapy(61 Gy chest [1.8-2.0 Gy/d])
starting on day 1
MS 26mo 5yrS 29%
• Is maintenance therapy required after consolidation docetaxel?
Gefitinib maintenance in inoperable IIIA/ IIIB NSCLC
SWOG 0023
Cisplatin50 mg/2 d 1,8,29,36
Etoposide50mg/m2 d1-5, 29-33
XRT 1.8- 2 Gy/d 61 Gy
DOCETAXEL75 mg/m2x 3 cycles
1o Endpoint: Overall Survival; 20 Endpoint: PFS, toxicity and correlative
PLACEBO
GEFITINIB500 mg/day250 mg/day
RANDOMIZE
Kelly et al. ASCO, 2007, Abstr# 7513.

22
Abstract # 7513Abstract # 7513Overall Survival Overall Survival
0%
20%
40%
60%
80%
100%
0 12 24 36 48 60Months After RANDOMIZATION
Gefitinb
Placebo
N
118
125
Events
71
54
Median
in Months
23
35
P = .01
1 YROS
2 YR OS
73% 46%
59%81%
Median FU time:27 months
Causes of Death by Treatment Arm
Parameter
Gefitinib
%
Placebo
%
Alive 47 71
Dead 71 54
Cancer 61 43
Toxicity 2 0
Other Causes 1 3
Unknown 7 8
N=83Unresectable stage IIIB NSCLC
Gandara et al. 2006, Clin Lung Ca; 8;116..
Docetaxel(75-100 mg/m2)
q3wfor 3 cycles
Is even consolidation docetaxel required?
Cisplatin(50 mg/m2 on days 1, 8, 29, 36) +
Etoposide(50 mg/m2 on days 1-5, 29-33) +
Radiotherapy(61 Gy chest [1.8-2.0 Gy/d])
starting on day 1
MS 26mo 5yrS 29%
Unresectable stage IIIA/B
NSCLC
Hanna et al, Proc ASCO 2007, Abstr# 7512
Docetaxel(75-100 mg/m2)
q3wfor 3 cycles
Concurrent chemo/RT with or without consolidation docetaxel
Cisplatin(50 mg/m2 on days 1, 8, 29, 36)
Etoposide(50 mg/m2 on days 1-5, 29-33)
Radiotherapy(59.4 Gy chest) starting on day 1
Observation
N=73
N=74
1° Endpoint: Overall Survival

23
Months since registration
0 10 20 30 40 50 60
Per
cent
of p
atie
nts
surv
ivin
g
0%
25%
50%
75%
100%
ObservationDocetaxel Consolidation
Abstract # 7512Overall Survival
Observation: 3yr S 27.6%Docetaxel: 3yr S 27.2%
P-value: 0.940
Unresectable stage III NSCLC
• Concurrent chemoradiotherapy• Is superior to sequential chemo-radiotherapy• Should be offered to eligible candidates.
• Consolidation or maintenance therapy• Does not improve OS
• Associated with increased toxicity
• Should not be routinely used
Goldstraw P et al. J Thorac Oncol. 2007;2:706-714.
Staging – Proposed changes
6th Edition T/M and Descriptor
Proposed T/M
T1 (≤ 2 cm) T1a
T1 (2 – 3 cm) T1b
T2 (≤ 5 cm) T2a
T2 (5 – 7 cm) T2b
T2 (> 7 cm) T3
T3 invasion T3
T4 (same lobe nodules) T3
T4 (extension) T4
M1 (ipsilateral lung) T4
T4 (pleural dissemination) M1a
M1 (contralateral lung) M1a
M1 (distant) M1b