nplex combination review dermatology - 3 paul s. anderson, nd medical board review services...
TRANSCRIPT

NPLEX Combination ReviewDermatology - 3
Paul S. Anderson, ND
Medical Board Review Services
Copyright MBRS
Nail Diseases
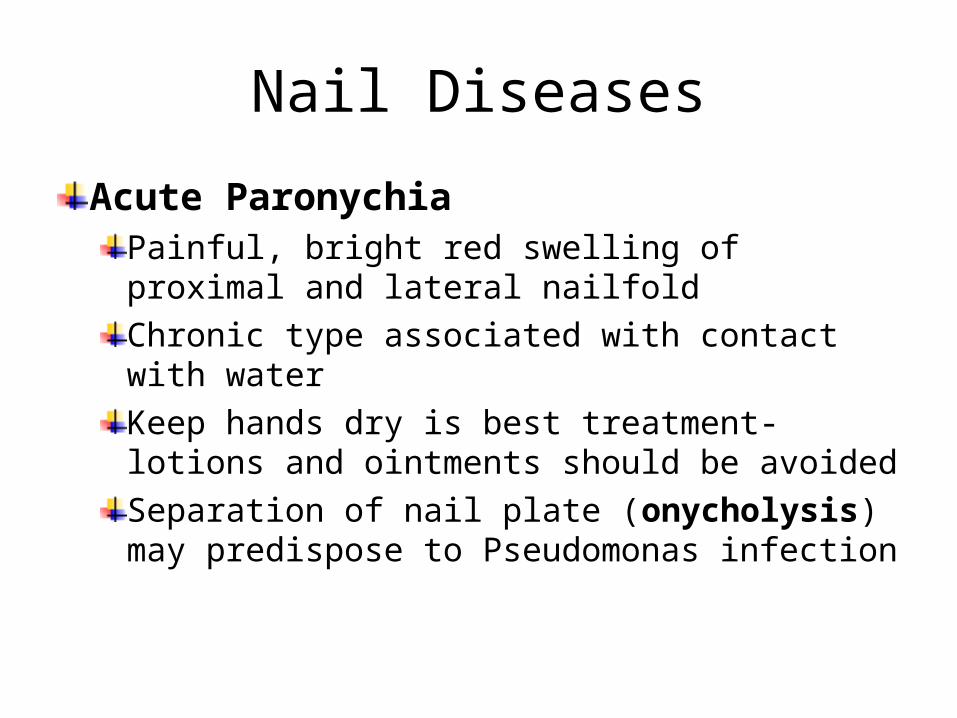
Acute ParonychiaPainful, bright red swelling of proximal and lateral nailfold
Chronic type associated with contact with water
Keep hands dry is best treatment-lotions and ointments should be avoided
Separation of nail plate (onycholysis) may predispose to Pseudomonas infection

Paronychia

Nail Diseases
Fungal
Tinea unguium
Trauma predisposes to infection
DDX: Psoriasis (pitting not found in tinea)
Treatment orally with fluconazole or itraconazole

Tinea Unguium
Contact DermatitisContact Dermatitis
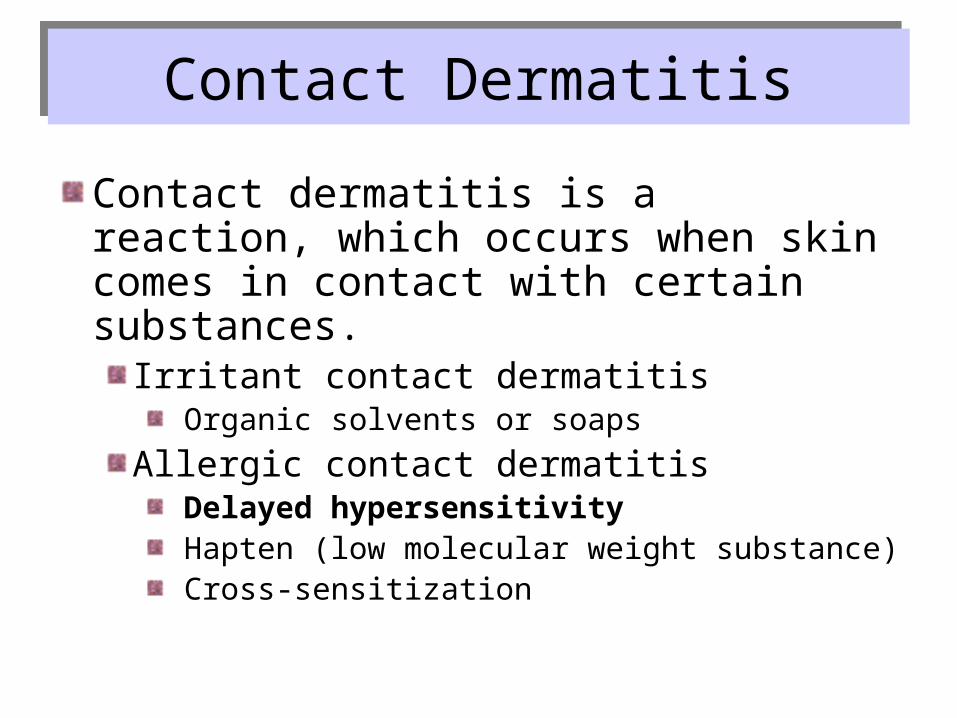
Contact dermatitis is a reaction, which occurs when skin comes in contact with certain substances.
Irritant contact dermatitisOrganic solvents or soaps
Allergic contact dermatitisDelayed hypersensitivityHapten (low molecular weight substance)Cross-sensitization

DiagnosisHistory of onset; work-home exposure; skin care; medications; soaps; clothing (be persistent with questioning)
If problem does not clear:
According to the American Academy of Allergy, Asthma, and Immunology, "Patch testing is the gold standard for contact allergen identification”
Not to be used for irritant contact dermatitis
Contact DermatitisContact Dermatitis
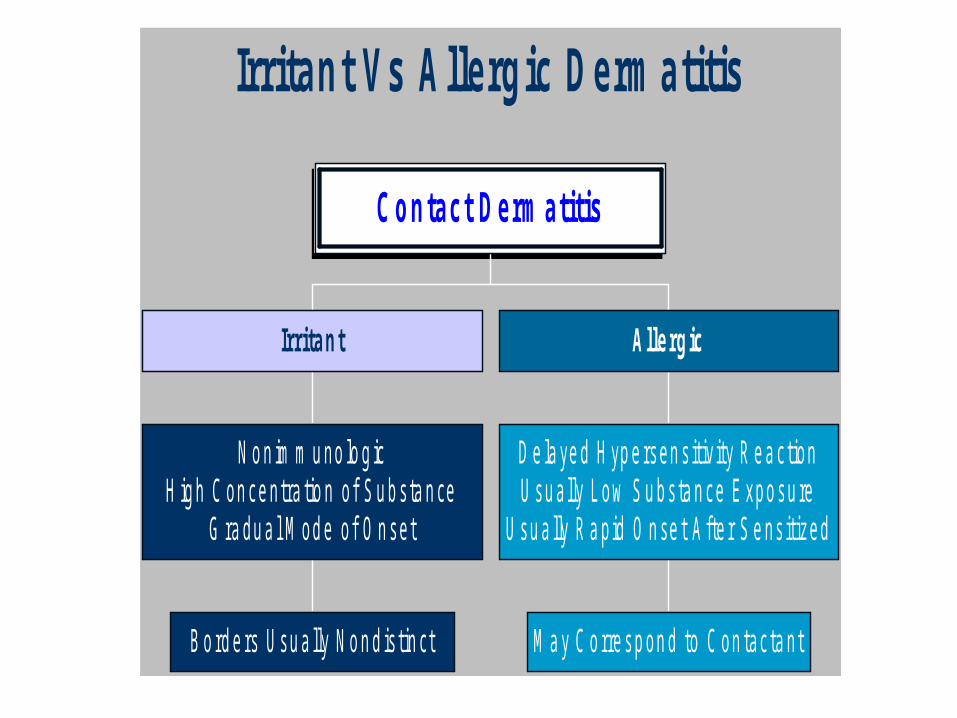
Irritant Vs A llergic D erm atitis
B o rd e rs U su a lly N o n d is tin ct
N o n im m u no lo g icH ig h C on ce n tra tio n o f S u b s ta n ce
G ra du a l M od e o f O n se t
Irritant
M a y C o rre sp on d to C on tac ta n t
D e la ye d H yp e rsen s it iv ity R e a c tionU su a lly L ow S u b s ta n ce E xpo su re
U su a lly R a p id O n se t A fte r S e ns it ized
Allergic
C ontact D erm atitis
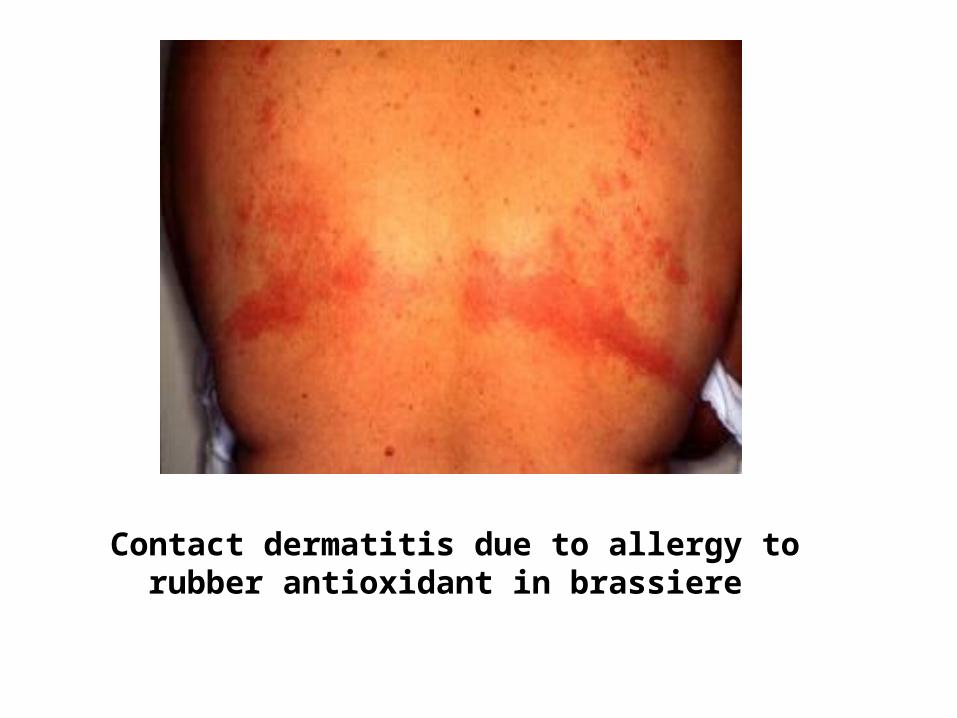
Contact dermatitis due to allergy to rubber antioxidant in brassiere

Contact Dermatitis

Atopic DermatitisAtopic Dermatitis
Major CriteriaPruritus Flexural lichenification (thickening of the skin) and linearity in adults Facial and extensor involvement in infants and young children Chronic or chronically relapsing dermatitis Personal or family history of atopy (asthma, allergic rhinoconjunctivitis, atopic dermatitis)
Labsserum IgE elevated above 200 IU/ml in 80-90%Eosinophilia


Psoriasis
About 2% of adults (Psoriasis vulgaris)
Triggers: rash starts after emotional stress, trauma to skin (Koebner’s phenomenon), strep throat
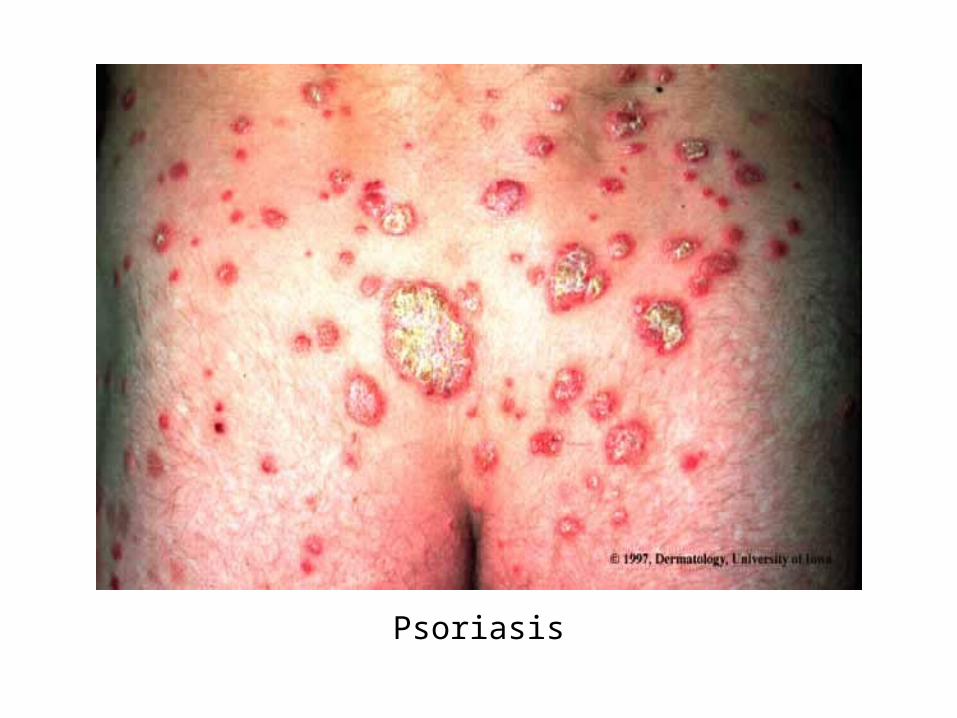
Red scaly-white papules and plaques; removal of scale results in blood drops (Auspitz phenomenon)

Psoriasis
• Plaque• Guttate-strep induced• Palmoplantar
pustulosis• Inverse
Psoriasis

Seborrheic dermatitis
Chronic superficial inflammatory process of hairy regions of the body
Pityriasis capitis (dandruff)
Cradle Cap (thick, yellow, crusty scalp lesions in infants)
Proliferation of Pityrosporum ovale (yeast)
Triggered by stress, fatigue, change of season or reduced general health

Seborrheic Dermatitis
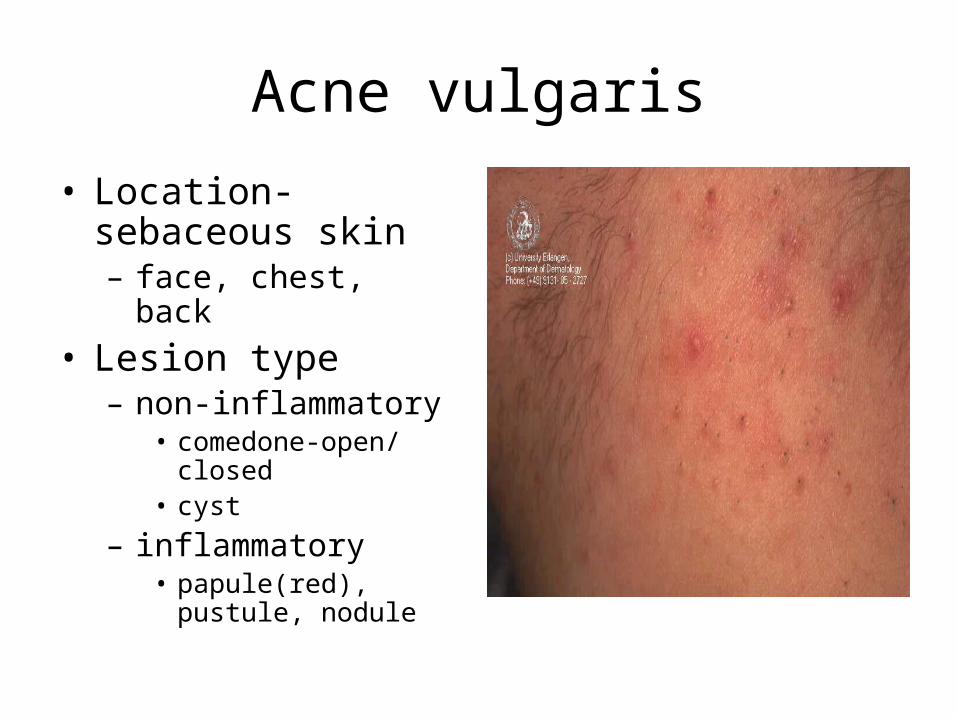
Acne vulgaris
• Location-sebaceous skin– face, chest, back
• Lesion type– non-inflammatory
• comedone-open/closed• cyst
– inflammatory• papule(red), pustule,
nodule
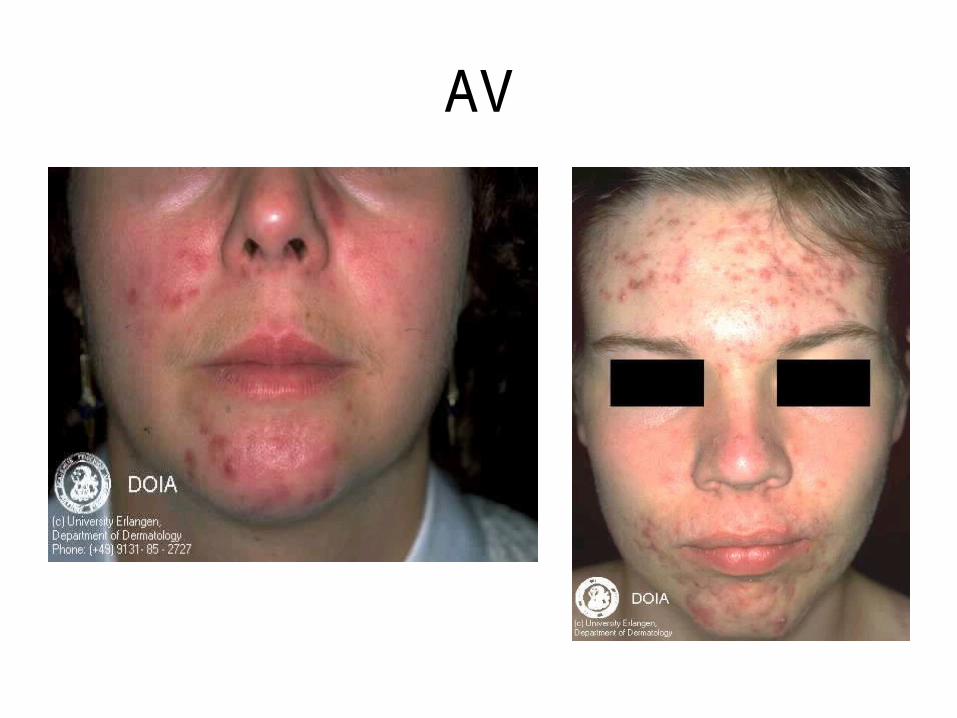
AV

Treatment
• Correct abnormal keratinization (plugging)– Vit A cream
• Kill bacteria– topical ABX, oral ABX,
Benzoyl peroxide
• Decrease inflammation– Tetracycline family
• Minocycline
– Diet- decrease refined sugars/fried foods.
– Sunlight/blue light
• Correct hormone imbalance
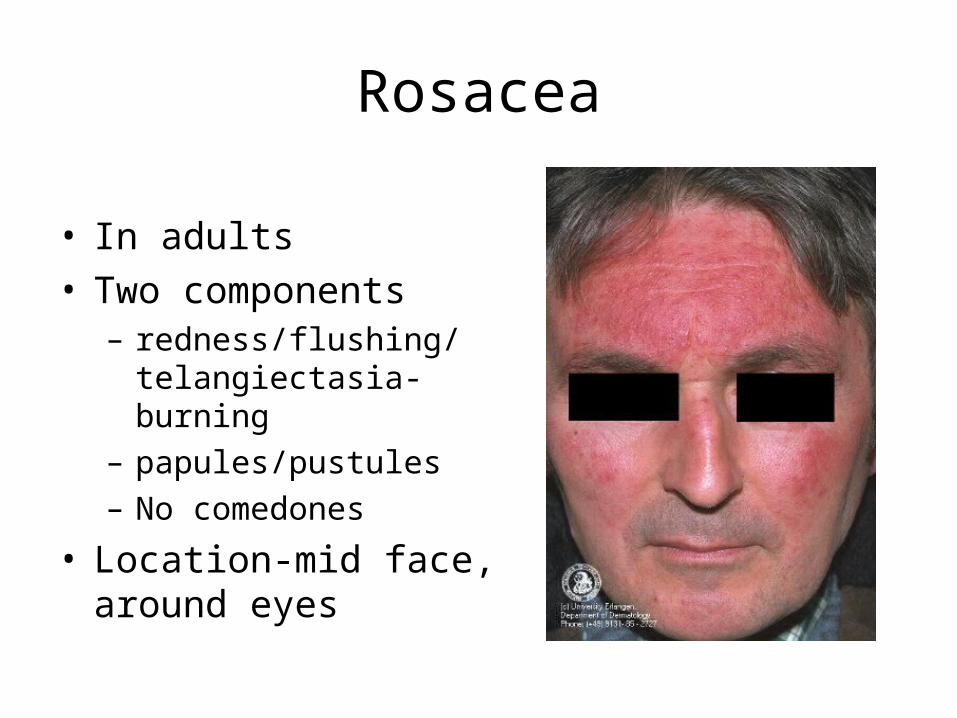
Rosacea
• In adults• Two components
– redness/flushing/telangiectasia-burning
– papules/pustules– No comedones
• Location-mid face, around eyes
Etiology
• Unknown- some relation to acne
• Racial group – Northern Europeons– Celtic– Men worse than
women
• Triggers– Emotional stress-
people who blush– Hot/cold air (exercise)– Food
• cheese, wine, spicy food, coffee
• Very Chronic
Pityriasis albaPityriasis alba
Children and young adults
Round or oval; slightly elevated, fine scaling plaque that leave pale marks (hypopigmented) usually on face, neck and arms
DDX: vitiligo, tinea versicolor (How do you tell?)
Vitiligo and tinea versicolor appear white; borders are distinct in vitiligo; tinea versicolor is rare on the face and areas more numerous and often confluent; KOH to settle the debate
Vitiligo and tinea versicolor appear white; borders are distinct in vitiligo; tinea versicolor is rare on the face and areas more numerous and often confluent; KOH to settle the debate
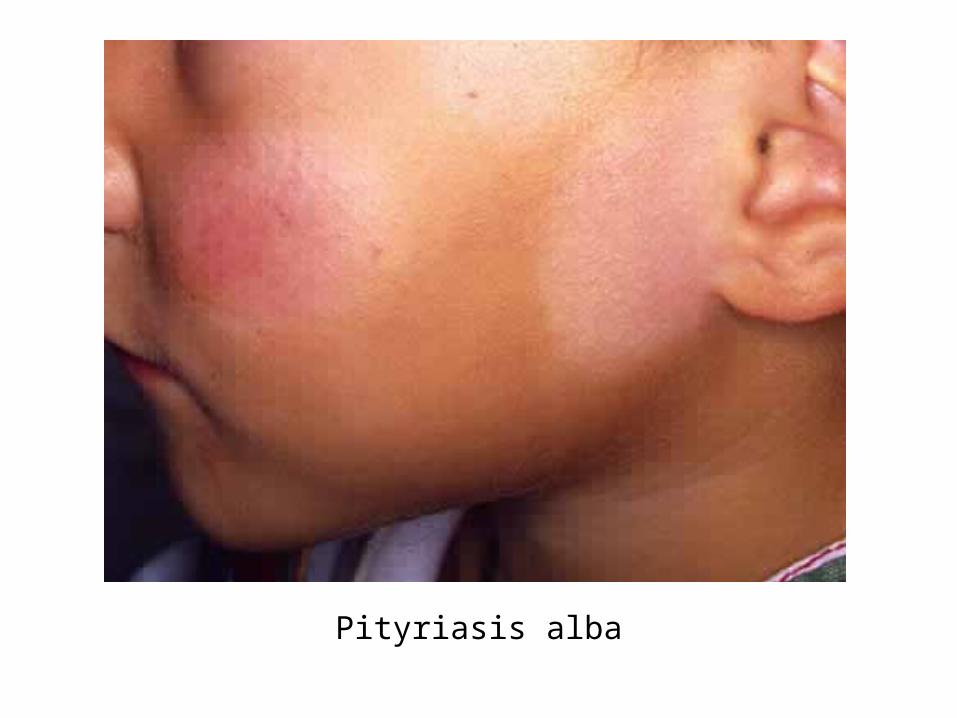
Pityriasis alba
Pityriasis rosea
• Teenagers and young adults; benign• No known cause but linked to
mycoplasma, picornavirus and human herpesvirus 7
• “Harold Patch” (plaque) precedes eruption then followed by smaller plaques (0.5 to 2 cm in diameter)
• Follows long axes parallel lines of cleavage starting at spine (Christmas tree-like pattern)
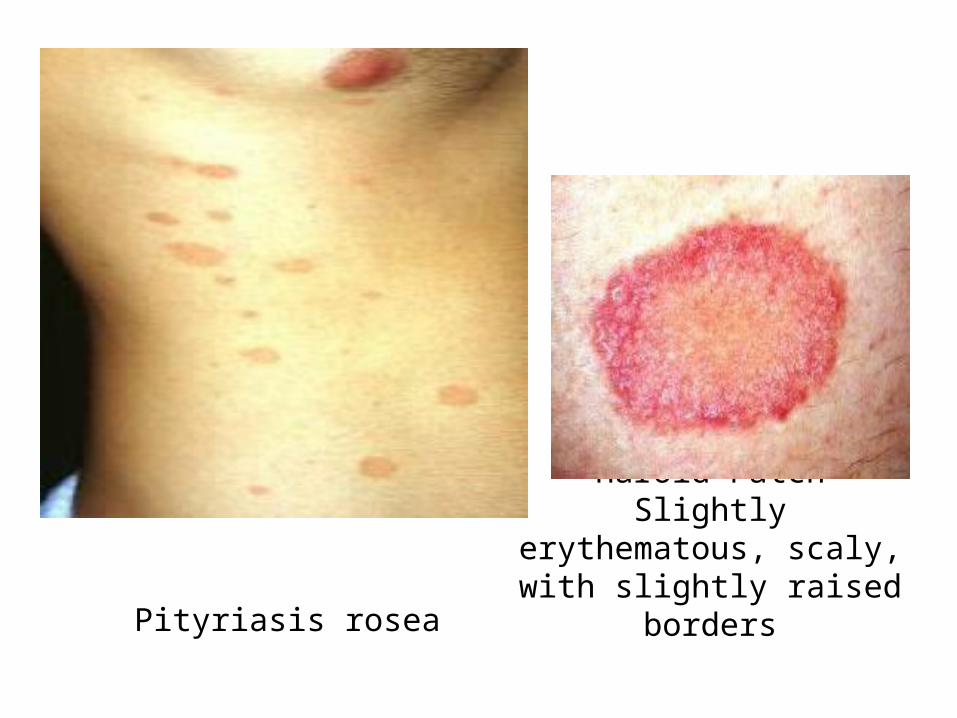
Harold PatchSlightly erythematous,
scaly, with slightly raised bordersPityriasis rosea
Lichen simplex (neurodermatitis)
Common disorder, usually adults
Repeated rubbing or scratching resulting in itchy patch of skin
Sharply demarcated, red, scaly plaque with prominent skin lines

Lichen Simplex
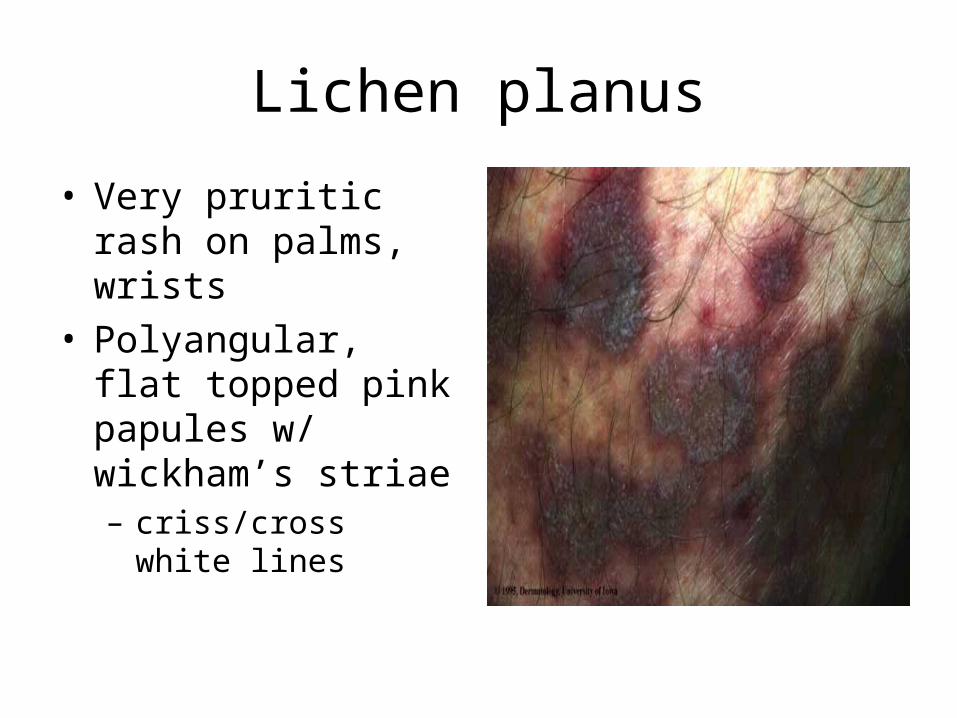
Lichen planus
• Very pruritic rash on palms, wrists
• Polyangular, flat topped pink papules w/ wickham’s striae– criss/cross white lines

Verruca vulgaris (warts)
Epithelial tumors caused by at least 60 types of human papillomavirusFrequent in older children, uncommon in elderlyCommon Type: flesh-colored papules evolve to dome-shaped, gray-brown, hyperkeratotic growths with black dots on the service

Verruca vulgaris (Common)

Tinea
Tinea incognito when the clinical appearance has changed because of inappropriate treatment
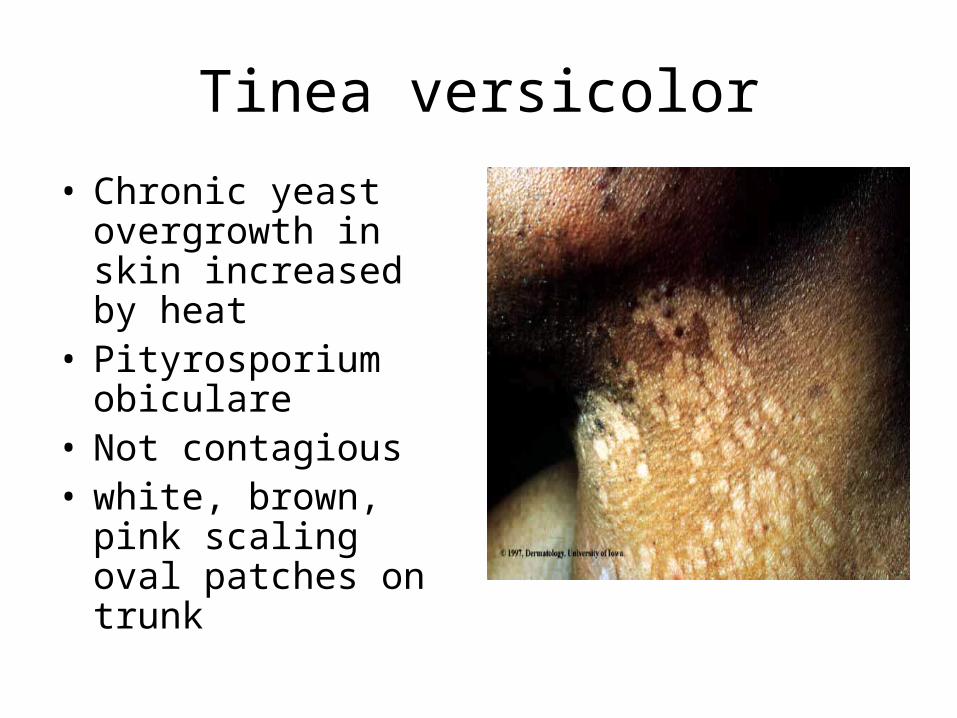
Tinea versicolor
• Chronic yeast overgrowth in skin increased by heat
• Pityrosporium obiculare
• Not contagious• white, brown, pink
scaling oval patches on trunk
Candidiasis
Oral called thrush in infantsAdult: check for diabetes, depressed immunity, elderly and patients with cancerProlonged corticosteroids or broad spectrum antibioticsCandidiasis of large skin folds
Warm and moist areas (under breasts, groin and armpits, diapers)

Dyshidrotic EczemaDyshidrotic Eczema
Symmetric, vesicular hand and foot dermatitis
Preceded by moderate to severe itching
Palms may be red and sweating
Aggravated by contact with irritants such as water, detergents and solvents
High incidence of nickel allergy


Vitiligo
• Pigment cells are destroyed resulting in white patches
• Associated with increased risk of autoimmune disorders (thyroid, pernicious anemia, Addison’s, and alopecia areata)
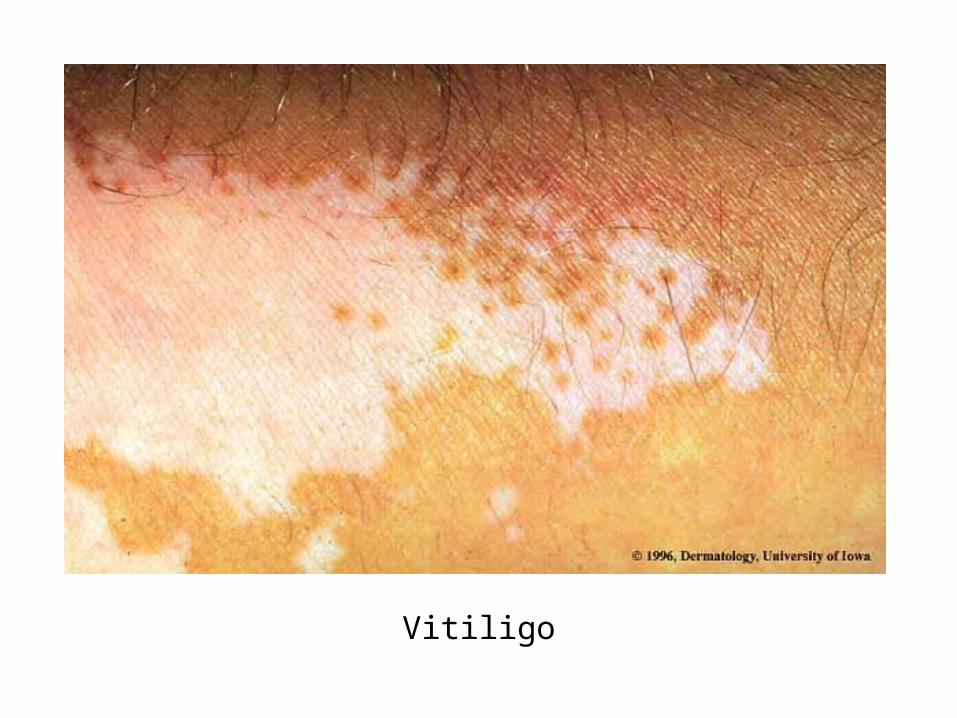
Vitiligo