novel psychoactive substances [email protected]
TRANSCRIPT

Novel Psychoactive [email protected]

NPS Background Confusing terminology
“Designer Drugs” “Bath Salts” “Legal Highs” Definition
“Psychoactive drugs, newly available in the UK, which are not prohibited by the United Nations Drug Conventions but which may pose a public health threat comparable to that posed by
substances listed in these conventions”
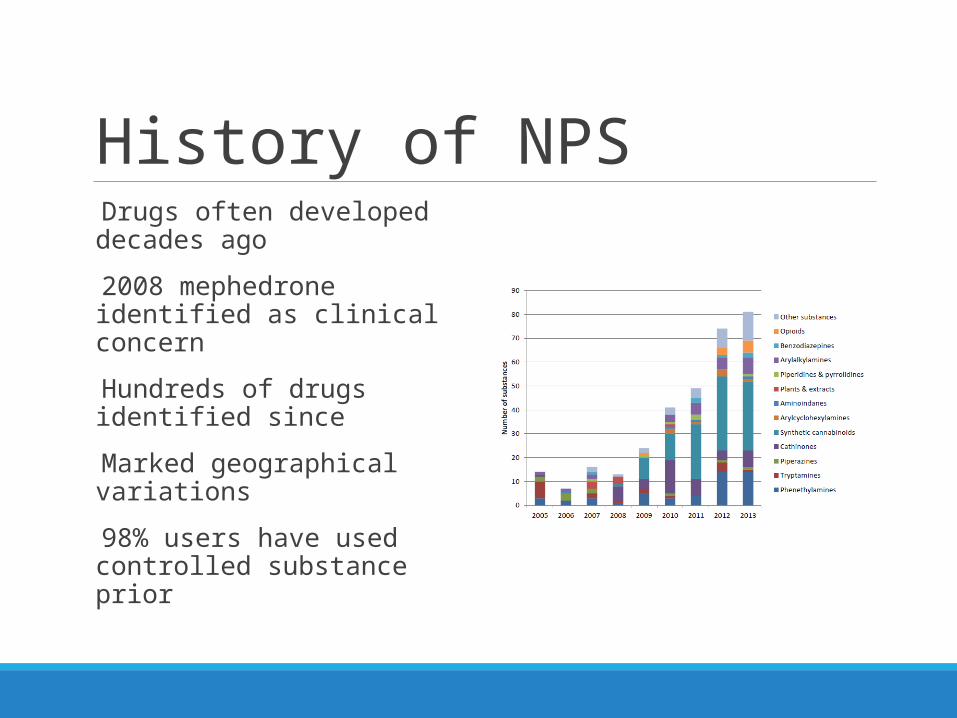
History of NPS Drugs often developed decades ago
2008 mephedrone identified as clinical concern
Hundreds of drugs identified since
Marked geographical variations
98% users have used controlled substance prior
Supply of NPS “Head shops”, Internet, Dealers ,Mates!
Branding Various compounds branded under the same name e.g. “burst” “Research chemicals” Marked “not for human consumption”
FEWS analysis 61% 2 active drugs 30% 3 active components 88% festival samples contained controlled drugs 2013/2014

Challenges Unknown toxicology
◦ Mechanism of action◦ Duration of action◦ Metabolism◦ Interactions (including prescription drugs)◦ Short term & long term harms
Identification of use◦ Self reporting◦ Post-mortem toxicology◦ Role of urine toxicology screens
Clinical Presentations Concern over health
Extended duration of symptoms
Abnormal behaviours◦ Mild abnormalities◦ Drug induced psychoses◦ Acute behavioural disturbance
Acute drug toxicity
Harm associated with intoxication
Consequences of method of drug use
Local Demographics Ages from 12 to 50
Equal sex distribution
Depends on the substance
Polysubstance use is markedly prevalent◦ Alcohol +++
Approx 44 needle exchange service users NPS
MSM and “slamming”

Synthetic Cannabinoids Sold openly from head shops
Annihilation, Psy-clone, Clockwork Orange, Damnation, Exodus etc
Potent endogenous cannabinoid receptor agonists
Commonly smoked, ? “vaping”
Often present with Nausea +++ Collapse Dissociation, coma Drug induced psychosis

Benzodiazepines Phenzepam, etizolam, diclazepam
1mg = 10mg diazepam
May or may not be detected on urine drug screens
Increasingly responsible for presumed opiate toxicity
Recent study from Abertay Uni & Police Scotland “street blues” found to contain from 8mg to 48mg diazepam Phenazepam & etizolam detected
Ketamine Mimics & Hallucinogens
Methoxetamine, 3-MePCP, methoxphenidine◦ Induce dissociation NMDA receptor antagonists◦ Prolonged duration of action◦ Cerebellar signs
N-BOMe, DOC
Sold on blotters (like LSD)
20 hour duration of action
Drug induced psychosis and threat to life behaviours


Cathinones Mephedrone, methedrone, butylone, MDPV
Meow Meow, bubbles, M-CAT, Meph (not meth or “ma meff!)
Similar mechanism of actions ◦ Catecholamine reuptake inhibitors◦ Dopamine releasers (particularly MDPV)
Commonly ingested, but insufflated, injected, and “bumping”
Predominantly stimulant effects, but some MDMA mimicry

Ethylphenidate Sold as “burst”
Ethylphenidate +/- benzocaine
Responsible for major outbreak of drug induced psychosis in Lothian
Related to methylphenidate but much more potent
Addictive Multiple hits per day (some over 6 times) Risky injecting sites Predominantly ex-heroin users who were stable
Injecting wounds causing significant concerns

Ecstasy Mimics BZP, PMA/PMMA, Benzo Fury, AMT, MDAI
Often sold as Ecstasy, or “legal equivalents” (most now illegal)
Mimic the empathogenic effect
Potent inducers of serotonin toxicity
Serotonin Toxicity Characterised by
Increased muscle activity Abnormal mental status Autonomic instability
Spectrum of toxicity
5-HT2A receptor thought to be responsible
Increased level of serotonin at synaptic level Decreased reuptake Serotonin release MAO – inhibition (direct receptor stimulation)


Acute Behavioural Disturbance
Challenging◦ Potentially life threatening to patient◦ Risk to care providers, police, public
Extremely difficult to manage
May be prolonged (e.g. desoxypipradol)
Resistant to conventional interventions
Doses of benzodiazepines & antipsychotics much greater
Avoid prolonged physical restraint
Emergency anaesthesia may be required
NPS & Mental Health NPS responsible for drug induced psychoses Ethylphenidate has 2 “phases”
◦ Acute florid episode associated with intoxication◦ Protracted symptomology for weeks following abstinence
Changes in neurotransmitters◦ Dopamine reuptake/release/? receptor stimulation◦ Serotonin reuptake/release/receptor stimulation◦ Nor-adrenaline metabolism
Poorly responsive to treatment Implications for treatment & continuation of medications
Summary NPS are here to stay
Challenging area◦ Limitations with identification of use◦ Toxicology◦ Diagnostic coding
Drug induced/related mental illness will rise
Don’t forget “classic” drugs of abuse